

Abstract
We present a case of paroxysmal atrioventricular block with atrial pacemaker shift, focusing on the change of P‐wave morphology.

Keywords: atrial pacemaker shift, paroxysmal atrioventricular block, P‐wave morphology, ventricular arrest
Dear Editor,
We would like to share a case of paroxysmal atrioventricular block (AVB) which is unique in that the tachycardia‐dependent paroxysmal AVB and the rate‐dependent atrial pacemaker shift occurred simultaneously.
A Japanese woman in her 40s had a history of symptomatic epilepsy that may have developed after she contracted viral encephalitis in 2001. The patient's advanced atrioventricular block was first documented in 2014. Since she was asymptomatic, we closely monitored her electrocardiogram (ECG) and found that her cardiac rhythm was changing to advanced AVB paroxysmally. An electrophysiological study revealed the findings of organic A‐H block but no other specific findings suggesting an intra/infra‐hisian block. Since the patient refused to undergo the implantation of a cardiac pacemaker, follow‐up examinations at our outpatient clinic were performed periodically.
In 2018, she experienced syncope and fell backward while walking and was admitted to our hospital once again. She was taking levetiracetam and gabapentin prescribed for symptomatic epilepsy, but had no other past medical history. Laboratory testing and imaging examination on her admission showed no specific extraordinary findings. A 12‐lead ECG revealed AV dissociation with a junctional escape rhythm of 40 bpm with sharp P‐waves in leads II, III, and aVF (Figure 1A). Despite these ECG findings, the patient was asymptomatic and we could not completely deny the involvement of the epilepsy. On another occasion, the patient's ECG showed 1:1 AV conduction and presumed sinus rhythm with dull P‐waves in leads II, III, and aVF (Figure 1B). On the second day of her admission, she experienced a syncopal episode. The telemetry ECG at this episode (Figure 2A) revealed complete AVB with 18.3 seconds of ventricular arrest, accompanied by an accelerating atrial rate. An atrial pacemaker shift was observed during the ventricular pause. A cardiac pacemaker was implanted on day 3.
FIGURE 1.
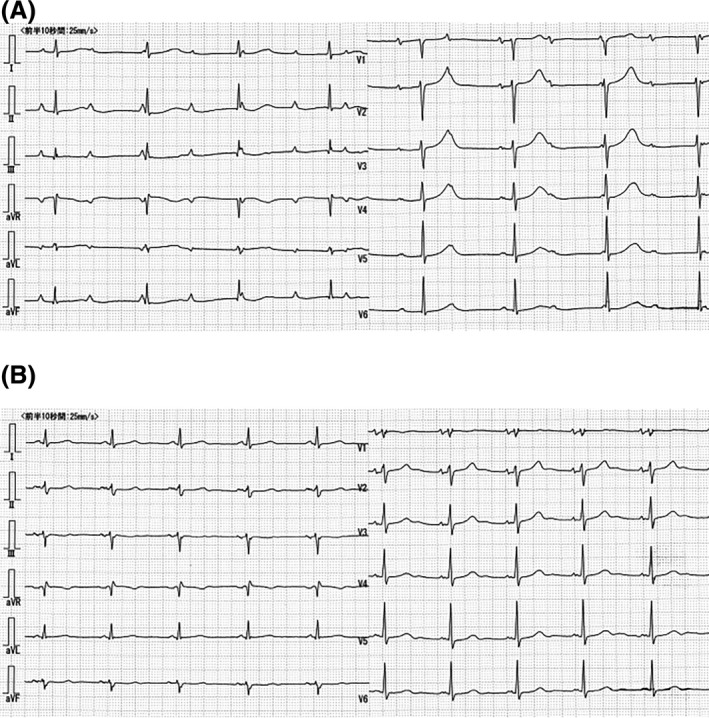
(A) Complete atrioventricular block (AVB) with a junctional escape rhythm of 40 bpm with P‐P intervals between 720 and 780 msec. Sharp P‐waves in leads II, III, and aVF were observed. (B) During 1:1 AV conduction (a presumed sinus rhythm), the P‐P intervals were between 960 and 1000 msec with dull P‐waves in leads II, III, and aVF
FIGURE 2.
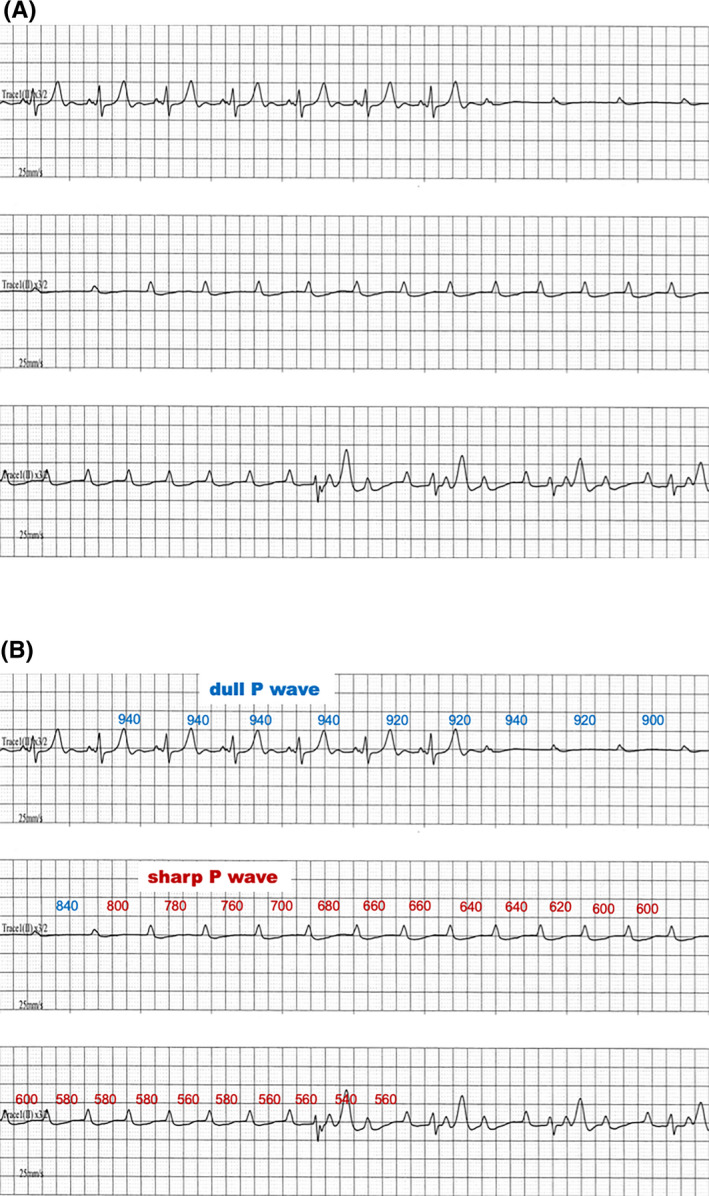
(A) The ECG monitoring at the syncopal episode on the second hospital day. (B) The P‐P intervals on the same ECG recording as that shown in panel A
Several groups have reported cases of paroxysmal AVB 1 , 2 , 3 , but the precise cause(s) and underlying mechanisms of paroxysmal AVB remain unclear in some of the cases. In our patient's case, paroxysmal AVB occurred with an accelerated atrial rate; that is, the so called "tachycardia‐dependent AVB". 2 In addition, PR prolongation just before paroxysmal AVB was not observed in our patient, and sinus acceleration during ventricular asystole were recognized. These findings are strongly suggestive of intrinsic conduction disease. 1 , 2 , 4
Although an atrial pacemaker shift is well‐known phenomenon, to the best of our knowledge there are no other case reports focusing on the change of P‐wave morphology during paroxysmal AVB. In our patient's case, telemetry ECG revealed that the morphology of the P‐waves before and after the pacemaker shift changed from dull to sharp (Figure 2A). Compared to the patient's 12‐lead ECG findings (Figure 1A,B), the morphologies shown by the telemetry ECG were similar to the waves of lead II. When the patient was on the resumed sinus rhythm, the morphology of the P‐wave in lead II (Figure 1B) was similar to the dull P‐wave on the telemetry ECG (Figure 2A). However, when the patient's 12‐lead ECG showed complete AVB in the past records (Figure 1A), the P‐wave in lead II was almost same morphology as the sharp P‐wave on the telemetry ECG (Figure 2A). Judging from a previous report about P‐wave morphology, the origin of the sharp P‐waves is most likely to be high cristae terminalis. 5 Figure 2B presents the P‐P intervals of both P‐waves on the same ECG recording as that shown in Figure 2A, and it reveals that the AVB occurred with slight P‐P shortening. In addition, the atrial pacemaker shift, from the dull P‐wave to the sharp P‐wave, occurred between 800 and 840 milliseconds (Figure 2B). The range of P‐P intervals of both P‐waves were clearly separated with some overlaps: 780‐1000 milliseconds in the dull P‐waves and 540‐800 milliseconds in the sharp P‐waves. We therefore suspect that the decrease in cardiac output resulting from the AVB and ventricular arrest accelerated the tonus of the sympathetic nerves, resulting in a shortened P‐P interval and inducing the pacemaker shift from the sinus node to the high cristae terminalis. An atrial pacemaker shift may have some involvement in occurrence of AVB.
DISCLOSURE STATEMENT
The authors have no conflict of interest to disclose.
REFERENCES
- 1. Shenasa M, Josephson ME, Wit AL. Paroxysmal atrioventricular block: electrophysiological mechanism of phase 4 conduction block in the His‐Purkinje system: a comparison with phase 3 block. Pacing Clin Electrophysiol. 2017;40:1234–41. [DOI] [PubMed] [Google Scholar]
- 2. Alboni P, Holz A, Brignole M. Vagally mediated atrioventricular block: pathophysiology and diagnosis. Heart. 2013;99:904–8. [DOI] [PubMed] [Google Scholar]
- 3. Aste M, Brignole M. Syncope and paroxysmal atrioventricular block. J Arrhythm. 2017;33:562–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Komatsu S, Sumiyoshi M, Miura S, Kimura Y, Shiozawa T, Hirano K, et al. A proposal of clinical ECG index “vagal score” for determining the mechanism of paroxysmal atrioventricular block. J Arrhythm. 2017;33:208–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kistler PM, Roberts‐Thomson KC, Haqqani HM, Fynn SP, Singarayar S, Vohra JK, et al. P‐wave morphology in focal atrial tachycardia: development of an algorithm to predict the anatomic site of origin. J Am Coll Cardiol. 2006;48:1010–7. [DOI] [PubMed] [Google Scholar]