

Abstract
As the COVID‐19 pandemic accelerates, one public health response has been for governments to impose quarantine ‘lockdowns’ which require people to socially isolate. In this study, we explored the level of psychological distress that people experienced in social isolation and the factors which might ameliorate or exacerbate it. Two hundred and thirteen participants (69% female) with a mean age of 37.82 years participated in an online study. They completed a series of questions designed as part of a larger cross‐national study. A positive attitude towards social isolation introduced by government as a strategy to reduce the transmission of COVID‐19 was predictive of positive coping strategies, and both attitude and coping predicted reduced psychological distress. Participants’ worries about contagion of COVID‐19, their financial status, and the economic and political impact of the COVID‐19 pandemic predicted increases in their psychological distress. Social support from family and work colleagues was not significant in reducing worries or psychological distress but it did positively predict engagement in coping. The findings and recommendations are discussed.
Practitioner points
Fostering a positive attitude towards social isolation in clients: reduces psychological distress, fosters engagement in positive coping behaviours.
Enhancing clients’ level of social support received will serve to increase positive coping and indirectly reduce psychological distress during social isolation.
Strategies to reduce clients’ COVID‐19 worries are important as worry contributes to their overall level of psychological distress.
Keywords: attitude, coping, COVID‐19, psychological distress, social support, worries
Background
SARS‐CoV‐2, known as Novel Coronavirus COVID‐19, is a highly infectious disease that emerged in late 2019 in Wuhan, China. Despite moves to implement quarantine restrictions, the virus spread rapidly outside the country. By mid‐July 2020, there were nearly 15 million confirmed cases among those tested for the virus and over 600,000 deaths attributed to COVID‐19 across nearly every country in the world. A true pandemic not seen since the Influenza pandemic of the early 20th Century.
Many governments have instigated what are effectively quarantine procedures to curb the transmission of the virus, which may vary across nations. In Australia, it involves people Staying Home and Working/Studying from Home unless involved in essential services. Many who work in the travel, and entertainment industries or in casual employment are not able to work from home. For them especially, the prospect of unemployment and financial hardship is a reality as are health concerns for people generally.
People quarantined during the SARS outbreak of 2002–2003 experienced a range of impairments including depression (Cacioppo et al., 2010; Hawryluck et al., 2004), loneliness, and increased blood pressure (Hawryluck et al., 2004). Similarly, people quarantined during an outbreak of equine influenza in Australia in 2007 experienced a higher incidence of psychological distress than the general population (Taylor et al., 2008). Kaniasty and Norris (2000) and Forbes et al. (2012) are among those who have shown that social support can ameliorate the impact of natural disasters. It might also be that support would reduce feelings of psychological distress and worry at this time.
Social isolation is government mandated, but how do people feel about it? Could a positive attitude towards the need for social isolation enhance positive coping strategies which together reduce feelings of psychological distress? Would support received from others promote engagement in coping as well as reduce people’s worries about the impact of COVID‐19 and indirectly, their levels of psychological distress? The aim in this study was to test a model directed towards answering these questions.
Method
Design
An online survey was used to collect data from the 16th April to 11th May 2020, during the initial period of social isolation imposed by the Australian government as part of its public health response to the COVID‐19 pandemic.
Participants
Two hundred and thirteen volunteers (69% female), mean age of 37.82 years (SD = 13.24), responded to an invitation to participate in this study. Respondents were from all states and territories in Australia, except South Australia, although the majority were from Victoria, followed by New South Wales and Queensland. The majority of participants (56%) were married/cohabitating, 34% were single, and 10% reported they were separated or divorced. Most respondents were University educated (87%), or had completed high school or an apprenticeship qualification (13%).
In terms of work status, 19.2% of respondents reported they were self‐employed or an employer, 68.4% indicated they were an employee, and 33.5% were students, but there was overlap between being an employee and a student. This overlap is not uncommon given the increasing need for students to work in order to support their studies (Grimmond et al., 2020). The occupations reported were highly diverse from students (17), lectures/teachers (10), retired (6), nurses (3), and one each across many other occupations such as accounting, baker, cook, real estate, and sales.
Procedure
The University’s Ethics Committee provided approval for the conduct of a larger study of which these data form part. Advertisements on social media sites (Facebook and LinkedIn) directed interested persons to the survey hosted on Qualtrics.com. Participants were advised that data are anonymous, participation voluntary, and submission of the completed survey constitutes informed consent. No incentives were offered for participation.
Materials
Participants provided demographic data and completed the following scales designed for this study.1
The Attitudes towards Social Isolation Scale (ASIS) has eight items: ‘I believe … (e.g., Social isolation is essential for everyone; Only way to control COVID‐19; Unnecessary)’ answered on a 5‐point Likert scale from 1 = Not at all to 5 = Absolutely. Four items are reversed coded. Cronbach’s α = .86 is strong.
The COVID‐19 Worry Scale (CWS) has 11 items: ‘As a result of COVID‐19, I worry that … (e.g. I will be in debt if social isolation persists; My children will get COVID‐19)’ answered on a 5‐point Likert scale from 1 = Not at all to 5 = Pretty much all the time. It has three factors: Financial Worries, Political/Anarchy Worries, and Fear of Contagion. Cronbach’s α ≥ .73 are satisfactory.
Psychological Distress Scale (PDS) has 15 questions: ‘Being in imposed social isolation because of COVID‐19 makes me feel … (e.g. miserable, lonely, and tense)’ answered on a 5‐point Likert scale from 1 = Not at all to 5 = Pretty much always. It has two factors: Lonely and Angry. Internal reliabilities are excellent, Cronbach’s α = .94 and .88, respectively.
Positive Coping Behaviours Scale (PCB) has nine items: ‘I am coping by … (e.g. Gardening, and Exercising)’ rated on a 5‐pt Likert scale from 1 = Not at all to 5 = Most of the time. PCB has two independent factors labelled Keeping Occupied and Healthy Behaviours. Cronbach’s α = .70 and .63, respectively, are satisfactory.
Social Support from Others Scale (S_FOS) has 11 items: ‘How much support are you receiving at this time? From …. (e.g. mother, partner, and work/study supervisor)’ answered on a 5‐point Likert scale from 1 = No support to 5 = Quite a Lot. S_FOS has three factors: Nuclear Family, Extended Family and Friends, and Work Colleagues. Cronbach’s α ≥ .82 are good.
Results
Data were analysed using SPSS and AMOS (Version 26) and screened for missing data and normality. Aside from nine respondents who failed to answer most questions, there was less than 5% randomly missing data which were replaced using item mean substitutions (Dodeen, 2003).
Structural equation modelling was used to test the hypothesized model. The data provided a reasonable fit to the model ( = 117.13, p < .001; χ2/df = 2.78; GFI = .88; RMSEA = .11; p/close < .001; SRMR = .10). The modification indices suggested a correlation between a positive attitude towards social isolation and fear of contagion. Following this modification, the fit of the data to the model improved (= 102.72, p < .001; χ2/df = 2.50; GFI = .90; RMSEA = .10; p/close = .001; SRMR = .10) (Figure 1).
Figure 1.
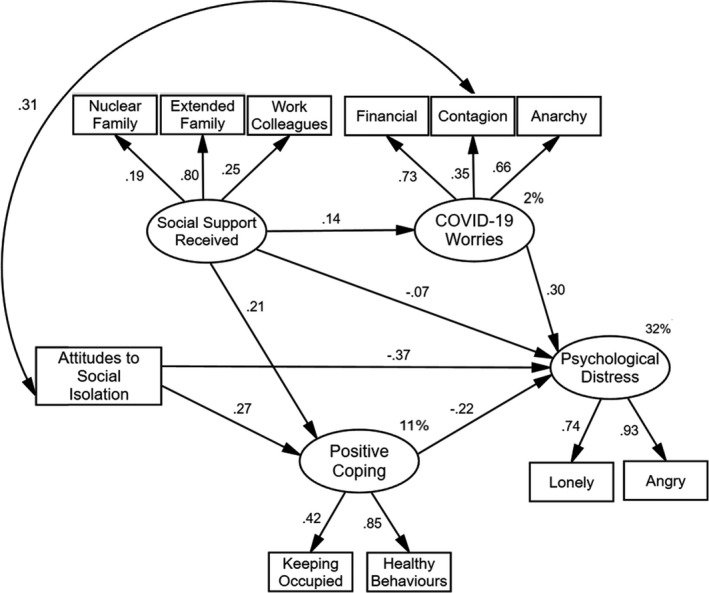
Results of model testing showing standardized regression weights (β) and squared‐multiple correlations (%). All values equal to and greater than .21 are significant at p < .05.
Thirty‐two per cent of the variance in psychological distress was explained by the variables in the model. A positive attitude towards social isolation negatively predicted psychological distress (β = −.37), but positively predicted participants’ engagement in coping strategies operationalized by keeping occupied and engaging in healthy behaviours (β = .27). Coping also reduced participants’ feelings of psychological distress (β = −.22), while people’s worries at this time: financial, fear of contagion, and fear of anarchy (e.g. government could collapse) contributed to increased psychological distress (β = .30). Social support from others significantly predicted participants’ engagement in positive coping strategies (β = .21) but did not significantly predict changes in their worries (β = .14) or feelings of psychological distress (β = .07).
The modification shows that contagion worries and a positive attitude towards social isolation were significantly correlated (r = .31). Standardized total effects between the latent variables are presented in Table 1. A positive attitude towards social isolation exerted the biggest effect on psychological distress through positive coping (β = −.43).
Table 1.
Standardized total effects among the latent variables in the model
| Latent variable | Social support received | Attitude towards social isolation | Positive coping | COVID‐19 worries |
|---|---|---|---|---|
| Positive coping | .21 | .27 | – | – |
| COVID‐19 worries | .15 | – | – | – |
| Psychological distress | −.07 | −.43 | −.22 | .30 |
Discussion
The aim in this study was to test a model of people’s psychological distress during social isolation. After adding a covariance path from worries about contagion to a positive attitude towards social isolation, the data provided a good fit to the model. It seems the more worried people are of contracting COVID‐19, the more positive they are towards social isolation (e.g. it is necessary and only way to control COVID‐19).
As in previous studies of people in quarantine (Cacioppo et al., 2010; Hawryluck et al., 2004; Taylor et al., 2008), participants in the current study also experienced psychological distress (Feeling lonely, anxious, and abandoned; and angry, annoyed, and bitter). Furthermore, they were worried about their finances (e.g. I will be in debt if social isolation continues); that they or their family would contract COVID‐19; and the stability of the economy and government (e.g. The country will go into depression; Our political system will collapse), all of which contributed to their psychological distress. It is not clear what impact Australian government initiatives to extend unemployment and job‐seeker payments to those eligible, as well as publicity and recommendations around safeguards to prevent contagion, have on people’s level of worry. A future study might consider the effectiveness of these strategies especially in those directly affected.
Attitude is a component of the theory of planned behaviour (Ajzen, 1991), which might explain why a positive attitude predicted engagement in coping behaviours (e.g. Catching up on chores, Sorting out things at home; chores: Eating well, Exercising). This positive attitude and coping behaviours were negatively related to psychological distress. It is encouraging that coping behaviours negatively predicted psychological distress as a lack of volition or engagement in activities has been associated with depression (Nitschke & Mackiewicz, 2005).
Social support was significantly predictive of engagement in coping behaviours, but it was not related to reducing worries or psychological distress. It may be that most support was in the form of encouragement via various media such as phone, text, and Facetime, rather than face‐to‐face, which reduced its effectiveness. Certainly little external tangible support could be offered during this time.
While the current findings reflect a snapshot of the impact of COVID‐19 during social isolation in an Australian sample, it is important to note that the sample was mostly from the eastern states, highly educated, and predominantly female. It is important that future studies extend the breadth of sampling with follow‐up studies to ascertain the ongoing impact of social isolation and the related impact of COVID‐19 in the broader Australian population.
In conclusion, it seems that fostering a positive attitude to social isolation as a government imposed strategy to reduce the spread of COVID‐19 is an important factor in people remaining active, looking after themselves, and reducing feelings of psychological distress. Future research needs to consider the sustainability of this positive attitude and its ongoing effect on psychological distress.
Conflicts of interest
All authors declare no conflict of interest.
Author contributions
Kathleen Anne Moore, PhD (Conceptualization; Methodology; Writing – original draft) James J Lucas (Formal analysis; Writing – review & editing).
Footnotes
The psychometric properties of these scales have been established, but due to word restrictions further details are not included here. The scales are available from the authors on request.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on request as per limitations of our ethics approval.
References
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. 10.1016/0749-5978(91)90020-T [DOI] [Google Scholar]
- Cacioppo, J. , Hawkley, L. , & Thisted, R. (2010). Perceived social isolation makes me sad: 5‐year cross‐lagged analysis of loneliness and depressive symptomology in the Chicago Health, Aging, and Social Relations Study. Psychology and Aging, 25, 453–463. 10.1037/a0017216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dodeen, H. M. (2003). Effectiveness of valid mean substitution in treating missing data in attitude assessment. Assessment & Evaluation in Higher Education, 2, 505–513. 10.1080/02602930301674 [DOI] [Google Scholar]
- Forbes, R. J. , Jones, R. , & Reupert, A. (2012). In the wake of the 2009 Gippsland fires: Young adults’ perceptions of post‐disaster social supports. Australian Journal of Rural Health, 20, 119–125. 10.1111/j.1440-1584.2012.01271.x [DOI] [PubMed] [Google Scholar]
- Grimmond, T. , Yazidjoglou, A. , & Strazdins, L. (2020). Earning to learn: The time‐health trade‐offs of employed Australian undergraduate students. Health Promotion International, daz133. 10.1093/heapro/daz133 [DOI] [PubMed] [Google Scholar]
- Hawryluck, L. , Gold, W. L. , Robinson, S. , Pogorski, S. , Galea, S. , & Styra, R. (2004). SARS control and psychological effects of quarantine, Toronto, Canada. Emerging Infectious Diseases, 10, 1206–1212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaniasty, K. , & Norris, F. H. (2000). Help‐seeking comfort and receiving social support: The role of ethnicity and context of need. American Journal of Community Psychology, 28, 545–581. [DOI] [PubMed] [Google Scholar]
- Nitschke, J. B. , & Mackiewicz, K. L. (2005). Prefrontal and anterior cingulate contributions to volition in depression. International Review of Neurobiology, 67, 73–94. [DOI] [PubMed] [Google Scholar]
- Taylor, M. R. , Agho, K. E. , Stevens, G. J. , & Raphael, B. (2008). Factors influencing psychological distress during a disease epidemic: Data from Australia's first outbreak of equine influenza. BMC Public Health, 8, 347. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on request as per limitations of our ethics approval.