

ABSTRACT
Background
Anticholinergic drugs are associated with significant cognitive and other adverse events in older adults, including those with Parkinson's disease (PD). Anticholinergic effects are considered lesser in younger individuals and the burden and outcomes in younger patients with PD are unknown.
Objectives
To determine the cumulative anticholinergic burden in a cohort of younger of patients with PD and to correlate the same with cognitive impairment and freezing of gait (FOG).
Methods
We conducted a cross‐sectional study to identify the cumulative anticholinergic burden from medications prescribed to patients with PD. Two standard scales, the Anticholinergic Cognitive Burden (ACB) scale and the ACB score, were used to calculate the anticholinergic burden from prescriptions. We identified commonly prescribed drugs contributing to anticholinergic effects and correlated the cumulative ACB score with cognitive impairment (Movement Disorder Society–Unified Parkinson's Disease Rating Scale item 1.1) and FOG (Movement Disorder Society–Unified Parkinson's Disease Rating Scale items 2.13 and 3.11).
Results
We recruited 287 patients with PD (68.9% male) with a mean age of 56.9 ± 11.8 years and a duration of symptoms 6.3 ± 6.9 years. Median ACB score was 4 (range 0–12). A total of 164 (58.4%) patients had total ACB score > 3. ACB score > 3 was independently associated with cognitive impairment (Odds Ratio, 2.55; 95% confidence interval, 1.43–4.53; P < 0.001) and FOG using patient‐reported measures (Odds Ratio, 3.192; 95% Confidence Interval, 1.68–6.07; P < 0.001) and objective measures (odds ratio, 2.41; 95% confidence interval, 1.27–4.6, P = 0.007).
Conclusion
Patients with PD are exposed to significant anticholinergic burden from drugs prescribed for PD and non‐PD indications. Higher anticholinergic burden is associated with cognitive impairment and FOG even in younger patients with PD.
Keywords: Parkinson's disease, anticholinergic burden, cognitive impairment, anticholinergic scales, freezing of gait
Anticholinergics are a common class of drugs used to treat the symptoms of Parkinson's disease (PD), particularly tremors. Anticholinergic drugs are often used in the early stages of PD, when symptoms are mild, and more than 50% of prescriptions to patients with PD across healthcare settings contain these drugs. 1 Levodopa in combination with a peripheral decarboxylase inhibitor is the mainstay of treatment in PD, and other medications such as dopamine agonists, monoamine oxidase‐B inhibitors, and catechol‐O‐methyl transferase inhibitors maybe used additionally as monotherapy or add ons. Some of these drugs also have additional anticholinergic effects along with their major effects on dopaminergic neurotransmission. In addition to these, patients with PD may also be prescribed drugs with primary or secondary anticholinergic effects for non‐PD indications, such as psychiatric symptoms and other medical comorbidities. 2 Primarily anticholinergic drugs and the secondary anticholinergic properties of drugs prescribed for PD and non‐PD indications can contribute to the overall anticholinergic burden in this population.
Anticholinergic drugs are associated with various side effects such as blurred vision, dry mouth, constipation, difficulty in voiding, and urinary retention. Anticholinergic burden is a concept used to quantify the cumulative effect of exposure to 1 or more drug having anticholinergic properties. 3 The elderly are particularly susceptible to anticholinergic cognitive side effects such as confusion, hallucinations, and cognitive impairment. 4 A retrospective study conducted in Finland identified anticholinergic exposure to be strongly associated with mortality in the older population. 5 , 6 Other studies confirmed this finding and also reported increased risk of hospitalization among the elderly exposed to anticholinergics. 7 , 8 , 9 , 10 Specifically in PD, patients with higher anticholinergic burden were more likely to have fractures, delirium, and readmissions. 11 Higher cumulative doses of anticholinergics were associated with increased risk of dementia in PD. 12 , 13 Long‐term exposure to anticholinergic drugs in PD was associated with increased cortical plaques or tangles pathologically. 14 Much of the literature on anticholinergic burden in PD and other diseases is focussed on the elderly as they are the most vulnerable to anticholinergic side effects.
In resource limited settings, primary anticholinergic drugs are widely prescribed for PD because of the ease of availability and low cost. Prescription patterns from India show that about 40% patients are on trihexyphenidyl at presentation to a tertiary care center. 15 A higher proportion of patients with younger age at onset in Indian cohorts in India is often considered as a reason for better tolerance to anticholinergic effects. 16 There is limited data on the cognitive and other adverse effects of anticholinergics, especially in the context of younger patients with PD. We aimed to assess the anticholinergic burden and its association with cognitive impairment and gait in this context.
Methods
We conducted a cross‐sectional study among consecutive patients with PD attending the movement disorder clinic at the All India Institute for Medical Sciences, New Delhi—a tertiary care university hospital. The study was hospital based and completed in 16 months. We included patients who had a clinical diagnosis of PD (United Kingdom Parkinson's Disease Society brain bank criteria) and prescriptions of current medications available. 17 Patients with atypical parkinsonism or vascular parkinsonism, those naïve to drugs, and those with other movement disorders were excluded. Written informed consent was obtained from all subjects prior to recruitment. This study was approved by the Institutional Ethics Committee.
We collected demographic details and relevant history including the medication log. Data regarding the names of medication, indications, doses (per administration), dose units, frequencies/schedules, dose forms, routes of administration, and start dates and end dates (if applicable) were collected for all patients. These included prescriptions from our hospital (for patients on follow‐up) and prescriptions from previous care providers (for new registrants to the clinic). All prescribed medications were numerically coded according to the Anatomical Therapeutic Chemical classification and entered into a computerized database. 18 Study data were collected and managed using the REDCap electronic data capture tools hosted at All India Institute of Medical Sciences, New Delhi. 19 , 20 The Movement Disorder Society (MDS)–Sponsored Revision of the Unified Parkinson's Disease Rating Scale (UPDRS) was used for assessing the motor symptoms and few nonmotor symptoms. 21 Patient, caregiver, or both were the data sources for the self‐rating items on MDS‐UPDRS. We used MDS‐UPDRS item 1.1 to assess cognitive impairment. This self‐reported cognitive impairment score has been shown to have good correlation with objective measures of cognitive impairment such as the Montreal Cognitive Assessment and has also been validated with other nonmotor scales. 22 , 23 The MDS‐UPDRS items 2.13 and 3.11 were both used to assess freezing of gait (FOG) as using only item 3.11 may miss FOG episodes at home, depending on medication status at the time of examination.
Calculation of Anticholinergic Burden
To date, no universally accepted scale is available to calculate the anticholinergic effects of different drugs, and each scale contains a different list of drugs with some drugs that may be overlapping. Each scale has its own criteria to measure anticholinergic activity, for example, some scales consider average daily dose and some the cumulative dose, serum concentration, or clinical cognitive decline in their criteria. 24 Despite these differences among scales, concordance also exists between anticholinergic burden scales. Despite limitations, serum anticholinergic activity is considered as a gold standard in quantifying anticholinergic burden, and this was incorporated into a clinical scale known as the Anticholinergic Burden Scale (ABS). 25 The ABS divides the anticholinergic drugs into 4 categories from 0 to 3, that is, 0 = no anticholinergic activity to 3 = definite/high anticholinergic activity. 25 , 26 , 27 , 28 , 29 , 30 Further scales retained the ordinal structure of the ABS while focusing on the clinical effects of anticholinergic burden such as poorer cognitive and functional outcomes. 30 Five concordant scales used to measure anticholinergic burden, especially in the older population, were identified in a systematic review. 24 In 2008, 2 other scales were published, the Anticholinergic Risk Scale and the Anticholinergic Cognitive Burden Scale (ACB), both of which also used an ordinal scale to rank medications. 28 , 31 The ACB was developed after reviewing literature of anticholinergic drugs associated with delirium, cognitive decline, and dementia. 31 As with the ABS, individual medications may be summed within the Anticholinergic Risk Scale and ACB to provide an overall anticholinergic burden score. A recent review identified the ACB scale to be suited for analysis of administrative data. 32 After reviewing 6 anticholinergic burden scales, we used a combination of the following 2 standard scales: ACB and the newly created ACB score developed in Germany to calculate the individual anticholinergic burden from prescriptions. 33 These were chosen as they are validated scales and as the newer ACB score included a larger number of drugs, particularly those available in India, and assessed them on similar criteria as the ACB scale. Cumulative ACB score was calculated as the sum of ACB scores of individual drugs. For drug combinations, ACB scores of the components were recorded individually. A total ACB score > 3 is known to be significantly associated with adverse outcomes. 34
Statistical Analysis
Continuous variables were summarized as mean ± standard deviation or median/range as appropriate. Univariate analysis using the chi‐squared test was used to assess the association between total ACB score, cognitive impairment, and FOG. ACB scores and MDS‐UPDRS item scores were dichotomized for multivariate analysis. Binomial logistic regression using a model that incorporated relevant clinical variables (age, gender, age at onset, duration of illness and dichotomized ACB score (≤3 or > 3)) was used to identify independent predictors of cognitive impairment (MDS‐UPDRS item 1.1 ≥ 1) and FOG (MDS‐UPDRS items 2.13 and 3.11 ≥ 1). All statistical analysis was done on SPSS version 24.0 (IBM Corp, Armonk, NY).
Results
We recruited 289 consecutive patients with PD from November 2018 to February 2020. Two subjects were excluded later as a result of incomplete clinical data. Data from 287 participants (69.3% men) were included in the final analysis. Mean age of the participants was 56.9 ± 11.8 years. Age at onset of PD was 50.2 ± 13.2 years, and duration of symptoms was 6.3 ± 6.9 years. Of the participants, 19.5% had familial PD. The mean MDS‐UPDRS Part III score was 27.4 ± 18.7. Patients were on a median of 4 (Interquartile Range = 4) medications. Median total ACB score was 4 (range 0–12). Total ACB score was >3 in 164 patients (58.4%). We identified 4 drugs with ACB score 3, 6 drugs with ACB score 2, and 19 drugs with ACB score 1 in this population (Table 1). Drugs with ACB score 0 are listed in the Table S1. At least 1 drug with an ACB score of 3 was being taken by 41.5% of patients, trihexyphenidyl was the most common of these drugs. Among the drugs contributing to anticholinergic burden, 14 (50%) were prescribed for indications related to PD (motor or nonmotor symptoms), whereas 14 (50%) were prescribed for non‐PD indications (Fig. 1).
TABLE 1.
Drugs with significant anticholinergic effects and number of patients
| ACB Score | Drug Name | ATC Code | N |
|---|---|---|---|
| 3 | Tolterodine | G04BD07 | 3 |
| Trihexyphenidyl | N04AA01 | 103 | |
| Quetiapine | N05AH04 | 11 | |
| Amitriptyline | N06AA09 | 2 | |
| 2 | Oxcarbazepine | N03AF02 | 2 |
| Carbamazepine | N03AF01 | 3 | |
| Amantadine | N04BB01 | 89 | |
| Baclofen | M03BX01 | 1 | |
| Pethidine | N02AB02 | 1 | |
| Cetrizine | R06AE07 | 1 | |
| 1 | Escitalopram | N06AB10 | 91 |
| Levodopa + carbidopa | N04BA02 | 291 | |
| Clonazepam | N03AE01 | 73 | |
| Domperidone | A03FA03 | 9 | |
| Etoricoxib | M01AH05 | 1 | |
| Metoprolol | C07AB02 | 2 | |
| Atenolol | C07AB03 | 5 | |
| Pramipexole | N04BC05 | 163 | |
| Metformin | A10BA02 | 12 | |
| Entacapone | N04BX02 | 24 | |
| Mirtazapine | N06AX11 | 1 | |
| Sertraline | N06AB06 | 2 | |
| Chlorthalidone | C03BA04 | 3 | |
| Selegiline | N04BD01 | 1 | |
| Metformin + sitagliptin | A10BD07 | 1 | |
| Metformin + pioglitazone | A10BD05 | 2 | |
| Gentamicin | J01GB03 | 1 | |
| Alprazolam | N05BA12 | 1 |
FIG. 1.
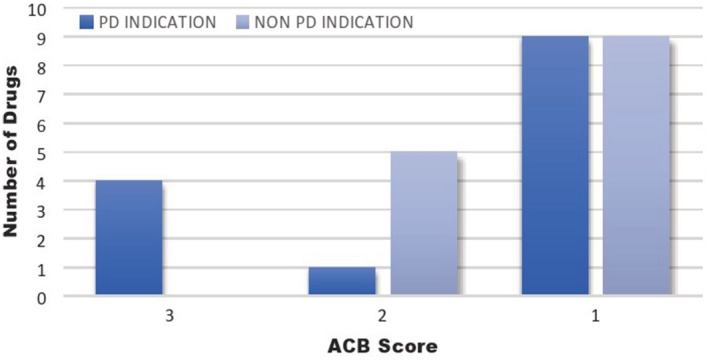
Distribution of medications with significant anticholinergic effects according to indication. All drugs with ACB score 3 were prescribed for motor or nonmotor symptoms related to PD. ACB, anticholinergic burden; PD, Parkinson's disease.
Cognitive impairment of any severity was reported by 30.3% (n = 87). FOG in the past 1 week was reported by 25.8% (n = 74), whereas it was observed on clinical examination in 23% (n = 66). Higher total ACB score was significantly associated with cognitive impairment (P = 0.034) and FOG as assessed by both MDS‐UPDRS items 2.13 (P < 0.001) and 3.11 (P < 0.001) (Figure S1). Regression models could account for upto 13% variance in the dependent variable with classification accuracy of up to 78.6%. In a model including current age, age at onset, duration of illness, gender, and ACB score, ACB score > 3 was the only independent predictor of cognitive impairment (Odds Ratio [OR], 2.55; 95% Confidence Interval [CI], 1.43–4.53; P < 0.001). ACB score > 3 was the strongest predictor of having experienced FOG during the past 1 week (OR, 3.192; 95% CI, 1.68–6.07; P < 0.001), followed by male gender (OR, 2.08; 95% CI, 1.16–3.74; P = 0.015). Similarly, ACB score > 3 was the strongest predictor of FOG on examination in the clinic (OR, 2.41; 95% CI, 1.27–4.6; P = 0.007) along with male gender (OR, 2.03; 95% CI, 1.12–3.70; P = 0.021) and age at onset (OR, 1.04; 95% CI, 1.002–1.08; P = 0.042). A later age of onset by 1 year increased the odds of having FOG by 4% (P = 0.042).
Discussion
Our results suggest that patients with PD in India are exposed to significant anticholinergic effects from medications. Among our patients, 58.4% had exposure to significant anticholinergic burden defined as total ACB score > 3. This is similar to cohorts from Canada (57.8%), 1 , 2 , 35 Spain (53.6%), and France (3 of 5 prescriptions) (Table 2). Concomitant anticholinergic use was also a common prescription error in patients with PD with dementia treated with cholinesterase inhibitors. 35 Of note, all the medications with individual ACB score > 3 were prescribed for PD and related indications (trihexyphenidyl, tolterodine, quetiapine, and amitriptyline). Although the highest risk category was dominated by PD‐related medications, a number of medications prescribed for non‐PD indications contributed to the cumulative anticholinergic burden. Trihexyphenidyl was the most commonly prescribed high‐risk medication (n = 103; 86.5%). Its beneficial effects on motor symptoms, especially tremor and low cost, make it a popular drug in our setting. 36 It is also often considered that younger patients with PD maybe more tolerant of the anticholinergic side effects of this drug.
TABLE 2.
Studies on frequency of anticholinergic burden in PD, without outcome assessment
| Serial No. | Study ID | Study Design | Number of Subjects (PD) | Age, Yrs (Mean ± SD or Median [Range]) | Anticholinergic Burden Assessment | Results |
|---|---|---|---|---|---|---|
| 1 | De Germay et al, 2016 1 | Audit of pharmacovigilance database | 471 | 72.2 ± 11.4 | Duran's list 37 | Atropinic burden ≥3 in 17.0% |
| 2 | Lertxundi et al, 2015 2 | Retrospective audit of hospital administrative data, in‐patients only | 1628 | 81 (30–102) | Duran's list, ACB, ADS, ARS 28 , 31 , 37 , 38 | 53.6% in‐patients had at least 1 anticholinergic drug |
| 3 | Mantri et al, 2019 35 | Retrospective audit of insurance database, patients with PD with ACHEI only | 73,093 | 78.9 ± 7.5 | ACB score | 44.5% of PD receiving ACHEI had concomitant prescription of anticholinergic drug |
Abbreviations: PD, Parkinson's disease; ID, identification; SD, standard deviation; ACB, Anticholinergic Cognitive Burden Scale; ADS, Anticholinergic Drug Scale; ARS, Anticholinergic Risk Scale; ACHEI, Acetyl Cholinesterase Inhibitor .
Contrary to this, our results show that even younger patients with PD bear the brunt of anticholinergic adverse effects. The mean age of onset of our patients was almost a decade younger compared with typical PD cohorts. The mean duration was about 6 years, and the majority of patients were younger than 60 years of age at the time of this study. Even in this relatively young population, one third reported cognitive impairment, and a quarter reported FOG. On multivariate analysis, cumulative anticholinergic burden was the strongest predictor of both cognitive impairment and FOG. Anticholinergics are known to impair immediate memory on neuropsychological testing in patients with PD, with exposures of as short durations as 4 months. 39 In non‐PD elderly, anticholinergics were directly associated with cognitive decline and mortality. 40 In a longitudinal study of patients with PD, anticholinergic drug exposure and duration of their use were strongly associated with later cognitive decline. 13 We could find 3 studies that have looked at the association of anticholinergic burden with clinical outcomes in PD in a real‐life setting, including 1 in the in‐patient setting (Table 3). The mean age of the population in all 3 previous studies was about 70 years, an age group already well known to be susceptible to the neurocognitive adverse effects of anticholinergics.
TABLE 3.
Studies on clinical outcomes of anticholinergic burden in PD
| Serial No. | Study ID | Study Design | Number of Subjects (PD) | Age, Yrs (Mean ± SD or Median [Range]) | Anticholinergic Burden Assessment | Results |
|---|---|---|---|---|---|---|
| 1 | Yarnall et al, 2015 41 | Prospective study (18 months follow‐up) | 219 | 68.6 ± 8.9 |
Anticholinergic Drug Scale 38 ADS ≥ 1 considered significant |
ADS ≥ 1 in 42.6% No difference in cognitive tests between PD with and without ADS ≥ 1 |
| 2 | Crispo et al, 2016 11 | Retrospective audit of hospital administrative data, in‐patients only | 16,302 | 82.3% >70 yrs | ARS 28 |
57.8% received medications with moderate/strong anticholinergic potential ARS ≥ 4 more likely to be admitted with fractures, delirium during index admission and to require ED visit or readmission after discharge |
| 3 | Ehrt et al, 2010 13 | Prospective cohort study | 235 | 74.7 ± 8.4 | Modified version of AA 5 | 43.4% received at least one drug with AA. At 8 yrs, higher cognitive decline in those who had been taking drugs with AA |
| 4 | Present study | Cross‐sectional study | 287 | 56.9 ± 11.8 | ACB score, modified ACB score |
ACB score ≥ 3 in 58.4%. ACB associated with cognitive impairment and FOG |
Abbreviations: PD, Parkinson's disease; ID, identification; SD, standard deviation; ADS, Anticholinergic Drug Scale; ARS, Anticholinergic Risk Scale; ED, emergency department; AA, Anticholinergic Activity; ACB, Anticholinergic Cognitive Burden Scale; FOG, freezing of gait.
Our results also revealed that higher anticholinergic burden was associated with FOG. One of the previous studies indicated that anticholinergic burden was higher in the in‐patients with PD admitted with fractures, although they did not assess FOG directly. 11 Cholinergic neuronal loss in the pedunculopontine–thalamic tracts has been associated with falls in PD. 42 The pedunculopontine nucleus, which is rich in cholinergic activity, is also a putative target for deep brain stimulation to improve FOG in PD and atypical parkinsonism. 43 Age and gender are known modulators of the clinical phenotype in PD. In general, women are known to have a more tremor‐dominant phenotype, associated with slower progression. 44 Duration of illness is also a well‐known predictor of gait disturbances including FOG, which are typically seen after a decade of PD. Our results are also consistent with these findings.
The novel contribution from our study is the evidence of significant cognitive‐related and gait‐related adverse effects in a younger cohort of patients with PD. Although these side effects are well known in elderly, they are often given lesser importance in younger patients. These findings highlight the need for judicious use of anticholinergics even in younger patients with PD. Many drugs that are the mainstay of PD treatment do have lesser anticholinergic effects, the cumulative effects of which may become significant clinically and hence a rational prescription strategy is necessary. Although prescription trends such as dopaminergic blocking agents are flagged in well‐known practice quality measures for PD, anticholinergic effects are not similarly highlighted. 45 Accordingly, in our study we could find the use of dopamine blocking agents in only 3 patients of 287, whereas more than 50% were on medications with significant anticholinergic effects.
There are many limitations to our study. We conducted a cross‐sectional analysis and longitudinal follow‐up of these patients after reducing the cholinergic burden will strengthen the evidence for a causal association. We used patient‐reported outcome parameters for cognition, which may be prone to recall bias, and objective measures of cognition such as the Montreal Cognitive Assessment and FOG questionnaires should be incorporated in future studies. As indicated by the regression model, additional factors such as mood, anxiety, and genetic factors may affect the outcome, which we have not addressed in this study. Individual dose and duration effects were not assessed as these were not part of the standard scales for anticholinergic burden that we used. Despite limitations, our study highlights trends in prescription patterns that may affect clinical outcomes and quality of life in PD. The existing body of evidence and our results suggest that equal focus should be placed on the rational use of medications with anticholinergic potential in younger patients with PD as in older adults to avoid adverse outcomes.
Author Roles
(1) Research Project: A. Conception, B. Organization, C. Execution; (2) Statistical Analysis: A. Design, B. Execution, C. Review and Critique; (3) Manuscript Preparation: A. Writing of the first draft, B. Review and Critique.
R.R.: 1A, 1C, 2A, 2B, 3A
A.S.: 1B, 1C, 2A, 2B, 3A
B.V.: 2B, 3B
N.C.: 2B,3B
A.G.: 2C, 3B
V.Y.V.: 2C, 3B
R.B.: 2C, 3B
M.B.S.: 2C,3B
A.K.S.: 2C, 3B
M.V.P.S.: 2C, 3B
Disclosures
Ethical Compliance Statement
This study was approved by Institutional Ethics Committee No. 173/06.04.2018, RP‐4/2018. Written informed consent was obtained from all subjects prior to recruitment. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
Funding Source and Conflict of Interest
This research was funded by Department of Biotechnology under the project entitled “The Indian Movement Disorder Registry and Biobank: Clinical and Genetic Evaluation of Movement Disorders in Indian Patients.” The authors declare that there are no conflicts of interest relevant to this work.
Financial Disclosures for the Previous 12 Months
The authors declare that there are no additional disclosures to report.
Supporting information
Figure S1 Heat map showing relationship among cumulative ACB score (top row), cognitive impairment (Movement Disorder Society–Unified Parkinson's Disease Rating Scale item 1.1), and freezing of gait (Movement Disorder Society–Unified Parkinson's Disease Rating Scale item 2.13 [FOG II and 3.11 [FOG III]. Each column represents an individual patient. The values in each row represent the corresponding patient values as shown in the color code legend. ACB, anticholinergic burden; FOG, freezing of gait.
{kind=link}
Table S1 Drugs with anticholinergic burden score 0 and number of patients.
Acknowledgment
The authors acknowledge Anandapadmanabhan R for his assistance with the logistics of the project.
Relevant disclosures and conflicts of interest are listed at the end of this article.
References
- 1. De Germay S, Montastruc J‐L, Rousseau V, et al. Atropinic (anticholinergic) burden in Parkinson's disease. Mov Disord 2016;31(5):632–636. 10.1002/mds.26595. [DOI] [PubMed] [Google Scholar]
- 2. Lertxundi U, Isla A, Solinis MA, et al. Anticholinergic burden in Parkinson's disease inpatients. Eur J Clin Pharmacol 2015;71(10):1271–1277. 10.1007/s00228-015-1919-7. [DOI] [PubMed] [Google Scholar]
- 3. Nishtala PS, Salahudeen MS, Hilmer SN. Anticholinergics: theoretical and clinical overview. Expert Opin Drug Saf 2016;15(6):753–768. 10.1517/14740338.2016.1165664. [DOI] [PubMed] [Google Scholar]
- 4. Tune LE. Anticholinergic effects of medication in elderly patients. J Clin Psychiatry 2001;62(Suppl 21):11–14. [PubMed] [Google Scholar]
- 5. Kumpula E‐K, Bell JS, Soini H, Pitkälä KH. Anticholinergic drug use and mortality among residents of long‐term care facilities: a prospective cohort study. J Clin Pharmacol 2011;51(2):256–263. 10.1177/0091270010368410. [DOI] [PubMed] [Google Scholar]
- 6. Panula J, Puustinen J, Jaatinen P, Vahlberg T, Aarnio P, Kivela S‐L. Effects of potent anticholinergics, sedatives and antipsychotics on postoperative mortality in elderly patients with hip fracture: a retrospective, population‐based study. Drugs Aging 2009;26(11):963–971. 10.2165/11317660-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 7. Roe CM, Anderson MJ, Spivack B. Use of anticholinergic medications by older adults with dementia. J Am Geriatr Soc 2002;50(5):836–842. 10.1046/j.1532-5415.2002.50208.x. [DOI] [PubMed] [Google Scholar]
- 8. Lechevallier‐Michel N, Molimard M, Dartigues J‐F, Fabrigoule C, Fourrier‐Réglat A. Drugs with anticholinergic properties and cognitive performance in the elderly: results from the PAQUID study. Br J Clin Pharmacol 2005;59(2):143–151. 10.1111/j.1365-2125.2004.02232.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Wilson NM, Hilmer SN, March LM, et al. Associations between drug burden index and falls in older people in residential aged care. J Am Geriatr Soc 2011;59(5):875–880. 10.1111/j.1532-5415.2011.03386.x. [DOI] [PubMed] [Google Scholar]
- 10. Desforges JF, Montamat SC, Cusack BJ, Vestal RE. Management of drug therapy in the elderly. N Engl J Med 1989;321(5):303–309. 10.1056/NEJM198908033210507. [DOI] [PubMed] [Google Scholar]
- 11. Crispo JAG, Willis AW, Thibault DP, et al. Associations between anticholinergic burden and adverse health outcomes in Parkinson disease. PLoS ONE 2016;11(3):e0150621 10.1371/journal.pone.0150621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Sheu J‐J, Tsai M‐T, Erickson SR, Wu C‐H. Association between anticholinergic medication use and risk of dementia among patients with Parkinson's disease. Pharmacotherapy 2019;39(8):798–808. 10.1002/phar.2305. [DOI] [PubMed] [Google Scholar]
- 13. Ehrt U, Broich K, Larsen JP, Ballard C, Aarsland D. Use of drugs with anticholinergic effect and impact on cognition in Parkinson's disease: a cohort study. J Neurol Neurosurg Psychiatry 2010;81(2):160–165. 10.1136/jnnp.2009.186239. [DOI] [PubMed] [Google Scholar]
- 14. Perry EK, Kilford L, Lees AJ, Burn DJ, Perry RH. Increased Alzheimer pathology in Parkinson's disease related to antimuscarinic drugs. Ann Neurol 2003;54(2):235–238. 10.1002/ana.10639. [DOI] [PubMed] [Google Scholar]
- 15. Surathi P, Kamble N, Bhalsing KS, Yadav R, Pal PK. Prescribing pattern for Parkinson's disease in Indian community before referral to tertiary center. Can J Neurol Sci 2017;44(6):705–710. 10.1017/cjn.2017.208. [DOI] [PubMed] [Google Scholar]
- 16. Punia S, Behari M, Govindappa ST, et al. Absence/rarity of commonly reported LRRK2 mutations in Indian Parkinson's disease patients. Neurosci Lett 2006;409(2):83–88. 10.1016/j.neulet.2006.04.052. [DOI] [PubMed] [Google Scholar]
- 17. van Hilten JJ, van der Zwan AD, Zwinderman AH, Roos RA. Rating impairment and disability in Parkinson's disease: evaluation of the Unified Parkinson's Disease Rating Scale. Mov Disord. 2020;17(5):867–876. [DOI] [PubMed] [Google Scholar]
- 18. Peng Y, Wang M, Xu Y, et al. Drug repositioning by prediction of drug's anatomical therapeutic chemical code via network‐based inference approaches [published online ahead of print March 28, 2020]. Brief Bioinform 2020. 10.1093/bib/bbaa027. [DOI] [PubMed] [Google Scholar]
- 19. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap): a metadata‐driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42(2):377–381. 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform 2019;95:103208 10.1016/j.jbi.2019.103208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. van Hilten JJ, van der Zwan AD, Zwinderman AH, Roos RA. Rating impairment and disability in Parkinson's disease: evaluation of the Unified Parkinson's disease Rating Scale. Mov Disord 1994;9(1):84–88. 10.1002/mds.870090113. [DOI] [PubMed] [Google Scholar]
- 22. Mills KA, Mari Z, Pontone GM, et al. Cognitive impairment in Parkinson's disease: association between patient‐reported and clinically measured outcomes. Parkinsonism Relat Disord 2016;33:107–114. 10.1016/j.parkreldis.2016.09.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Gallagher DA, Goetz CG, Stebbins G, Lees AJ, Schrag A. Validation of the MDS‐UPDRS part I for nonmotor symptoms in Parkinson's disease. Mov Disord 2012;27(1):79–83. 10.1002/mds.23939. [DOI] [PubMed] [Google Scholar]
- 24. Naples JG, Marcum ZA, Perera S, et al. Concordance between anticholinergic burden scales. J Am Geriatr Soc 2015;63(10):2120–2124. 10.1111/jgs.13647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Carnahan RM, Lund BC, Perry PJ, Pollock BG, Culp KR. The anticholinergic drug scale as a measure of drug‐related anticholinergic burden: associations with serum anticholinergic activity. J Clin Pharmacol 2006;46(12):1481–1486. 10.1177/0091270006292126. [DOI] [PubMed] [Google Scholar]
- 26. Kersten H, Wyller TB. Anticholinergic drug burden in older people's brain ‐ how well is it measured? Basic Clin Pharmacol Toxicol 2014;114(2):151–159. 10.1111/bcpt.12140. [DOI] [PubMed] [Google Scholar]
- 27. Hilmer SN, Mager DE, Simonsick EM, et al. A drug burden index to define the functional burden of medications in older people. Arch Intern Med 2007;167(8):781–787. 10.1001/archinte.167.8.781. [DOI] [PubMed] [Google Scholar]
- 28. Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med 2008;168(5):508–513. 10.1001/archinternmed.2007.106. [DOI] [PubMed] [Google Scholar]
- 29. Boustani MA, Campbell NL, Khan BA, et al. Enhancing care for hospitalized older adults with cognitive impairment: a randomized controlled trial. J Gen Intern Med 2012;27(5):561–567. 10.1007/s11606-012-1994-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Salahudeen MS, Duffull SB, Nishtala PS. Anticholinergic burden quantified by anticholinergic risk scales and adverse outcomes in older people: a systematic review. BMC Geriatr 2015;15:31 10.1186/s12877-015-0029-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Campbell N, Boustani M, Limbil T, et al. The cognitive impact of anticholinergics: a clinical review. Clin Interv Aging 2009;4:225–233. 10.2147/cia.s5358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Lozano‐Ortega G, Johnston KM, Cheung A, et al. A review of published anticholinergic scales and measures and their applicability in database analyses. Arch Gerontol Geriatr 2020;87:103885 10.1016/j.archger.2019.05.010. [DOI] [PubMed] [Google Scholar]
- 33. Kiesel EK, Hopf YM, Drey M. An anticholinergic burden score for German prescribers: score development. BMC Geriatr 2018;18(1):239 10.1186/s12877-018-0929-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. De Vreese LP, Mantesso U, De Bastiani E, Marangoni A, Weger E, Gomiero T. Anticholinergic burden in adult and elderly people with intellectual disabilities: results from an Italian multicenter cross‐sectional study. PLoS ONE 2018;13(10):e0205897 10.1371/journal.pone.0205897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Mantri S, Fullard M, Gray SL, et al. Patterns of dementia treatment and frank prescribing errors in older adults with Parkinson disease. JAMA Neurol 2019;76(1):41–49. 10.1001/jamaneurol.2018.2820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Katzenschlager R, Sampaio C, Costa J, Lees A. Anticholinergics for symptomatic management of Parkinson's disease. Cochrane Database Syst Rev 2003;2:CD003735 10.1002/14651858.CD003735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Durán CE, Azermai M, Vander Stichele RH. Systematic review of anticholinergic risk scales in older adults. Eur J Clin Pharmacol 2013;69(7):1485–1496. 10.1007/s00228-013-1499-3. [DOI] [PubMed] [Google Scholar]
- 38. Kersten H, Molden E, Willumsen T, Engedal K, Bruun Wyller T. Higher Anticholinergic Drug Scale (ADS) scores are associated with peripheral but not cognitive markers of cholinergic blockade. Cross sectional data from 21 Norwegian nursing homes. Br J Clin Pharmacol 2013;75(3):842–849. 10.1111/j.1365-2125.2012.04411.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Cooper JA, Sagar HJ, Doherty SM, Jordan N, Tidswell P, Sullivan EV. Different effects of dopaminergic and anticholinergic therapies on cognitive and motor function in Parkinson's disease. A follow‐up study of untreated patients. Brain 1992;115 (Pt 6:1701–1725. 10.1093/brain/115.6.1701. [DOI] [PubMed] [Google Scholar]
- 40. Fox C, Richardson K, Maidment ID, et al. Anticholinergic medication use and cognitive impairment in the older population: the medical research council cognitive function and ageing study. J Am Geriatr Soc 2011;59(8):1477–1483. 10.1111/j.1532-5415.2011.03491.x. [DOI] [PubMed] [Google Scholar]
- 41. Yarnall AJ, Lawson RA, Duncan GW, et al. Anticholinergic load: is there a cognitive cost in early Parkinson's disease? J Parkinsons Dis 2015;5(4):743–747. 10.3233/JPD-150664. [DOI] [PubMed] [Google Scholar]
- 42. Bohnen NI, Müller MLTM, Koeppe RA, et al. History of falls in Parkinson disease is associated with reduced cholinergic activity. Neurology 2009;73(20):1670–1676. 10.1212/WNL.0b013e3181c1ded6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Wang J‐W, Zhang Y‐Q, Zhang X‐H, Wang Y‐P, Li J‐P, Li Y‐J. Deep brain stimulation of pedunculopontine nucleus for postural instability and gait disorder after Parkinson disease: a meta‐analysis of individual patient data. World Neurosurg 2017;102:72–78. 10.1016/j.wneu.2017.02.110. [DOI] [PubMed] [Google Scholar]
- 44. Georgiev D, Hamberg K, Hariz M, Forsgren L, Hariz G‐M. Gender differences in Parkinson's disease: a clinical perspective. Acta Neurol Scand 2017;136(6):570–584. 10.1111/ane.12796. [DOI] [PubMed] [Google Scholar]
- 45. Cheng EM, Tonn S, Swain‐Eng R, et al. AAN Parkinson disease quality measures: Report of the quality measurement and reporting subcommittee of the American Academy of Neurology. Neurology 2010;75(22):2021–2027. 10.1212/WNL.0b013e3181ff96dd. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1 Heat map showing relationship among cumulative ACB score (top row), cognitive impairment (Movement Disorder Society–Unified Parkinson's Disease Rating Scale item 1.1), and freezing of gait (Movement Disorder Society–Unified Parkinson's Disease Rating Scale item 2.13 [FOG II and 3.11 [FOG III]. Each column represents an individual patient. The values in each row represent the corresponding patient values as shown in the color code legend. ACB, anticholinergic burden; FOG, freezing of gait.
Table S1 Drugs with anticholinergic burden score 0 and number of patients.