

COVID-19, caused by the severe acute respiratory syndrome corona virus 2 (SARS-CoV-2), is the ongoing pandemic which has been unprecedented.[1] We are witnessing some extraordinary times which were unimaginable even a few months ago. These desperate times have called for certain desperate measures which include worldwide lockdowns. In the past 20 years, we have witnessed two major epidemics caused by coronaviruses: SARS-COV in 2002 and Middle East respiratory syndrome (MERS)-COV in 2012. The number of people infected due to these two viruses were minuscule (8000 by SARS-COV and 800 by MERS-COV) in comparison to the current COVID 19 pandemic (confirmed cases – 4,013,728 and deaths – 278,993 on May 12, 2020).[2] This has been attributed to the difference in R0 values (3–6 for SARS-COV-2), high viral loads in the upper respiratory tract, and the potential for infected persons with SARS-CoV-2 to shed and transmit the virus even while being asymptomatic.[3,4] R0 (R naught), also known as reproduction number, indicates how contagious an infectious disease is. An R0 of 3–6 in simple terms means that a person suffering from the infection will transmit it to an average of 3–6 people. The rising number of current pandemic mirrors those of the Spanish flu of 1918. Similarly, it might not be surprising that the COVID 19 pandemic may last for a long time.[5] The worst affected countries such as the USA, Italy, and Spain have mobilized the entire health resources from all specialties to the COVID teams for managing these cases. So much so that in New York, each doctor has been labeled a COVID doctor.[6]
In a resource-limited country like ours, we have to gear up to tackle the surge. At the time of this writing, we in India are in our third extension of the lockdown period. Around 96,000 cases have been diagnosed countrywide and more than 3000 deaths have been reported so far.[7] Fighting the COVID pandemic and at the same time, balancing the collateral damage is the target. The collateral damage includes morbidity and deaths due to socioeconomic impact of lockdowns and due to nonCOVID illnesses.
Being a tertiary care center as well as a COVID-dedicated facility, our institution is involved in formulating and implementing strategies for optimizing health-care outcomes. The dynamism of the current situation can be gauged by the fact that repeated attempts of reinstating elective services have been deferred. This is causing a delay in the treatment of urological illnesses. As soon as the lockdown is eased, the rush of patients who were simply “managing” their illnesses will flock the outpatient departments (OPDs). Hence, we should be ready with an action plan to prioritize and triage these patients to manage this damage. Through this document, we wish to provide a framework for performing elective and emergency urological procedures and discuss the changing paradigm of urological practice in this COVID era.
SCREENING FOR COVID
During the initial phase of the lockdown, patients visiting the emergency department in our hospital were being screened using a symptom-based questionnaire [Figure 1] and were initially stratified as COVID suspect or not. Those who were suspected to have COVID underwent reverse transcriptase–polymerase chain reaction (RT-PCR) test. Based on this method after the screening, we admitted 62 patients during this lockdown period. With increasing COVID-positive cases in the community and planned resumption of elective services, we believe that this screening method based on symptom-based questionnaire alone will not be sufficient., Considering the high infectivity and perioperative mortality (20%) in COVID 19 carriers/patients, every attempt should be made to diagnose carriers of SARS-CoV-2 before surgery.[8]
Figure 1.
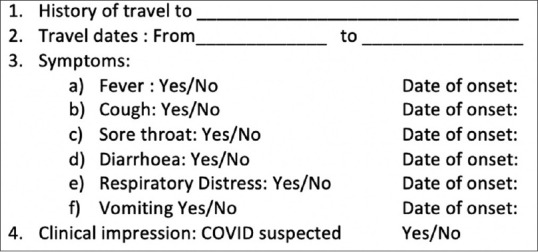
Symptom-based questionnaire for screening of patients
Upper airway secretions collected by oropharyngeal and nasopharyngeal swabs are most commonly used for doing RT-PCR testing. Studies have shown that the detection rate of RT-PCR in samples collected from the upper respiratory tract for SARS-CoV-2 was 38%–63% only.[9,10] Hence, screening with only oral and nasal swabs can miss out a large proportion of SARS-CoV-2 carriers. Li et al. have shown that serological testing using combined immunoglobulin M (IgM) and IgG rapid enzyme-linked immunosorbent assay (ELISA) kits can detect SARS-CoV-2 with a sensitivity and specificity of 88.66% and 90.63%, respectively.[11] They recommended that a combination of nucleic acid RT-PCR and IgM/IgG antibody test can provide the accurate diagnosis of SARS-CoV-2 infection. Hence, any patient who is tested negative on RT-PCR should also undergo serological testing with IgM and IgG ELISA for detecting carriers.[12,13] However, the availability of serological test kits and their questionable reliability (based on the recent report from the Indian Council for Medical Research showing the sensitivity of rapid ELISA kits is around 6%–71%) pose serious problems in incorporating these tests in the treatment algorithm.[14] Hence, we advocate continued use of symptom-based screening and addition of RT-PCR before embarking on the elective procedure to save the treating team from cross-infection.[13]
Based on the above protocol, we operated 44 patients during this lockdown period, and none of these patients developed symptoms of COVID following surgery [Table 1]. In case the patient is deemed a confirmed/suspected COVID case, they should be referred to a dedicated health facility for treating COVID cases in accordance with the 3-tier classification of health facility by the government of India.[15] Our institution has a separate dedicated COVID hospital block with operation theaters (OTs), intensive care units, wards, in-house investigation laboratories, and imaging facilities.
Table 1.
Urological surgical burden before and after lockdown over comparable time duration at our tertiary care center
| Surgical procedure (emergency) | Cases performed just before lockdown (over 45 days) | Cases performed during lockdown (March 25, 2020-May 10, 2020) |
|---|---|---|
| TURBT | 42 | 31 |
| Radical cystectomy and ileal conduit | 0 | 4 |
| Nephrectomy | 11 | 1 |
| Debridement for Fournier’s gangrene | 2 | 4 |
| Open clot evacuation | 1 | 1 |
| High inguinal orchiectomy | 4 | 1 |
| Radical nephroureterectomy | 0 | 1 |
| Bladder repair | 1 | 1 |
| Total Emergency surgeries | 61 | 44 |
| Surgical procedure (elective) | ||
| Endourologic surgeries | 141 | 0 |
| Laparoscopic surgeries | 39 | 0 |
| Robot assisted surgeries | 46 | 0 |
| Open surgeries | 37 | 0 |
| Total elective surgeries | 263 | 0 |
| Overall surgeries | 324 | 44 |
TURBT=Transurethral resection of bladder tumor
EMERGENCY UROLOGICAL SURGERIES
Since the beginning of lockdown, all elective outpatient clinics and elective inpatient admissions have been suspended at our institution and as recommended by all guidelines, only emergency procedures are being done.[16,17] The rationale for this is to conserve the already strained health-care resources. We have been catering to emergency services which primarily involve malignancies with active hematuria, urosepsis, and urological trauma [Table 1]. Cases of obstructive uropathy with or without sepsis secondary to stones/stricture in the urinary tract are being managed by urgent diversion using percutaneous nephrostomy (n = 16) or double-J stent placement (n = 3). Cases of acute or impeding urinary retention secondary to benign prostatic hyperplasia or urethral stricture are being managed by per-urethral catheterization or suprapubic catheter placement (n = 26). Neoadjuvant chemotherapy was administered to fit patients to defer elective surgery (n = 3). As elective procedures have come to a standstill, emergency procedures are expected to rise further. There is a 86% fall in urological surgeries during the lockdown period at our center.
ELECTIVE UROLOGICAL SURGERIES
Telemedicine instead of physical OPD visit should be used for consultation and planning elective surgeries. This will help in minimizing visits at the OPDs. Recently, the Ministry of Health and Family Welfare has provided guidelines for carrying out telemedicine services.[18] All hospitals should create their own Standard Operating Procedures (SOPs) for conducting telemedicine services. Elective surgeries should be planned only when the number of COVID positive cases poses a low burden on the health-care resources of the hospital. Therefore, continuous audit of the bed occupancy status, amount of hospital staff, and equipment available should be done before considering elective surgeries. Needless to say, malignancies should get top priority. Patients with other benign conditions should also be prioritized according to the disease. For example, patients with obstructing renal or ureteric stones already on double-J stent or percutaneous nephrostomy should also be given priority.[19] After prioritizing the cases, they should be planned for operation only after screening for SARS-CoV-2. Both the European association of Urology (EAU) and Urological Society of India (USI) have released their advisories regarding stratification of various urological procedures.[16,17]
ANESTHESIA CONSIDERATIONS
General anesthesia (GA) leads to aerosol generation as it involves close manipulation of the oral cavity and upper airway tract. It therefore poses the highest chance of transmission to OT team. Hence, avoiding GA would significantly reduce exposure to patients’ respiratory secretions. It will also protect the anesthesia machine and its accessory equipment's from getting into contact with the respiratory secretions. Hence, wherever feasible, regional anesthesia (RA) should be considered. Patients undergoing surgery under RA should always wear a filtering facepiece 2/3 mask.
RA has lower postoperative cardiopulmonary and thromboembolic complications due to continued postoperative analgesia and early ambulation. There have been concerns regarding the presence of virus in cerebrospinal fluid and consequential transmission to the anesthetic team during the administration of RA.[20] Zhong et al. have suggested that anesthetists should use level 3 personal protective equipment (PPE) while giving spinal anesthesia.[21] All our endoscopic cases were performed under spinal anesthesia.
Patients who are considered for GA should be induced by an experienced anesthesiologist. High-efficiency hydrophobic filters should be used between the face mask and breathing circuit. 100% preoxygenation with rapid sequence intubation should be preferred.[22] Awake fiberoptic intubation should be avoided at any cost. Tracheal intubation should be always be preferred over laryngeal mask airway.[22] In addition to RA, an obturator block may be used during resection of bladder tumors.[23] Although most urologists prefer GA for endoscopic renal surgery, RA has equivalent efficacy and safety outcomes with possibly reduced operative time, hospitalization stay, blood transfusion rates, and postoperative pain without compromising stone clearance rates.[24,25,26,27]
GENERAL SURGICAL CONSIDERATIONS
Minimum staff should be posted in the OT and should wear PPE, as suggested by the hospital policy. PPE in the form of N95 masks, goggles or face shield, impervious gowns, and gloves should be used. Hand hygiene should be strictly followed. Donning and doffing procedures should be strictly adhered to. OTs should be adequately ventilated with preferably negative pressure ventilation and High-efficiency particulate air (HEPA) filters should be mandatory.
Endourological procedures
There is a high chance of contacting the patient's urine while doing these procedures. Evidence for virus presence in urine is not robust. While viral RNA has been identified in the urine samples of 6.9% patients who had recovered from COVID-19, others have reported that virus shedding in urine is absent.[10,28] However, to decrease the chance of contamination, the entire operating team should take necessary precautions such as the use of fluid impervious drapes, disposable equipment, and closed drainage of returning irrigation fluid.
Laparoscopic/robot-assisted procedures
There are concerns regarding laparoscopic surgeries due to risk of transmission of virus from aerosol created by CO2 gas used for pneumoperitoneum or smoke plume generated from electrocautery.[29] These are based on studies on hepatitis B virus, HIV, and human papilloma virus in surgical smoke.[30,31,32] As of now, there has been no report of transmission of SARS-CoV-2 to the operative personnel following laparoscopy. All the surgical societies currently hold that there is insufficient evidence to recommend for or against an open versus laparoscopic approach in COVID era.[16,17,33,34] However, the Royal College of Surgeons and EAU Robotic Urology Section stated that laparoscopy should be considered only in select individual cases.[33,34] The USI has also issued advisory to avoid laparoscopic and robotic procedures.[17]
The generation of aerosol/pneumoperitoneum leak can occur at various points during laparoscopy: during exchange/insertion of instruments and trocars; practice of intermittent venting of the abdomen off smoke through stopcock of the trocar; and while decompressing the abdomen at the end of the procedure or for retrieval of specimen or for conversion to open surgery. To minimize the risk of transmission, we recommend the following precautionary measures.
Port incisions should be of appropriate size and ribbed or ballooned ports should be used to prevent air leak. The use of integrated intelligent flow system such as AirSeal system (Conmed, NY, USA), etc., is recommended. Operating pressures should be kept to minimum (8–10 mmHg).[30,31,32] Ultrasonic device and electrocautery should be activated for a minimum time at minimum energy settings to decrease smoke plume formation. Instrument change should be kept to minimum. Suction device or wet gauze pieces/sponges should be used to prevent aerosol transmission. Smoke evacuation should be minimized using stopcock and it should be done through a dependent port attached to a vacuum suction unit. Before placing an incision for specimen retrieval, the abdomen should be deflated completely using suction and release of gas by the filtered port with the use of vacuum.
In case dedicated air seal systems are not available, filters used in mechanical ventilator circuits may be borrowed from the anesthetist. For robot-assisted surgeries, the majority of the precautions apply. In addition, the use of reducers should be minimized and if used, they should be snugly fit to avoid leak. However, we recommend that in COVID era, the use of laparoscopy should be minimized wherever possible. We have resorted to open surgical approach even for patients who were surgically fit candidates for laparoscopy.
Open procedures
Adequate measures to minimize the generation of aerosol like minimal use of electrocautery and harmonic shears, minimal energy settings, and the use of smoke evacuation devices intraoperatively should be followed. The majority of oncological procedures have been performed under RA with equivalent outcomes.[35,36] In pelvic surgeries, Combined Epidural Spinal Anasthesia (CESA) offers the advantages of reduced volume need, decreased perioperative blood loss, and maintaining postoperative analgesia.[37] For pelvic surgeries, Trendelenburg position should be minimized to avoid pulmonary congestion, respiratory compromise, and aerosol production. Substitution urethroplasty using buccal mucosal graft (BMG) needs a special mention here.[38] It is the only urological procedure where a urosurgeon comes in close contact with the oral cavity. In the era of COVID-19, harvesting BMG could pose a potential risk of cross infection between the patient and health-care workers. In our opinion, avoiding BMG and the use of inner preputial graft (IPG) for substitution urethroplasty may be safer with equivalent outcomes.[39] We feel that open procedures are likely to increase across specialties in the current era.
SURGERY IN CONFIRMED COVID-19 CASES
COVID 19-confirmed cases should be evaluated by a multidisciplinary team, and the treatment of the viral illness takes precedence over the underlying urological disease, unless emergent. All the SOPs related to surgery in a COVID positive case should be followed as recommended by the WHO.[40] A flowchart depicting the management of urological cases in the current COVID era is given in Figure 2.
Figure 2.
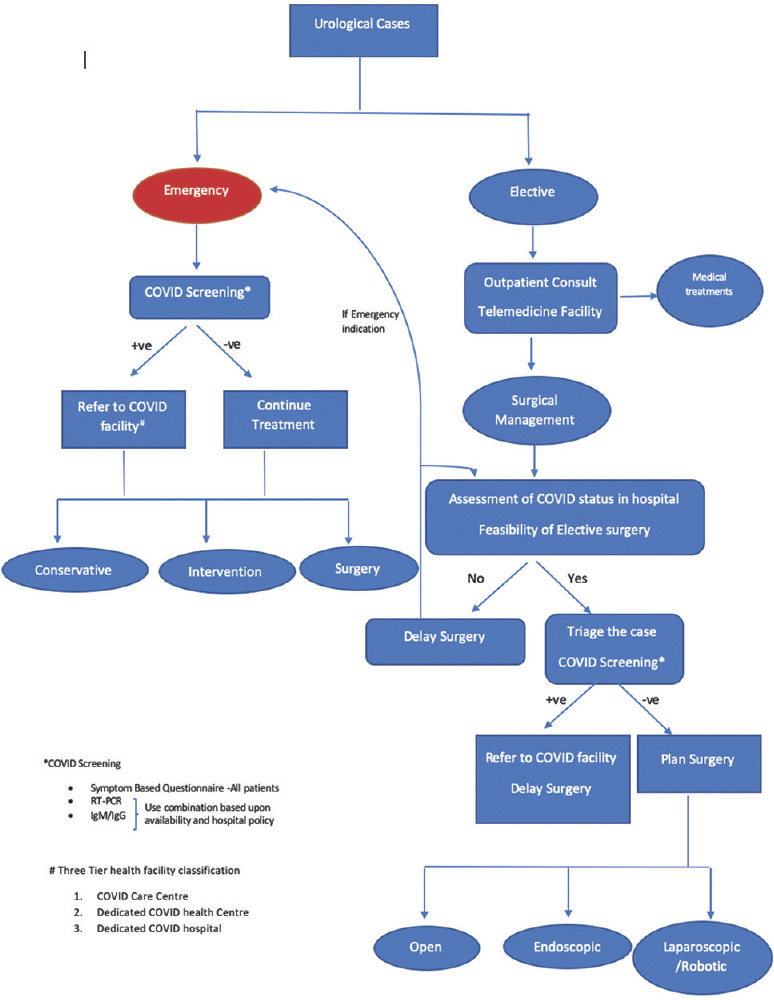
Algorithm for management of urological patients during COVID era
In summary, SARS-CoV-2 is here to stay and major modifications loom over surgical practices. Resource allocation in the management of COVID-19 and emergency services will take precedence over elective procedures. Screening for COVID-19 should be the norm. Universal precautions and use of PPE should be strictly adhered to. RA should be considered over GA, wherever feasible. Open surgical approach should be preferred over minimally invasive approach till further evidence is available. Limiting the casualties due to COVID-19 and addressing the collateral damage by non-COVID illnesses are the need of the hour.
Financial support and sponsorship:
Nil.
Conflicts of interest:
There are no conflicts of interest.
Footnotes
Financial support and sponsorship: Nil.
Conflicts of Interest: There are no conflicts of interest.
REFERENCES
- 1.WHO Director-General's Opening Remarks at the Media Briefing on COVID-19. 2020. [Last accessed on 2020 Mar 11]. Available from: http://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 .
- 2.Cornavirus Disease (COVID-19) Pandemic. [Last accessed on 2020 May 12]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 .
- 3.Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA. 2020;14(323(14)):1406–7. doi: 10.1001/jama.2020.2565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382:1177–9. doi: 10.1056/NEJMc2001737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Boston Consulting Group. Epidemic Projections. [Last accessed on 2020 May 22]. Available from: https://lasillarotarm.blob.core.windows.net/docs/2020/04/04/bostonconsultinggroup_1.pdf .
- 6.Jaiswal R. An Indian Doctor, Working in New York ER, Describes War vs. Coronavirus. [Last accessed on 2020 May 18]. Available from: https://www.ndtv.com/blog/an-indian-doctor-working-in-new-york-er-describes-war-vscoronavirus-2219095 .
- 7. [Last accessed on 2020 Mar 18]. Available from: https://www.covid19india.org/
- 8.Lei S, Jiang F, Su W, Chen C, Chen J, Mei W, et al. Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. E Clinical Medicine 2020. 2020 Apr 5;:100331. doi: 10.1016/j.eclinm.2020.100331. doi: 10.1016/j.eclinm.2020.100331. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Liu R, Han H, Liu F, Lv Z, Wu K, Liu Y, et al. Positive rate of RT-PCR detection of SARS-CoV-2 infection in 4880 cases from one hospital in Wuhan, China, from Jan to Feb 2020. Clin Chim Acta. 2020;505:172–5. doi: 10.1016/j.cca.2020.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wang W, Xu Y, Gao R, Lu R, Han K, Wu G, et al. Detection of SARS-CoV-2 in Different Types of Clinical Specimens [published online ahead of print, 2020 Mar 11] JAMA. 2020;323:1843–4. doi: 10.1001/jama.2020.3786. doi:10.1001/jama.2020.3786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Li Z, Yi Y, Luo X, Xiong N, Liu Y, Li S, et al. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis [published online ahead of print, 2020 Feb 27] J Med Virol. 2020 doi: 10.1002/jmv.25727. 10.1002/jmv.25727. doi:10.1002/jmv.25727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhang W, Du RH, Li B, Zheng XS, Yang XL, Hu B, et al. Molecular and serological investigation of 2019-nCoV infected patients: Implication of multiple shedding routes. Emerg Microbes Infect. 2020;9:386–9. doi: 10.1080/22221751.2020.1729071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Al-Muharraqi MA. Testing recommendation for COVID-19 (SARS-CoV-2) in patients planned for surgery - continuing the service and 'suppressing’ the pandemic [published online ahead of print, 2020 Apr 13] Br J Oral Maxillofac Surg. 2020;S0266-4356:30164–9. doi: 10.1016/j.bjoms.2020.04.014. doi:10.1016/j.bjoms.2020.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Coronavirus Update: Covid-19 Rapid Testing Kits use Suspended for Two Days Due to ‘Errors’. [Last accessed on 2020 May 18]. Available from: https://www. hindustantimes.com/india-news/coronavirus-update-covid-19-rapid-testing-kits-use-suspended-for-two-days-due-to-errors/story-iUw9gw1CL2KL5BwmApQ5sN.html .
- 15.Containment Plan for Large Outbreaks: Novel Coronavirus Disease 2019 (COVID-19). Ministry of Health and Family Welfare Government of India. [Last accessed on 2020 May 12]. Available from: https://www.mohfw.gov.in/pdf/3ContainmentPlanforLargeOutbreaksofCOVID19Final.pdf .
- 16.Ribal MJ, Cornford P, Briganti A, Knoll T, Gravas S, Babjuk M, et al. European Association of Urology Guidelines Office Rapid Reaction Group: An Organization-Wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. Eur Urol. Apr 27; doi: 10.1016/j.eururo.2020.04.056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kumar A. Corona Virus Disease USI Information Centre. [Last accessed on 2020 May 12]. Available from: https://usi.org.in/New/Spe_pdf/USI%20Corona%20advise%20edited.pdf .
- 18.Telemedicine Practice Guidelines Enabling Registered Medical Practitioners to Provide Healthcare Using Telemedicine. [Last accessed on 2020 May 12]. Available from: https://www.mohfw.gov.in/pdf/Tele medicine.pdf .
- 19.Proietti S, Gaboardi F, Giusti G. Endourological stone management in the Era of the COVID-19. Eur Urol. 2020 Apr 14; doi: 10.1016/j.eururo.2020.03.042. S0302-2838(20)30217-7. doi: 10.1016/j.eururo.2020.03.042. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wu Y, Xu X, Chen Z, Duan J, Hashimoto K, Yang L, et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav Immun. 2020 Mar 30; doi: 10.1016/j.bbi.2020.03.031. S0889-1591(20)30357-3 pii: S0889-1591(20)30357-3. [doi: 10.1016/j.bbi.2020.03.031] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zhong Q, Liu YY, Luo Q, Zou YF, Jiang HX, Li H, et al. Spinal anaesthesia for patients with coronavirus disease 2019 and possible transmission rates in anaesthetists: Retrospective, single-centre, observational cohort study. Br J Anaesth. 2020;124(6):670. doi: 10.1016/j.bja.2020.03.007. pii: S0007-0912(20)30161-6. [doi: 10.1016/j.bja.2020.03.007] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Peng PWH, Ho PL, Hota SS. Outbreak of a new coronavirus: What anaesthetists should know. Br J Anaesth. 2020;124:497–501. doi: 10.1016/j.bja.2020.02.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ling Y, Xu SB, Lin YX, Tian D, Zhu ZQ, Dai FH, et al. Persistence and clearance of viral RNA in 2019 novel coronavirus disease rehabilitation patients. Chin Med J (Engl) 2020;133:1039–43. doi: 10.1097/CM9.0000000000000774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Panagoda PI, Vasdev N, Gowrie-Mohan S. Avoiding the obturator jerk during TURBT. Curr Urol. 2018;12:1–5. doi: 10.1159/000447223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bosio A, Dalmasso E, Alessandria E, Agosti S, Pizzuto G, Peretti D, et al. Retrograde intra-renal surgery under spinal anesthesia: The first large series. Minerva Urol Nefrol. 2018;70:333–9. doi: 10.23736/S0393-2249.18.02926-0. [DOI] [PubMed] [Google Scholar]
- 26.Zeng G, Zhao Z, Yang F, Zhong W, Wu W, Chen W. Retrograde intrarenal surgery with combined spinal-epidural vs. general anesthesia: A prospective randomized controlled trial. J Endourol. 2015;29:401–5. doi: 10.1089/end.2014.0249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Çakici MÇ, Özok HU, Erol D, Çatalca S, Sari S, Özdemir H, et al. Comparison of general anesthesia and combined spinal-epidural anesthesia for retrograde intrarenal surgery: A prospective randomized trial in one center. Minerva. Urol Nefrol. 2019;71:636–43. doi: 10.23736/S0393-2249.19.03481-7. [DOI] [PubMed] [Google Scholar]
- 28.Pu C, Wang J, Tang Y, Yuan H, Li J, Bai Y, et al. The efficacy and safety of percutaneous nephrolithotomy under general versus regional anesthesia: A systematic review and meta-analysis. Urolithiasis. 2015;43:455–66. doi: 10.1007/s00240-015-0776-2. [DOI] [PubMed] [Google Scholar]
- 29.Yeo D, Yeo C, Kaushal S, Tan G. COVID-19 and the general surgical department–measures to reduce spread of SARS-COV-2 among surgeons. Ann Surg. 2020 doi: 10.1097/SLA.0000000000003957. [Apr 13;10.1097/SLA.0000000000003957. doi: 10.1097/SLA.0000000000003957. Online ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Vigneswaran Y, Prachand VN, Posner MC, Matthews JB, Hussain M. What is the appropriate use of laparoscopy over open procedures in the current COVID-19 climate? J Gastrointest Surg. 2020 Apr 13;1 doi: 10.1007/s11605-020-04592-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mallick R, Odejinmi F, Clark TJ. Covid 19 pandemic and gynaecological laparoscopic surgery: Knowns and unknowns. Facts Views Vis Obgyn. 2020;12:3–7. [PMC free article] [PubMed] [Google Scholar]
- 32.Morris SN, Fader AN, Milad MP, Dionisi HJ. Understanding the “scope” of the problem: Why laparoscopy is considered safe during the COVID-19 pandemic. J Minim Invasive Gynecol. 2020;27:789–91. doi: 10.1016/j.jmig.2020.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Updated Intercollegiate General Surgery Guidance on COVID-19. [Last accessed on 2020 May 12]. Available rom: https://www.rcseng.ac.uk/coronavirus/joint-guidancefor-surgeons-v2/
- 34.Mottrie A. ERUS (EAU Robotic Urology Section) Guidelines During COVID-19 Emergency. [Last accessed on 2020 May 12]. Available from: https://uroweb.org/wp-content/uploads/ERUS-guidelines-for-COVID-def.pdf .
- 35.Friedrich-Freksa M, Schulz E, Nitzke T, Wenzel O, Popken G. Performing radical cystectomy and urinary diversion in regional anesthesia: Potential risk reduction in the treatment of bladder cancer. Urol Int. 2013;91:103–8. doi: 10.1159/000348542. [DOI] [PubMed] [Google Scholar]
- 36.Kofler O, Prueckner S, Weninger E, Tomasi R, Karl A, Niedermayer S, et al. Anesthesia for open radical retropubic prostatectomy: A comparison between combined spinal epidural anesthesia and combined general epidural anesthesia. Prostate Cancer. 2019;2019:4921620. doi: 10.1155/2019/4921620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nakano M, Matsuzaki M, Narita S, Watanabe J, Morikawa H, Murata H, et al. Comparison of radical retropubic prostatectomy under combined lumbar spinal and epidural anesthesia with that under combined general and epidural anesthesia. Nihon Hinyokika Gakkai Zasshi. 2005;96:11–6. doi: 10.5980/jpnjurol1989.96.11. [DOI] [PubMed] [Google Scholar]
- 38.Sharma G, Sharma S, Parmar K. Buccal mucosa or penile skin for substitution urethroplasty: A systematic review and meta-analysis. Indian J Urol. 2020;36:81–8. doi: 10.4103/iju.IJU_298_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Parmar K, Tyagi S, Singh SK, Kumar S, Mete U, Mohan R, et al. Comparative analysis of successful outcome after substitution urethroplasty with “Buccal Mucosa Graft versus Inner Preputial Skin Graft” for anterior urethral stricture disease. European Urology Supplements. 2019;18(1):e524. [Google Scholar]
- 40.World Health Organization. Novel Coronavirus (2019-nCoV) Technical Guidance: Infection Prevention and Control. [Last accessed on 2020 May 17]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/infection-prevention-and-control .