

Abstract
Cardioneuroablation is an emerging therapy to treat vasovagal syncope, functional atrioventricular block and sinus dysfunction. Currently, there are several effective approaches due to the complex modulation of autonomic nervous system. In this review, we describe techniques of this innovative therapy based on published literature and our experiences.
Keywords: Cardioneuroablation, Ganglionated Plexus, Catheter Ablation, Vasovagal Syncope, Sinus Dysfunction, Atrioventricular Block
Introduction
The autonomic nervous system affects the physiological function of cardiovascular system.1,2 Tonic activation of the vagus may result in hypotension, bradycardia, and potentially vasovagal syncope (VVS).2-5 Ganglionated plexi (GPs), intrinsic structures located in the epicardial atrial fat pads, connect preganglionic and postganglionic nerve fibers to affect heart rate, atrial and ventricular refractoriness and cardiac function. The GPs are selected as the primary targets for cardioneuroablation because of their physiological function and their anatomical location that can be targeted easily by ablation catheter.6-8
Although cardioneuroablation has been applied to treat VVS, functional atrioventricular block and sinus dysfunction for more than fifteen years, significant progress has been made in the last few years. There are different ablation strategies and approaches to localize and ablate GPs.9-22 This review is dedicated to summarize available techniques of this therapy.
Targets of Cardioneuroablation
Previous studies have found that, there are seven major GPs located in protuberances and/or grooves of the heart wall, such as interatrial tissues, connective folding tissues between atrium and pulmonary veins, tissues adjacent to coronary arteries, and interventricular tissues. Since the atria are much thinner than the ventricles, radiofrequency energy can be transmitted more easily to the GPs via the atria,23,24 and thus effective autonomic denervation can be achieved via the endocardial approach in the atria.
Although there are different targeting approaches and ablation strategies, the GPs in left atrium (LA) and/or right atrium (RA) are mostly targeted. Pachon et al 9-11 performed comprehensive GPs ablation from both RA and LA via spectral mapping-guided ablation and additional anatomical-guided ablation to treat VVS, functional AV block and sinus dysfunction. Aksu et al 15,22,25,26 simplified the strategy choosing major GPs via RA and LA as primary targets; and they achieved successful results. Zhao and Qin just performed anatomic GPs ablation in both LA and RA to treat symptomatic sinus bradycardia.13,18 Contrary to these bi-atrial ablation methods, different groups investigated the potential role of LA or RA only approaches. Our team defined a new technique via catheter ablation of GPs only in the LA on the basis of linear ablation of atrial fibrillation in which the vagal reflex was frequently observed.12,14,21 Debruyne et al 20 performed unifocal right-sided ablation targeted in the posteroseptal side of the junction between the RA and the superior vena cava (SVC) to treat VVS and functional sinus node dysfunction.
Due to the complex intermodulation between GPs, it is necessary to select the essential GPs as primary ablation targets while avoiding the potential adverse effects caused by excessive ablation. Chiou et al 27 demonstrated that, most of the vagal fibers to the atria sinus and atrioventricular nodes travel through a fat pad located on the right pulmonary artery between SVC and aortic root (SVCaorta fat pad), which was proposed to be the “head station” between the extrinsic and the intrinsic cardiac autonomic nervous system. Debruyne et al 20 directly targeted this special GP site via RA during cardioneuroablation. In previous research, our team retrospectively analyzed the processes of cardioneuroablation in 115 VVS patients. Four targeted GPs located in the connective tissues between atrium and pulmonary veins Figure 1, were ablated as order of the left superior GP (LSGP) –the left inferior GP (LIGP) –the right inferior GP (RIGP) –the right anterior GP (RAGP). Among the above ablated GPs, we observed a unique phenomenon that ablation of RAGP would immediately increase heart rate within few seconds and maintain this effect long-term, while there were just vagal responses observed during ablation of other GPs.21 Supporting this observation, Aksu et al 28 demonstrated that cardioneuroablation, starting from the RAGP, results in significant decrease of positive vagal response ratio during radiofrequency application on the left superior GP in a retrospective study. These experiences may indicate that, RAGP would be the most important target for cardioneuroablation. However, there has been no comparison study between RSGP ablation only and ablation of all LAGPs. So, we still cannot argue whether an approach targeting RSGP only will be enough in all cases. Further study is needed to clarify the exquisite regulatory mechanism of GPs.
Figure 1. The 3-dimensional endocardial surface of the left atrium, right atrium, and locations of ganglionated plexi.

The blue points represent the locations of ganglionated plexi (GPs). LSGP: left superior ganglionated plexus; LIGP: left inferior ganglionated plexus; RAGP: right anterior ganglionated plexus; RIGP: right inferior ganglionated plexus.
Approaches to Identify Ganglionated Plexi
The most difficult step for the cardioneuroablation procedure is to identify GPs. An anatomically guided approach is the basic method; few electrophysiologists use this simple way to perform GPs ablation.13,18,20 The location of GPs can be marked according to the routine anatomical sites in the 3-dimensional electroanatomic mapping of the RA and LA Figure 1. Debruyne et al 20 further applied both computed tomographic scan and electroanatomic mapping to localize the GPs sites.
Because of the individual variability of GP sites, it is not enough to use anatomical guidance alone. Currently, the commonly used identification approaches include high-frequency stimulation (HFS) and spectral guided method.9,11,12,14,15,21,22 The HFS was initially designed to identify GPs location during circumferential pulmonary vein isolation for atrial fibrillation.29In this technique, HFS with frequency of 20 Hz, voltage of 10–20 V, and pulse duration of 5 ms is delivered to each GP site. During HFS, existence of positive vagal response defining as transient ventricular asystole, atrioventricular block, or R-R interval increased by 50% demonstrates vagal innervation sites Figure 2. The main limitation of this method is inadvertent induction of atrial fibrillation. To avoid induction of atrial fibrillation, programmed HFS during atrial refractory period (10-20 ms followed initial designed atrial stimulation) and with duration of 3-5 seconds might be used.14,21 Even in case of induced atrial fibrillation, mean R-R interval increase of >50% could also be used to evaluate positive vagal response.30
Figure 2. Vagal response to high frequency stimulation.

During high frequency stimulation on the left superior ganglionated plexus site, a significant prolongation on RR interval is seen in surface ECG and intracardiac electrograms
Spectral guided method was first introduced by Pachon et al 9 to identify GPs location. The atrial myocardium was divided into a compact schema with normal working atrial myocardium and a fibrillar schema with neural fiber interposition. The anatomic locations of GPs with penetration of the nervous fibers changed myocardial conduction and the frequency spectrum of the endocardial potential which shifts from the compact conduction pattern to the fibrillar. Thus, while the compact atrial myocardium presents a homogeneous spectrum with one main frequency around 40 Hz and uniform conduction resulting from a mass of well-connected cells, fibrillar myocardium containing neural fiber interposition demonstrates a heterogeneous and fractionated spectrum with frequencies higher than 100 Hz. The limitation of spectral guided method is that, special pre-amplifier and spectral analysis software cannot be obtained by all electrophysiological labors.
Aksu et al15,22 further simplified this method by targeting the fractionated electrograms in the routine anatomical GPs locations. In their study, bipolar endocardial atrial electrograms were evaluated for amplitude and number of deflections at filter settings of 200–500 Hz and a sweep speed of 200 mm/s. Amplitude was defined as the voltage difference between highest and lowest deflections of each electrogram. Number of deflections was determined by counting the number of turning points (positive to negative direction or vice versa) in each electrogram. Electrograms were divided into: (1) normal atrial electrogram, which demonstrates deflection number of less than 4; (2) low-amplitude fractionated electrogram, which demonstrates greater or equal to four deflections and amplitude of less than 0.7 mV; and (3) high-amplitude fractionated electrogram, which demonstrates greater or equal to four deflections and an amplitude greater or equal to 0.7mV. The sites demonstrating lowamplitude and high-amplitude fractionated electrogram pattern in a region that is consistent with probable localization of GPs on LA were targeted Figure 3.15,22 The main advantage of this technique is that, it can be performed with conventional electrophysiological equipment by changing filter settings of device.
Figure 3. Low-amplitude and high-amplitude fractionated electrograms are seen during electroanatomic mapping guided cardioneuroablation.
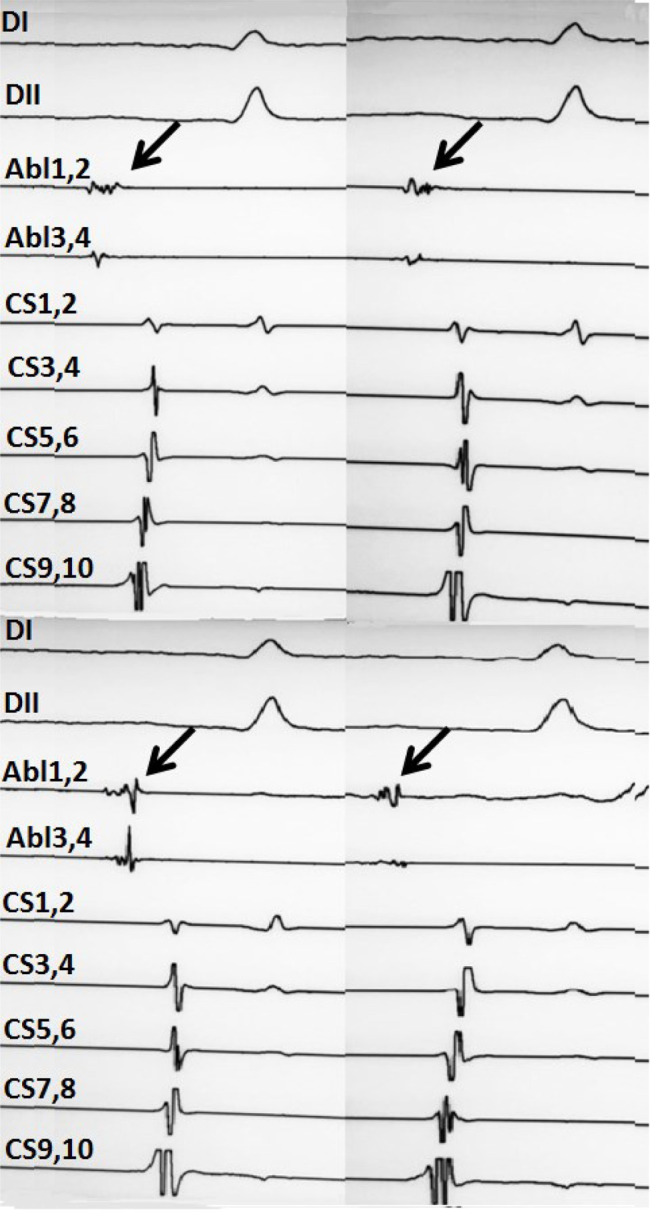
The arrows in above indicate low amplitude fragmanted electrogram and the arrows in below show high amplitude fragmanted electrograms, respectively. This figure provided by Dr Tolga Aksu from University of Health Sciences, Kocaeli Derince Training and Research Hospital, Kocaeli, Turkey
Ablation of Ganglionated Plexi
It is worthy of note that, all of these approaches were performed with 3D navigation systems (Ensite™ system by Abbott or CARTO™ system by Biosense Webster). Irrigated and non-irrigated catheters were used for cardioneuroablation in previous clinical studies. In the earliest published literature, Pachon et al 9 applied 4 mm nonirrigated catheter with the thermo-controlled system. The upper limit of power was set to 30 W. Radiofrequency energy were delivered in the targets near the pulmonary veins with maximum temperature of 600C and deliver time of 15 s, while delivered in other points with maximum temperature of 700C and deliver time of 30 s. With the development of technique, they chose two ablation models in further researches; the thermo-controlled radiofrequency was applied limited to 50 W/600C (non-irrigated) and 30 W/450C (irrigated) respectively.11 In previous studies, our team used non-irrigated catheters with limitation set of 60 W/60°C and delivered at least 30 s until inhibition of the VR in each GP.12,14 Considering of the efficiency and safety of procedure, we tried to reduce the maximum temperature to 40 W and converted to the application of irrigated catheter (40 W/430C, irrigation flow of 17 mL/min). According to the experience of our team, a bi-directional catheter would be a better choice to guarantee optimal tissue contact essential factor to create transmural injury.31 Aksu et al 15,25,32 consistently used irrigated catheter with power limit of 35 W, maximum temperature of 430C, and irrigation flow of 18 mL/min in their studies. Debruyne et al 20 furtherly chose contact force sensing catheter using a power of 40 W and a contact force > 8 g to ensure the ablation lesion.
During ablation of GPs, the most common response of each GP site is a vagal response such as transient ventricular asystole, atrioventricular block, or an increase of R-R interval. According to our previous research, among all the GPs ablated via LA, LSGP was the most frequent site demonstrating positive vagal response, while RAGP is the only target with heart rate increase during radiofrequency energy delivery.14,21
The long-term clinical outcome of cardioneuroablation may be affected by incomplete ablation and consequent reinnervation by non-elimination of intramural parasympathetic postganglionic neurons. Repeat endocardial or epicardial pathway ablation may solve this problem in the future.
Endpoints of Cardioneuroablation
The simplest endpoint of cardioneuroablation is elimination of positive vagal response during ablation. Unfortunately, it is often difficult to evaluate the residual function of GPs by this rough method. Other endpoints usually depend on the approaches of GPs identification. We believe that the RAGP may need a different endpoint due to the unique response in most cases during the ablation, which often result in a rapid rise of sinus rhythm. In our lab, after completion of GP ablation, HFS is applied to recheck the vagal response status of each GP. In case of ongoing vagal response in any GP site, further ablation is performed up to complete elimination.12,14,21 With this endpoint, we obtained excellent long-term clinical outcomes.12,14,21 However, HFS may not necessarily predict longterm effects of cardioneuroablation; a negative HFS response after RF may be caused by the thermal effect of radiofrequency ablation.
Aksu et al 15,22 performed electroanatomic mapping guided cardioneuroablation, the primary endpoints of their procedure is near complete elimination of all targeted fragmented electrograms, and elimination of positive vagal response during ablation. They also applied atropine 30 minutes after cardioneuroablation to detect an acute anticholinergic response. Achievement of 75% of final sinus rate detected before procedure was accepted as clinical endpoint in patients with VVS and sinus node dysfunction. Decrease of >25% in PR interval was accepted as clinical endpoint for patients with atrioventricular block.28,32 Pachon et al 33 invented a neurostimulator to directly stimulate the vagal trunks during procedure and achieved stepwise strict control of the vagal denervation grade. The extracardiac vagal stimulation would be a reasonable technique to assess the endpoint of cardioneuroablation in the future.
In the end, we summarized the techniques of cardioneuroablation including locations of targeted GPs, approaches to identify GPs, ablation catheters, and main procedural endpoints from published clinical researches (case reports excluded) in Table 1.
Table 1. Techniques for cardioneuroablation in published clinical researches.
NMS: neurally mediated syncope; AVB: atrioventricular block; SND: sinus node dysfunction; RA: right atrium; LA: left atrium; SA: spectral analysis; AA: anatomical approach; VVS: vasovagal syncope; HFS: high-frequency stimulation; VR: vagal response; VRAF: vagal-related atrial fibrillation; NG: not given; SB: sinus bradycardia.
# Only patients in denervation group were included in the evaluation.
| Study | Enrolled patients | Included diseases | locations of targeted GPs | Approaches to identify GPs | Ablation catheter | Main endpoints |
|---|---|---|---|---|---|---|
| Pachon, et al.9 2005 | 21 | NMS, AVB, SND | RA, LA | SA, AA | Non-irrigated | Elimination of the potentials according to SA; Persistent increase in the sinus rate and Wenckebach point. |
| Pachon, et al.11 2011 | 43 | NMS | RA, LA | SA, AA | Non-irrigated, Irrigated | Elimination of the potentials according to SA; Atropine test. |
| Yao, et al.12 2012 | 10 | VVS | LA | HFS | Non-irrigated | Elimination of the VR during ablation. |
| Pachon, et al.33 2015 | 47# | VRAF, NMS | NG | SA, AA | NG | Vagal stimulation; Atropine test. |
| Zhao, et al.13 2015 | 11 | symptomatic SB | RA, LA | HFS, AA | Irrigated | Elimination of the VR during ablation; HFS after ablation. |
| Sun, et al.14 2016 | 57 | VVS | LA | HFS, AA | Non-irrigated | Elimination of the VR during ablation; HFS after ablation. |
| Aksu, et al.15 2016 | 22 | NMS, AVB, SND | RA, LA | SA, HFS, AA | Irrigated | Elimination of fractionated potentials; Elimination of parasympathetic response to HFS; Persistent increase in the sinus rate AND Wenckebach point; Completely elimination of AV block. |
| Qin, et al.18 2017 | 62 | symptomatic SB | RA, LA | AA | Irrigated | Ablation of atrial electrical activity (peak-to-peak bipolar electrogram <0.1 mV); Elimination of the VR during ablation. |
| Rivarola et al.19 2017 | 14 | NMS, AVB, SND | RA, LA | AA | Irrigated | The R-R interval, Wenckebach cycle length, and AH interval shortening, associated with a negative response to atropine. |
| Debruyne et al.20 2018 | 20 | NMS, SND | RA | AA | Irrigated | P-P interval was < 70% of the baseline procedural P-P interval, was <600 ms after 5 minutes of waiting time; Atropine test. |
| Aksu, et al.22 2019 | 20 | VVS | RA, LA | SA, HFS, AA | Irrigated | Near complete elimination of all targeted atrial electrograms; Elimination of positive VR to ablation; Elimination of positive VR to HFS. |
| Hu et al.21 2019 | 115 | VVS | LA | HFS, AA | Non-irrigated | Elimination of the VR during ablation; HFS after ablation. |
| Aksu, et al.28 2019 | 49 | VVS, AVB, SND | RA, LA | SA, HFS, AA | Irrigated | Near complete elimination of all targeted atrial electrograms; Atropine test; Achievement of 75% of final sinus rate detected before procedure in patients with VVS and SND; Decrease > 25% in PR interval in patients with AVB. |
| Aksu, et al.32 2020 | 65 | VVS, AVB, SND | RA+LA vs.RA | SA, HFS, AA | Irrigated | Near complete elimination of all targeted atrial electrograms; Atropine test; Achievement of 75% of final sinus rate detected before procedure in patients with VVS and SND; Decrease > 25% in PR interval in patients with AVB. |
Conclusions
Cardioneuroablation is an emerging and apparently promising therapy. A few clinical trials have revealed the efficiency of this innovative strategy for VVS and autonomic related bradycardias. However, there are still many underlying questions need to be answered by more controlled clinical trials, which may also change the guidelines for the treatment of syncope and arrhythmia in the future.
References
- 1.Goldberger Jeffrey J, Arora Rishi, Buckley Una, Shivkumar Kalyanam. Autonomic Nervous System Dysfunction: JACC Focus Seminar. J. Am. Coll. Cardiol. 2019 Mar 19;73 (10):1189–1206. doi: 10.1016/j.jacc.2018.12.064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Baschieri Francesca, Cortelli Pietro. Circadian rhythms of cardiovascular autonomic function: Physiology and clinical implications in neurodegenerative diseases. Auton Neurosci. 2019 Mar;217 ():91–101. doi: 10.1016/j.autneu.2019.01.009. [DOI] [PubMed] [Google Scholar]
- 3.Jardine D L. Vasovagal syncope: new physiologic insights. Cardiol Clin. 2013 Feb;31 (1):75–87. doi: 10.1016/j.ccl.2012.10.010. [DOI] [PubMed] [Google Scholar]
- 4.Alboni Paolo, Holz Anna, Brignole Michele. Vagally mediated atrioventricular block: pathophysiology and diagnosis. Heart. 2013 Jul;99 (13):904–8. doi: 10.1136/heartjnl-2012-303220. [DOI] [PubMed] [Google Scholar]
- 5.Sheldon Robert S, Grubb Blair P, Olshansky Brian, Shen Win-Kuang, Calkins Hugh, Brignole Michele, Raj Satish R, Krahn Andrew D, Morillo Carlos A, Stewart Julian M, Sutton Richard, Sandroni Paola, Friday Karen J, Hachul Denise Tessariol, Cohen Mitchell I, Lau Dennis H, Mayuga Kenneth A, Moak Jeffrey P, Sandhu Roopinder K, Kanjwal Khalil. 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015 Jun;12 (6):e41–63. doi: 10.1016/j.hrthm.2015.03.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hou Yinglong, Scherlag Benjamin J, Lin Jiaxiong, Zhang Ying, Lu Zhibing, Truong Kim, Patterson Eugene, Lazzara Ralph, Jackman Warren M, Po Sunny S. Ganglionated plexi modulate extrinsic cardiac autonomic nerve input: effects on sinus rate, atrioventricular conduction, refractoriness, and inducibility of atrial fibrillation. J. Am. Coll. Cardiol. 2007 Jul 03;50 (1):61–8. doi: 10.1016/j.jacc.2007.02.066. [DOI] [PubMed] [Google Scholar]
- 7.Hou Yinglong, Scherlag Benjamin J, Lin Jiaxiong, Zhou Jing, Song Jianguo, Zhang Ying, Patterson Eugene, Lazzara Ralph, Jackman Warren M, Po Sunny S. Interactive atrial neural network: Determining the connections between ganglionated plexi. Heart Rhythm. 2007 Jan;4 (1):56–63. doi: 10.1016/j.hrthm.2006.09.020. [DOI] [PubMed] [Google Scholar]
- 8.Hou Yuemei, Zhou Qina, Po Sunny S. Neuromodulation for cardiac arrhythmia. Heart Rhythm. 2016 Feb;13 (2):584–92. doi: 10.1016/j.hrthm.2015.10.001. [DOI] [PubMed] [Google Scholar]
- 9.Pachon Jose C, Pachon Enrique I, Pachon Juan C, Lobo Tasso J, Pachon Maria Z, Vargas Remy N A, Jatene Adib D. "Cardioneuroablation"--new treatment for neurocardiogenic syncope, functional AV block and sinus dysfunction using catheter RF-ablation. Europace. 2005 Jan;7 (1):1–13. doi: 10.1016/j.eupc.2004.10.003. [DOI] [PubMed] [Google Scholar]
- 10.Pachon M Jose C, Pachon M Enrique I, Lobo Tasso J, Pachon M Juan C, Pachon M Zelia C, Vargas Remy N A, Manrique Ricardo M, Jatene Adib D. Syncopal high-degree AV block treated with catheter RF ablation without pacemaker implantation. Pacing Clin Electrophysiol. 2006 Mar;29 (3):318–22. doi: 10.1111/j.1540-8159.2006.00340.x. [DOI] [PubMed] [Google Scholar]
- 11.Pachon Jose Carlos M, Pachon Enrique Indalecio M, Cunha Pachon Maria Zelia, Lobo Tasso Julio, Pachon Juan Carlos M, Santillana Tomas Guilhermo P. Catheter ablation of severe neurally meditated reflex (neurocardiogenic or vasovagal) syncope: cardioneuroablation long-term results. Europace. 2011 Sep;13 (9):1231–42. doi: 10.1093/europace/eur163. [DOI] [PubMed] [Google Scholar]
- 12.Yao Yan, Shi Rui, Wong Tom, Zheng Lihui, Chen Wensheng, Yang Long, Huang Wen, Bao Jingru, Zhang Shu. Endocardial autonomic denervation of the left atrium to treat vasovagal syncope: an early experience in humans. Circ Arrhythm Electrophysiol. 2012 Apr;5 (2):279–86. doi: 10.1161/CIRCEP.111.966465. [DOI] [PubMed] [Google Scholar]
- 13.Zhao Liang, Jiang Weifeng, Zhou Li, Wang Yuanlong, Zhang Xiaodong, Wu Shaohui, Xu Kai, Liu Xu. Atrial autonomic denervation for the treatment of long-standing symptomatic sinus bradycardia in non-elderly patients. J Interv Card Electrophysiol. 2015 Aug;43 (2):151–9. doi: 10.1007/s10840-015-9981-8. [DOI] [PubMed] [Google Scholar]
- 14.Sun Wei, Zheng Lihui, Qiao Yu, Shi Rui, Hou Bingbo, Wu Lingmin, Guo Jinrui, Zhang Shu, Yao Yan. Catheter Ablation as a Treatment for Vasovagal Syncope: Long-Term Outcome of Endocardial Autonomic Modification of the Left Atrium. J Am Heart Assoc. 2016 Jul 08;5 (7) doi: 10.1161/JAHA.116.003471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Aksu Tolga, Golcuk Ebru, Yalin Kivanç, Guler Tümer Erdem, Erden Ismail. Simplified Cardioneuroablation in the Treatment of Reflex Syncope, Functional AV Block, and Sinus Node Dysfunction. Pacing Clin Electrophysiol. 2016 Jan;39 (1):42–53. doi: 10.1111/pace.12756. [DOI] [PubMed] [Google Scholar]
- 16.Rivarola Esteban, Hardy Carina, Sosa Eduardo, Hachul Denise, Furlan Valter, Raimundi Fabrizio, Scanavacca Mauricio. Selective atrial vagal denervation guided by spectral mapping to treat advanced atrioventricular block. Europace. 2016 Mar;18 (3):445–9. doi: 10.1093/europace/euv142. [DOI] [PubMed] [Google Scholar]
- 17.Fukunaga Masato, Wichterle Dan, Peichl Petr, Aldhoon Bashar, Čihák Robert, Kautzner Josef. Differential effect of ganglionic plexi ablation in a patient with neurally mediated syncope and intermittent atrioventricular block. Europace. 2017 Jan;19 (1):119–126. doi: 10.1093/europace/euw100. [DOI] [PubMed] [Google Scholar]
- 18.Qin Mu, Zhang Yu, Liu Xu, Jiang Wei-Feng, Wu Shao-Hui, Po Sunny. Atrial Ganglionated Plexus Modification: A Novel Approach to Treat Symptomatic Sinus Bradycardia. JACC Clin Electrophysiol. 2017 Sep;3 (9):950–959. doi: 10.1016/j.jacep.2017.01.022. [DOI] [PubMed] [Google Scholar]
- 19.Rivarola Esteban W, Hachul Denise, Wu Tan, Pisani Cristiano, Hardy Carina, Raimundi Fabrizio, Melo Sissy, Darrieux Francisco, Scanavacca Mauricio. Targets and End Points in Cardiac Autonomic Denervation Procedures. Circ Arrhythm Electrophysiol. 2017 Feb;10 (2) doi: 10.1161/CIRCEP.116.004638. [DOI] [PubMed] [Google Scholar]
- 20.Debruyne Philippe, Rossenbacker Tom, Collienne Christine, Roosen John, Ector Bavo, Janssens Luc, Charlier Filip, Vankelecom Bart, Dewilde Willem, Wijns William. Unifocal Right-Sided Ablation Treatment for Neurally Mediated Syncope and Functional Sinus Node Dysfunction Under Computed Tomographic Guidance. Circ Arrhythm Electrophysiol. 2018 Sep;11 (9) doi: 10.1161/CIRCEP.118.006604. [DOI] [PubMed] [Google Scholar]
- 21.Hu Feng, Zheng Lihui, Liang Erpeng, Ding Ligang, Wu Lingmin, Chen Gang, Fan Xiaohan, Yao Yan. Right anterior ganglionated plexus: The primary target of cardioneuroablation? Heart Rhythm. 2019 Oct;16 (10):1545–1551. doi: 10.1016/j.hrthm.2019.07.018. [DOI] [PubMed] [Google Scholar]
- 22.Aksu Tolga, Guler Tumer Erdem, Mutluer Ferit Onur, Bozyel Serdar, Golcuk Sukriye Ebru, Yalin Kivanc. Electroanatomic-mapping-guided cardioneuroablation versus combined approach for vasovagal syncope: a cross-sectional observational study. J Interv Card Electrophysiol. 2019 Mar;54 (2):177–188. doi: 10.1007/s10840-018-0421-4. [DOI] [PubMed] [Google Scholar]
- 23.Ho S Y, Sanchez-Quintana D, Cabrera J A, Anderson R H. Anatomy of the left atrium: implications for radiofrequency ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 1999 Nov;10 (11):1525–33. doi: 10.1111/j.1540-8167.1999.tb00211.x. [DOI] [PubMed] [Google Scholar]
- 24.Tan Hong-Wei, Wang Xin-Hua, Shi Hai-Feng, Zhou Li, Gu Jia-Ning, Liu Xu. Left atrial wall thickness: anatomic aspects relevant to catheter ablation of atrial fibrillation. Chin. Med. J. 2012 Jan;125 (1):12–5. [PubMed] [Google Scholar]
- 25.Aksu Tolga, Guler Tumer Erdem, Bozyel Serdar, Yalin Kivanc. Stepwise Approach to the Different Parts of Vasovagal Syncope in a Patient Undergoing Cardioneuro Ablation. Journal of atrial fibrillation. 2018 Feb;10 (5) doi: 10.4022/jafib.1797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Aksu Tolga, Güler Tümer Erdem, Yalın Kıvanç, Bozyel Serdar, Mutluer Ferit Onur. A new and simple technique for vagal ganglia ablation in a patient with functional atrioventricular block: Electroanatomical approach. Turk Kardiyol Dern Ars. 2018 Sep;46 (6):494–500. doi: 10.5543/tkda.2017.15163. [DOI] [PubMed] [Google Scholar]
- 27.Chiou C W, Eble J N, Zipes D P. Efferent vagal innervation of the canine atria and sinus and atrioventricular nodes. The third fat pad. Circulation. 1997 Jun 03;95 (11):2573–84. doi: 10.1161/01.cir.95.11.2573. [DOI] [PubMed] [Google Scholar]
- 28.Aksu Tolga, Guler Tumer Erdem, Bozyel Serdar, Yalin Kivanc. Vagal responses during cardioneuroablation on different ganglionated plexi: Is there any role of ablation strategy? Int. J. Cardiol. 2020 Apr 01;304 ():50–55. doi: 10.1016/j.ijcard.2019.12.003. [DOI] [PubMed] [Google Scholar]
- 29.Lemery Robert, Birnie David, Tang Anthony S L, Green Martin, Gollob Michael. Feasibility study of endocardial mapping of ganglionated plexuses during catheter ablation of atrial fibrillation. Heart Rhythm. 2006 Apr;3 (4):387–96. doi: 10.1016/j.hrthm.2006.01.009. [DOI] [PubMed] [Google Scholar]
- 30.Po Sunny S, Nakagawa Hiroshi, Jackman Warren M. Localization of left atrial ganglionated plexi in patients with atrial fibrillation. J. Cardiovasc. Electrophysiol. 2009 Oct;20 (10):1186–9. doi: 10.1111/j.1540-8167.2009.01515.x. [DOI] [PubMed] [Google Scholar]
- 31.Mantziari Lilian, Suman-Horduna Irina, Gujic Marko, Jones David G, Wong Tom, Markides Vias, Foran John P, Ernst Sabine. Use of asymmetric bidirectional catheters with different curvature radius for catheter ablation of cardiac arrhythmias. Pacing Clin Electrophysiol. 2013 Jun;36 (6):757–63. doi: 10.1111/pace.12113. [DOI] [PubMed] [Google Scholar]
- 32.Aksu Tolga, Guler Tumer Erdem, Bozyel Serdar, Golcuk Sukriye Ebru, Yalin Kivanc, Lakkireddy Dhanunjaya, Gopinathannair Rakesh. Medium-term results of cardioneuroablation for clinical bradyarrhythmias and vasovagal syncope: effects on QT interval and heart rate. J Interv Card Electrophysiol. 2020 Feb 07; () doi: 10.1007/s10840-020-00704-2. [DOI] [PubMed] [Google Scholar]
- 33.Pachon M Jose C, Pachon M Enrique I, Santillana P Tomas G, Lobo Tasso J, Pachon Carlos T C, Pachon M Juan C, Albornoz V Remy N, Zerpa A Juan C. Simplified Method for Vagal Effect Evaluation in Cardiac Ablation and Electrophysiological Procedures. JACC Clin Electrophysiol. 2015 Oct;1 (5):451–460. doi: 10.1016/j.jacep.2015.06.008. [DOI] [PubMed] [Google Scholar]