

Abstract
Objective
The COVID‐19 outbreak in Italy caused a major health emergency and high uncertainty. We studied how media outlets, risk perception, state anxiety, and emotion regulation impacted peoples’ reactions and undertaking of protective behaviours aimed at reducing the spread of the virus.
Design
Data were collected in two cross‐sectional waves (N = 992 at T1; N = 1031 at T2): at the beginning of the outbreak and once the national lockdown was imposed.
Methods
Participants completed online surveys on their perception of the COVID‐19 outbreak. Moreover, they were asked to self‐report on their emotion regulation, state anxiety, and protective behaviours.
Results
Media exposure and wave predicted risk perception. An interaction between wave, risk perception, and emotion regulation predicted the number of protective behaviours people undertook. Specifically, in the second wave, the number of protective behaviours was predicted by risk perception only among those who were ineffective at regulating emotions. Instead, effective regulators undertook the same number of behaviours regardless of their level of risk perception. In the second wave, we also found that the risk perception by emotion interaction predicting protective behaviours was mediated by state anxiety.
Conclusions
The present study provides important insights on how people experienced the early stages of the outbreak. This information could prove valuable in the coming months to understand who might have been more impacted by the stress caused by the COVID‐19 pandemic and the consequent restrictive measures.
Keywords: COVID‐19, risk perception, emotion regulation, protective behaviour
Statement of contribution.
What is already known on this subject?
-
●
Media exposure is associated with increased risk perception of COVID‐19.
-
●
People show resistance to the protective measures enacted to contain the virus spread.
-
●
Risk perception predicts increased compliance with protective measures.
What does this study add?
-
●
Risk perception increased once the countrywide lockdown was enforced.
-
●
Emotion regulation moderated the association between risk perception and compliance with protective behaviours.
-
●
At the start of the lockdown, state anxiety mediated the association between risk perception and protective behaviours.
Italy was probably the first Western country to face an outbreak of the new coronavirus. The first case was registered on 23 February, and since then, the numbers increased exponentially causing many deaths and a huge health emergency. Since these early stages, people underwent more and more strict containment measures that led to a complete lockdown of the country (Governo Italiano Presidenza del Consiglio dei Ministri, 2020). This unprecedented health crisis drew the attention of all the media that for weeks were solely focused on the development of the pandemic in terms of health issues and government responses. The increasing severity of the situation (Grasselli, Pesenti, & Cecconi, 2020) together with the huge media coverage (Zarocostas, 2020) was likely to be matched by an increase in people’s risk perception (Schmälzle, Häcker, Renner, Honey, & Schupp, 2013). For instance, recent data from the United States showed that people who looked to the news more (vs. less) experienced higher perceived vulnerability and, in turn, more depressive symptoms (Olagoke, Olagoke, & Hughes, 2020). Therefore, the media and other environmental factors may have a relevant impact on how people experienced the virus outbreak and the subsequent restrictions.
Italian citizens were asked to accept severe restrictions to their freedom and to comply with a wide range of behaviours intended to protect them and reduce the spread of the virus. However, there were large differences in how people respected these directives. Consistent with the Italian experience, data from the United Kingdom showed that some of the factors leading to face mask wearing are the following: age, gender, where a person lives (urban environment or not), existing health issues, depression, stress, and anxiety (Shevlin et al., 2020). Furthermore, the degree of compliance with these behaviours could have had a potentially significant impact on when the peak of cases was reached (Fisher, & Wilder‐Smith, 2020). As a consequence, the government was forced to repeatedly tighten the rules and the controls in the streets.
The psychological literature shows that risk perception and people’s behaviours at large are significantly impacted by the way they feel about something. Slovic and colleagues proposed the affect heuristic to explain how emotions can influence people’s reactions (Slovic, Finucane, Peters, & MacGregor, 2004). This heuristic suggests that people attach an emotional value to the stimuli and events in their lives. As a result, they approach things that elicit positive affective reactions and tend to avoid those that elicit negative affective reactions. To complicate things further, the COVID‐19 pandemic is characterized by a high degree of uncertainty since some patients can be asymptomatic and even science lacks the tools to fight it (e.g., a vaccine). According to research in risk perception, these are characteristics that lead to a sense of dread and anxiety (Slovic, 1987) that need to be regulated in order to avoid irrational responses. As a result, it is likely that people who are more (vs. less) effective at regulating their emotions would be able to comply with the restrictions regardless of how they are feeling about the virus outbreak and for a longer time. Consistently, people who perceive a high risk of being infected by the virus should be more willing to use a mask or avoid unnecessary social activities (e.g., meetings or travels). As a result, these people will end up following more closely the restrictions and protective actions imposed by the government. This prediction is consistent with recent work showing that one of the factors leading to face mask wearing is indeed a heightened risk perception (Shevlin et al., 2020).
Further, based on the important role emotions have in shaping how people perceive risk, in the present study, we tested whether, during the COVID‐19 outbreak, emotion regulation could moderate the relationship between people’s reactions and their behaviours (Cohen, & Ochsner, 2018; Eippert et al., 2007). Some people are better prepared to identify and deal with their emotions and to regulate the way emotions impact their behaviours. As a result, they are better at adjusting to changes and responding to challenges, something that has a direct impact on their well‐being (Hu et al., 2014).
Given the characteristics of the pandemic, we assessed how emotion regulation, the amount of exposure to media outlets, and the number of cases were related to people’s risk perception, and in turn the protective behaviours they undertook. Although people may think that watching more news and accruing information can lead to a sense of control and reduce the feeling of threat, the opposite is often true. Recent work showed that this is what happened to many during the spread of COVID‐19 since the media often focused on the number of people who died or were infected (Van Bavel et al., 2020; Wise, Zbozinek, Michelini, Hagan, & Mobbs, 2020).
In addition, we measured the relation between these variables at two crucial time points: immediately after the outbreak of the virus in Italy (wave 1) and as soon as the countrywide lockdown was imposed by the government (wave 2). Major health crises and worldwide disasters may have devastating effects on physical and psychological well‐being (Cohen Silver et al., 2013; Rajkumar, 2020), not to mention the economic impacts they can have on people’s lives. Moreover, Lades et al. (2020) showed that during the COVID‐19 pandemic people’s well‐being was related to how they were able to spend their time. In Italy, when the virus outbreak started people were still able to leave their homes and meet with friends, two activities that have a positive impact on well‐being (Lades, Laffan, Daly, & Delaney, 2020), whereas after the lockdown they had to stay home, and outdoor activities were severely restricted. As a result, it is important to understand the role that emotion regulation could play in relation to how people reacted to the virus outbreak.
Specifically, we expected that:
Hypothesis 1
Watching more news should make the threat of coronavirus more vivid and, as a result, increase risk perception.
Hypothesis 2
Risk perception should be higher in wave 2 (after the start of the lockdown) than in wave 1.
Regarding the protective behaviours, many of the actions required to keep the spread of the coronavirus under control were met with some resistance by people (Giuffrida & Cochrane, 2020). As a result, in wave 2 (vs. wave 1) and when risk perception is high (vs. low), people should be more willing to undertake these actions and abide by government instructions. This would be consistent with prior data showing that risk perception is an important predictor of protective behaviour in a pandemic (see, Bish & Michie, 2010). Critically, we expect to find a moderating role of emotion regulation. When emotion regulation is low, people should use the level of risk perception as a cue to guide their behaviour. If risk perception is high and people feel threatened by the virus outbreak, they should undertake more protective behaviours, despite the ensuing discomfort and restriction to their freedom; in contrast, if risk perception is low, the annoyance of being limited by the restrictions should lead these people to undertake fewer protective actions. This prediction is consistent with the affect heuristic and the role of emotion in decision‐making (Slovic et al., 2004). The impact of risk perception should be much smaller when people have good emotion regulation. These people should be able to abide by externally enforced restrictions even when not feeling under risk and despite the inconvenience that could arise. This is consistent with prior work showing that these people can detach from their emotional reactions and deal with conditions that induce stress or pose them a challenge (Petrides, Niven, & Mouskounti, 2006; Sevdalis, Petrides, & Harvey, 2007). Thus:
Hypothesis 3
After the start of the lockdown, high (vs. low) risk perception should lead to undertake more protective behaviours, but only for people who have low (vs. high) emotion regulation.
Finally, in wave 2, given the overall increase in the number of cases and deaths, we assessed whether the above factors predicted people’s state anxiety in the midst of the coronavirus crisis. Specifically, based on the classical stress model proposed by Lazarus and Folkman (1984) we tested a mediation model. In the classic stress model, the recognition of the threat, for example in terms of risk perception, initiates a process that includes an emotional response, potentially an anxious one, to end with the enacting of a behaviour. Here, we assessed the role of anxiety as a mediator of the relation between risk perception and protective behaviours.
Thus:
Hypothesis 4
People with high (vs. low) risk perception should experience more (vs. less) state anxiety. In turn, state anxiety should mediate the association between risk perception and protective behaviours in wave 2.
Method
Participants
For the current study, 3,282 participants were recruited in a repeated cross‐sectional design, during two temporally different data collections (wave 1: N = 1603, 67.64% female, mean age 30.95 years ranging from 18 to 72; wave 2: N = 1679, 67.99% female, mean age 30.63 years ranging from 18 to 75). At each wave, following the initial data acquisition, participants who were not answering from Italy and were younger than 18 years old were excluded. Only fully completed surveys were included in the analyses. Hence, wave 1 includes 992 participants, while wave 2 includes 1,031 participants. Full information about the participants and a comparison between the wave 1 and wave 2 samples are provided in Table 1.
Table 1.
Characteristics of the participants and response to main survey items in the two waves of the study a
| Characteristics | Wave 1 (N = 992) | Wave 2 (N = 1031) | Difference |
|---|---|---|---|
| Age, year (range) | 30.95 (18–72) | 30.63 (18–75) | 0.566 |
| Gender | |||
| Female, no. (%) | 671 (67.64%) | 701 (67.99%) | 0.148 |
| Highest level of education | |||
| Primary school, no. (%) | 0 (0%) | 1 (0.09%) | 0.679 |
| Middle school, no. (%) | 36 (3.63%) | 50 (4.85%) | |
| High school, no. (%) | 427 (43.04%) | 460 (44.62%) | |
| Bachelor’s degree, no. (%) | 333 (33.57%) | 303 (29.39%) | |
| Master’s degree, no. (%) | 170 (17.14%) | 187 (18.14%) | |
| Specialization/Doctorate, no. (%) | 26 (2.62%) | 30 (2.91%) | |
| Income | |||
| >10,000 (%) | 75 (7.56%) | 65 (6.30%) | 0.043 |
| 10,000–19,999 (%) | 180 (18.15%) | 190 (18.43%) | |
| 20,000–29,999 (%) | 12 (1.21%) | 9 (0.87%) | |
| 30,000–39,999 (%) | 239 (24.09%) | 260 (25.22%) | |
| 40,000–49,999 (%) | 144 (14.52%) | 153 (14.84%) | |
| 50,000–59,999 (%) | 83 (8.37%) | 93 (9.02%) | |
| 60,000–69,999 (%) | 49 (4.94%) | 50 (4.85%) | |
| 70,000–79,999 (%) | 29 (2.92%) | 29 (2.81%) | |
| 80,000–89,999 (%) | 28 (2.82%) | 27 (2.62%) | |
| 90,000–99,999 (%) | 14 (1.41%) | 17 (1.65%) | |
| 100,000–109,999 (%) | 4 (0.40%) | 3 (0.29%) | |
| 110,000–119,999 (%) | 10 (1.01%) | 7 (0.68%) | |
| 120,000–129,999 (%) | 3 (0.30%) | 3 (0.29%) | |
| 130,000–139,999 (%) | 1 (0.10%) | 3 (0.29%) | |
| 140000–149,999 (%) | 2 (0.20%) | 0 (0%) | |
| >150,000 (%) | 3 (0.30 %) | 1 (0.10%) | |
| Prefer not to say (%) | 116 (11.70%) | 121 (11.74%) | |
| Political orientation | |||
| Extreme left wing, no. (%) | 23 (2.32%) | 26 (2.52%) | 2.473* |
| Left wing, no. (%) | 273 (27.52%) | 285 (27.64%) | |
| Centre‐left wing, no. (%) | 273 (27.52%) | 335 (32.50%) | |
| Centre wing, no. (%) | 151 (15.22%) | 152 (14.74%) | |
| Centre‐right wing, no. (%) | 144 (14.52%) | 142 (13.77%) | |
| Right wing, no. (%) | 117 (11.79%) | 85 (8.25%) | |
| Extreme right wing, no. (%) | 11 (1.11%) | 6 (0.58%) | |
| Religiosity, 7‐points scale (SD) | 2.927 (1.78) | 2.944 (1.824) | 0.204 |
| Trust authorities, 1–7 scale (SD) | 3.957 (1.415) | 4.250 (1.357) | 4.765*** |
| Symptoms reported in the last 48 hours | |||
| Coughing, no. (%) | 205 (20.67%) | 176 (17.07%) | 4.273* |
| Runny nose, no. (%) | 313 (31.55%) | 283 (27.45%) | 4.096* |
| Fever, no. (%) | 32 (3.23%) | 17 (1.65%) | 5.319* |
| General malaise, no. (%) | 143 (14.42%) | 123 (11.93%) | 2.734 |
| Sore throat, no. (%) | 122 (12.30%) | 123 (11.93%) | 0.064 |
| Headache, no. (%) | 290 (29.23%) | 257 (24.93%) | 4.752* |
| Media exposure | |||
| Social media (%) | 344 (34.70%) | 503 (48.80%) | 41.36*** |
| National newspapers (%) | 443 (44.70%) | 582 (56.50%) | 28.13*** |
| Local newspapers (%) | 228 (23.00%) | 342 (33.20%) | 25.93*** |
| Press agencies (%) | 151 (15.20%) | 259 (25.10%) | 30.66*** |
| Newscasts (%) | 566 (57.10%) | 747 (72.50%) | 52.62*** |
| Shows on TV (%) | 186 (18.80%) | 317 (30.70%) | 38.95*** |
| National health bureau (%) | 525 (52.90%) | 677 (65.70%) | 34.04*** |
| WHO (%) | 378 (38.10%) | 460 (44.60%) | 8.84** |
| Scientific journals (%) | 93 (9.40%) | 142 (13.80%) | 9.53** |
| Protective behaviours | |||
| Bought a face mask (%) | 63 (6.40%) | 288 (27.90%) | 164.23*** |
| Called the doctor (%) | 39 (3.90%) | 75 (7.30%) | 10.63** |
| Washed hands more often (%) | 663 (66.80%) | 921 (89.30%) | 150.58*** |
| Cancelled meeting (%) | 423 (42.60%) | 897 (87.00%) | 438.79*** |
| Cancelled travel plans (%) | 196 (19.80%) | 550 (53.30%) | 245.03*** |
The table reports the following statistics: t test for age, education, income, political orientation, religiosity, and trust in authorities; chi‐square for gender, each of the symptoms, each of the media sources included in the media exposure measure, and each of the behaviours included in the protective behaviours measure.
Compared to the general Italian population in our sample, participants were younger (mean for the Italian population = 45.70), there were more females (Italian population = 51.29%), whereas the mean income was similar (Italian population = 31,393 Euros).
p < .05; **p < .01; ***p < .001.
Materials and procedure
The first wave of data collection was posted online between 24 February and 29 February 2020, when the virus outbreak in Italy had just begun, and the first deaths were recorded in the Veneto and Lombardy regions. The second wave of data collections was posted online between 10 March and 20 March 2020 immediately after the Italian government enacted a full country lockdown. Both surveys followed the same posting procedures.1 and were disseminated on social media platforms (e.g., Facebook) and through instant messaging (e.g., WhatsApp) to collect data on risk perception and behaviours undertaken to avoid virus contagion. Facebook posts were shareable to facilitate snowball sampling and instant messaging also included groups with the specific request to share the survey. Informed consent was obtained from all participants who were informed of the purpose, risks, and benefits of the study.
In addition to demographic data, participants were asked about recent cold and flu‐like symptoms (i.e., coughing, runny nose, fever, general malaise, sore throat, and headache). Other questions addressed media exposure to information related to COVID‐19 (e.g., social media, national newspapers, local newspapers, press agencies, newscasts, TV programs, health bureau communications, WHO, scientific journals), whereas participants’ risk perception was measured with a single item asking participants to rate how high they perceived the risk of contracting COVID‐19 (see full materials in the Appendix 1). In addition, participants were asked to complete the trait emotional intelligence questionnaire (TEIQue‐SF; α = .88; Petrides, 2009). The TEIQue‐SF includes 30 items measuring people’s emotion regulation and experience. Participants answer each item on a 7‐point scale ranging from 1 (‘completely disagree’) to 7 (‘completely agree’). State anxiety was measured, in wave 2, by way of the State‐Trait Anxiety Inventory (STAI; α = .65; Spielberg, 1983). The state subscale of STAI includes 20 items measuring whether people experienced a series of emotional reactions recently. Participants answer each item on a 4‐point scale ranging from 1 (‘almost never’) to 4 (‘almost always’). Finally, we kept track of the number of infected cases recorded per million Italian citizens on the days in which the two surveys were posted online. The dependent variable of our study was the protective behaviours that people reported to have undertaken around the time they answered the surveys (see Table 1).
Data analysis
Mainly we ran multiple regression analyses with a backward model selection procedure. The decision of using an exploratory approach in the analysis was due to the lack of literature studying how the variables of interest could be associated with people’s reactions and behaviours during a pandemic. Specifically, we used the Akaike information criterion (AIC) model comparison to compare sets of candidate models fitted to the same data using the step AIC function in R (Akaike, 1973; McElreath, 2016). The biggest advantage of this approach is the selection of the most plausible model and ranking and weighting of the remaining models in a pre‐defined set (Burnham, Anderson, & Huyvaert, 2011). Results were interpreted in terms of AIC, Akaike weights, significance, size of coefficients, and explained variance. Generally, smaller AIC values are indicators of a more parsimonious model. Finally, we ran a mediation analysis using the R software and the ‘lavaan’ package (Rosseel, 2012) to assess whether state anxiety mediated the relation between the variables of interest and the protective behaviours in wave 2.
Results
Descriptive statistics and correlations
Descriptive statistics showed that, consistent with the trend of the epidemic and the restrictive measures put in place by the government, risk perception was higher in the second wave than in the first (Table 2). Similarly, in the second wave (vs. the first), people attended to more news outlets and undertook more protective behaviours.
Table 2.
Descriptive statistics and differences between wave 1 and wave 2 for the main study variables
| Wave 1 | Wave 2 | t | d | 95% C.I. | |||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | Range | M | SD | Range | ||||
| Emotion reg. | 4.91 | .73 | 2.43–6.80 | 4.88 | .75 | 2.13–6.83 | −.85 | .04 | [−0.04, 0.09] |
| Risk perception | 41.94 | 26.88 | 0–100 | 66.33 | 23.66 | 0–100 | −21.69*** | .96 | [−26.60, −22.19] |
| Media exposure | 2.59 | 1.49 | 0–8 | 3.42 | 1.58 | 0–8 | −12.13*** | .54 | [−0.96, −0.70] |
| Behaviours | 1.40 | 1.01 | 0–5 | 2.65 | .98 | 0–5 | −28.39*** | 1.26 | [−1.34, −1.17] |
| Cases per million | 4.41 | 2.09 | 2.18–14.69 | 211.93 | 88.01 | 121.98–590.67 | −74.24*** | 3.33 | [−.212.99, −202.03] |
p < .05; **p < .01; ***p < .001.
We then checked the correlations among the study variables. Results showed some differences between the first and second wave (Table 3). In the first wave, risk perception correlated, positively only with the number of protective behaviours participants undertook to avoid being infected, whereas in the second wave, it correlated positively with behaviours as well as media exposure and the actual rate of infected cases per million Italian citizens. In addition, media exposure was positively correlated with the number of protective behaviours.
Table 3.
Correlations between the main study variables split by wave (wave 1 in the bottom left side and wave 2 in the top right side of the correlation matrix)
| Wave 2 | ||||||
|---|---|---|---|---|---|---|
| Emotion reg. | Risk perception | Media exposure | Behaviours | Cases per million | ||
| Wave 1 | ||||||
| Emotion reg. | ‐‐‐ | −.04 | .02 | .08** | −.03 | |
| Risk perception | −.01 | ‐‐‐ | .08** | .18*** | .13*** | |
| Media exposure | .03 | .05 | ‐‐‐ | .15*** | .00 | |
| Behaviours | .00 | .20*** | .14*** | ‐‐‐ | .11*** | |
| Cases per million | .02 | .05 | −.01 | −.03 | ‐‐‐ | |
p < .05; **p < .01; ***p < .001.
Risk perception
To assess which factors predicted risk perception, we ran a backward model selection analysis with a starting model that included emotion regulation, media exposure, wave, their two‐way and the three‐way interactions, while controlling for age, trust in authorities, political orientation, income, education, and rate of cases per a million inhabitants. The final and most plausible model (AdjR 2 = .20, p < .001, AIC baseline = 13050.42; AIC model = 13038.29) included only the main effects of media exposure (β = .07, B = 1.52, SE = .36, t = 3.19, p = .001, 95% C.I. [0.45, 1.87]), wave (β = .29, B = 16.37, SE = 2.17, t = 7.53, p < .001, 95% C.I. [12.11, 20.63]), political orientation (β = .08, B = 1.56, SE = .40, t = 3.88, p < .001, 95% C.I. [0.77, 2.35]), and rate of cases per a million inhabitants (β = .15, B = .04, SE = .01, t = 3.97, p < .01, 95% C.I. [0.02, 0.05]).
Protective behaviours
To test which factors predicted the number of protective behaviours undertaken by participants, we ran a backward model selection analysis. We started from a fully saturated model with a four‐way interaction between emotion regulation, media exposure, wave, and risk perception, while controlling for the same covariates as in the previous model. The final and most plausible model is reported in Table 4. The key finding of this analysis is a significant three‐way interaction between emotion regulation, wave, and risk perception. We probed the interaction by way of a slope analysis. In the first wave, regardless from the level of risk perception, emotion regulation never predicted behaviours (p = .40 or higher). In the second wave, risk perception moderated the relationship between emotion regulation and protective behaviours. As risk perception increased the correlation between emotion regulation and behaviours decreased. Specifically, a Neyman–Johnson analysis showed that emotion regulation was significantly related to behaviours for all values of risk perception below 67.53. In other words, for participants who perceived low or average levels of risk perception an increase in the number of behaviours undertaken was associated with a higher emotion regulation (Figure 1).
Table 4.
Regression model predicting the number of behaviours participants undertook to protect themselves from infection
| β | B | SE | t | 95% C.I. | |
|---|---|---|---|---|---|
| Intercept | .003 | 1.61 | .97 | 1.65 | [−0.30, 3.52] |
| Emotion regulation | −.22 | −.36 | .19 | −1.87 | [−0.73, 0.02] |
| Media exposure | .49 | .36 | .18 | 1.99* | [0.005, 0.71] |
| Wave | −.65 | −1.53 | .69 | −2.23* | [−2.89, −.18] |
| Risk perception | −.27 | −.01 | .02 | −.65 | [−0.05, 0.02] |
| Trust authorities | .05 | .04 | .02 | 2.44* | [0.01, 0.07] |
| Political orientation | −.04 | −.04 | .02 | −2.33* | [−0.07, −0.01] |
| Education | .05 | .06 | .03 | 2.54* | [0.01, 0.11] |
| Cases per million | .11 | .001 | .0004 | 3.13** | [0.0004, 0.002] |
| Emotion regulation × Media exposure | −.45 | −.06 | .04 | −1.79 | [−0.14, 0.01] |
| Emotion regulation × Wave | 1.12 | .49 | .14 | 3.56*** | [0.22, 0.75] |
| Emotion regulation × Risk perception | −.47 | .004 | 004 | 1.09 | [−0.003, 0.01] |
| Media exposure × Risk perception | −.49 | −.004 | .003 | −1.37 | [−0.01, 0.002] |
| Wave × Risk perception | 1.40 | .03 | .01 | 2.43* | [0.01, 0.05] |
| Emotion regulation × Media exposure × Risk perception | .58 | .001 | .001 | 1.61 | [−0.0002, 0.002] |
| Emotion regulation × Wave × Risk perception | −1.51 | .01 | .002 | −2.60** | [−0.01, −0.001] |
| Adj R 2 = .34, p < .001, AIC baseline = −154.09; AIC model = −160.80 | |||||
p < .05; **p < .01; ***p < .001.
Figure 1.
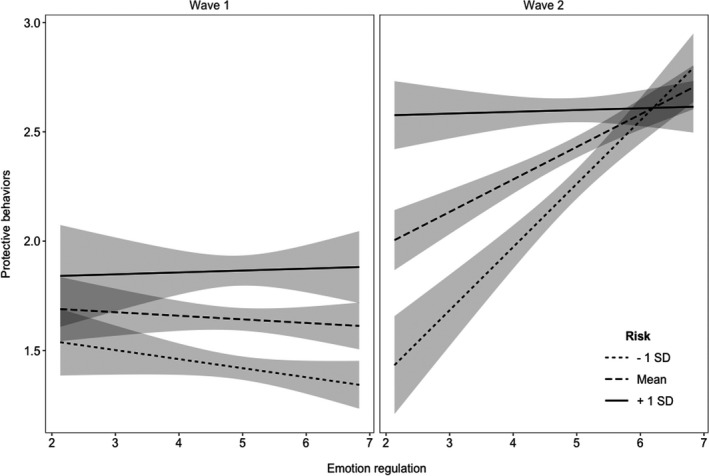
Slopes for emotion regulation depending on wave and participants’ risk perception levels.
State anxiety
We then focused only on wave 2 in which we also measured state anxiety. First of all, we ran a backward model selection analysis. We started from a fully saturated model with a three‐way interaction between emotion regulation, media exposure, and risk perception, while controlling for the same covariates as in the previous models. The final and most plausible model is reported in Table 5. We found significant main effects for emotion regulation, media exposure, and risk perception but no interaction effects.
Table 5.
Regression model predicting participants’ state anxiety
| β | B | SE | t | 95% C.I. | |
|---|---|---|---|---|---|
| Intercept | .004 | 64.74 | 2.72 | 23.80*** | [59.40, 70.08] |
| Emotion regulation | −.18 | −2.22 | .37 | −6.06*** | [−2.95, −1.50] |
| Media exposure | .27 | 1.53 | .49 | 3.12** | [0.57, 2.50] |
| Risk perception | .24 | .09 | .03 | 3.55*** | [0.04, 0.14] |
| Education | .12 | 1.18 | .30 | 3.91*** | [0.59, 1.77] |
| Cases per million | −.05 | −.005 | .003 | −1.58 | [−0.01, 0.001] |
| Media exposure × risk perception | −.19 | −.01 | .007 | −1.74 | [−0.03, 0.002] |
| Adj R 2 = .08, p < .001, AIC baseline = 4474.75; AIC model = 4464.46 | |||||
p < .05; **p < .01; ***p < .001.
Based on these results, we tested whether state anxiety could mediate the relation between risk perception and people’s protective behaviours while also including the interaction between risk perception and emotion regulation (see Figure 2). Results revealed that people’s behaviours were predicted by both the interaction and state anxiety. Both the indirect path (β = .02, B = .44, SE = .0002, z = 2.88, p = .002, 95% C.I. = [0.0003, 0.001]) and the overall model (β = .45, B = .44, SE = .08, z = 5.62, p = .002, 95% C.I. = [0.21, 0.69]) were significant supporting the conclusion that state anxiety partially mediated the relation between risk perception and protective behaviours.
Figure 2.
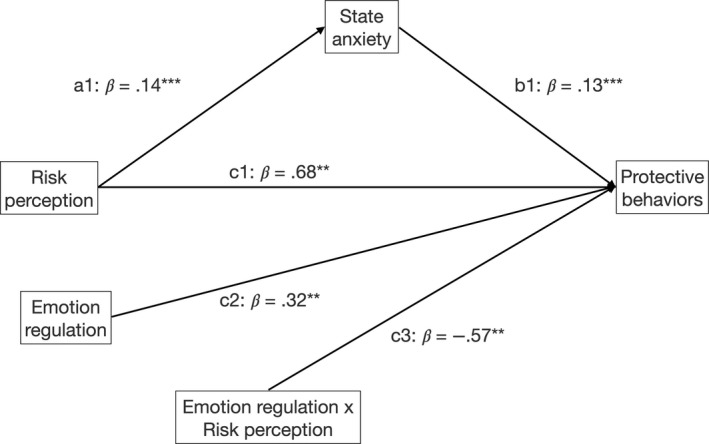
Model assessing the role of state anxiety as a mediator of the relation between risk perception and the number of protective behaviours undertook by people during the lockdown (wave 2).
Discussion
In the present study, we reported how people’s risk perception varies in relation to exposure to media outlets, time, and number of cases. Risk perception in turn predicted the protective behaviours that people undertook to contain the spread of the virus. Importantly, at the most intense time during the crisis (wave 2), when the countrywide lockdown was imposed, this relation was moderated by how well people regulated their emotions. These results were further explained by the mediating role of state anxiety on the relation between risk perception and protective behaviours. People who perceived more risk experienced a higher level of state anxiety and undertook more protective behaviours.
Towards the end of February 2020, Italy experienced the outbreak of the COVID‐19 infection. Initially, just a few cases were reported, and the government enacted mild containment measures locking down specific areas. This initial reaction was not enough to stop the spread of the virus and, on 9 March, the government decided to put the whole country in lockdown. At this point, every Italian citizen was somehow directly impacted by this major health crisis and had to deal with it and the lifestyle changes it imposed. Consistent with these developments, we found a higher risk perception in the second wave compared to the first. In addition, at both these times, the media were flooded with news and statistics about the number of positive cases and deaths as well as news about the hospitals struggle to treat all patients. As a result of the grim reality portrayed by the media, looking at them more was associated with a higher risk perception. This is consistent with recent evidence related to the pandemic as well as with work in the field of risk perception showing that images and news reported by the media can increase the sense of threat experienced by people (Slovic et al., 2004; Rubaltelli, Scrimin, Moscardino, Priolo, & Buodo, 2018). Finally, risk perception was associated with the increase in the rate of cases per million inhabitants and was higher for right‐wing versus left‐wing respondents. This result might depend on the fact that the COVID‐19 outbreak is characterized by a high degree of uncertainty and right‐wing people have been found to be cognitively less flexible (Tetlock, 2007). Importantly, of all the variables associated with risk perception, the main predictors were time (wave 2 vs. wave 1) and the number of positive cases in days in which data were collected. As expected, people’s risk perception was mainly associated with the start of the lockdown and the much higher number of positive cases registered at that time.
Between wave 1 and wave 2, there was an increase in the number of behaviours people undertook to avoid infection. Results showed that the main predictor was a three‐way interaction between wave, risk perception, and emotion regulation, although media exposure also was associated with the willingness to undertake protective behaviours. Specifically, only in wave 2, the relation between risk perception and protective behaviours was moderated by emotion regulation, indicating that when risk perception was low or average the effect of emotion regulation was significant whereas people always undertook a high number of protective behaviours when they perceived high risk. In other words, this means that, when the countrywide lockdown was imposed, people who were more effective in regulating their emotions undertook a high number of protective behaviours regardless of their risk perception. Instead, for ineffective regulators, the increased number of protective behaviours was related to their risk perception. This finding is consistent with the literature on emotion regulation and how people react to real‐life emotionally loaded events (e.g., terrorist attacks; Scrimin & Rubaltelli, 2019), although it was reported for the first time in relation to a global pandemic. Importantly, emotion regulation was not associated with a lower risk perception as it was found in other contexts. Instead, emotion regulation moderated the relation between risk perception and people’s willingness to undertake protective behaviours. Consistent with our hypotheses, emotion regulation had a moderating role on people’s resistance to undertake protective measures. Individuals with a high emotion regulation were willing to undertake a similar number of protective behaviours regardless of their level of risk perception. In contrast, when emotion regulation was low, people’s willingness to undertake protective behaviours was associated with their risk perception. Consistent with the affect heuristic (Slovic et al., 2004), when they perceived the risk as high, this information could have become a cue that led them to undertake a number of protective behaviours similar to that of individuals with high emotion regulation. When risk perception was low, these people undertook significantly fewer protective behaviours. This might have happened because they were bothered by the imposed restrictions, but they did not feel as much under threat to be motivated to comply with the protective measures. These findings are consistent with past literature showing that people who are effective at regulating can modulate the effect of their emotions and their behaviours are not necessarily affected by the way they feel (Sevdalis et al., 2007).
As a result, in the midst of the COVID‐19 outbreak, these people were more likely to follow guidelines on protective behaviours even without feeling particularly threatened by the coronavirus. They did not need to follow an emotional cue to abide by the restrictions set to keep the spread of the virus under control. In contrast, people who are ineffective at regulating their emotions tend to behave in a way that is highly influenced by the way they feel (Mikolajaczak, Petrides, Coumans, & Luminet, 2009). This is shown by our finding that people with a low score on emotion regulation were undertaking a higher number of protective behaviours when feeling threatened by the coronavirus (high risk perception) than when they were feeling safe (low‐risk perception).
Finally, in wave 2, we decided to measure participants’ state anxiety since the lockdown introduced by the government had likely had a different effect on how each person felt about the evolution of the virus outbreak. A mediation model showed that, at the peak of the virus outbreak, risk perception predicted anxiety, which, in turn, predicted the number of behaviours undertaken by people. Importantly, despite the mediating role of anxiety, risk perception remained a significant predictor of protective behaviours and this relation was still moderated by emotion regulation. This result shows that, among people who were worst regulators, those who perceived a higher risk undertook more protective behaviours, likely as a way to control their anxiety about the crisis. At the same time, ineffective regulators who did not perceive the level of risk as high failed to undertake enough protective behaviours. This is likely because they lacked the emotional cue represented by a heightened sense of anxiety. These findings are consistent with our interpretation that people who have low emotion regulation needed an emotional cue to find the motivation to undertake behaviours that can protect them from the virus.
The present work provided a first picture of how Italians reacted to the early outbreak of the coronavirus in the country and then adapted to the countrywide lockdown that imposed severe limitations to their freedom and obliged them to significantly change their lifestyles, thus causing an additional source of stress. Our goal was to get a better understanding of the environmental and psychological factors that could predict how people reacted in these very challenging and dramatic times. We do not pretend to have tested an exhaustive list of factors and we acknowledge that how people react to the COVID‐19 outbreak could differ by country because of cultural factors and the specific measures implemented by each government. It is also important to note some limitations of our study. First of all, we included several predictors in our models and results should be interpreted carefully because of potential issues with multiple comparisons. Furthermore, it should be kept in mind that the same responders were not sampled at each wave. While it is plausible to think that risk perception and behaviours changed as a function of time passing, the exponential growth of COVID‐19 cases, and the stringent lockdown, other factors related to sample composition might be causing part of the changes. Hence, the observed differences between samples should be interpreted with caution. Also, related to the sample characteristics, a further limit is the convenience sampling and recruitment strategy which might have influenced a range of responses. However, it should be noted here that we were careful to start the snowball sampling from very different populations (e.g., University students, parents, sales agents, book club). Finally, we did not ask participants about their general health status or whether they had any pre‐existing issues that, if infected by the coronavirus, could increase the severity of their symptoms. This information could have been useful to assess whether risk perception and protective behaviours were impacted by the health status of the respondents. Recent work by Shevlin et al. (2020) suggests that, in the UK, people with health issues were more likely to be in favour of mask wearing.
Notwithstanding these points, the present study provides important information regarding how people experienced the early stages of the outbreak. This information could prove very valuable in the coming months to understand who is more likely to be impacted by the stress caused by the COVID‐19 pandemic as well by all the imposed limitations. Even among the people who make a quick recovery, some might be less effective at regulating their emotions and feel highly threatened by the crisis. Despite not showing visible signs of sufferance, these people may be severely impacted by the sustained stress and anxiety they endured during the long lockdown especially if they undertook protective behaviour out of fear. Similarly, among the worst regulators, we may need to protect those who did not perceive the risk as high and failed to protect themselves well enough. As countries move towards slowly resuming normal activities these individuals might put themselves at serious risk and potentially cause a new outbreak of the virus. These factors should be accounted for when implementing and communicating the next steps and the long‐term measures to be followed in the aftermath of the COVID‐19 outbreak. Specifically, since over time people have shown to adjust differently to the pandemic, it is important to monitor the population in order to be able to target the intervention. One possible suggestion might be that of having people self‐report on their behaviours and stress response, for example through a free public application. This would allow not only to target the interventions but also to offer some basic advice on strategies to foster emotion regulation skills. Importantly, a second suggestion for health professionals could be to offer simple training sessions to help individuals to regulate emotion and become more resilient in the face of the pandemic.
Conflict of interests
All authors declare no conflict of interest.
Author contribution
Enrico Rubaltelli, PhD (Conceptualization; Formal analysis; Supervision; Writing – original draft; Writing – review & editing). Elisa Tedaldi (Conceptualization; Methodology; Writing – review & editing). Noemi Orabona (Conceptualization; Methodology; Writing – review & editing). Sara Scrimin, PhD (Conceptualization; Formal analysis; Supervision; Writing – original draft; Writing – review & editing).
Appendix 1.
Survey questions (translated from Italian to English)
The survey questions were roughly the same in both waves, any differences between the two surveys are reported in the text below.
-
Gender:
Female
Male
Non‐binary
Prefer not to say
Age: _________ years old
Please, insert below your ZIP code: _________
-
What is your level of education?
Primary school
Middle school
High school
Bachelor’s degree
Master’s degree
Specialization/Doctorate
-
What is your household income?
> 10,000 (%)
10,000–19,999
20,000–29,999
30,000–39,999
40,000–49,999
50,000–59,999
60,000–69,999
70,000–79,999
80,000–89,999
90,000–99,999
100,000–109,999
110,000–119,999
120,000–129,999
130,000–139,999
140,000–149,999
> 150,000
Prefer not to say
-
Answer the following question moving the cursor along the line ranging from 0 (not high at all) to 100 (very high):
How high is the risk of contracting COVID‐19?
During the last 48 hours, did you experience any of the following symptoms?
| Coughing | Yes | No |
| Runny nose | Yes | No |
| Fever | Yes | No |
| General malaise | Yes | No |
| Sore throat | Yes | No |
| Headache | Yes | No |
During the last week, did you undertake any of the following behaviours?
| Bought a mask | Yes | No |
| Called the doctor | Yes | No |
| Washed hands more often | Yes | No |
| Cancelled meetings | Yes | No |
| Cancelled travel plans | Yes | No |
Where did you look and read news and information about COVID‐19?
| Facebook and other social media | Yes | No |
| National newspapers | Yes | No |
| Local newspapers | Yes | No |
| Press agencies | Yes | No |
| Newscasts | Yes | No |
| Shows on TV | Yes | No |
| National health bureau | Yes | No |
| WHO | Yes | No |
| Scientific journals | Yes | No |
Trait Emotional Intelligence Questionnaire – Short Form (Petrides, 2009).
State‐Trait Anxiety Inventory (state anxiety subscale; Spielberg, 1983 – only in wave 2)
-
What is your political orientation?
Extreme left wing
Left wing
Center‐left wing
Center‐right wing
Right wing
Extreme right wing
-
Independently from your specific faith, how much do you consider yourself as a religious person?
1 (not at all)
2
3
4
5
6
7 (very much)
-
Please, report on the scale below your trust in the authorities:
1 (not at all)
2
3
4
5
6
7 (very much)
Footnotes
Recruitment occurred mainly through Facebook pages. The advertisement of the study was posted in several groups. We chose to start the snowball sampling from very different populations (e.g., University students, parents, sales agents, book clubs) in order to include a diverse sample. We then relied on snowball sampling. In addition, the survey was spread also through WhatsApp groups. The initial groups were directly linked to the research team but once again we relied on snowball sampling asking who completed the survey to share it in other groups.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- Akaike, H. (1973). Maximum likelihood identification of Gaussian autoregressive moving average models. Biometrika, 60, 255–265. 10.1093/biomet/60.2.255 [DOI] [Google Scholar]
- Bish, A. , & Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. British Journal of Health Psychology, 15, 797–824. 10.1348/135910710X485826 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burnham, K. P. , Anderson, D. R. , & Huyvaert, K. P. (2011). A model selection and multimodel inference in behavioral ecology: some background, observations, and comparisons. Behavioral Ecology and Sociobiology, 65(1), 23–35. 10.1007/s00265-010-1029-6. [DOI] [Google Scholar]
- Cohen, N. , & Ochsner, K. N. (2018). From surviving to thriving in the face of threats: the emerging science of emotion regulation training. Current Opinions in Behavioral Science, 24, 143–155. 10.1016/j.cobeha.2018.08.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen Silver, R. , Holman, E. A. , Pizarro Andersen, J. , Poulin, M. , McIntosh, D. N. , & Gil‐Rivas, V. (2013). Mental‐ and physical‐health effects of acute exposure to media images of the September 11, 2001, Attacks and the Iraq War. Psychological Science, 24, 1623–1634. 10.1177/0956797612460406 [DOI] [PubMed] [Google Scholar]
- Eippert, F. , Veit, F. , Veiskopf, N. , Erb, M. , Eippert, F. , Veit, F. , Veiskopf, N. , Erb, M. , Birbaumer, N. , & Anders, S. (2007). Regulation of emotional responses elicited by threat‐related stimuli. Human Brain Mapping, 28, 409–423. 10.1002/hbm.20291 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher, D. , & Wilder‐Smith, A. (2020). The global community needs to swiftly ramp up the response to contain COVID‐19. Lancet, 395, 1109–1110. 10.1016/S0140-6736(20)30679-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giuffrida, A. , & Cochrane, L. (2020). Italy imposes draconian rules to stop spread of coronavirus. The Guardian, February 23. Retrieved from https://www.theguardian.com/world/2020/feb/23/italy‐draconian‐measures‐effort‐halt‐coronavirus‐outbreak‐spread.
- Governo Italiano Presidenza del Consiglio dei Ministri . (2020) DECRETO DEL PRESIDENTE DEL CONSIGLIO DEI MINISTRI 8 marzo 2020. Retrieved on March 14, 2020, from https://www.gazzettaufficiale.it/gazzetta/serie_generale/caricaDettaglio?dataPubblicazioneGazzetta=2020‐03‐08&numeroGazzetta=59&elenco30giorni=true.
- Grasselli, G. , Pesenti, A. , & Cecconi, M. (2020). Critical care utilization for the COVID‐19 outbreak in Lombardy, Italy. JAMA, 323, 1545–1546. 10.1001/jama.2020.4031 [DOI] [PubMed] [Google Scholar]
- Hu, T. , Zhang, D. , Wang, J. , Mistry, R. , Ran, G. , & Wang, X. (2014). Relation between emotion regulation and mental health: a meta‐analysis review. Psychological reports, 114, 341–362. 10.2466/03.20.PR0.114k22w4 [DOI] [PubMed] [Google Scholar]
- Lades, L. K. , Laffan, K. , Daly, M. , & Delaney, L. (2020). Daily emotional well‐being during the COVID‐19 pandemic. British Journal of Health Psychology. 10.1111/bjhp.12450 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarus, R. S. , & Folkman, S. (1984). Stress, appraisal, and coping. New York, NY: Springer publishing company. [Google Scholar]
- McElreath, R. (2016). Statistical rethinking: A Bayesian course with examples in R and Stan, Vol. 122. Boca Raton, FL: CRC Press. [Google Scholar]
- Mikolajaczak, M. , Petrides, K. V. , Coumans, N. , & Luminet, O. (2009). The moderating effect of trait emotional intelligence on mood deterioration following laboratory‐induced stress. International Journal Clinical Health Psychology, 9, 455–477. [Google Scholar]
- Olagoke, A. A. , Olagoke, O. O. , & Hughes, A. M. (2020). Exposure to coronavirus news on mainstream media: The role of risk perceptions and depression. British Journal of Health Psychology, online first available at. 10.1111/bjhp.12427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petrides, K. V. (2009). Psychometric properties of the trait emotional intelligence questionnaire (TEIQue). In James D. A. P., Donald H. S., & Con Stough (Eds.), Assessing Emotional Intelligence (pp. 85‐101). Boston: Springer. [Google Scholar]
- Petrides, K. V. , Niven, L. , & Mouskounti, T. (2006). The trait emotional intelligence of ballet dancers and musicians. Psicothema, 18, 101–107. [PubMed] [Google Scholar]
- Rajkumar, R. P. (2020). COVID‐19 and mental health: A review of the existing literature. Asian Journal of Psychiatry, 52, 102066. 10.1016/j.ajp.2020.102066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosseel, Y. (2012). lavaan: An R Package for Structural Equation Modeling. Journal of Statistical Software, 48, 1–36. [Google Scholar]
- Rubaltelli, E. , Scimin, S. , Moscardino, U. , Priolo, G. , & Buodo, G. (2018). Media exposure to terrorism and people’s risk perception: The role of environmental sensitivity and psychophysiological response to stress. British Journal of Psychology, 109, 656–673. 10.1111/bjop.12292 [DOI] [PubMed] [Google Scholar]
- Schmälzle, R. , Häcker, F. , Renner, B. , Honey, C. J. , & Schupp, H. T. (2013). Neural correlates of risk perception during real‐life risk communication. Journal of Neuroscience, 33, 10340–10347. 10.1523/JNEUROSCI.5323-12.2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scrimin, S. , & Rubaltelli, E. (2019). Dehumanization after terrorism: the role of psychophysiological emotion regulation and trait emotional intelligence. Current Psychology. 10.1007/s12144-019-00189-x [DOI] [Google Scholar]
- Sevdalis, N. , Petrides, K. V. , & Harvey, N. (2007). Trait emotional intelligence and decision‐related emotions. Personality and Individual Differences, 42, 1347–1358. 10.1016/j.paid.2006.10.012 [DOI] [Google Scholar]
- Shevlin, M. , McBride, O. , Murphy, J. , Gibson Miller, J. , Hartman, T. K. , Levita, L. , Butter, S. (2020). Demographic, health and mental health predictors of face mask wearing in the UK population during the COVID‐19 lockdown period. OSF preprints. Retrieved from: osf.io/5j7qz.
- Slovic, P. (1987). Perception of risk. Science, 236, 280–285. 10.1126/science.3563507 [DOI] [PubMed] [Google Scholar]
- Slovic, P. , Finucane, M. , Peters, E. , & MacGregor, D. G. (2004). Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Analysis, 24, 311–322. 10.1111/j.0272-4332.2004.00433.x [DOI] [PubMed] [Google Scholar]
- Spielberg, C. D. (1983). Manual for the state‐trait anxiety inventory STAI (Form Y). Palo Alto (CA) Consulting Psychology Press. [Google Scholar]
- Tetlock, P. E. (2007). Psychology and politics: The challenges of integrating levels of analysis in social science. In Kruglanski A. W. & Higgins E. T. (Eds.), Social psychology (Chapter 39), (pp. 888–912). New York, NY: The Guilford Press. [Google Scholar]
- Van Bavel, J. J. , Baicker, K. , Boggio, P. S. , Capraro, V. , Cichocka, A. , Cikara, M. , … Willer, R. , (2020). Using social and behavioral science to support COVID‐19 pandemic response. Nature Human Behavior, 4, 460–471. 10.1038/s41562-020-0884-z [DOI] [PubMed] [Google Scholar]
- Wise, T. , Zbozinek, T. , Michelini, G. , Hagan, C. C. , & Mobbs, D. (2020). Changes in risk perception and protective behavior during the first week of the COVID‐19 pandemic in the United States. Psyarxiv. Retrived from: https://psyarxiv.com/dz428/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zarocostas, J. (2020). How to fight an infodemic. Lancet, 10225, 676. 10.1016/S0140-6736(20)30461-X [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.