

1. INTRODUCTION
CORONA‐19 pandemic is caused by SARS‐CoV‐2 virus. It began towards the end of 2019 in China, and soon became a worldwide epidemic, more than more than 649 000 people died and 16 million cases were accounted by 26 July 2020 (https://www.worldometers.info/coronavirus/). The disease generally starts like sore throat, continue with cough, dyspnea and fever, and then may affect the entire body and may eventually kill the patient. Scientists are trying to find medication for its treatment, but it seems like a faraway target at the moment. COVID‐19 pathogenesis may cause aggressive inflammatory response in the airways, may damage the airways and the alveoli, in the lungs, and make carbon dioxide and exchange difficult (Figure 1), as a result the metabolism of the patient can not provide sufficient energy to support the life processes.
FIGURE 1.
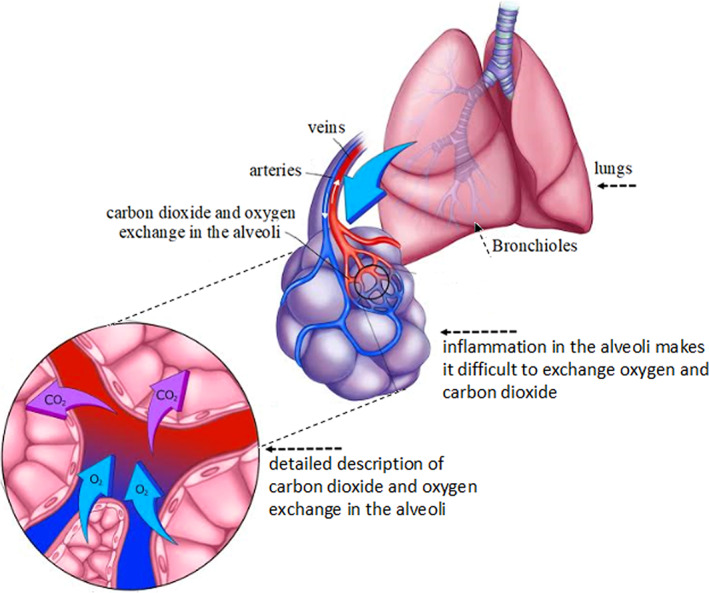
COVID‐19 inflammation in the lungs, at the alveoli, makes CO2 and O2 exchange difficult, as a result rate of the metabolism decreases [Colour figure can be viewed at wileyonlinelibrary.com]
2. THE ENERGY BUDGET
In order to maintain a healthy life, energy supplied by the energy metabolism must be sufficient to meet the expenses for the life processes (Figure 2). Movement, circulation, respiration, excretion, growth, nutrition, nervous and endocrine control systems are called the life‐processes in the literature, they represent the expenses and are achieved by the allocation of appropriate levels of energy for all of them. If the metabolism of the person provides sufficient energy to fulfill the life processes, he/she may be called a “healthy” person. Inflammation of the lung tissue disturbs this process, and depending on the deficiency of the oxygen supply, as a result ATP production via metabolic activity will decrease. ATP is the energy currency of the cells and produced in the metabolism in two stages (Figure 3): Reaction (1) occurs in the cytoplasm,
| (1) |
and reaction (2) occurs in the mitochondria:
| (2) |
FIGURE 2.
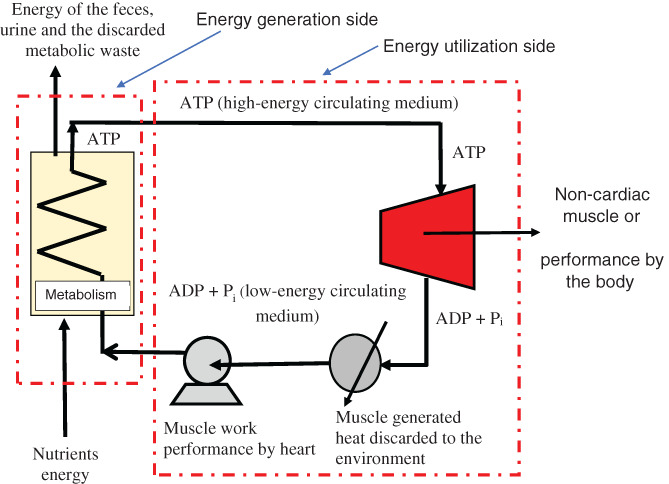
Schematic description of energy (ATP) generation and utilization in the human body. ADP + Pi are converted into ATP via metabolic activity by utilizing the energy extracted from the nutrients. When the metabolism and is capable of producing sufficient amounts of ATP, the body of the person may utilize it to fulfil the life processes [Colour figure can be viewed at wileyonlinelibrary.com]
FIGURE 3.
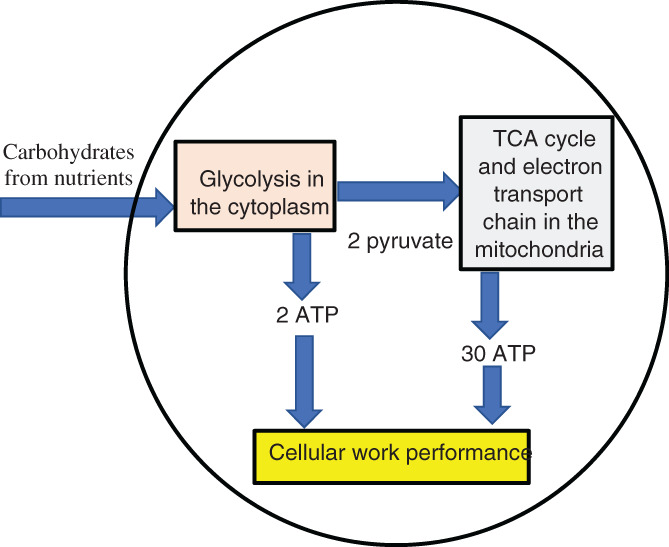
Schematic description of energy (ATP) generation and utilization in the cells [Colour figure can be viewed at wileyonlinelibrary.com]
As it is clearly seen here that, it is possible to produce two moles of ATP from one mole of glucose via reaction (1) and twenty‐eight moles of ATP from two moles of PYR (pyruvate). PYR, which is produced in the cytoplasm is then transported to mitochondria for further processing in the tri‐carboxylic acid cycle and electron transport chain. When we look at reactions (1) and (2), we see that less than 10% of the total ATP is produced in the cytoplasm and more than 90% is produced in the mitochondria. In addition to serving as the part of the cellular energy generation, the tri‐carboxylic acid cycle also serves for producing intermediaries for the cellular chemical synthesis. In the life processes of the pregnant mice, Semerciöz et al. 1 determined that 27.8% of the metabolites are withdrawn from the tricarboxylic acid cycle to be used for synthesis of the cellular constituents. ATP is delivered to the locations of the cell where energy is needed, it is hydrolyzed in accordance with reaction (3) to produce ADP and organic phosphate and as a result, 30.5 kJ/mol ATP of energy may be released:
| (3) |
Chemical reactions which need energy to occur are coupled with reaction (3), since they would never occur otherwise. When aerobic respiration, as described by reaction (2) cannot occur, because of the lack of sufficient oxygen supply to the muscles, a fraction of pyruvic acid is removed from the metabolism after being converted into lactic acid. In general, lactic acid accumulates in the muscle cells when sufficient oxygen is not supplied to the muscles during heavy exercise. Lactic acid accumulation is perceived as pain in case of COVID‐19 disease.
3. ENERGY DEFICIENCY IN COVID‐19 DISEASE
Energy deficiency, which may occur as a result of COVID‐19 disease is described in Figure 4. COVID‐19 makes it very difficult to provide the energy needed for the life processes, because of the deficit of O2. COVID‐19 patients may be transferred to a respiratory unit, where higher pressures of oxygen are applied to compensate for the increased resistance to oxygen transport in the lungs. 2 In the respiratory unit, pressure of oxygen cannot exceed three times of the partial pressure of the oxygen of the air, otherwise the lungs may be damaged. Impact of the COVID‐19 disease may be assessed in five levels. At the highest impact, patients may be found positive, but recover without any symptoms or clinical signs. COVID‐19 patients who has the most severe symptoms, may have difficulty in respiration, experience misfunctioning of multiple organs and shock. Patients who experience severe symptoms are usually provided with higher oxygen supply, up to 300% of the partial pressure of oxygen in the air.
FIGURE 4.
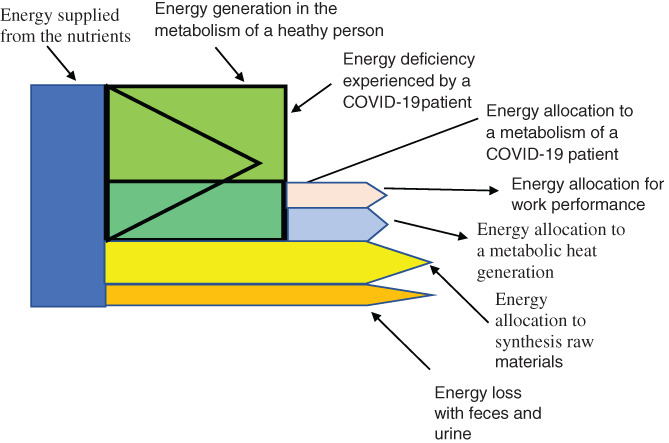
Distribution of the energy extracted from the nutrients for the life processes of a healthy person and the energy deficiency caused after the decrease of the rate of metabolism due to the COVID‐19 disease (not in scale) [Colour figure can be viewed at wileyonlinelibrary.com]
If a patient has high body temperature, exergetic or energetic rates of his/her metabolism increases by 10% to sustain the energy requirement. Patient needs to compensate this energy requirement by cutting it from those of the life processes. Viral infections, after starting controlling the metabolism of the patients, change the energy and material reserve allocations to maximize their interests. 3 At the initial stages, the disease utilizes the energy of the nutrients, and in the later stages it scavenges the healthy tissues while abusing the metabolism of the patient. Distortion of the energy management is observed in various health problems, including cancer 4 and heart failure. 5 A disease may start scavenging the healthy tissues when it reaches to a vigorous level (Figure 5) to provide raw material and energy to establish the changes associate with the disease.
FIGURE 5.
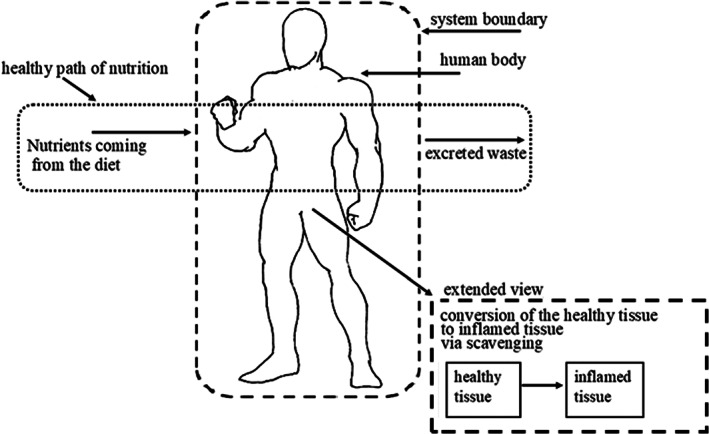
Allocation of the exergy or energy of the nutrients the scavenged tissue in the body of a diseased person
4. ENTROPIC CHANGES IMPOSED BY THE DISEASE
A fraction of the nutrition and the disease related entropy generation in cancer patients were reported by Öngel et al 6 ; while the nutrition related entropy generation rate was 19 kJ/kg K year, the disease related entropy generation was 9‐folds of that in skin cancer and 191‐folds of it in lung cancer. The rate of exergy destruction, , is expressed in terms of the entropy generation rate as with the expression , where Tb is the temperature of the patient. When the body temperature of the patient is 37.5°C, in addition to 16.2 kJ/day of exergy destruction in the nutrition‐related metabolic activity, the patient needs to provide 145.4 kJ/day of exergy to compensate the disease related exergy destruction in skin cancer and 3087 kJ/day of exergy to compensate the disease related exergy destruction in lung cancer. When metabolic activity of a patient decreases by 33%, the exergetic deficiency experienced by the COVID‐19 patient would be 0.46 W/kg, 2 corresponding to 2779 MJ/day in a 70 kg patient and in a more severe case when metabolic activity decreases by 66%, this would be 5558 MJ/day. In the more severe case, the exergetic cost of COVID‐19 to a patient with skin cancer would be 5558 + 145.4 = 5703 MJ/day and it will be 5558 + 3087 = 8645 MJ/day in the case of lung cancer. If the patient has fever, exergy requirement may increase by approximately 10%. Every disease may affect the exergy need of a person in a similar way. When the patient will not be able provide the needed exergy, he/she would die.
5. CLOSING REMARKS
Like several other health problems, COVID‐19 disease is associated with the difficulty of keeping balance energy budget in the body. As the energy budget worsen, patient tries to balance the budget by scavenging building blocks and energy from the healthy tissues. When the budget becomes unmanageable the patient dies. The disease may be more fatal for the elder patients, both because they may have additional health problems or also because they may have a slower energy metabolism, or their metabolism may produce at a slower rate.
Özilgen M, Yilmaz B. COVID‐19 disease causes an energy supply deficit in a patient. Int J Energy Res. 2021;45:1157–1160. 10.1002/er.5883
REFERENCES
- 1. Semerciöz AS, Yılmaz B, Özilgen M. Thermodynamic assessment of the allocation of the energy and exergy of the nutrients for the life processes during pregnancy. B. J Nutr. 2020;127(7):742‐753. 10.1017/S0007114520001646. [DOI] [PubMed] [Google Scholar]
- 2. Yılmaz B, Ercan S, Akduman S, Özilgen M. Energetic and exergetic costs of COVID‐19 infection on the body of a patient. Int J Exergy. 2020;32(3):314‐327. [Google Scholar]
- 3. Thaker SK, Ch'ng J, Christofk HR. Viral hijacking of cellular metabolism. BMC Biol. 2019;1(59). 10.1186/s12915-019-0678-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Garland J. Energy management‐ a critical role in cancer induction. Crit Rev Oncol Hemat, 2013. 2013;88(1):198‐217. [DOI] [PubMed] [Google Scholar]
- 5. Barclay CJ. Getting energy to where it is needed is the problem in the failing heart. J Physiol, 2016. 2008;586(21):5037‐5038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Öngel ME, Yıldız C, Özilgen M, Yılmaz B. Nutrition and disease‐related entropy generation in cancer. Int J Exergy, 2020: in press.