

Abstract
A current topic in dentistry concerns the biocompatibility of the materials, and in particular, conservative dentistry and endodontics ones. The mineral trioxide aggregate (MTA) is a dental material with biocompatibility properties to oral and dental tissues. MTA was developed for dental root repair in endodontic treatment and it is formulated from commercial Portland cement, combined with bismuth oxide powder for radiopacity. MTA is used for creating apical plugs during apexification, repairing root perforations during root canal therapy, treating internal root resorption, and pulp capping. The objective of this article is to investigate MTA features from a clinical point of view, even compared with other biomaterials. All the clinical data regarding this dental material will be evaluated in this review article. Data obtained from the analysis of the past 10 years’ literature highlighted 19 articles in which the MTA clinical aspects could be recorded. The results obtained in this article are an important step to demonstrate the safety and predictability of oral rehabilitations with these biomaterials and to promote a line to improve their properties in the future.
Keywords: dental materials, Portland cements, dentin, pulp exposure, pulp capping, root canal filling
Introduction
The mineral trioxide aggregate (MTA) is a hydrophilic and biocompatible endodontic cement, capable of stimulating healing and osteogenesis. It consists of a powder of fine trioxides (tricalcium oxide, silicon oxide, bismuth oxide) and other hydrophilic particles (tricalcium silicate, tricalcium aluminate, responsible for the chemical and physical properties of this aggregate), which hardens in the presence of humidity. 1 2 3 4 5 The hydration of the powder results in the formation of a colloidal gel with pH 12.5, which solidifies in a structure in about 3 to 4 hours. 6 7 8 9
In the past 10 years, the MTA found its application in the field of dentistry with specific fit within the conservative and endodontic treatments. A dental trauma is an event that cannot be predicted and usually it is not easy for the clinicians to manage it. The dentist should therefore be prepared to intervene in patient who has suffered a dental trauma. Early intervention is often crucial to improve the prognosis of the trauma itself. In the presence of a coronal fracture with dentine exposure, the primary objective should be to seal dentinal tubules. Especially in a young patient, the size and number of dentinal tubules are large: even a small amount of exposed dentin therefore allows a large number of plaque bacteria and their metabolites to move to the underlying pulp and cause inflammation. An occurrence of this type could, sometimes in short time, lead to necrosis. When the dental trauma has caused a pulp exposure, the emergency intervention consists with the management of the exposed pulp. One of the treatments, besides the endodontic treatment, is direct capping or partial pulpotomy. Partial pulpotomy could be performed using MTA. The MTA could be applied as cement for its high compatibility, which has a mechanism similar to calcium hydroxide (Ca(OH) 2 ) (extremely basic) and therefore a powerful antibacterial.
Unlike Ca(OH) 2 , however, the MTA hardens, reaching a good consistency; it is, therefore, extremely suitable for any restoration. Fast hardening therefore allows partial pulpotomies performed with MTA to be restored in a definitive manner. 7
Pulp consisting of a cellular component, vessels and nerves; this tissue is called mature mucosal connective tissue. Endodontic therapy is used if a tooth carious or traumatic injury has caused an irreversible alteration of the pulp tissue and its necrosis. It is also possible to use this method if the dental element is to be involved in prosthetic rehabilitations, which due to the considerable reduction of the dental tissue, it would determine, with high probability, an irreversible pulp alteration. During endodontic treatment, blood contamination should be absolutely avoided, and the roots canal system needs to be dry, to obtain a successful root canal filling. During direct pulp capping or perforation sealing, it is fundamental to control the bleeding and obtain a dry field too. The mechanism of action of the MTA is related with the clinical features of the human oral cavity. MTA, when placed in direct contact with human tissues, is able to release calcium ions for cell proliferation. Moreover, it creates an antibacterial environment by its alkaline pH, regulating the cytokine production. Therefore, it favors the migration and differentiation of hard tissue producing cells forming hydroxyapatite on MTA surface and providing a biological seal. Finally, during a surgical endodontic procedure, the retrograde cavity should be completely dry. This cement differs from all other materials currently in existence, thanks to its biocompatibility, its antibacterial properties, its marginal adaptation, and its sealing capacities, and finally, thanks to its hydrophilic nature. It is important to understand the functioning of this biomaterial, its behavior with contact with other materials used in dentistry, and above all, over time or from a clinical and radiographic point of view. 10 11 12 Investigating these topics requires a research into the international literature, which also includes the use of cutting-edge technologies for examination. 13 14 15 16
The purpose of this review is to evaluate all the recent scientific literature concerning this topic and to evaluate all its clinical features. The evaluation of different studies offers information about the facets of the material related to endodontics, conservative dentistry, and oral surgery.
Materials and Methods
Protocol and Registration
This article has been registered as review in a systemic review database called PROSPERO. It is an International Prospective Register of Systematic Reviews about health and social care. Obtained PROSPERO registration number is 156248 on October 27, 2019. The main question of this study has been elaborated following PICOT (Population/Intervention/Comparison/Outcome/Time) study design.
This review follows a protocol according to PROSPERO and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Transparent Reporting of Systematic Reviews and Meta-Analyses).
Eligibility Criteria
The results obtained from the literature search were filtered, through software and manual screening, according to the following inclusion and exclusion criteria:
-
Inclusion criteria
∘ Human studies
∘ Information about MTA clinical use
∘ Information about MTA and other biomaterials in endodontics
∘ In vitro and in vivo studies about MTA
∘ Last 10 years of studies
-
Exclusion criteria
∘ In silica studies
∘ Not on human studies
∘ Not in English
∘ Not accessible title or abstract
∘ Not enough information about main question
Information Sources
Results were obtained after a research and a screening on scientific international database as PubMed, Embase, and Web of Science. Automatic filter and platforms software have been used for results screening.
Search
Search has been conducted using this keyword on information sources: “Mineral Trioxide Aggregate.” Search date is August 1, 2019.
The database search protocol details are: (“mineral trioxide aggregate” [Supplementary Concept] OR “mineral trioxide aggregate” [All Fields]) AND (“2009/10/30” [PDat]: “2019/10/27” [PDat] AND “humans” [MeSH Terms]).
Keywords have been chosen by authors after a discussion with the aim to include as large as possible number of results ( Fig. 1 ).
Fig. 1.
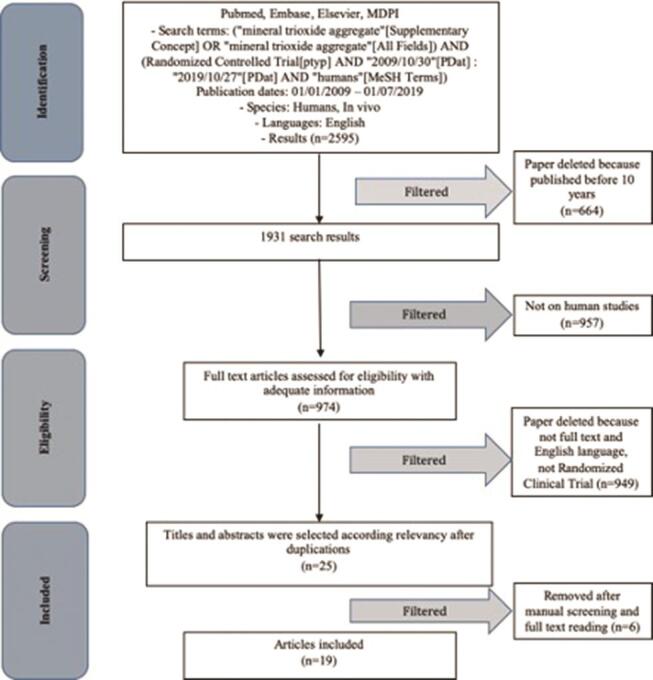
Preferred reporting items for systematic reviews and meta-analyses flow chart.
PICO questions are:
In dental patients, what is the effect of MTA use on pulp vitality?
How MTA features could improve clinical success on dental patients?
Study Selection
Authors with the aim to include relevant studies for this review have conducted selection process. After applying the electronic eligibility criteria, the authors conducted a manual study selection independently.
Data Collection Process
Two independent authors from two different universities conducted the data collection process (D.R., University of Naples and L.F., University of Messina). After data screening completion, they clarified any doubt with other expert reviewers (M.D.T. and L.L.).
Data Items
The following data items were considered during data collection; summary measures and data items are shown in Tables 1 2 :
Table 1. All mineral trioxide aggregate use.
| Conservative dentistry | Indirect pulp capping |
| Direct pulp capping | |
| Endodontic dentistry | Root filling |
| Root filling with postcore indication |
Table 2. Main results and item investigated on reviews.
| Authors (y) | Sample | Items | Outcomes | Type of study |
|---|---|---|---|---|
| Abbreviations: MTA, mineral trioxide aggregate; RCT, randomized controlled trial; ZOE, zinc oxide eugenol. | ||||
| Çelik et al (2019) 20 | 24 + 20 | MTA vs. Biodentine | Differences on success, p = 0.646 | RCT |
| Erfanparast et al (2018) 21 | 46 × 2 (split mouth) | Resin modified Portland cement vs. MTA | Differences are not significant, p > 0.05 | RCT |
| Koc Vural et al (2017) 22 | 49 + 51 | MTA vs. calcium hydroxide | There are no differences between used materials, p = 0.238 (or higher) | RCT |
| Kang et al (2017) 23 | 33 + 36 + 35 | ProRoot MTA vs. Ortho MTA vs. RetroMTA | No significant differences between groups | RCT |
| Bakhtiar et al (2017) 24 | 9 + 9 + 9 | TheraCal vs. Biodentine vs. ProRoot MTA | Normal pulp organization ( p = 0.06); dentinal bridge formation ( p = 0.001) | RCT |
| Asl Aminabadi et al (2016) 25 | 40 + 40 + 40 + 40 | Simvastatin vs. 3Mix vs. 3Mixtatin vs. MTA | No differences between MTA and 3Mixtatin ( p > 0.05) | RCT |
| Aminabadi et al (2016) 26 | 40 + 40 | 3Mixtatin vs. MTA | Clinical differences between groups | RCT |
| Nowicka et al (2015) 27 | 11 + 11 + 11 + 11 | Calcium hydroxide, MTA, Biodentine, Single Bond Universal | Reparative formed dentin was less in Single Bond Universal group; the mean density of dentin bridges was the highest in the MTA group and the lowest in the Single Bond Universal group | RCT |
| Kang et al (2015) 28 | 49 + 47 + 47 | RetroMTA vs. Ortho MTA vs. PRoRoot MTA | Clinical success rate is similar and not statistically significant | RCT |
| Bonte et al (2015) 29 | 15 + 15 | MTA vs. calcium hydroxide | Success rate demonstrated a difference between groups, p < 0.7 | RCT |
| Petrou et al (2014) 30 | 31 + 26 + 29 | Calcium hydroxide vs. medical Portland cement vs. white MTA | Difference between groups are not significant ( p = 0.72) | RCT |
| Hilton et al (2013) 31 | 181 + 195 | Calcium hydroxide vs. MTA | Failure rate at 24 mo was 31.5% for calcium hydroxide and 19.7% for MTA | RCT |
| Gandolfi et al (2013) 32 | 8 + 8 | AH Plus vs. MTA Flow | MTA flow sealer created a dense apatite layer after 7 d | RCT |
| Bernabé et al (2013) 33 | 34 | ProRoot MTA | Sonic vibration could be considered an efficient aid to improve MTA sealing ability | RCT |
| Sönmez et al (2012) 34 | 15 + 15 + 15 + 6 | AH Plus vs. MTA Fillapex vs. ProRoot MTA vs. control | MTA Fillapex had higher microleakage values, p < 0.05 | RCT |
| Leye Benoist et al (2012) 35 | 60 | MTA vs. calcium hydroxide | Success rates are different between groups at 3 mo, p = 0.02 | RCT |
| Ghoddusi et al (2012) 36 | MTA vs. ZOE) | MTA and ZOE showed both clinical success | RCT | |
| Hansen et al (2011) 37 | 12 + 12 | ProRoot MTA vs. EndoSequence Root Repair Material | pH level was higher for MTA and EndoSequence p < 0.05 | RCT |
| Yildirim et al (2009) 38 | 15 + 15 + 15 + 6 | Gutta-percha vs. Gutta-percha prepared with gates vs. MTA vs. control | MTA showed less microleakage, p < 0.005 | RCT |
-
Investigated data items on articles ( Table 2 )
∘ Authors and year—article authors and year of publication (references have been added)w
∘ Sample—sample size and groups size
∘ Outcome—main results of the study
∘ Type of study—type of article.
Summary Measures
Summary measures are shown in Table 1 .
Synthesis of Results
The authors performed the summary of the results manually, after reading the title, abstract, and full text of each article.
Risk of Bias
A risk of bias evaluation was performed according to Higgins et al. Risk of bias has been conducted to improve review quality according to PRISMA statement too. 17 18 19 20
Results
Study Selection
The results were obtained in relation to the “Materials and Methods” instructions. Using the set out in paragraph 2.4 keywords, 2,595 results were obtained. Subsequently, according to eligibility criteria, results have been screened. The authors decided to maintain only past 10 years results to underline the novelty and accuracy on diagnostics method as well as the quality of the new technologies results in the field of MTA application. A total of 1,931 results remained after this first screening. Only 25 studies on human have been considered, and the authors analyzed full text and English articles. The last step to complete the revision of the results was to compare only review articles type. Only 19 results, after a reading and a manual authors screening, were resulted eligible for this study ( Fig. 1 ).
Results of Individual Studies
Results of individual studies are listed in Table 2 Fig. 2 . The results are divided accordingly to PRISMA statement and organized into sample, items, outcomes, and type of study. Authors’ name and year have been restricted following the interval time range of 10 years.
Fig. 2.
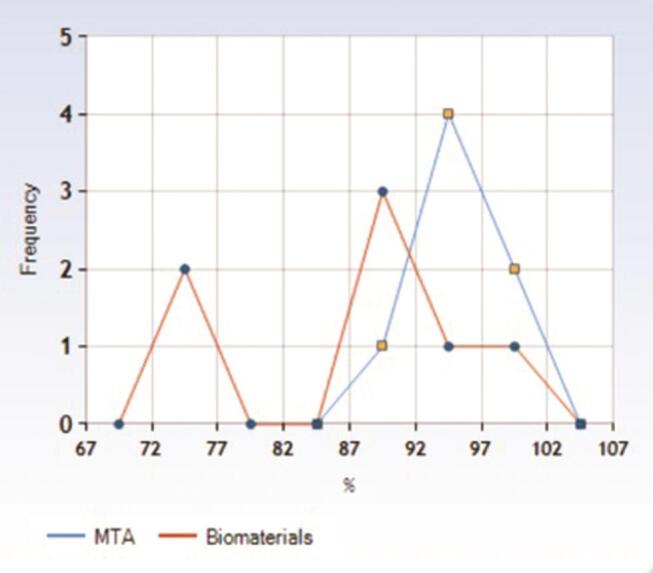
Success rate frequency polygon chart of MTA (blue) versus other biomaterials. MTA, mineral trioxide aggregate.
Synthesis of Results
Çelik et al 20 analyzed differences between two groups of patients involved in pulpotomy treatment. The MTA groups had a 100% success rate at 24 months instead of 89.4% with Biodentine use. According to Erfanparast et al, 21 there are no significant differences on resin-modified Portland cement-based materials versus MTA in direct pulp capping. After 12 months, the success rate for MTA and resin-modified one were 94.5 and 91.8%, respectively. Koc Vural et al 22 evaluated differences between Ca(OH) 2 and MTA. The follow-up term for a total of 100 samples was of 24 months. Four Ca(OH) 2 capped teeth and two MTA capped received endodontic emergency treatments. But there are no significant differences between groups. Kang et al 23 studied clinical differences between three MTA groups (ProRoot MTA, Ortho MTA, and RetroMTA). The success rate at 1 year was high with no significant differences; the success rates were 96, 92.8, and 96%, respectively (as listed in parentheses). Bakhtiar et al 24 investigated differences on third molar pulpotomy between three different materials (TheraCal, Biodentine, and ProRoot). They showed how there were no clinical signs on ProRoot MTA and Biodentine groups as two patients reported significant pain in TheraCal group. Pulp reorganization was seen in 33.33% of ProRoot MTA, 11.11% of TheraCal, and 66.67% of Biodentine groups. Moreover, dentinal bridge formation was seen on 11% of TheraCal and 56% of ProRoot MTA. Asl Aminabadi et al 25 tested clinical differences between four groups for direct pulp capping. Noncaries pulpal exposures were treated with simvastatin, 3Mix, 3Mixtatin, or MTA. At the end of a 12-month follow-up period, the overall success rates were 93.8% (MTA), 91.9% (3Mixtatin), 62.5% (3Mix), and 57.1% (simvastatin). According to the authors, there were no significant differences ( p = 0.05) between MTA and 3Mixtatin groups. 3Mixtatin groups had a statistical difference on simvastatin and 3Mix groups ( p < 0.01). Another study of Aminabadi et al 26 confirmed 3Mixtatin efficiency on pulp capping. The authors inspected MTA versus 3Mixtatin on direct pulp capping with a 96.8% of success rate against MTA with 48.6% of referred pain. Nowicka et al 27 evaluated differences on direct pulp capping between four groups: Ca(OH) 2 , MTA, Biodentine, and Single Bond Universal. The reparative dentin formed in the Ca(OH) 2 , MTA, and Biodentine was superior to the Single Bond Universal group. Moreover, the dentin bridges density was the highest in the MTA group and the lowest in the Single Bond Universal group. Kang et al 28 published a report about differences on three MTA materials. At 12 months, the radiographic success rates in these groups were 100% (RetroMTA), 97.4% (Ortho MTA), and 100% (ProRoot MTA). The Kaplan–Meier’s survival function relative to clinical and radiographic rates did not differ between groups. According to Bonte et al, 29 MTA at 12 months produced mineralized barrier in 82.4% of cases instead of Ca(OH) 2 (50%). Pain and tenderness to percussion had disappeared in both groups. In a Petrou et al 30 randomized controlled trial, it was demonstrated at ~6.3 months of time on 86 patients how Ca(OH) 2 versus medical Portland cement versus white MTA did not show any statistical difference. The total success rate was 90.3%. Hilton et al 31 recently published a study about the clinical and radiographic differences on two direct capping materials groups, Ca(OH) 2 versus MTA. MTA showed a less failure rate ( p = 0.046). Gandolfi et al 32 analyzed, through a three-dimensional microcomputed tomography (3D micro-CT) analysis, differences between AH Plus and MTA flow on their microstructure. Bernabé et al 33 tested the MTA sealing ability for apicectomy. They filled with MTA plus sonic, ultrasonic, or no vibration. The sonic vibration could improve sealing level. Sönmez et al 34 showed differences on the apical microleakage between AH Plus, MTA Fillapex, and ProRoot MTA. Fillapex had better results about microleakage and there are no statistical differences between AH Plus and MTA. Leye Benoist et al 35 highlighted differences between Ca(OH) 2 and MTA for indirect pulp capping. At 3 months, the success rate of MTA was 93% instead of 73% for Ca(OH) 2 . At 6 months, the success rate was 89.6% for MTA instead of 73%. The mean initial residual dentine thickness was 0.23 mm, this value has been increased to 0.121 mm with MTA and 0.136 with Ca(OH) 2 at 3-month time. According to Ghoddusi et al, 36 there are no statistical differences between MTA or zinc oxide eugenol (ZOE) in pulpotomy after a carious or traumatic pulp exposure. Hansen et al 37 considered the pH level with the use of different biomaterials for pulp capping. The authors studied MTA, Endodontic Sealing(ES); control pairs were filled with Ca(OH) 2 (positive group) and saline (negative). The pH was measured at 20 minutes, 3 hours, 24 hours, and 1–2 to 3–4 weeks. The MTA pH was significantly higher during the time than ES (at 1 week, p < 0.0001). Yildirim et al 38 discovered differences on filling between gutta-percha with two methods and MTA. Cervino et al obtained better results with MTA, then showed less microleakage ( Fig. 3 ). 7
Fig. 3.
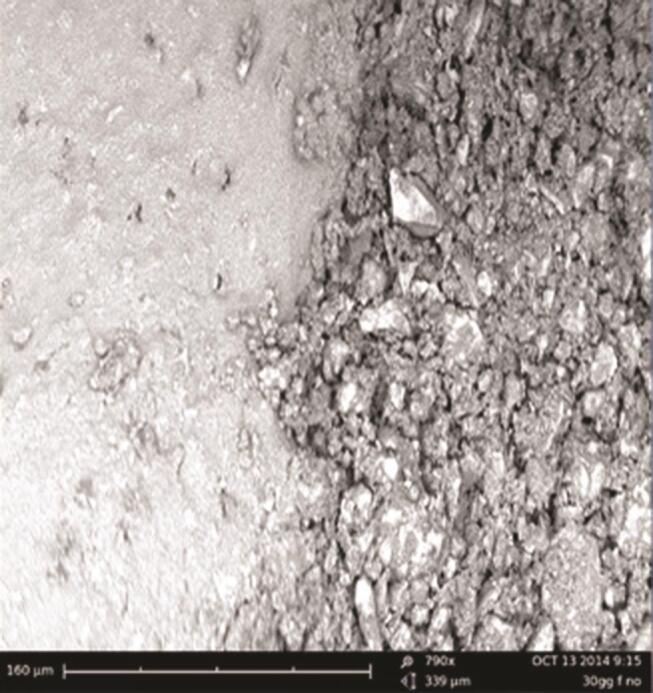
SEM microleakage between MTA and bonding agents. The MTA use could, in some cases, make the definitive reconstruction complex due to the physical–chemical properties of itself and difficulty of use with hydrophobic substances. MTA, mineral trioxide aggregate; SEM, scanning electron microscope.
Discussion
All the conclusions of the selected articles for this present review have been summarized in this section as follows: Çelik et al 20 evaluated clinical success differences between MTA and Biodentine. The authors showed how both MTA and Biodentine are appropriate options for pulpotomy. According to this study, it seems how the etiology of pulp exposure is the crucial on pulpal response (mechanical or carious) whether or not the kind of material applied. Erfanparast et al 21 concluded that resin-based Portland cement results are comparable to MTA for primary molars after 12 months of follow-up and no significant differences can be underlined between the two biomaterials investigated. Koc Vural et al performed a similar study, about the comparison of two endodontic materials. 22 The authors reported that Ca(OH) 2 and MTA are both accepting pulp-capping materials at a 24-month follow-up term.
Kang et al 23 in a 1-year follow-up study investigated three different materials applied to pulpotomy technique. The procedure was classified as safe and predictable with ProRoot MTA, Ortho MTA, or RetroMTA documented through clinical and radiographical data. Bakhtiar et al 24 published an in vitro study about how some endodontic biomaterials could be efficient than others for the pulp capping procedures. The authors performed histology to evaluate dentinal bridge formation and organization after teeth extraction (disodontiasis third molar). Data demonstrated how Biodentine and ProRoot MTA work better than TheraCal.
According to Asl Aminabadi et al, 25 there are no radiographic and clinical differences between MTA and 3Mixtatin, and it could represent a valid alternative in direct pulp capping. Aminabadi et al 26 evaluated at 24 months the efficiency of 3Mixtatin, showing how this biomaterial could have better clinical result than MTA from a clinical and radiographic point of view. According to the authors, it could represent the future pulp capping material.
Several published articles underlined the clinical features of the MTA just evaluating clinical and radiological data. Nowicka et al 27 demonstrated how the reparative dentin bridges are dependent on the material used. Biodentine and MTA resulted in the highest volumes after the cone beam radiography. According to Kang et al, 28 RetroMTA, Ortho MTA, and ProRoot MTA success rates did not differ and are indistinguishable, and these results indicate that pulpotomy could be performed with a high success rate with all the evaluated biomaterials. Bonte et al 29 showed how there is no statistical difference between Ca(OH) 2 and MTA, but MTA produced a better dentin healing, apexification using MTA could give better results than Ca(OH) 2 .
Petrou et al 30 concluded that MTA or medical Portland cements are preferable to Ca(OH) 2 for indirect pulp capping because those materials are nonresorbable materials. Hilton et al 31 showed how MTA is superior for direct pulp capping to Ca(OH) 2 . Gandolfi et al 32 concluded in their study, after a 3D micro-CT analysis, that MTA flow created an apatite layer after 7 days, and AH Plus even after 28 days. Bernabé et al 33 showed how MTA could be useful item for root canal filling after apicectomy; moreover, a sonic vibration could improve sealing ability. Sönmez et al 34 concluded that the sealing ability of AH Plus and ProRoot is similar, but MTA Fillapex showed microleakage compared with the other two materials.
Some studies reported how the results could be modified if the evaluation is reported at 3, 6 months, or 1 year after the treatment. This clinical condition demonstrated how the patient response could be individual and not related to the materials or technique applied. According to Leye Benoist et al, 35 a higher success rate was observed in the MTA group instead of Ca(OH) 2 . Differences were significant at 3 months but not at 6 months, with no dentine thickness differences, showing time of evaluation importance. Ghoddusi et al 36 concluded that there are no statistical differences between ZOE or MTA treatments, but MTA was successful, expensive, and because of dentin bridges could complicate future root canal therapy. Data reported by Hansen et al 37 demonstrated how the MTA produce an intracanal higher pH than ES. The same result was demonstrated by Yildirim et al. 38 MTA can be used in the root canals as apical filling materials, in particular, in teeth with postcore indication.
All these results extrapolated by the selected articles provide us documented clinical information and the MTA seems to be as having excellent abilities from the point of view of biocompatibility, as could be seen from the studies, but also of stability over time. 39 40 41 The nanocharacteristic of the MTA could be related about its interactions with the human tissue during the endodontic treatment. Remineralizing potential intercepting early lesion progression as nanosized calcium phosphate, carbonate hydroxyapatite nanocrystals, nanoamorphous calcium phosphate, and nanoparticulate bioactive glass particularly with provision of self-assembles protein that furnish essential role in biomimetic repair even in the dental field. The unique size of nanomaterials makes them fascinating carriers for dental products. 42 43 44 45 46 47 48 49 50 Thus, it is recently claimed that fortifying the adhesives with nanomaterials that possess biological merits does not only enhance the mechanical and physical properties of the adhesives but also help attain and maintain a durable adhesive joint and enhanced longevity. It is also necessary to report how these conservative therapies often do not expose patients to invasive surgical or not risks, practices that in patients with unfavorable systemic conditions would be complex to apply. Accordingly, this review will focus on the current status and the future implications of nanotechnology in preventive and adhesive dentistry. In dental materials, the main applications of nanotechnology have been to achieve better mechanical properties, higher abrasion resistance, less shrinkage, improved optical, and esthetic properties, and to provide antimicrobial properties. Antimicrobial activity is an important property for nanomaterials used in dentistry because of the lack of this property in resin-based materials. MTA is a biomaterial that has numerous possibilities for endodontic therapy, as animal studies and clinical results are highly encouraging. It can also be used in deciduous dentition, with deep carious lesion or exposure to the traumatic pulp intended for endodontic therapy. 51 52 53 54 55 56 57 58 59 60 61 The MTA could not be used to save all teeth with pulp involvement; however, with a meticulous technique, it could serve as a pulp drug in advance to add to a clinical use. Modern nanotechnology is used in the production of a variety of dental materials such as light-cured composite resins, adhesive systems, impression materials, ceramics, dental implant coatings, and bioceramics, among others. In pediatric age, a whole series of dental malocclusions could occur. There could be different types of dental malocclusions: some are genetic, and others are caused by external factors; the big difference in the treatment of these malocclusions in pediatric and in adulthood is that in children, treatment tends to be much less invasive as the bones have yet to fully develop and it is easier to intervene to correct their shape. Therefore, it should be understood how the absence of a dental element, extracted rather than saved, thanks to an endodontic treatment, even in borderline conditions, thanks to the use of these cements, could have repercussions on the whole stomatognathic system. 62 63 Moreover, the material is versatile, guaranteeing different uses, and having excellent characteristics in being in contact with the materials for reconstruction. 64 65 66 67 68 69 70 71 72 73 74 75 76 77
Conclusion
The results of this review would be certainly useful to fully understand the characteristics and advantages of this biomaterial from a clinical point of view; our structural analysis of the material explains its clinical behavior; and the studies examined are the proof. The numerous clinical, histological, and radiographic tests make this material a safe and predictable material in the endodontic and conservative dentistry fields. Some studies have shown better characteristics than the MTA, above all, from an antibiotic point of view. This could act as a starting point for the improvement of this material and the creation of even better materials.
Funding Statement
Funding None.
Footnotes
Authors’ ContributionsConflict of Interest Conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, original draft preparation, and review and editing of the manuscript were done by G.C., M.D.T., and L.F.; visualization was performed by D.R., L.N., and C.D.A.; data were curated by G.A., M.T., F.G., and A.T.; L.L. supervised the entire work and L.F. performed project administration.
None declared.
References
- 1.Tu M G, Sun K T, Wang T H et al. Effects of mineral trioxide aggregate and bioceramics on macrophage differentiation and polarization in vitro. J Formos Med Assoc. 2019;118(10):1458–1465. doi: 10.1016/j.jfma.2019.07.010. [DOI] [PubMed] [Google Scholar]
- 2.Serin Kalay T. Effects of intracoronal bleaching agents on the surface properties of mineral trioxide aggregate. Odontology. 2019;107(04):465–472. doi: 10.1007/s10266-019-00418-6. [DOI] [PubMed] [Google Scholar]
- 3.Lopes M B, Soares V CG, Fagundes F HR et al. Analysis of molecular changes induced by mineral trioxide aggregate on sPLA2. Braz Dent J. 2019;30(05):453–458. doi: 10.1590/0103-6440201902463. [DOI] [PubMed] [Google Scholar]
- 4.Liu Y, Liu X M, Bi J et al. Cell migration and osteo/odontogenesis stimulation of iRoot FS as a potential apical barrier material in apexification. Int Endod J. 2020;53(04):467–477. doi: 10.1111/iej.13237. [DOI] [PubMed] [Google Scholar]
- 5.Lin YT, Lin YJ. Success rates of mineral trioxide aggregate, ferric sulfate, and sodium hypochlorite pulpotomies: a prospective 24-month study. J Formos Med Assoc 2019 [DOI] [PubMed]
- 6.Lapinska B, Klimek L, Sokolowski J, Lukomska-Szymanska M. Dentine surface morphology after chlorhexidine application-SEM study. Polymers (Basel) 2018;10(08):905. doi: 10.3390/polym10080905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cervino G, Fiorillo L, Spagnuolo G et al. Interface between MTA and dental bonding agents: scanning electron microscope evaluation. J Int Soc Prev Community Dent. 2017;7(01):64–68. doi: 10.4103/jispcd.JISPCD_521_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lo Giudice G, Cutroneo G, Centofanti A et al. Dentin morphology of root canal surface: a quantitative evaluation based on a scanning electronic microscopy study. BioMed Res Int. 2015;2015:164065. doi: 10.1155/2015/164065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zarra T, Lambrianidis T, Vasiliadis L, Gogos C. Effect of curing conditions on physical and chemical properties of MTA. Int Endod J. 2018;51(11):1279–1291. doi: 10.1111/iej.12938. [DOI] [PubMed] [Google Scholar]
- 10.Colombo M, Poggio C, Dagna A et al. Biological and physico-chemical properties of new root canal sealers. J Clin Exp Dent. 2018;10(02):e120–e126. doi: 10.4317/jced.54548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lo Giudice G, Cicciù M, Cervino G, Lizio A, Visco A M. Flowable resin and marginal gap on tooth third medial cavity involving enamel and radicular cementum: a SEM evaluation of two restoration techniques. Indian J Dent Res. 2012;23(06):763–769. doi: 10.4103/0970-9290.111256. [DOI] [PubMed] [Google Scholar]
- 12.Fiorillo L, Cervino G, Herford A S et al. Interferon crevicular fluid profile and correlation with periodontal disease and wound healing: a systemic review of recent data. Int J Mol Sci. 2018;19(07):E1908. doi: 10.3390/ijms19071908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.De Stefano R. Psychological factors in dental patient care: odontophobia. Medicina (Kaunas) 2019;55(10):678. doi: 10.3390/medicina55100678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cicciù M, Fiorillo L, Cervino G. Chitosan use in dentistry: a systematic review of recent clinical studies. Mar Drugs. 2019;17(07):417. doi: 10.3390/md17070417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Savovic J, Turner R M, Mawdsley D et al. Association between risk-of-bias assessments and results of randomized trials in Cochrane reviews: the ROBES meta-epidemiologic study. Am J Epidemiol. 2018;187(05):1113–1122. doi: 10.1093/aje/kwx344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mansournia M A, Higgins J P, Sterne J A, Hernán M A. Biases in randomized trials: a conversation between trialists and epidemiologists. Epidemiology. 2017;28(01):54–59. doi: 10.1097/EDE.0000000000000564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cochrane Bias Methods Group, Cochrane Statistical Methods Group . Higgins J P, Altman D G, Gøtzsche P C. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Coburn K M, Vevea J L. Publication bias as a function of study characteristics. Psychol Methods. 2015;20(03):310–330. doi: 10.1037/met0000046. [DOI] [PubMed] [Google Scholar]
- 19.Bachelet V C, Pardo-Hernandez H. Quality of reporting and risk of bias of randomized clinical trials published in Spanish and Latin American journals. Medwave. 2019;19(01):e7573. doi: 10.5867/medwave.2019.01.7573. [DOI] [PubMed] [Google Scholar]
- 20.Çelik B N, Mutluay M S, Arıkan V, Sarı Ş. The evaluation of MTA and Biodentine as a pulpotomy materials for carious exposures in primary teeth. Clin Oral Investig. 2019;23(02):661–666. doi: 10.1007/s00784-018-2472-4. [DOI] [PubMed] [Google Scholar]
- 21.Erfanparast L, Iranparvar P, Vafaei A. Direct pulp capping in primary molars using a resin-modified Portland cement-based material (TheraCal) compared to MTA with 12-month follow-up: a randomised clinical trial. Eur Arch Paediatr Dent. 2018;19(03):197–203. doi: 10.1007/s40368-018-0348-6. [DOI] [PubMed] [Google Scholar]
- 22.Koc Vural U, Kiremitci A, Gokalp S. Randomized clinical trial to evaluate MTA indirect pulp capping in deep caries lesions after 24-months. Oper Dent. 2017;42(05):470–477. doi: 10.2341/16-110-C. [DOI] [PubMed] [Google Scholar]
- 23.Kang C M, Sun Y, Song J S et al. A randomized controlled trial of various MTA materials for partial pulpotomy in permanent teeth. J Dent. 2017;60:8–13. doi: 10.1016/j.jdent.2016.07.015. [DOI] [PubMed] [Google Scholar]
- 24.Bakhtiar H, Nekoofar M H, Aminishakib P et al. Human pulp responses to partial pulpotomy treatment with TheraCal as compared with Biodentine and ProRoot MTA: a clinical trial. J Endod. 2017;43(11):1786–1791. doi: 10.1016/j.joen.2017.06.025. [DOI] [PubMed] [Google Scholar]
- 25.Asl Aminabadi N, Satrab S, Najafpour E, Samiei M, Jamali Z, Shirazi S. A randomized trial of direct pulp capping in primary molars using MTA compared to 3Mixtatin: a novel pulp capping biomaterial. Int J Paediatr Dent. 2016;26(04):281–290. doi: 10.1111/ipd.12196. [DOI] [PubMed] [Google Scholar]
- 26.Aminabadi N A, Huang B, Samiei M, Agheli S, Jamali Z, Shirazi S. A randomized trial using 3Mixtatin compared to MTA in primary molars with inflammatory root resorption: a novel endodontic biomaterial. J Clin Pediatr Dent. 2016;40(02):95–102. doi: 10.17796/1053-4628-40.2.95. [DOI] [PubMed] [Google Scholar]
- 27.Nowicka A, Wilk G, Lipski M, Kołecki J, Buczkowska-Radlińska J. Tomographic evaluation of reparative dentin formation after direct pulp capping with Ca(OH)2, MTA, Biodentine, and dentin bonding system in human teeth. J Endod. 2015;41(08):1234–1240. doi: 10.1016/j.joen.2015.03.017. [DOI] [PubMed] [Google Scholar]
- 28.Kang C M, Kim S H, Shin Y et al. A randomized controlled trial of ProRoot MTA, Ortho MTA and RetroMTA for pulpotomy in primary molars. Oral Dis. 2015;21(06):785–791. doi: 10.1111/odi.12348. [DOI] [PubMed] [Google Scholar]
- 29.Bonte E, Beslot A, Boukpessi T, Lasfargues J J. MTA versus Ca(OH)2 in apexification of non-vital immature permanent teeth: a randomized clinical trial comparison. Clin Oral Investig. 2015;19(06):1381–1388. doi: 10.1007/s00784-014-1348-5. [DOI] [PubMed] [Google Scholar]
- 30.Petrou M A, Alhamoui F A, Welk A, Altarabulsi M B, Alkilzy M, H. Splieth C. A randomized clinical trial on the use of medical Portland cement, MTA and calcium hydroxide in indirect pulp treatment. Clin Oral Investig. 2014;18(05):1383–1389. doi: 10.1007/s00784-013-1107-z. [DOI] [PubMed] [Google Scholar]
- 31.Northwest Practice-based Research Collaborative in Evidence-based Dentistry (NWP) Hilton T J, Ferracane J L, Mancl L.Comparison of CaOH with MTA for direct pulp capping: a PBRN randomized clinical trial J Dent Res 20139207(Suppl)16S–22S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gandolfi M G, Parrilli A P, Fini M, Prati C, Dummer P M. 3D micro-CT analysis of the interface voids associated with Thermafil root fillings used with AH Plus or a flowable MTA sealer. Int Endod J. 2013;46(03):253–263. doi: 10.1111/j.1365-2591.2012.02124.x. [DOI] [PubMed] [Google Scholar]
- 33.Bernabé P F, Gomes-Filho J E, Bernabé D G et al. Sealing ability of MTA used as a root end filling material: effect of the sonic and ultrasonic condensation. Braz Dent J. 2013;24(02):107–110. doi: 10.1590/0103-6440201301973. [DOI] [PubMed] [Google Scholar]
- 34.Sönmez I S, Oba A A, Sönmez D, Almaz M E. In vitro evaluation of apical microleakage of a new MTA-based sealer. Eur Arch Paediatr Dent. 2012;13(05):252–255. doi: 10.1007/BF03262880. [DOI] [PubMed] [Google Scholar]
- 35.Leye Benoist F, Gaye Ndiaye F, Kane A W, Benoist H M, Farge P. Evaluation of mineral trioxide aggregate (MTA) versus calcium hydroxide cement (Dycal(®)) in the formation of a dentine bridge: a randomised controlled trial. Int Dent J. 2012;62(01):33–39. doi: 10.1111/j.1875-595X.2011.00084.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ghoddusi J, Shahrami F, Alizadeh M, Kianoush K, Forghani M. Clinical and radiographic evaluation of vital pulp therapy in open apex teeth with MTA and ZOE. N Y State Dent J. 2012;78(03):34–38. [PubMed] [Google Scholar]
- 37.Hansen S W, Marshall J G, Sedgley C M. Comparison of intracanal EndoSequence root repair material and ProRoot MTA to induce pH changes in simulated root resorption defects over 4 weeks in matched pairs of human teeth. J Endod. 2011;37(04):502–506. doi: 10.1016/j.joen.2011.01.010. [DOI] [PubMed] [Google Scholar]
- 38.Yildirim T, Taşdemir T, Orucoglu H. The evaluation of the influence of using MTA in teeth with post indication on the apical sealing ability. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(03):471–474. doi: 10.1016/j.tripleo.2009.04.036. [DOI] [PubMed] [Google Scholar]
- 39.Jinga S I, Voicu G, Stoica-Guzun A, Stroescu M, Grumezescu AM, Bleotu C. Biocellulose nanowhiskers cement composites for endodontic use. Dig J Nanomater Biostructures. 2014;9(02):543–550. [Google Scholar]
- 40.Voicu G, Bǎdǎnoiu A I, Ghiţulicǎ C D, Andronescu E. Sol-gel synthesis of white mineral trioxide aggregate with potential use as biocement. Dig J Nanomater Biostructures. 2012;7(04):1639–1646. [Google Scholar]
- 41.Tao O, Wu D T, Pham H M, Pandey N, Tran S D. Nanomaterials in craniofacial tissue regeneration: a review. Appl Sci. 2019;9(02):317. [Google Scholar]
- 42.Jun S K, Yoon J Y, Mahapatra C et al. Ceria-incorporated MTA for accelerating odontoblastic differentiation via ROS downregulation. Dent Mater. 2019;35(09):1291–1299. doi: 10.1016/j.dental.2019.05.024. [DOI] [PubMed] [Google Scholar]
- 43.Opačić-Galić V, Petrović V, Jokanović V, Živković S. Histological evaluation of tissue reactions to newly synthetized calcium silicate-and hydroxyapatite-based bioactive materials - in vivo study. Srp Arh Celok Lek. 2017;145(00):63–63. [Google Scholar]
- 44.Huq N L, Myroforidis H, Cross K J et al. The interactions of CPP-ACP with saliva. Int J Mol Sci. 2016;17(06):E915. doi: 10.3390/ijms17060915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Heller D, Helmerhorst E J, Oppenheim F G. Saliva and serum protein exchange at the tooth enamel surface. J Dent Res. 2017;96(04):437–443. doi: 10.1177/0022034516680771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Gibbins H L, Yakubov G E, Proctor G B, Wilson S, Carpenter G H. What interactions drive the salivary mucosal pellicle formation? Colloids Surf B Biointerfaces. 2014;120:184–192. doi: 10.1016/j.colsurfb.2014.05.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Culp D J, Robinson B, Parkkila S et al. Oral colonization by Streptococcus mutans and caries development is reduced upon deletion of carbonic anhydrase VI expression in saliva. Biochim Biophys Acta. 2011;1812(12):1567–1576. doi: 10.1016/j.bbadis.2011.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hannig M, Hannig C. Nanomaterials in preventive dentistry. Nat Nanotechnol. 2010;5(08):565–569. doi: 10.1038/nnano.2010.83. [DOI] [PubMed] [Google Scholar]
- 49.Khurshid Z, Zafar M, Qasim S, Shahab S, Naseem M, AbuReqaiba A. Advances in nanotechnology for restorative dentistry. Materials (Basel) 2015;8(02):717–731. doi: 10.3390/ma8020717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Kanaparthy R, Kanaparthy A. The changing face of dentistry: nanotechnology. Int J Nanomedicine. 2011;6:2799–2804. doi: 10.2147/IJN.S24353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Subramani K, Ahmed W, Hartsfield J K. 2012. Nanobiomaterials in Clinical Dentistry. [Google Scholar]
- 52.Cicciù M, Cervino G, Terranova A et al. Prosthetic and mechanical parameters of the facial bone under the load of different dental implant shapes: a parametric study. Prosthesis. 2020;1:41–53. [Google Scholar]
- 53.Cicciù M. Prosthesis: new technological opportunities and innovative biomedical devices. Prosthesis. 2020;1:1–2. [Google Scholar]
- 54.Crimi S, Fiorillo L, Bianchi A et al. Herpes virus, oral clinical signs and QoL: systematic review of recent data. Viruses. 2019;11(05):463. doi: 10.3390/v11050463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Zhang N, Zhang K, Xie X et al. Nanostructured polymeric materials with protein-repellent and anti-caries properties for dental applications. Nanomaterials (Basel) 2018;8(06):393. doi: 10.3390/nano8060393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Guazzo R, Gardin C, Bellin G et al. Graphene-based nanomaterials for tissue engineering in the dental field. Nanomaterials (Basel) 2018;8(05):349. doi: 10.3390/nano8050349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Troiano G, Laino L, Cicciù M et al. Comparison of two routes of administration of dexamethasone to reduce the postoperative sequelae after third molar surgery: a systematic review and meta-analysis. Open Dent J. 2018;12:181–188. doi: 10.2174/1874210601812010181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Laino L, Cicciù M, Fiorillo L et al. Surgical risk on patients with coagulopathies: guidelines on hemophiliac patients for oro-maxillofacial surgery. Int J Environ Res Public Health. 2019;16(08):1386. doi: 10.3390/ijerph16081386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Fiorillo L, De Stefano R, Cervino G et al. Oral and psychological alterations in haemophiliac patients. Biomedicines. 2019;7(02):33. doi: 10.3390/biomedicines7020033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Cervino G, Fiorillo L, Monte I P et al. Advances in antiplatelet therapy for dentofacial surgery patients: focus on past and present strategies. Materials (Basel) 2019;12(09):1524. doi: 10.3390/ma12091524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Herford A S, Lu M, Akin L, Cicciù M. Evaluation of a porcine matrix with and without platelet-derived growth factor for bone graft coverage in pigs. Int J Oral Maxillofac Implants. 2012;27(06):1351–1358. [PubMed] [Google Scholar]
- 62.Sambataro S, Cervino G, Bocchieri S, La Bruna R, Cicciù M. TMJ dysfunctions systemic implications and postural assessments: a review of recent literature. J Funct Morphol Kinesiol. 2019;4:58. doi: 10.3390/jfmk4030058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Sambataro S, Bocchieri S, Cervino G et al. Correlations between malocclusion and postural anomalies in children with mixed dentition. J Funct Morphol Kinesiol. 2019;4:45. doi: 10.3390/jfmk4030045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Cicciù M, Risitano G, Lo Giudice G, Bramanti E. Periodontal health and caries prevalence evaluation in patients affected by Parkinson’s disease. Parkinsons Dis. 2012;2012:541908. doi: 10.1155/2012/541908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Cicciù M, Bramanti E, Cecchetti F, Scappaticci L, Guglielmino E, Risitano G. FEM and Von Mises analyses of different dental implant shapes for masticatory loading distribution. Oral Implantol (Rome) 2014;7(01):1–10. [PMC free article] [PubMed] [Google Scholar]
- 66.Cicciù M, Beretta M, Risitano G, Maiorana C. Cemented-retained vs screw-retained implant restorations: an investigation on 1939 dental implants. Minerva Stomatol. 2008;57(04):167–179. [PubMed] [Google Scholar]
- 67.Algarni A A, Mussi M C, Moffa E B et al. The impact of stannous, fluoride ions and its combination on enamel pellicle proteome and dental erosion prevention. PLoS One. 2015;10(06):e0128196. doi: 10.1371/journal.pone.0128196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Rodríguez-Lozano F J, López-García S, García-Bernal D et al. In vitro effect of putty calcium silicate materials on human periodontal ligament stem cells. Appl Sci. 2020;10(01):325. [Google Scholar]
- 69.Tatullo M, Spagnuolo G, Codispoti B et al. PLA-based mineral-doped scaffolds seeded with human periapical cyst-derived MSCs: a promising tool for regenerative healing in dentistry. Materials (Basel) 2019;12(04):E597. doi: 10.3390/ma12040597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Spagnuolo G, Codispoti B, Marrelli M, Rengo C, Rengo S, Tatullo M. Commitment of oral-derived stem cells in dental and maxillofacial applications. Dent J (Basel) 2018;6(04):E72. doi: 10.3390/dj6040072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.de Oliveira N G, de Souza Araújo P R, da Silveira M T, Sobral A PV, Carvalho M V. Comparison of the biocompatibility of calcium silicate-based materials to mineral trioxide aggregate: systematic review. Eur J Dent. 2018;12(02):317–326. doi: 10.4103/ejd.ejd_347_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Ferreira M M, Botelho M F, Abrantes M, Carvalho L, Carrilho E. Histologic evaluation of the effect of mineral trioxide aggregate-Fillapex as a root canal sealer in rat teeth submitted to late replantation. Eur J Dent. 2017;11(01):89–93. doi: 10.4103/ejd.ejd_106_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Scrascia R, Fiorillo L, Gaita V, Secondo L, Nicita F, Cervino G. Implant-supported prosthesis for edentulous patient rehabilitation. From temporary prosthesis to definitive with a new protocol: a single case report. Prosthesis. 2020;2(01):10–24. [Google Scholar]
- 74.Ortensi L, Vitali T, Bonfiglioli R, Grande F. New tricks in the preparation design for prosthetic ceramic laminate veeners. Prosthesis. 2019;1(01):29–40. [Google Scholar]
- 75.Lee D S, Lim M J, Choi Y, Rosa V, Hong C U, Min K S. Tooth discoloration induced by a novel mineral trioxide aggregate-based root canal sealer. Eur J Dent. 2016;10(03):403–407. doi: 10.4103/1305-7456.184165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Bayram E, Bayram H M. Fracture resistance of immature teeth filled with mineral trioxide aggregate, bioaggregate, and Biodentine. Eur J Dent. 2016;10(02):220–224. doi: 10.4103/1305-7456.178310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Akcay H, Arslan H, Akcay M, Mese M, Sahin N N. Evaluation of the bond strength of root-end placed mineral trioxide aggregate and Biodentine in the absence/presence of blood contamination. Eur J Dent. 2016;10(03):370–375. doi: 10.4103/1305-7456.184150. [DOI] [PMC free article] [PubMed] [Google Scholar]