

Abstract
Background
This study examined the social cognition determinants of social distancing behavior during the COVID‐19 pandemic in samples from Australia and the US guided by the health action process approach (HAPA).
Methods
Participants (Australia: N = 495, 50.1% women; US: N = 701, 48.9% women) completed HAPA social cognition constructs at an initial time‐point (T1), and one week later (T2) self‐reported their social distancing behavior.
Results
Single‐indicator structural equation models that excluded and included past behavior exhibited adequate fit with the data. Intention and action control were significant predictors of social distancing behavior in both samples, and intention predicted action and coping planning in the US sample. Self‐efficacy and action control were significant predictors of intention in both samples, with attitudes predicting intention in the Australia sample and risk perceptions predicting intention in the US sample. Significant indirect effects of social cognition constructs through intentions were observed. Inclusion of past behavior attenuated model effects. Multigroup analysis revealed no differences in model fit across samples, suggesting that observed variations in the parameter estimates were relatively trivial.
Conclusion
Results indicate that social distancing is a function of motivational and volitional processes. This knowledge can be used to inform messaging regarding social distancing during COVID‐19 and in future pandemics.
Keywords: action planning, coping planning, dual‐phase model, health action process approach, physical distancing, self‐efficacy, social cognition
INTRODUCTION
The COVID‐19 pandemic has had unprecedented global effects on mortality, way of life, national economies, and physical and mental health not previously experienced in modern times. It has presented governments, healthcare services, and education facilities with wide‐scale and complex logistical challenges on how to manage the rapid spread of the disease and minimise the projected human and economic costs. Given that, to date, there is no vaccine to protect against COVID‐19, non‐pharmacological intervention is the only currently available means to reduce the spread of SARS‐CoV‐2, the virus that causes COVID‐19, and “flatten the curve” of infection rates. In response, national and statewide governmental measures aimed at minimising transmission of the virus including “stay at home” orders, closure of businesses and places of congregation, and travel restrictions have had a substantive impact on mortality rates (Worldometer, 2020). As rates of infection dissipate in some countries, particularly in countries like Australia that have relatively low rates of daily infections, governments are now beginning to ease restrictions. However, preventive behaviors aimed at reducing infection rates remain highly pertinent given concerns over the potential for infection rates to rise again and fears of a “second wave”. Furthermore, some countries who are easing lockdown measures, such as some states in the US, still have high localised rates of infection, highlighting the imperative of ongoing performance of preventive behaviors to manage infection transmission.
Based on World Health Organization (WHO) recommendations (World Health Organization, 2020) and previous research on behaviors known to reduce virus transmission (Jefferson et al., 2011; Rabie & Curtis, 2006; Smith et al., 2015), two key sets of COVID‐19‐related behaviors that may apply to the population as a whole have been proposed (Michie et al., 2020). The first set is “personal protective behaviors” that are aimed at the individual in order to protect themselves or others (e.g. washing hands frequently, practicing respiratory hygiene). The second set involves behaviors aimed at ensuring physical distance between people (e.g. social distancing, stay at home orders). Despite knowledge of these key behaviors in the prevention of virus transmission (e.g. Islam et al., 2020), there is a relative dearth of information on the determinants and mechanisms of action that underpin these preventive behaviors and how to strengthen individuals’ capacity to adopt them. In the absence of direct evidence, knowledge to inform practice guidelines that governments and organisations can use to mobilise individuals into performing COVID‐19 preventive behaviors has been gleaned from applying general principles from behavioral science and the models of behavior that underpin them (Lunn et al., 2020; Michie et al., 2020; British Psychological Society, 2020; West et al., 2020) as well as findings of previous empirical investigations in the psychological literature on similar health and risk behaviors (e.g. face mask use, handwashing, distancing; Chu et al., 2020; Reyes Fernández et al., 2016; Zhang, Chung, et al., 2019; Zhang et al., 2020). Although this approach is potentially useful in structuring thinking and recommendations in urgent times, there is a pressing need for direct evidence that identifies the key determinants of these COVID‐19 preventive behaviors and the processes involved. This knowledge can then be used to inform development of effective interventions to promote uptake and adherence to these behaviors. This is especially important given that individuals’ beliefs may affect their adoption of non‐pharmacological measures to prevent virus transmission (Teasdale et al., 2014).
Prominent among social cognition theories are dual‐phase models which aim to provide a comprehensive theoretical account of health behavior uptake and participation, and the processes involved (Hagger, Cameron, Hamilton, Hankonen, & Lintunen, 2020; Hagger, Smith, Keech, Moyers, & Hamilton, 2020). One such dual‐phase theory that has been frequently applied to predict multiple health behaviors is the Health Action Process Approach (HAPA; Schwarzer, 2008; Schwarzer & Hamilton, 2020). The HAPA is an integrated model that combines features of stage, continuum, and dual‐phase social cognition models. A key feature of the model is the distinction made between motivational (where an individual is in a deliberative mindset while setting a goal/forming an intention) and volitional (where an individual is in an implementation mindset while pursuing their goal) phases involved in behavioral enactment. In the motivational phase, intentions are conceptualised as the most important determinant of behavior. Intentions are proposed to be a function of three sets of belief‐based constructs: outcome expectancies (beliefs that the target behavior will lead to outcomes that have utility for the individual, conceptually identical to an individual’s attitudes toward the behavior), self‐efficacy (beliefs in personal capacity to successfully perform the target behavior and overcome challenges and barriers to its performance), and risk perceptions (beliefs in the severity of a health condition that may arise from not performing the target behavior and personal vulnerability toward it).
In the volitional phase of the HAPA, planning and action control strategies are important self‐regulatory strategies that determine subsequent enactment of the target behavior (Schwarzer, 2008; Schwarzer & Hamilton, 2020). Two forms of planning are proposed: action planning, a task‐facilitating strategy that relates to how individuals prepare themselves in performing a behavior, and coping planning, a distraction‐inhibiting strategy that relates to how individuals prepare themselves in avoiding foreseen barriers and obstacles that may arise when performing a specific behavior, and potentially competing behaviors that may derail the behavior. In addition, action control, a self‐regulatory strategy for promoting behavioral maintenance through the monitoring and evaluation of a behavior against a desired behavioral standard, is also an important direct determinant of behavior (Hamilton et al., 2018; Reyes Fernández et al., 2016).
Behavioral intention operates as a “bridge” between the motivational and volitional phases, while planning serves to link intentions with behavior. Previous research has provided support for the HAPA constructs in predicting health preventive behaviors, with prominent roles for outcome expectancies, forms of self‐efficacy, planning and action control, with risk perceptions only relevant in certain contexts (see Schwarzer & Hamilton, 2020; Zhang, Zhang, et al., 2019). Furthermore, the model has been used as a basis for effective behavior change interventions aimed at promoting increased participation in health‐related behaviors (Schwarzer & Hamilton, 2020).
The Present Study
Given that social distancing is a key evidence‐based behavior that will minimise transmission of SARS‐CoV‐2 if performed consistently at the population level, the aim of the present study was to apply the HAPA to identify the social cognition and self‐regulatory determinants of this preventive behavior in samples of adults from two countries, Australia and the US. These two countries provided an opportunity to examine the determinants of social distancing because they experienced rapid increases in COVID‐19 cases at relatively similar times during the pandemic and introduced public health advice as well as “lockdown” measures and “shelter‐in‐place” orders to minimise transmission, including social distancing. Specifically, the current research aimed to identify potentially modifiable determinants that are reliably related to social distancing intentions and behavior, which may form targets of behavioral interventions to reduce COVID‐19 infection rates, and, going forward, other communicable diseases transmitted through person‐to‐person contact. The value of applying the HAPA is that it provides information on phase‐relevant constructs in determining this important behavior. Proposed predictions among model constructs are summarised diagrammatically in Figures 1 and 2. Figure 1 presents the HAPA predictions excluding effects of past social distancing behavior.
FIGURE 1.
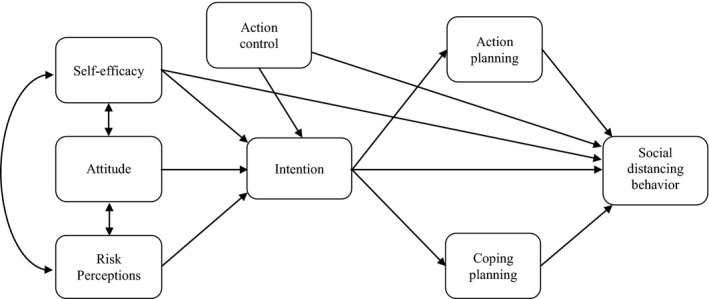
Proposed model illustrating effects among health action process approach (HAPA) constructs excluding past behavior.
FIGURE 2.
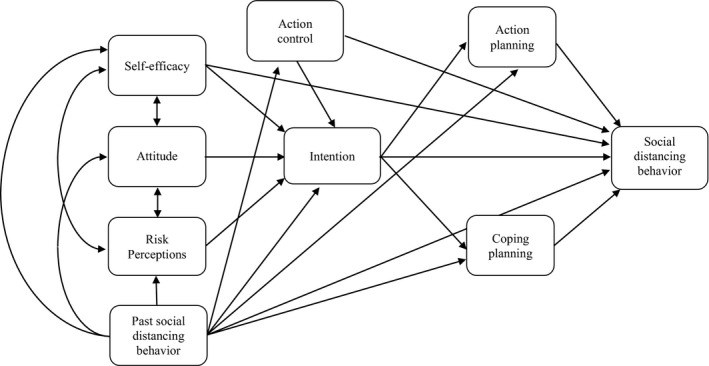
Proposed model illustrating effects among health action process approach (HAPA) constructs including past behavior.
Intention to perform social distancing was expected to be predicted by attitude (as a proxy for outcome expectancies), self‐efficacy, and risk perceptions, and social distancing behavior was expected to be predicted by self‐efficacy, intentions, action planning, coping planning, and action control. Intention was proposed to mediate effects of attitude, self‐efficacy, and risk perceptions on behavior. In addition, intention was expected to predict action planning and coping planning such that the planning constructs mediate the intention–behavior relationship. Action control was proposed to predict behavior directly. Although it is strictly a self‐regulation technique aimed at facilitating better behavioral enactment, as proposed by the original HAPA (e.g. Schwarzer, 2008), individuals who are effective at action control (i.e. self‐monitoring) may also more likely form strong intentions. Action control implies not only the recall of behavior but also the recall of intentions. Self‐monitoring of the concurrent behavior, therefore, may make the individual aware of their intention as well as their behavior, focusing on possible discrepancies between the two. It is plausible, then, that action control can be specified as a predictor of both intention and behavior. The coexistence of intention and action control within the same dataset allows this key question to be tested; which of the two factors may be more proximal to the behavioral outcome? Action control might not be a time‐specific variable, and individuals may self‐monitor their behaviors at any point in time (see Zhou et al., 2015), even before goal setting. Actions can be monitored before making intentions, while doing so, or afterwards. Thus, examining the indirect (via intention) and direct effects of action control on behavior is intuitively meaningful, although not supported by the original HAPA, and tested in the present study. Figure 2 outlines the inclusion of past behavior in the model to test its sufficiency. Although model effects were expected to hold with the inclusion of past behavior, it was expected to attenuate the size of the proposed effects consistent with previous studies (Brown et al., 2020; Hagger et al., 2018). This was expected to be the case in the current study due to the relatively brief one‐week follow up. The attenuation effect was proposed to model past decision making and effects of other unmeasured constructs on behavior.
METHOD
Participants
A sample of Australian (N = 495, 50.1% women) and US (N = 701, 48.9% women) residents were recruited via an online research panel company. To be eligible for inclusion, participants needed to be aged 18 years or older and were required to not be subject to formal quarantine for COVID‐19. In addition to the inclusion criteria, participants were screened on the demographic characteristics of age, gender, and geographical region and quotas were imposed to ensure that the sample comprised similar proportions of these characteristics to the national population of each country. Sample characteristics are presented in Table S1. Data were collected in April and May 2020 during which time residents throughout Australia and all states in the US were subject to “stay at home” orders to reduce transmission of the coronavirus.
Design and Procedure
The study adopted a prospective correlational design with self‐report measures of HAPA constructs (attitudes, self‐efficacy, risk perceptions, intentions, action planning, coping planning, and action control) and past engagement in social distancing behavior administered at an initial time‐point (T1) in a survey administered using the QualtricsTM online survey tool. Participants were informed that they were participating in a survey on their social distancing behavior and were provided with an information sheet outlining study requirements. They were also provided with a consent form to which they had to affirm before proceeding with the survey. Participants were also provided with an information sheet providing instructions on how to complete the study measures. In addition, they were provided with a definition of the target behavior: “The following survey will ask about your beliefs and attitudes about ‘social distancing’. What do we mean by social distancing? Social distancing (also known as ‘physical distancing’) is deliberately increasing the physical space between people to avoid spreading illness. The World Health Organization and other world leading health authorities suggest that you should maintain at least a 1–2 m (3–6 feet) distance from other people to lessen the chances of getting infected with COVID‐19. When answering the questions in this survey, think about your social distancing behavior (i.e. maintaining at least a 1–2 m (3–6 feet) distance from other people).” One week later (T2), participants were contacted a second time by the panel company and were asked to self‐report their social distancing behavior over the previous week using the same behavioral measure administered at T1. Participants received a fixed sum of money for their participation based on expected completion time consistent with the panel company’s published rates. Approval for study procedures was granted prior to data collection from the Griffith University Human Research Ethics Committee.
Measures
Study measures were carried out on multi‐item psychometric instruments developed using published guidelines and adapted for use with the target behavior in the current study (Schwarzer, 2008). Participants provided their responses on scales with 7‐point response options. Complete study measures are provided in Table S2.
Social Cognition Constructs. Measures of attitudes, self‐efficacy, risk perceptions, intentions, action planning, coping planning, and action control from the HAPA were developed according to guidelines (Schwarzer, 2007). Attitude was measured using three semantic differential items in response to a common stem: “My maintaining social distancing in the next week would be...”, followed by a series of bi‐polar adjectives (e.g. (1) worthless – (7) valuable). Self‐efficacy was measured using four items (e.g. “I am confident that I could maintain social distancing”, scored (1) strongly disagree to (7) strongly agree). Risk perception was measured using two items (e.g. “It would be risky for me to not maintain social distancing”, scored (1) strongly disagree to (7) strongly agree). Intention was measured using three items (e.g. “I intend to maintain social distancing”, scored (1) strongly disagree to (7) strongly agree). Action planning was measured using four items. Participants were required to respond to the stem: “In the next week, I have made a plan regarding...”, followed by the four items of the scale (e.g. “…when to maintain social distancing”) on Likert scales ranging from strongly disagree (1) to strongly agree (7). Coping planning was measured using four items. Participants were required to respond to the stem: “To keep my intention to maintain social distancing in the next week in difficult situations, I have made a plan...”, followed by the four items of the scale (e.g. “…what to do if something interferes with my goal of maintaining social distancing”) on Likert scales ranging from strongly disagree (1) to strongly agree (7). Action control was measured using three items (e.g. “I have consistently monitored when, how often, and how to maintain social distancing”), scored (1) strongly disagree to (7) strongly agree).
Past Behavior and Behavior.Participants self‐reported their participation in the target behavior maintaining social distancing in relation to others to minimise transmission of the coronavirus that causes COVID‐19. The measure comprised two items prompting participants to report their frequency of social distancing behavior in the previous week: “In the past week, how often did you maintain social distancing?”, scored (1) never to (7) always and “In the past week, I maintained social distancing”, scored (1) false to (7) true.
Demographic Variables. Participants self‐reported their age in years, gender, employment status (currently unemployed/full time caregiver, currently full‐time employed, part‐time employed, on leave without pay/furloughed), marital status (married, widowed, separated/divorced, never married, in a de facto relationship), annual household income stratified by 11 income levels based on Australia and US national averages, and highest level of formal education (completed junior/lower/primary school, completed senior/high/secondary school, post‐school vocational qualification/diploma, further education diploma, undergraduate university degree, postgraduate university degree). Binary income (low income versus middle/high income),1 highest education level (completed school education only versus completed post‐school education), and ethnicity (white/Caucasian versus non‐white) variables were computed for use in subsequent analyses.
Data analysis
Hypothesised relations among HAPA constructs in the proposed model were tested in the Australia and US sample separately using single‐indicator structural equation models implemented in the lavaan package in R (R Core Team, 2020; Rosseel, 2012). We opted for single‐indicator models over a full latent variable structural equation model due to the complexity of the model and the large number of parameters. The single‐indicator approach utilises scale reliabilities to provide an estimate of the measurement error of each variable in the model. Specifically, each variable in the model was indicated by its averaged composite with the error variance fixed at a value based on the reliability estimates using the formula: 1‐reliability*scale variance. Simulation studies have demonstrated that parameter estimates and model fit of single‐indicator models compare very favorably with full latent variable structural equation models, particularly when sample sizes are small (Savalei, 2019).
We freed parameters between the single‐indicator latent variables according to our proposed model. Two models were estimated, one excluding effects of past social distancing behavior (Model 1, Figure 1) and one which controlled for past behavior (Model 2, Figure 2) by freeing parameter estimates from past behavior on each construct in the model. We also controlled for effects of the following demographic variables in each model by freeing paths from each variable to all other model variables: gender, age, ethnicity, income, and education level. Missing data were handled using the full information maximum likelihood (FIML) method. The FIML approach is a preferred approach to handling missing data as simulation studies indicate that it leads to unbiased parameter estimates in structural equation modeling (Enders & Bandalos, 2001; Wothke, 1998).
Model comparisons across the Australia and US samples were conducted using multigroup analyses. An initial configural multisample model for the model excluding past behavior was estimated (Model 3), which provided evidence for the tenability of the model in accounting for the data across both samples. This was followed by a restricted model in which the parameter estimates representing proposed relations among the HAPA constructs and behavior were constrained to equality across the two samples (Model 4). The fit of the constrained model did not differ significantly from the configural model across the two samples, which provided evidence that model parameters did not differ substantially. This was established using a formal likelihood ratio test of the goodness‐of‐fit chi‐square for the configural and constrained models (Byrne et al., 1989). We also examined differences in the CFI; differences of less than .01 between values for the configural and constrained models have also been proposed as indicative of invariance of parameters (Cheung & Rensvold, 2002). The configural (Model 5) and constrained (Model 6) multisample analyses were repeated for the model including past behavior.
Models were implemented using the maximum likelihood estimator with bootstrapped standard errors with 1,000 bootstrap replications. Goodness of fit of the models with the data was evaluated using multiple criteria comparing the proposed model with the baseline model including the goodness‐of‐fit chi‐square (χ2), the comparative fit index (CFI), the standardised root mean‐squared of the residuals (SRMR), and the root mean square error of approximation (RMSEA) and its 90% confidence interval (90% CI). Since the chi‐square value is often statistically significant in complex models and has been shown to lead to the rejection of adequate models, we focused on the incremental fit indices. Specifically, values for the CFI should exceed 0.95, values for the SRMR should be less than or equal to 0.08, and values for the RMSEA should be below 0.05 with a narrow 90% confidence interval (Hu & Bentler, 1999). Data files, analysis scripts, and output are available online: https://osf.io/mrzex/
RESULTS
Participants
Attrition across the two data collection occasions resulted in final sample sizes of 365 (M age = 49.78, SD = 16.89; 50.1% women; attrition rate 26.27%) and 440 (M age = 51.77, SD = 16.26; 46.6% women; attrition rate = 37.23%) participants retained at follow‐up in the Australia and US samples, respectively. There were no missing data for the social cognition and behavior variables as participants could not advance through the survey without providing a response. There were a few instances of missing data for the demographic variables ranging from 0.5 per cent to 8.8 per cent in the Australia sample, and 0.9 per cent to 6.4 per cent in the US sample as participants could opt not to respond to these items as they represented personal data. Missing data are reported in Table S3.
Sample characteristics at follow‐up are presented in Table S4, and comparisons on study variables between those retained in the study at follow‐up and those lost to attrition are presented in Table S3. Attrition analyses in the Australia sample revealed that participants lost to attrition were younger and were more likely to be non‐white. However, there were no differences in proportion of gender, income, and education level. A MANOVA with the social cognition constructs and past behavior as dependent variables and attrition status (lost to attrition vs. included at follow‐up) revealed no differences (Wilks’ Lambda = 0.973, F(8) = 1.60, p = .115, partial η2 = 0.026). Attrition analyses in the US sample also indicated that participants lost to attrition were younger, and more likely to be men, non‐white, and lower educated, and have low income, than those remaining in the study at follow‐up. The MANOVA testing for differences on social cognition and past behavior variables among participants lost to attrition and those included at follow‐up revealed statistically significant differences (Wilks’ Lambda = 0.957, F(8) = 3.90, p < .001, partial η2 = 0.043). Follow‐up tests revealed that mean values for past behavior, attitudes, intentions, and self‐monitoring with respect to social distancing were significantly lower among participants lost to attrition compared to those retained at follow‐up. However, effect sizes for these differences were small (ds < 0.23).
Preliminary Analyses
Descriptive statistics for study variables are presented in Table S4. Participants reported high levels of intention (Australia sample, M = 6.54, SD = 0.66; US sample, M = 6.39, SD = 0.85) and behavior (Australia sample, M = 6.10, SD = 0.67; US sample, M = 6.40, SD = 0.97) with respect to social distancing. Internal consistency of the social cognition constructs was estimated using Revelle's (2018) omega and internal consistency of the behavior variables and risk perception was estimated using the Spearman‐Brown as they comprised two items each. Results are presented in Table S4. All constructs in both samples exhibited acceptable internal consistency, and these data were used to estimate measurement error in subsequent single‐item structural equation models. Scale variance, descriptive statistics, and computed error variance terms used in structural equation models are also presented in Table S4. Correlations among the model constructs and behavior and socio‐demographic variables are presented in Table S5.
Structural Equation Models
The single‐indicator structural equation models that excluded (Model 1) and included (Model 2) past behavior exhibited adequate model fit with the data for both the Australia and US samples (see Table S6). Standardised parameter estimates and distribution statistics for each model in the Australia and US samples are presented in Tables 1 and 2,2 respectively. Focusing first on the models excluding past behavior, intention and action control were statistically significant predictors of social distancing behavior in both samples, with no significant effects for self‐efficacy, action planning, and coping planning. There were also no significant effects of intention on action planning or coping planning in the Australia sample, while intention predicted both planning constructs in the US sample. Self‐efficacy and action control were significant predictors of intention in both samples, with attitudes predicting intention in the Australia sample only and risk perceptions predicting intention in the US sample, although the effect in the Australia sample fell short of statistical significance by a trivial margin (p = .077). There were significant indirect effects of self‐efficacy on behavior mediated by intention in both samples, and significant indirect effects of risk perceptions and action control on behavior mediated by intentions in the US sample only. Intention and action control had significant total effects on behavior in both samples, with a further total effect of self‐efficacy in the US sample.
TABLE 1.
Standardised Path Coefficients for Direct and Indirect Effects for the Single‐Indicator Structural Equation Model of the Health Action Process Approach in the Australia Sample
| Effect | Model excluding past behavior | Model including past behavior | ||||||
|---|---|---|---|---|---|---|---|---|
| β | p | CI95 | β | p | CI95 | |||
| LL | UL | LL | UL | |||||
| Direct effects | ||||||||
| Int → Beh | 0.261 | .026 | 0.027 | 0.445 | −0.077 | .542 | −0.327 | 0.125 |
| AP → Beh | 0.040 | .712 | −0.082 | 0.144 | 0.004 | .966 | −0.094 | 0.110 |
| CP → Beh | −0.041 | .606 | −0.084 | 0.043 | −0.078 | .371 | −0.103 | 0.029 |
| AC → Beh | 0.276 | .024 | 0.036 | 0.303 | 0.174 | .148 | −0.033 | 0.241 |
| SE → Beh | 0.060 | .546 | −0.087 | 0.168 | 0.051 | .566 | −0.081 | 0.157 |
| PB → Beh | – | – | – | – | 0.725 | <.001 | 0.416 | 1.109 |
| Att → Int | 0.182 | .001 | 0.042 | 0.182 | 0.135 | .023 | 0.009 | 0.160 |
| SE → Int | 0.314 | <.001 | 0.135 | 0.326 | 0.241 | <.001 | 0.099 | 0.258 |
| RP → Int | 0.150 | .077 | 0.005 | 0.225 | 0.083 | .290 | −0.032 | 0.168 |
| AC → Int | 0.232 | .006 | 0.046 | 0.256 | 0.158 | .019 | 0.020 | 0.182 |
| PB → Int | – | – | – | – | 0.370 | <.001 | 0.223 | 0.532 |
| Int → AP | 0.074 | .338 | −0.133 | 0.388 | 0.038 | .594 | −0.185 | 0.326 |
| PB → AP | – | – | – | – | 0.357 | <.001 | 0.378 | 0.928 |
| Int → CP | −0.212 | <.001 | −0.746 | −0.243 | −0.244 | <.001 | −0.868 | −0.293 |
| PB → CP | – | – | – | – | 0.421 | <.001 | 0.680 | 1.388 |
| PB → Att | – | – | – | – | 0.326 | <.001 | 0.319 | 0.807 |
| PB → SE | – | – | – | – | 0.359 | <.001 | 0.322 | 0.832 |
| PB → RP | – | – | – | – | 0.417 | <.001 | 0.458 | 0.892 |
| Indirect effects | ||||||||
| Att → Int→Beh | 0.048 | .082 | 0.002 | 0.062 | −0.010 | .545 | −0.026 | 0.015 |
| SE → Int→Beh | 0.082 | .042 | 0.006 | 0.108 | −0.019 | .548 | −0.057 | 0.025 |
| RP → Int→Beh | 0.039 | .262 | −0.001 | 0.076 | −0.006 | .694 | −0.028 | 0.013 |
| AC → Int→Beh | 0.061 | .082 | 0.004 | 0.079 | −0.012 | .598 | −0.042 | 0.012 |
| Int → AP→Beh | 0.003 | .806 | −0.012 | 0.030 | 0.000 | .984 | −0.012 | 0.020 |
| Int → CP→Beh | 0.009 | .628 | −0.022 | 0.045 | 0.019 | .428 | −0.016 | 0.068 |
| Int → Plan→Beh a | 0.012 | .633 | −0.026 | 0.061 | 0.019 | .468 | −0.018 | 0.077 |
| Total effectsb | ||||||||
| Int → Beh | 0.273 | .015 | 0.053 | 0.453 | −0.058 | .621 | −0.289 | 0.131 |
| SE → Beh | 0.142 | .100 | −0.013 | 0.208 | 0.032 | .691 | −0.092 | 0.126 |
| AC → Beh | 0.336 | .007 | 0.063 | 0.336 | 0.162 | .176 | −0.058 | 0.226 |
β = Standardised parameter estimate; CI95 = 95% bootstrapped confidence interval of parameter estimate (unstandardised); LL = Lower limit of CI95; UL = Upper limit of CI95. Int = Intention; Beh = Behavior; AP = Action planning; CP = Coping planning; AC = Action control; SE = Self‐efficacy; PB = Past behavior; Att = Attitude; RP = Risk perceptions.
Sum of indirect effects of both action planning and coping planning on behavior.
TABLE 2.
Standardised Path Coefficients for Direct and Indirect Effects for the Single‐Indicator Structural Equation Model of the Health Action Process Approach in the US Sample
| Effect | Model excluding past behavior | Model including past behavior | ||||||
|---|---|---|---|---|---|---|---|---|
| β | p | CI95 | β | p | CI95 | |||
| LL | UL | LL | UL | |||||
| Direct effects | ||||||||
| Int → Beh | 0.382 | <.001 | 0.152 | 0.602 | 0.054 | .647 | −0.181 | 0.283 |
| AP → Beh | −0.046 | .566 | −0.138 | 0.074 | −0.106 | .193 | −0.191 | 0.033 |
| CP → Beh | −0.012 | .914 | −0.136 | 0.116 | 0.035 | .678 | −0.073 | 0.135 |
| AC → Beh | 0.479 | .001 | 0.159 | 0.573 | 0.182 | .112 | −0.028 | 0.308 |
| SE → Beh | 0.026 | .665 | −0.084 | 0.149 | 0.016 | .785 | −0.103 | 0.137 |
| PB → Beh | – | – | – | – | 0.747 | <.001 | 0.548 | 1.054 |
| Att → Int | 0.082 | .184 | −0.030 | 0.159 | 0.015 | .780 | −0.071 | 0.096 |
| SE → Int | 0.371 | <.001 | 0.247 | 0.506 | 0.347 | <.001 | 0.232 | 0.487 |
| RP → Int | 0.239 | .001 | 0.082 | 0.297 | 0.156 | .017 | 0.028 | 0.219 |
| AC → Int | 0.244 | .001 | 0.082 | 0.294 | 0.079 | .242 | −0.034 | 0.156 |
| PB → Int | – | – | – | – | 0.424 | <.001 | 0.273 | 0.624 |
| Int → AP | 0.190 | .004 | 0.074 | 0.458 | 0.145 | .105 | −0.050 | 0.458 |
| PB → AP | – | – | – | – | 0.439 | <.001 | 0.432 | 0.930 |
| Int → CP | −0.167 | .004 | −0.493 | −0.106 | −0.161 | .023 | −0.531 | −0.072 |
| PB → CP | – | – | – | – | 0.561 | <.001 | 0.748 | 1.268 |
| PB → Att | – | – | – | – | 0.521 | <.001 | 0.548 | 0.807 |
| PB → SE | – | – | – | – | 0.377 | <.001 | 0.292 | 0.527 |
| PB → RP | – | – | – | – | 0.582 | <.001 | 0.682 | 0.956 |
| Indirect effects | ||||||||
| Att → Int→Beh | 0.031 | .292 | −0.010 | 0.086 | 0.001 | .910 | −0.009 | 0.015 |
| SE → Int→Beh | 0.142 | .005 | 0.056 | 0.256 | 0.019 | .652 | −0.065 | 0.107 |
| RP → Int→Beh | 0.091 | .024 | 0.019 | 0.140 | 0.008 | .657 | −0.026 | 0.034 |
| AC → Int→Beh | 0.093 | .023 | 0.021 | 0.137 | 0.004 | .775 | −0.010 | 0.036 |
| Int → AP→Beh | −0.009 | .613 | −0.049 | 0.022 | −0.015 | .299 | −0.045 | 0.014 |
| Int → CP→Beh | 0.002 | .922 | −0.039 | 0.043 | −0.006 | .729 | −0.046 | 0.025 |
| Int → Plan→Beh a | −0.007 | .836 | −0.074 | 0.054 | −0.021 | .397 | −0.075 | 0.027 |
| Total effects a | ||||||||
| Int → Beh | 0.376 | <.001 | 0.177 | 0.577 | 0.033 | .766 | −0.185 | 0.256 |
| SE → Beh | 0.168 | .007 | 0.041 | 0.287 | 0.034 | .512 | −0.071 | 0.140 |
| AC → Beh | 0.572 | <.001 | 0.251 | 0.619 | 0.186 | .105 | −0.022 | 0.313 |
β = Standardised parameter estimate; CI95 = 95% bootstrapped confidence interval of parameter estimate (unstandardised); LL = Lower limit of CI95; UL = Upper limit of CI95. Int = Intention; Beh = Behavior; AP = Action planning; CP = Coping planning; AC = Action control; SE = Self‐efficacy; PB = Past behavior; Att = Attitude; RP = Risk perceptions.
Sum of indirect effects of both action planning and coping planning on behavior.
The total effect is computed as the sum of the indirect effects of the independent variable on the dependent variable through all model variables plus the direct effect.
Inclusion of past behavior led to an attenuation of model effects, consistent with previous research (Brown et al., 2020; Hagger et al., 2018). Notably, effects of all HAPA constructs on behavior were reduced to a trivial size and were not statistically significant. Effects of constructs on intentions remained with the same pattern as those in the model excluding past behavior for both samples, albeit with smaller effect sizes. The only exception was the action control–intention effect, which was reduced to a trivial size and non‐significance in the US sample. Past behavior predicted all model constructs with medium‐to‐large effect sizes in both samples.3
Multi‐Group Analysis
Comparisons of model fit across the Australia and US samples revealed adequate fit of the configural models excluding (Model 3) and including (Model 5) past behavior, lending support for the tenability of the proposed pattern of model effects across the samples (Table S6). Constraining regression coefficients to be invariant for the models including (Model 4) and excluding (Model 6) past behavior resulted in no significant change in model fit according to the goodness‐of‐fit chi‐square and the CFI with differences in the CFI across models less than .01 (Table S6). These findings suggested that any observed differences in the parameter estimates of the models across the Australia and US samples were relatively trivial. This is consistent with the highly consistent pattern of effects in the models in each sample with relatively minor sample‐specific variation.
DISCUSSION
The empirical literature has highlighted the imperative of non‐pharmacological interventions in reducing the transmission of communicable viruses and preventing infection (Jefferson et al., 2011; Rabie & Curtis, 2006; Smith et al., 2015). In the context of the COVID‐19 pandemic, participation in behaviors that prevent virus transmission is essential given the absence of a vaccine or clinically proven pharmacological therapy. Sustained, population‐level participation in such behaviors is not only important to reduce infections in the current pandemic phase, but also in the phases of easing restrictions to avoid a potential “second wave” of infections. There is a pressing need for evidence of potentially modifiable determinants of COVID‐19 preventive behaviors, such as social distancing, on which to base interventions promoting population level participation in these behaviors.
The current study aimed to address this need by identifying the theory based social cognition determinants of social distancing behavior, and the processes involved, in samples from Australia and the US. The study adopted a correlational prospective survey design guided by the HAPA. Consistent with HAPA predictions, intention and action control were identified as significant direct predictors of social distancing behavior in both samples, while intention predicted action planning and coping planning in the US sample. Further, self‐efficacy and action control were identified as significant predictors of intention in both samples. Attitudes and risk perceptions were additional predictors in the Australia and US samples, respectively. Significant indirect effects were also observed; self‐efficacy predicted behavior mediated by intention in both samples, and risk perceptions and action control were found to predict behavior mediated by intentions in the US sample only. Despite these limited differences, it should be noted that comparisons of the models across the Australia and US samples suggested that observed differences in parameter estimates across the samples were relatively trivial. Findings are consistent with the auxiliary assumption promulgated in the HAPA, and social cognition theories more generally, that the effects of the belief‐based constructs reflect generalised processes that have a consistent pattern of effects across contexts, populations, and behaviors. In sum, the current findings indicate that individuals’ social distancing behavior is a function of both motivational and volitional processes, and this provides formative data on potential targets for behavioral interventions aimed at promoting participation in this preventive behavior.
Theoretical Implications
Results of this study provide qualified support for the application of the HAPA, with its focus on constructs that represent dual phases of action. Findings demonstrate a prominent role for self‐efficacy as the key determinant of intentions, and intentions as the key determinant of behavior across both samples. These findings are in line with applications of the HAPA in multiple health behavioral contexts (Zhang, Zhang, et al., 2019), as well as research on social cognition constructs more broadly (Hamilton, van Dongen, & Hagger, 2020; McEachan et al., 2011). Confidence in engaging in health behaviors and capacity to overcome setbacks and barriers have been consistently linked with future behavioral performance (Warner & French, 2020). The pervasive effect of intention on behavior is also aligned with a substantive literature on social cognition theories demonstrating intentions as the pre‐eminent determinant of behavior (Hamilton, van Dongen, et al., 2020; McEachan et al., 2011). Overall, these effects suggest that social distancing behavior should be conceptualised as a reasoned action.
However, the current study also demonstrated a prominent role for constructs representing volitional processes in the enactment of behavior. In particular, action control, a construct reflecting individuals’ application of key self‐regulatory skills to enact behavior, was a consistent predictor of both intentions and behavior across the samples. Individuals possessing these skills are not only more likely to form intentions to perform social distancing behaviors, but are also more likely to engage in the behavior through, for example, an automatic process. Specifically, the direct effect not mediated by intentions suggests that individuals with good action control might be more effective in structuring their environment or forming habits that promote enactment of social distancing without the need for extensive deliberation or weighing up of options. Over time, these individuals are likely to form habits, that is, performance of behaviors that are activated through cues and contexts independent of the goals and intentions that originally gave rise to them (Aarts et al., 1998; Hagger, 2019; Verplanken & Orbell, 2003; Wood, 2017). Research has suggested that individuals possessing these skills are effective in controlling their actions more broadly, but also that such skills can be acquired or learned (Gardner, 2015; Gardner et al., 2020), which provides a potential avenue for intervention: training people to be more effective in regulating their own actions.
Interestingly, current research shows that risk perceptions have small effects on intentions and subsequent behavior. Risk perceptions had small but significant effects in the US sample, and a small effect which fell short of statistical significance in the Australia sample. This pattern of effects is consistent with applications of the HAPA and other social cognition models like protection motivation theory, which found relatively modest or null effects of risk perceptions on intentions and behavior (Zhang, Chung, et al., 2019). In the context of COVID‐19 prevention and social distancing behavior, it is common knowledge that the infection will not have serious consequences for the majority of the population, and is likely only to be serious for those with underlying conditions or impaired immunity, or the elderly. As a consequence, perceived risk may not be a major influence on decisions to act. Instead, it seems that self‐efficacy and action control are more pervasive and consistent determinants of behavior, and these may be more pertinent targets for intervention.
Action and coping planning were expected to mediate intention–behavior effects in the current model, such that planning is an important part of the process of intention enactment for social distancing. However, findings indicated that neither form of planning mediated intention effects on behavior, contrary to HAPA predictions. These findings are not, however, unique, and previous research has demonstrated considerable variability in the role of planning in intention enactment, and effect sizes are often small (Rhodes et al., 2020; Zhang et al., 2019). Taken together, it seems that volitional processes such as action control are far more pervasive in promoting social distancing intentions and behavior.
Introduction of past behavior in the current model had marked influences on the size of model effects, rendering effects of almost all model constructs on intentions and behavior trivial and not statistically significant. One interpretation of these findings is that the current model is not sufficient in accounting for social distancing over time. However, it was not unexpected that past behavior would have pervasive effects on subsequent behavior over such short range prediction and, given the high stability of social distancing behavior, it is unsurprising that it accounts for model effects over time. It must also be stressed that past behavior alone is not a construct and does not, therefore, offer any information other than on the stability of social distancing behavior (Ouellette & Wood, 1998). Some have proposed that past behavior is indicative of habitual influences on behavior, but research examining habit as a construct suggests that it is more than performing a behavior frequently, and that the quality of the behavioral experience, such as experiencing it as automatic or without explicit thought, better characterises habitual processes (Aarts et al., 1998; Hagger, 2019; Verplanken & Orbell, 2003). Nevertheless, the residual effect of past behavior may provide some indication of unmeasured constructs on subsequent behavior, particularly those that bypass effects of intentions and are more likely rooted in non‐conscious processes that lead to behavior, such as implicit attitudes or motives.
Practical Implications
Research applying social cognition models like the HAPA provides useful guidance for the development of future behavioral interventions aimed at promoting social distancing behaviors. Although participants’ intentions toward, and actual participation in, social distancing behavior were relatively high, scores and variability estimates suggested that some participants were reporting lapses in their social distancing behavior. Such lapses present considerable risks to coronavirus transmission, particularly in areas of high prevalence where the likelihood of contact with infected persons is substantially elevated. Our research provides some indication of the constructs that should be targeted for change and also the types of behavior change techniques that make up the content of interventions (Hagger, Cameron, et al, 2020; Hagger, Smith, et al., 2020; Kok et al., 2016). Based on current findings, strategies to promote self‐efficacy should be foremost in potential targets of interventions to promote intentions and behavior. Interventions that have manipulated mastery experience (i.e. practicing a behavior) and vicarious experience (i.e. observing a model performing the behavior) have been shown to be successful in strengthening self‐efficacy, as have interventions that provide feedback on past or others’ performance (Warner & French, 2020). Tailoring of these strategies could also be considered and targeted at uptake of the behavior for those that have not already adopted the behavior (e.g. demonstration of appropriate social distance when in line to purchase goods) or at maintenance of the behavior (e.g. developing a rule of thumb on keeping an appropriate social distance every time when in line to purchase goods).
Action control was another key determinant of intentions and behavior. This suggests that it is important that individuals acquire monitoring and self‐regulatory strategies with respect to their social distancing behavior. For example, action control involves consistent monitoring as to whether an individual follows through on their intentions for the target behavior (Schwarzer & Hamilton, 2020). Monitoring helps identify discrepancies in behavior (e.g. not being at an appropriate social distance when in line to purchase goods), and noting a discrepancy can trigger taking additional action to ensure goals are achieved (e.g. adjusting the distance) or for disengaging from the goal (e.g. abandoning the goods and leaving the shop) (Webb & de Bruin, 2020). In order to promote better action control, interventions may prompt self‐monitoring (e.g. through self‐observation of social distancing behavior) or be monitored by others (e.g. shop attendant prompts an individual to increase their social distance).
Given that constructs such as attitudes and risk perceptions were not strong, consistent determinants of social distancing behavior, strategies targeting change in these constructs may not be at the forefront of behavioral interventions to promote social distancing. However, context‐specific interventions that target change in attitudes for individuals in Australia and risk perceptions, particularly for individuals in the US, may assist in promoting stronger intentions. Strategies aimed at promoting attitude change and increased risk perceptions usually involve information provision (e.g. providing information about health consequences, highlighting the pros over the cons of social distancing) and communication‐persuasion (e.g. using credible sources to deliver messages, using framing/reframing methods) about the importance of maintaining social distancing (Hamilton & Johnson, 2020). However, reviews suggest that such strategies relate more to short‐term change rather than sustained, longer‐term impact on behavior (Jepson et al., 2010). Another approach could be the use of fear appeals which seek to arouse negative emotional reactions in order to promote self‐protective motivation and action (Kok et al., 2016). However, caution is needed when using fear appeals to attempt to change behavior as excessively heightened fear may be counter‐productive in motivating individuals to engage in preventive behaviors (Kok et al., 2018; Lin, 2020), and may even be counter‐productive because they are responses aimed at mitigating fear, such as avoidance or denial, neither of which may manage the risk itself (Hagger et al., 2017; Leventhal et al., 1998). There is evidence that messages that highlight risk but also provide coping information to increase self‐efficacy (Kok et al., 2018) and that use positive prosocial language (Heffner et al., 2020) may be effective because they are more readily accepted and prevent defensive and avoidant reactions. However, current evidence suggests that interventions targeting change in attitudes and risk perception are unlikely to be enough to promote social distancing.
Strengths, Limitations, and Avenues for Future Research
The present research has a number of strengths including focus on social distancing, a key preventive behavior aimed at reducing transmission of SARS‐CoV‐2 to prevent COVID‐19 infections; adoption of a fit‐for‐purpose theoretical model, the HAPA, that provides a set of a priori predictions on the motivational and volitional determinants of the target behavior; recruitment of samples from two countries, Australia and the US, with key demographic characteristics that closely match those of the population; and the use of prospective study design and structural equation modelling techniques. A number of limitations to the current data should also be noted. That there was substantive attrition at follow‐up in both samples is an important limitation. Non‐trivial attrition could result in selection bias. For example, participants who are more motivated or engaged may be overrepresented in the sample. In the current study, participants were provided with multiple reminders to complete measures at follow‐up, but more intensive recruitment and incentivisation of non‐responders may have further minimised attrition rates. It should be noted that participant drop‐out affected the demographic profile of the samples, particularly among underrepresented groups. This is particularly relevant to the current context given data indicating that COVID‐19 infection and mortality rates are higher in underrepresented minority and socioeconomic groups (CDC, 2020). A potential solution would be to oversample in underrepresented groups in which attrition rates are likely to be high and should be considered in future research. Furthermore, our recruitment strategy was focused on producing samples with characteristics that corresponded with those of the national population on gender and state. However, the samples were not stratified by salient demographic or socioeconomic variables. The current samples cannot be characterised as representative of the Australian or US population. Taking these biases into account, the current findings should not be considered directly generalisable to the broader population.
In addition, the current study adopted a prospective design, which provided a basis for the temporal ordering of constructs in the model. However, the correlational design of the current study means that inferences of causality are based on theory rather than the data. Furthermore, the current design did not permit modeling of the stability or change in model constructs over time. The latter represents an important caveat when utilising current data as a basis for intervention. Future research should aim to adopt cross‐lagged panel designs that model change in constructs over time, and utilise intervention or experimental designs that target change in model constructs and observe their effects on behavior. Also, the study was conducted over a one‐week period. Although this is a relatively brief follow‐up period, it was considered appropriate given the high speed of virus transmission and the need for prompt adoption of social distancing in the population to prevent widespread infection. The current results, however, do not confirm the extent to which model constructs predict social distancing over a longer period, and long‐term follow‐up would be necessary to support the application of the HAPA in accounting for maintenance of social distancing, which is especially important as lockdown restrictions ease in order to prevent a “second wave” of infection. The present study also relied exclusively on self‐report measures which may introduce additional error variance through recall bias and socially desirable responding. Future studies may consider verification of behavioral data with non‐self‐report data such as the use of GPS mapping of mobile phones or using observation to verify rates of social distancing behavior in particular contexts (e.g. workplaces, grocery stores). It might also be useful for future studies to investigate the role of social factors, as suggested in the HAPA, on social distancing behavior. This is particularly important given the considerable potential for “social” influences to affect individuals’ behavior in minimising person‐to‐person contact with others outside the individual’s immediate household. Precedence for these effects comes from previous research which has found that pressure from important others and moral obligation toward others predicts adherence to COVID‐19 preventive behaviors, including social distancing (Hagger, Cameron, et al, 2020; Hagger, Smith, et al., 2020; Lin et al., 2020). Finally, this research was conducted during a period when it is likely that participants were already engaging in social distancing and, thus, already had substantive experience with the behavior, indicated by the high scale mean scores for past behavior (M = 6.5 on a 7‐point scale) in both samples. This likely explains the substantive effect of past behavior in attenuating model effects and the need for longitudinal designs or using methods such as ecological momentary assessment that capture moment‐by‐moment changes over time in behavior.
CONCLUSION
Given the urgent need for populations to adopt COVID‐19 preventive behaviors, such as social distancing, the present study applied the HAPA to predict key motivational and volitional determinants of social distancing behavior in samples across two different countries, Australia and the US. Overall, the current findings provide qualified support for some of the core proposed effects among the motivational and volitional factors in the model, as well as their effects on individuals’ social distancing behavior. The current study fills a knowledge gap in the literature on the social psychological processes that guide social distancing behavior in an unprecedented context of a pandemic and suggests that the motivational and volitional constructs of self‐efficacy, intention, and action control, in particular, may have utility in explaining this important COVID‐19 preventive behavior. Despite the correlational design, the current findings suggest multiple potential routes to behavioral performance that can serve as a basis for the development of intervention and enable further testing of effects of the techniques on both behavior change and the targeted theory constructs.
Supporting information
Table S1. Sample Characteristics and Descriptive Statistics for Study Variables at Baseline and at One‐Week Follow‐Up.
Table S2. Items and Response Scales for Health Action Process Approach Variables.
Table S3. Attrition Analyses Comparing Differences on Demographic Variables and Social Cognition Constructs for Participants Included at Follow‐Up and Participants Lost to Attrition.
Table S4. Factor Loadings, Reliability Estimates, ErrorVariances, and Descriptive Statistics for the Health Action Process Approach Variables.
Table S5. Intercorrelations Among Model Variables Used in Single‐Indicator Structural Equation Models.
Table S6. Goodness‐of‐Fit Statistics for the Single‐Indicator Structural Equation Model of the Health Action Process Approach in the Australian and US Samples and Multigroup Models with Comparisons.
Table S7. Standardized Path Coefficients for Direct and Indirect Effects for the Single‐Indicator Structural Equation Model of the Health Action Process Approach in the Australian Sample.
Table S8. Standardized Path Coefficients for Direct and Indirect Effects for the Single‐Indicator Structural Equation Model of the Health Action Process Approach in the US Sample.
Acknowledgements
Martin S. Hagger’s contribution was supported by a Finland Distinguished Professor (FiDiPro) award (Dnro 1801/31/2105) from Business Finland.
Footnotes
Our cut‐off for low vs. medium‐to‐high income was based on national income data for citizens on low incomes in the US (for a family of four, the low income threshold is US$25,465 per year; Semega et al., 2020) and Australia (for a family of four, the low‐income average is $562 per week; AIHW 2020). Participants reporting incomes of $400–$599 per week ($20,800–$31,199 per year) or below were classified as low income.
Full parameter estimates for the models in the Australia and US samples are provided in Tables S7 and S8, respectively.
The social distancing behavior and past behavior variables were associated with large skewness and kurtosis values. We checked to see whether the skewness and kurtosis values affected findings. So, we re‐estimated our structural equation models using a square root transformation of these variables. The reanalysis revealed virtually identical coefficients and the exact pattern of effects found for the analysis using the untransformed behavior variables. Analysis scripts and output for this auxiliary analysis are available online: https://osf.io/mrzex/?view_only=3ae43e6fa81c48c6880e65d068f5435b
DATA AVAILABILITY STATEMENT
Data files and analysis scripts are available online from the Open Science Framework project for this study: https://osf.io/mrzex/?view_only=3ae43e6fa81c48c6880e65d068f5435b
REFERENCES
- Aarts, H. , Verplanken, B. , & van Knippenberg, A. (1998). Predicting behavior from actions in the past: Repeated decision making or a matter of habit? Journal of Applied Social Psychology, 28(15), 1355–1374. 10.1111/j.1559-1816.1998.tb01681.x [DOI] [Google Scholar]
- AIHW (2020). Australia's children. Canberra: Australian Institute of Health and Welfare. Retrieved 25 August 2020 from: https://www.aihw.gov.au/reports/children‐youth/australias‐children/contents/income‐finance‐and‐employment‐snapshots/family‐economic‐situation [Google Scholar]
- Brown, D.J. , Hagger, M.S. , & Hamilton, K. (2020). The mediating role of reasoned‐action and automatic processes from past‐to‐future behavior across three health behaviors. Social Science and Medicine, 258, 113085. 10.1016/j.socscimed.2020.113085 [DOI] [PubMed] [Google Scholar]
- Byrne, B.M. , Shavelson, R.J. , & Muthén, B. (1989). Testing for the equivalence of factor covariance and means structures: The issue of partial measurement invariance. Psychological Bulletin, 105, 456–466. 10.1037/0033-2909.105.3.456 [DOI] [Google Scholar]
- CDC (2020). COVID‐19 in racial and ethnic minority groups. Retrieved 25 June 2020 from: https://www.cdc.gov/coronavirus/2019‐ncov/need‐extra‐precautions/racial‐ethnic‐minorities.html [Google Scholar]
- Cheung, G.W. , & Rensvold, R.B. (2002). Evaluating goodness‐of‐fit indexes for testing measurement invariance. Structural Equation Modeling, 9, 233–255. 10.1207/S15328007SEM0902_5 [DOI] [Google Scholar]
- Chu, D.K. , Akl, E.A. , Duda, S. , Solo, K. , Yaacoub, S. , Schünemann, H.J. , … Schünemann, H.J. (2020). Physical distancing, face masks, and eye protection to prevent person‐to‐person transmission of SARS‐CoV‐2 and COVID‐19: A systematic review and meta‐analysis. The Lancet, 395, 1973–1987. 10.1016/S0140-6736(20)31142-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders, C.K. , & Bandalos, D.L. (2001). The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling, 8(3), 430–457. 10.1207/S15328007SEM0803_5 [DOI] [Google Scholar]
- Gardner, B. (2015). A review and analysis of the use of “habit” in understanding, predicting and influencing health‐related behaviour. Health Psychology Review, 9(3), 277–295. 10.1080/17437199.2013.876238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gardner, B. , Rebar, A. , & Lally, P. (2020). Habit interventions. In Hagger M.S., Cameron L., Hamilton K., Hankonen, N. & Lintunen T. (Eds.), Handbook of behavior change (pp. 599–616). Cambridge: Cambridge University Press. [Google Scholar]
- Hagger M. S. (2019). Habit and physical activity: Theoretical advances, practical implications, and agenda for future research. Psychology of Sport and Exercise, 42, 118–129. 10.1016/j.psychsport.2018.12.007 [DOI] [Google Scholar]
- Hagger M. S., Polet J., Lintunen T. (2018). The reasoned action approach applied to health behavior: Role of past behavior and tests of some key moderators using meta‐analytic structural equation modeling. Social Science & Medicine, 213, 85–94. 10.1016/j.socscimed.2018.07.038 [DOI] [PubMed] [Google Scholar]
- Hagger, M.S. , Cameron, L. , Hamilton, K. , Hankonen, N. , & Lintunen, T. (Eds.) (2020). Handbook of behavior change. Cambridge: Cambridge University Press. 10.1017/9781108677318 [DOI] [Google Scholar]
- Hagger, M.S. , Koch, S. , Chatzisarantis, N.L.D. , & Orbell, S. (2017). The common sense model of self‐regulation: Meta‐analysis and test of a process model. Psychological Bulletin, 143(11), 1117–1154. 10.1037/bul0000118 [DOI] [PubMed] [Google Scholar]
- Hagger, M.S. , Smith, S.R. , Keech, J.J. , Moyers, S.A. , & Hamilton, K. (2020). Predicting social distancing behavior during the COVID‐19 pandemic: An integrated social cognition model. Annals of Behavioral Medicine, 10.1093/abm/kaaa073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton, K. , Cornish, S. , Kirkpatrick, A. , Kroon, J. , & Schwarzer, R. (2018). Parental supervision for their children's toothbrushing: Mediating effects of planning, self‐efficacy, and action control. British Journal of Health Psychology, 23(2), 387–406. 10.1111/bjhp.12294 [DOI] [PubMed] [Google Scholar]
- Hamilton, K. , & Johnson, B.T. (2020). Attitude and persuasive communication interventions. In Hagger M.S., Cameron L., Hamilton K., Hankonen, N. & Lintunen T. (Eds.), Handbook of behavior change (pp. 445–460). Cambridge: Cambridge University Press. 10.1017/97811086773180.031 [DOI] [Google Scholar]
- Hamilton, K. , van Dongen, A. , & Hagger, M.S. (2020). An extended theory of planned behavior for parent‐for‐child health behaviors: A meta‐analysis. Health Psychology, 10.1037/hea0000940 [DOI] [PubMed] [Google Scholar]
- Heffner, J. , Vives, M. , & FeldmanHall, O. (2020). Emotional responses to prosocial messages increase willingness to self‐isolate during the COVID‐19 pandemic. PsyArXiv Preprint. 10.31234/osf.io/qkxvb [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu, L. , & Bentler, P.M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Islam, N. , Sharp, S.J. , Chowell, G. , Shabnam, S. , Kawachi, I. , Lacey, B. , … White, M. (2020). Physical distancing interventions and incidence of coronavirus disease 2019: Natural experiment in 149 countries. BMJ, 370, m2743. 10.1136/bmj.m2743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jefferson, T. , Del Mar, C.B. , Dooley, L. , Ferroni, E. , Al‐Ansary, L.A. , Bawazeer, G.A. , … Conly, J.M. (2011). Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database of Systematic Reviews, 7, CD006207. 10.1002/14651858.CD006207.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jepson, R.G. , Harris, F.M. , Platt, S. , & Tannahill, C. (2010). The effectiveness of interventions to change six health behaviours: A review of reviews. BMC Public Health, 10(1), 538. 10.1186/1471-2458-10-538 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kok, G. , Gottlieb, N.H. , Peters, G.‐J.Y. , Mullen, P.D. , Parcel, G.S. , Ruiter, R.A. , … Bartholomew, L.K. (2016). A taxonomy of behaviour change methods: An Intervention mapping approach. Health Psychology Review, 10(3), 297–312. 10.1080/17437199.2015.1077155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kok, G. , Peters, G.‐J.Y. , Kessels, L.T.E. , ten Hoor, G.A. , & Ruiter, R.A.C. (2018). Ignoring theory and misinterpreting evidence: The false belief in fear appeals. Health Psychology Review, 12(2), 111–125. 10.1080/17437199.2017.1415767 [DOI] [PubMed] [Google Scholar]
- Leventhal, H. , Leventhal, E.A. , & Contrada, R.J. (1998). Self‐regulation, health, and behavior: A perceptual‐cognitive approach. Psychology & Health, 13(4), 717–733. 10.1080/08870449808407425 [DOI] [Google Scholar]
- Lin, C.‐Y. (2020). Social reaction toward the 2019 novel coronavirus (COVID‐19) [Editorial]. Social Health and Behavior, 3(1), 1–2. 10.4103/SHB.SHB_11_20 [DOI] [Google Scholar]
- Lin, C.‐Y. , Imani, V. , Rajabi Majd, V. , Ghasemi, Z. , Griffiths, M.D. , Hamilton, K. , … Pakpour, A.H. (2020). Using an integrated social cognition model to predict COVID‐19 preventive behaviors. British Journal of Health Psychology, 10.1111/bjhp.12465 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lunn, P.D. , Timmons, S. , Barjaková, M. , Belton, C.A. , Julienne, H. , & Lavin, C. (2020). Motivating social distancing during the COVID‐19 pandemic: An online experiment. https://www.esri.ie/pubs/WP658.pdf [DOI] [PubMed] [Google Scholar]
- McEachan, R.R.C. , Conner, M. , Taylor, N.J. , & Lawton, R.J. (2011). Prospective prediction of health‐related behaviours with the Theory of Planned Behaviour: A meta‐analysis. Health Psychology Review, 5(2), 97–144. 10.1080/17437199.2010.521684 [DOI] [Google Scholar]
- Michie, S. , West, R. , Rogers, M.B. , Bonell, C. , Rubin, G.J. , & Amlôt, R. (2020). Reducing SARS‐CoV‐2 transmission in the UK: A behavioural science approach to identifying options for increasing adherence to social distancing and shielding vulnerable people. British Journal of Health Psychology, 10.1111/bjhp.12428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ouellette J. A., Wood W. (1998). Habit and intention in everyday life: The multiple processes by which past behavior predicts future behavior.. Psychological Bulletin, 124, (1), 54–74. 10.1037/0033-2909.124.1.54 [DOI] [Google Scholar]
- R Core Team (2020). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing. https://www.R‐project.org/ [Google Scholar]
- Rabie, T. , & Curtis, V. (2006). Handwashing and risk of respiratory infections: A quantitative systematic review. Tropical Medicine and International Health, 11(3), 258–267. 10.1111/j.1365-3156.2006.01568.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Revelle, W. (2018). psych: Procedures for psychological, psychometric, and personality research. https://cran.r‐project.org/web/packages/psych/index.html [Google Scholar]
- Reyes Fernández, B. , Knoll, N. , Hamilton, K. , & Schwarzer, R. (2016). Social‐cognitive antecedents of hand washing: Action control bridges the planning–behaviour gap. Psychology & Health, 31(8), 993–1004. 10.1080/08870446.2016.1174236 [DOI] [PubMed] [Google Scholar]
- Rhodes, R. , Grant, S. , & de Bruin, G.‐J. (2020). Planning and implementation intention interventions. In Hagger M.S., Cameron L., Hamilton K., Hankonen, N. & Lintunen T. (Eds.), Handbook of behavior change (pp. 572–585). Cambridge: Cambridge University Press. [Google Scholar]
- Rosseel, Y. (2012). Lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36. https://doi.org/http://www.jstatsoft.org/v48/i02/ [Google Scholar]
- Savalei, V. (2019). A comparison of several approaches for controlling measurement error in small samples. Psychological Methods, 24, 352–370. 10.1037/met0000181 [DOI] [PubMed] [Google Scholar]
- Schwarzer, R. (2007). The Health Action Process Approach (HAPA): Assessment tools. http://www.hapa‐model.de/ [Google Scholar]
- Schwarzer, R. (2008). Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Applied Psychology: An International Review, 57(1), 1–29. 10.1111/j.1464-0597.2007.00325.x [DOI] [Google Scholar]
- Schwarzer, R. , & Hamilton, K. (2020). Changing behaviour using the health action process approach. In Hagger M.S., Cameron L., Hamilton K., Hankonen, N. & Lintunen T. (Eds.), Handbook of behavior change (pp. 89–103). Cambridge: Cambridge University Press. [Google Scholar]
- Semega, J. , Kollar, M. , Creamer, J. , & Mohanty, A. (2020). Income and poverty in the United States: 2018. United States Census Bureau. [Google Scholar]
- Smith, S.M.S. , Sonego, S. , Wallen, G.R. , Waterer, G. , Cheng, A.C. , & Thompson, P. (2015). Use of non‐pharmaceutical interventions to reduce the transmission of influenza in adults: A systematic review. Respirology, 20(6), 896–903. 10.1111/resp.12541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teasdale, E. , Santer, M. , Geraghty, A.W.A. , Little, P. , & Yardley, L. (2014). Public perceptions of non‐pharmaceutical interventions for reducing transmission of respiratory infection: Systematic review and synthesis of qualitative studies. BMC Public Health, 14(1), 589. 10.1186/1471-2458-14-589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- British Psychological Society (2020). Behavioural science and disease prevention: Psychological guidance. https://www.bps.org.uk/sites/www.bps.org.uk/files/Policy/Policy%20‐%20Files/Behavioural%20science%20and%20disease%20prevention%20‐%20Psychological%20guidance%20for%20optimising%20policies%20and%20communication.pdf [Google Scholar]
- Verplanken, B. , & Orbell, S. (2003). Reflections on past behavior: A self‐report index of habit strength. Journal of Applied Social Psychology, 33(6), 1313–1330. [Google Scholar]
- Warner, L.M. , & French, D.P. (2020). Confidence and self‐efficacy interventions. In Hagger M.S., Cameron L., Hamilton K., Hankonen, N. & Lintunen T. (Eds.), Handbook of behavior change (pp. 461–478). Cambridge: Cambridge University Press. 10.1017/97811086773180.032 [DOI] [Google Scholar]
- Webb, T.L. , & de Bruin, M. (2020). Monitoring interventions. In Hagger M.S., Cameron L., Hamilton K., Hankonen, N. & Lintunen T. (Eds.), Handbook of behavior change (pp. 537–553). Cambridge: Cambridge University Press. [Google Scholar]
- West, R. , Michie, S. , Rubin, G.J. , & Amlôt, R. (2020). Applying principles of behaviour change to reduce SARS‐CoV‐2 transmission. Nature Human Behaviour, 4(5), 451–459. 10.1038/s41562-020-0887-9 [DOI] [PubMed] [Google Scholar]
- Wood, W. (2017). Habit in personality and social psychology. Personality and Social Psychology Review, 21(4), 389–403. 10.1177/1088868317720362 [DOI] [PubMed] [Google Scholar]
- World Health Organization (2020). Coronavirus disease (COVID‐19) advice for the public. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019/advice‐for‐public [Google Scholar]
- Worldometer (2020). Worldometer COVID‐19 coronavirus pandemic. https://www.worldometers.info/coronavirus/ [Google Scholar]
- Wothke, W. (1998). Longitudinal and multi‐group modeling with missing data. In Little, K.U. Schnabel, & J. Baumert T.D. (Eds.), Modeling longitudinal and multiple group data: Practical issues, applied approaches and specific examples (pp. 2019–2240). Mahwah, NJ: Lawrence Erlbaum Publishers. [Google Scholar]
- Zhang, C.‐Q. , Chung, P.‐K. , Liu, J.‐D. , Chan, D.K.C. , Hagger, M.S. , & Hamilton, K. (2019). Health beliefs of wearing facemasks for Influenza A/H1N1 prevention: A qualitative investigation of Hong Kong older adults. Asia Pacific Journal of Public Health, 31(3), 246–256. 10.1177/1010539519844082 [DOI] [PubMed] [Google Scholar]
- Zhang, C.‐Q. , Fang, R. , Zhang, R. , Hagger, M.S. , & Hamilton, K. (2020). Predicting hand washing and sleep hygiene behaviors among college students: Test of an integrated social‐cognition model. International Journal of Environmental Research and Public Health, 17, 1209. 10.3390/ijerph17041209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, C.‐Q. , Zhang, R. , Schwarzer, R. , & Hagger, M.S. (2019). A meta‐analysis of the health action process approach. Health Psychology, 38(7), 623–637. 10.1037/hea0000728 [DOI] [PubMed] [Google Scholar]
- Zhou, G. , Gan, Y. , Miao, M. , Hamilton, K. , Knoll, N. , & Schwarzer, R. (2015). The role of action control and action planning on fruit and vegetable consumption. Appetite, 91, 64–68. 10.1016/j.appet.2015.03.022 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Sample Characteristics and Descriptive Statistics for Study Variables at Baseline and at One‐Week Follow‐Up.
Table S2. Items and Response Scales for Health Action Process Approach Variables.
Table S3. Attrition Analyses Comparing Differences on Demographic Variables and Social Cognition Constructs for Participants Included at Follow‐Up and Participants Lost to Attrition.
Table S4. Factor Loadings, Reliability Estimates, ErrorVariances, and Descriptive Statistics for the Health Action Process Approach Variables.
Table S5. Intercorrelations Among Model Variables Used in Single‐Indicator Structural Equation Models.
Table S6. Goodness‐of‐Fit Statistics for the Single‐Indicator Structural Equation Model of the Health Action Process Approach in the Australian and US Samples and Multigroup Models with Comparisons.
Table S7. Standardized Path Coefficients for Direct and Indirect Effects for the Single‐Indicator Structural Equation Model of the Health Action Process Approach in the Australian Sample.
Table S8. Standardized Path Coefficients for Direct and Indirect Effects for the Single‐Indicator Structural Equation Model of the Health Action Process Approach in the US Sample.
Data Availability Statement
Data files and analysis scripts are available online from the Open Science Framework project for this study: https://osf.io/mrzex/?view_only=3ae43e6fa81c48c6880e65d068f5435b