

Abstract
Background
A clear picture of people’s adoption of protective behaviours, and a thorough understanding of psychosocial correlates in the context of contagious diseases such as COVID‐19, is essential for the development of communication strategies, and can contribute to the fight against epidemics.
Methods
In this paper, we report a survey on the adoption of the recommended protective behaviours before and during the epidemic. We also assessed demographic correlates, and beliefs (towards COVID‐19 and protective behaviours, towards SARS‐CoV‐2 transmission, social dilemma variables, and perceived external cues) of a representative sample of British residents. Data were collected during the early stage of the COVID‐19 epidemic that spread worldwide in 2020.
Results
Results showed a marked increase in the adoption of protective behaviour. We also identified targets for intervention in variables related to transmission of the virus and social dilemma‐related beliefs. Sex differences in the adoption of protective measures, as well as differences associated with the frequency of social contacts, were associated with differences in beliefs.
Conclusions
These findings suggest changeable determinants, which could be targeted in global communication about COVID‐19, or in interventions targeting specific sub‐groups not following the protective measures.
Keywords: epidemic, HBM, pandemic, psychological factors, social dilemma
INTRODUCTION
The novel coronavirus disease (COVID‐19), an infectious illness caused by SARS‐CoV‐2, emerged in December 2019 and has rapidly created a global health emergency of unprecedented scale in recent history. Over four months, the COVID‐19 outbreak has gone from being relatively contained in Hubei province, China, to affecting almost every country. The World Health Organization (2020) declared a pandemic on 11 March. In an effort to stem the epidemic, countries encouraged people to adopt a range of protective behaviours, such as social distancing or frequent handwashing. However, such measures are only effective if protective behaviours are widely adopted by the population (Hallsworth, 2020; Michie et al., 2020). Moreover, in critical situations such as this pandemic, where rapid behaviour change is necessary, it is crucial that public health policies and interventions be evidence‐based, rather than rely on intuition (Faggiano et al., 2014; Wilson & Juarez, 2015). Having a clear picture of people’s adoption of protective behaviours, and a thorough understanding of psychosocial correlates in the context of COVID‐19, can inform communication strategies and contribute to fighting against the present and future outbreaks (Arden & Chilcot, 2020). In this paper, we report a survey on protective behaviours, beliefs towards the outbreak, and demographic correlates of a representative sample of British residents.
In their review of research on protective behaviours during pandemics, Bish and Michie (2010, 2011) identified a number of demographic and attitudinal determinants: sex, age, education level, external cues, sense of vulnerability, perceived severity of the illness, social norms, perceived efficacy and barriers, and trust in authorities. Beyond the elements addressed by Bish and Michie (2011), much remains to be learned.
First, rarely have the aforementioned determinants of protective behaviours been examined simultaneously in one study, and the potential links between demographic characteristics and beliefs (i.e. mediation relationship, Desrichard et al., 2007) remain underexplored.
Second, most research has focused on the determinants of motivation to protect oneself from the disease (Geldsetzer, 2020; Wolf et al., 2020; but see Luttrell & Petty, 2020). However, the COVID‐19 outbreak highlights another function of protective behaviours: to avoid transmitting the virus to others. This pro‐social motivation is particularly relevant, as emphasis has been placed on the low severity of COVID‐19 in some groups (i.e. younger people). Amongst these less‐concerned groups, the motivation to protect oneself may be lower than the motivation to protect others (i.e. more vulnerable groups) or to participate in reducing the spread of the epidemic.
Third, communication regarding the COVID‐19 epidemic also emphasises the collective aspect of the fight. Therefore, motivation to adopt protective behaviours can take the form of a large‐scale social dilemma (Ling Hoh Teck & Chyong, 2020) wherein individuals’ immediate personal interests are in conflict with collective interests (Attari et al., 2014; Van Lange et al., 2013). A number of variables may play a role in influencing people’s cooperation in social dilemmas, such as perceived descriptive norm (perception of what others are doing) (Cialdini et al., 1990), perceived collective efficacy (“Are we able to do it?”) (Koletsou & Mancy, 2011), collective outcome expectancy (one’s belief that collective behaviour can contribute to reducing the spread of the epidemic) (Moussaoui & Desrichard, 2016), reverse altruism (not engaging in the behaviour because only others would benefit from it) (Attari et al., 2014), "drop‐in‐the‐bucket" feeling (one is disinclined to act because it seems one’s contribution will be too small to make a tangible difference) (Attari et al., 2014; Bonniface & Henley, 2008), the “sucker effect” (one does not act because nobody else is doing so, thus one would look like a sucker for making an effort) (Kerr, 1983; Orbell & Dawes, 1981), and “free‐riding” (one does not see the need to act, because many other people are doing so, and one’s contribution thus seems unnecessary) (Orbell & Dawes, 1981). Though some of these variables have been studied in health‐related contexts (e.g. vaccination; Betsch et al., 2013; Ibuka et al., 2014)), they have yet to be examined during a pandemic.
Finally, the majority of past research has been conducted after the acute phase of the epidemic episode, with retrospective designs—yet studying people’s responses during the crisis constitutes an invaluable opportunity to better understand the processes at work.
The Current Research
The primary aims of this research are to capture people’s protective behaviour and the extent to which it has changed, examine demographic and beliefs correlates of such behaviours, and explore the relationships between these variables. In our research, we draw on the Health Belief Model (Rosenstock, 1974) and social dilemma frameworks. The present study also provides insights into the distinction between personal goals (protecting oneself from infection) and collective goals (reducing the spread of illness). Analyses of demographic variables rarely consider socio‐cognitive mechanisms. In this paper, we test a mediation model where demographic characteristics influence protective behaviours via beliefs. Past behaviour is also taken into account, as the literature has shown that past behaviour is the best predictor of future behaviour (Ajzen, 2011; Ouellette & Wood, 1998). The framework used in this paper is presented in Figure 1.
FIGURE 1.
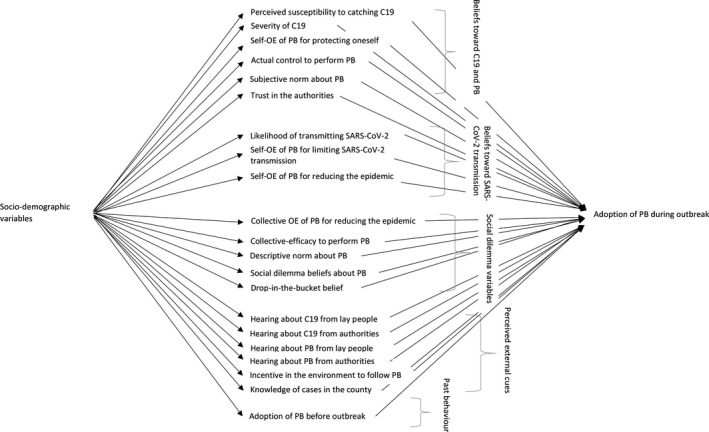
Theoretical framework of the effect of socio‐demographic variables on the adoption of protective behaviours during outbreak, and potential mediators. Abbreviations: PB = protective behaviours. C19 = COVID‐19. OE = outcome expectancy.
In order to shed light on these elements that may contribute to better understanding beliefs and behaviours during an epidemic, and to enhance the public health response in the face of the COVID‐19 outbreak, we conducted an online survey on a nationally representative sample of UK residents. At the time of the survey (20 March), the UK was still at a relatively early stage of the outbreak (the first cases had surged in the country two weeks earlier), and whilst guidelines recommending social distancing had been issued, and further measures had been announced (e.g. closing schools), the British government had not yet implemented the containment seen in other countries (these measures were announced on 23 March) (BFPG, 2020).
METHOD
Participants
In order to ensure participation from a wide range of people and to maximise generalisability, we requested a nationally representative sample of N = 1000 UK residents from our sample provider, Prolific. To ensure representativeness, the sample has been stratified across three demographic variables: age, sex, and ethnicity. More information on representativeness is presented in supporting information (Appendix A). Due to the way in which the platform works, 1,031 participants started the survey. Of those respondents, 25 were excluded in accordance with our analysis plan, resulting in a sample size of N = 1,006 people. Sample size determination is described in the Supporting Information (Appendix B).
Design and Procedure
The research protocol was examined by and received expedited ethical approval from the University’s Ethical Review Board. We registered our questionnaire and our analysis plan on the Open Science Framework (https://osf.io/67bk5/?view_only=1d102f1b47a041ce8c272a4daa8ad786). The present paper reports the first of a three‐wave survey following the evolution of beliefs and behaviour during the epidemic.
Participants were invited to take part in an online survey entitled “Coronavirus Outbreak: Investigating Perception of COVID‐19 and protective behaviours”. Following the consent form, the survey began by examining the extent to which participants follow protective measures. Next, items assessing beliefs were presented in randomised order. Finally, participants answered socio‐demographic questions. At the very end of the survey, an item asked them if they had answered seriously, given the importance of the results in the fight against COVID‐19. It was clearly indicated that their answer to this question would have no impact on their payment. Following this, they were thanked for their participation, and had the opportunity to leave a comment.
Measures
Past and current protective behaviours. Ten behaviours were assessed, adapted from the UK’s National Health Service recommendations at the time. For each behaviour, participants indicated the degree to which they engaged in it on a typical day prior to the COVID‐19 outbreak, and more recently (over the last 10 days). Answers were recorded on a 5‐point Likert response scale ranging from 1 = never to 5 = very often/always. We averaged the items to compute two global scores indicating frequency of adoption of the 10 behaviours: one reflecting behaviour before the outbreak (M = 2.99, SD = 0.63) and the other reflecting behaviour during the outbreak (M = 4.17, SD = 0.56).
Beliefs measures. Items measured beliefs towards COVID‐19 and protective behaviours, beliefs towards SARS‐CoV‐2 transmission, social dilemma variables, and perceived external cues. Two items were used for each construct unless otherwise specified. Beliefs variables were assessed using a 5‐point scale (1 = strongly disagree, 5 = strongly agree). Beliefs measures, examples of items and reliability are presented in the Supporting Information (Appendix C).
Socio‐demographic characteristics. The following variables were measured: age, sex, education level, civil status, number of people living in the household, frequency of social contacts, and geographical area (region/country and county).
Analysis Plan
In order to meet the paper’s goal, we began by analysing the evolution of protective behaviour adoption over time. Associations between beliefs were explored using correlations. Then, the associations between beliefs and socio‐demographic variables were tested to select potential mediators. The association between beliefs and protective behaviour was analysed both through multiple linear regression and using Confidence Interval‐Based Estimation of Relevance (CIBER) (Crutzen & Peters, 2019; Jamovi Project, 2019; R Core Team, 2018). CIBER provides a visual depiction of the distribution of answers, indicating which constructs could be the target of an intervention, or, on the contrary, on which variable people already score very high (e.g. if participants already think that people important to them approve of them following the protective measures, it may not be a priority to communicate on subjective norm). Variables with broad distribution or very low scores suggest that there is room for improvement. The right‐hand column illustrates the association between the belief’s score and behaviour (see Figure 3). A variable with a higher association would be more interesting in a behaviour change perspective, as modifying this belief could lead to significant change in behaviour.
FIGURE 3.
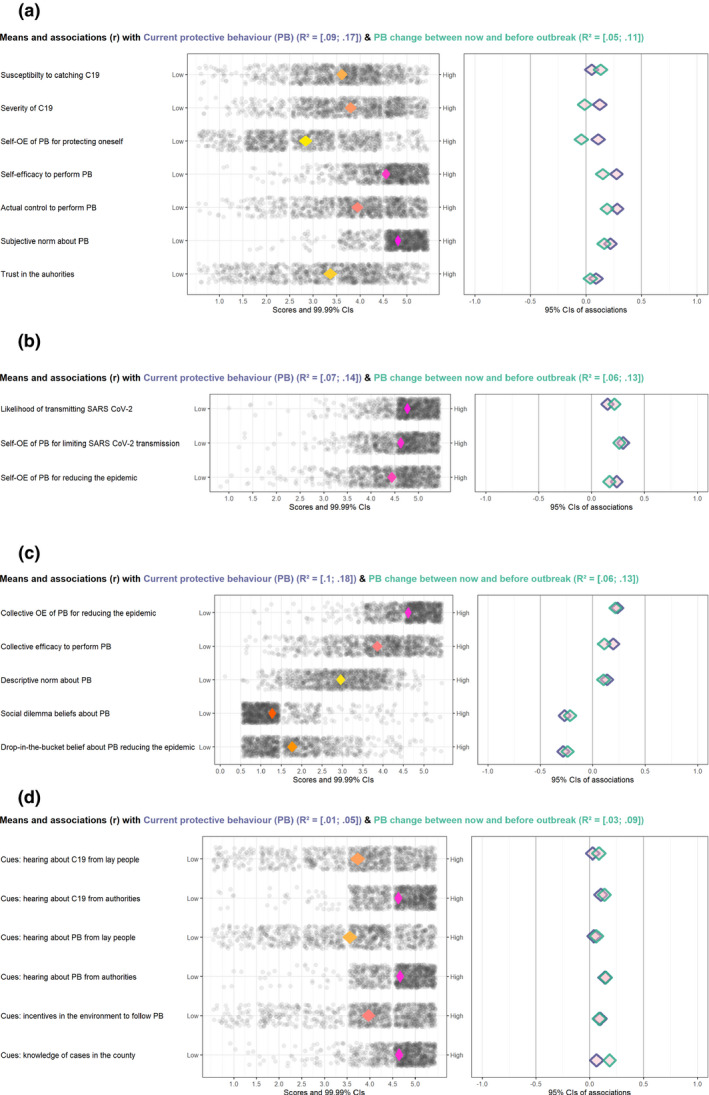
a. CIBER plots of means and associations (r) of beliefs towards COVID‐19 with adoption of. protective behaviours. Legend: In the right‐hand graphs, purple diamonds represent the score of current protective behaviour, and green diamonds represent the score of change between now and before outbreak. Figure 3b. CIBER plots of means and associations (r) of beliefs towards SARS‐CoV‐2 transmission with adoption of protective behaviours. Legend: In the right‐hand graphs, purple diamonds represent the score for current protective behaviour, and green diamonds represent the score of change between now and before outbreak. Figure 3c. CIBER plots of means and associations (r) of social dilemma variables with adoption of protective behaviours. Legend: In the right‐hand graphs, purple diamonds represent the score for current protective behaviour, and green diamonds represent the score of change between now and before outbreak. Figure 3d. CIBER plots of means and associations (r) of perceived external cues with adoption of protective behaviours. Legend: In the right‐hand graphs, purple diamonds represent the score for current protective behaviour, and green diamonds represent the score of change between now and before outbreak. Note: Abbreviations: PB = protective behaviours. C19 = COVID‐19. OE = outcome expectancy.
Finally, mediations were tested for demographic variables showing an association with protective behaviours. Parallel mediations were tested using the PROCESS macro (Hayes, 2018).
In order to control for false discovery caused by multiple comparisons, we adjusted the significance threshold. To do this we used the Benjamini‐Hochberg correction (Benjamini & Hochberg, 1995), which uses a false discovery rate estimation and allows a good compromise between type I and type II errors (Noble, 2009). For a given analysis, p‐values are ordered from the smallest (rank = 1) to the largest. The adjusted p‐value is the p‐value times m/i, where m is the number of the test and i the rank of each test (McDonald, 2009; Noble, 2009).
RESULTS
Descriptive Statistics on Socio‐Demographic Characteristics, Beliefs, and Current Protective Behaviours
Descriptive statistics on the socio‐demographic variables are presented in Table 1, together with mean scores of current protective behaviours for each group. Sex differences were noted, with women having a higher score on current protective behaviours. The association with age did not appear to be linear, like the link with education level, and the number of people living with the respondent. People with fewer social contacts seemed to have higher scores for protective behaviours.
TABLE 1.
Descriptive Statistics of Socio‐Demographic Variables and Average Level of Protective Behaviours [with 99% CI]
| Count | Percentage | Score of current protective behaviours | ||||
|---|---|---|---|---|---|---|
| M | SD | 99% CI [LL, UL] | ||||
| Sex | ||||||
| Men | 489 | 48.7 | 4.07 | 0.60 | [4.00, 4.14] | |
| Women | 515 | 51.3 | 4.26 | 0.49 | [4.20, 4.31] | |
| Age | ||||||
| less than 25 | 115 | 11.4 | 4.09 | 0.57 | [3.95, 4.23] | |
| 25–34 | 177 | 17.6 | 4.20 | 0.53 | [4.10, 4.30] | |
| 35–44 | 184 | 18.3 | 4.20 | 0.56 | [4.09, 4.31] | |
| 45–54 | 167 | 16.6 | 4.09 | 0.61 | [3.97, 4.21] | |
| 55–64 | 258 | 25.6 | 4.21 | 0.53 | [4.12, 4.29] | |
| 65 and more | 107 | 10.6 | 4.16 | 0.55 | [4.01, 4.30] | |
| Educational level | ||||||
| No formal qualifications | 14 | 1.4 | 3.94 | 0.40 | [3.61, 4.26] | |
| Secondary education | 130 | 12.9 | 4.19 | 0.56 | [4.06, 4.32] | |
| High school | 317 | 31.4 | 4.10 | 0.57 | [4.02, 4.19] | |
| Tertiary | 547 | 54.3 | 4.20 | 0.55 | [4.14, 4.26] | |
| Number of people living with the respondent | ||||||
| Zero | 3 | 0.3 | 4.43 | 0.29 | [2.78, 6.09] | |
| One | 172 | 17.1 | 4.10 | 0.60 | [3.98, 4.22] | |
| Two | 367 | 36.4 | 4.20 | 0.54 | [4.13, 4.27] | |
| Three and more | 466 | 46.2 | 4.16 | 0.55 | [4.10, 4.23] | |
| Civil status | ||||||
| Single | 337 | 33.4 | 4.12 | 0.59 | [4.03, 4.20] | |
| In a relationship/ married/ civil partnered | 671 | 66.6 | 4.19 | 0.53 | [4.14, 4.24] | |
| Number of social contacts | ||||||
| None at all | 98 | 9.7 | 4.29 | 0.51 | [4.16, 4.43] | |
| A little | 526 | 52.2 | 4.21 | 0.55 | [4.15, 4.28] | |
| A moderate amount | 213 | 21.1 | 4.05 | 0.60 | [3.95, 4.16] | |
| A lot | 91 | 9.0 | 4.08 | 0.51 | [3.94, 4.22] | |
| A great deal | 80 | 7.9 | 4.10 | 0.54 | [3.94, 4.26] | |
| Country | ||||||
| England | 871 | 86.4 | 4.17 | 0.55 | [4.12, 4.22] | |
| Northern Ireland | 10 | 1.0 | 4.08 | 0.77 | [3.28, 4.87] | |
| Scotland | 85 | 8.4 | 4.17 | 0.58 | [4.01, 4.34] | |
| Wales | 42 | 4.2 | 4.14 | 0.57 | [3.90, 4.38] | |
| Number of cases in the country | ||||||
| Low | 137 | 13.6 | 4.16 | 0.59 | [4.02, 4.29] | |
| High | 871 | 86.4 | 4.17 | 0.55 | [4.12, 4.22] | |
Temporal Evolution of Protective Behaviours
Figure 2 shows the evolution of protective behaviour before the coronavirus crisis and during the last 10 days, for the global score and individual behaviour items. There was a marked increase in nearly all behaviours, ts < −22.68, ps < .001, except for a reduction in participation in social activities, t(994) = 52.56, p < .001, and no significant difference in “use public transportation only if needed”, t(892) = −0.37, p = .714. Adoption frequencies of each protective behaviour are presented in the Supporting Information (Appendix D). The strongest increase in the adoption of protective behaviour was observed for avoiding touching one’s face with unwashed hands: only 14.2 per cent did it often or very often before the crisis, and 65.8 per cent reported doing it often or very often during the crisis. A similar increase was also observed for hand washing after coughing/sneezing/blowing one’s nose (done often or very often by 26.8% of the respondents before, and 73.5% during the crisis), and for handwashing when getting home or into work (performed rarely or sometimes by 46.3% before the crisis, and 88.1% reported doing it always during the crisis). On the contrary, some protective behaviours had higher levels of adoption even before the crisis, notably: washing hands with soap and water for at least 20 s or using hand sanitiser; covering one’s mouth and nose with a tissue or one’s sleeve when coughing/sneezing; and putting used tissues in the bin immediately after coughing/sneezing/blowing one’s nose.
FIGURE 2.
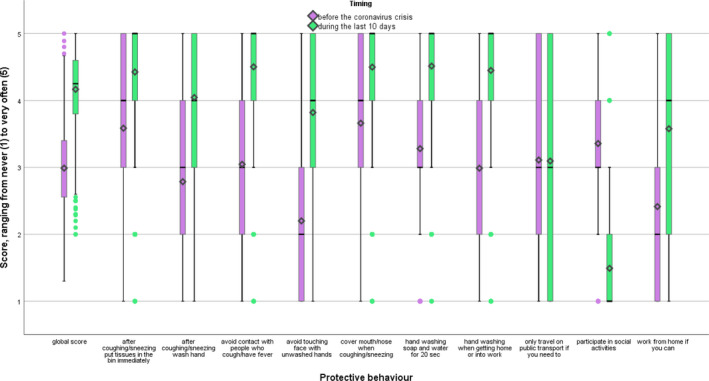
Boxplots of the protective behaviour scores, before the coronavirus crisis (violet) and during the last 10 days (green). Note: Boxplots represent first to third quartiles. Means are represented by a diamond shape, medians by a straight line.
Association between Beliefs
Statistical associations between beliefs were assessed using correlations (Benjamini‐Hochberg correction: significance threshold = .034). Susceptibility and severity had weak associations with other beliefs and were mostly associated with each other (r = .269). A strong association was found between self‐efficacy to perform protective behaviours and actual control (r = .566). Self‐efficacy to perform protective behaviours was also associated with collective‐efficacy to perform protective behaviours (r = .460). Self‐outcome expectancy of protective behaviours for limiting SARS‐CoV‐2 transmission and for reducing the epidemic were strongly correlated (r = .615), and both were also associated with collective outcome expectancy of protective behaviours for reducing the epidemic (r = .623 and .691, respectively). All three variables were also negatively associated with drop‐in‐the‐bucket belief (r = −.487, −.556 and −.458, respectively). Drop‐in‐the‐bucket belief was positively related to social dilemma beliefs (r = .329). Perceived external cues were not strongly associated with the other constructs measured. Hearing about COVID‐19 from lay people was positively associated with hearing about protective behaviours from lay people (r = .775), and hearing about COVID‐19 from authorities was positively associated with hearing about protective behaviours from authorities (r = .698) (for full results table, see the Supporting Information (Appendix E).
Association between Beliefs and Socio‐Demographic Variables
Associations between beliefs and socio‐demographic variables are presented in Table 2 (Benjamini‐Hochberg correction: significance threshold =.008). Sex was associated with variables from the social dilemma framework, with women less likely to have drop‐in‐the‐bucket beliefs, for example. Higher educational level was associated notably with hearing more about COVID‐19 and protective behaviours from lay people. Number of people living with the respondent was associated only with perceived severity of COVID‐19: participants living with more people perceived it as less severe relative to those living with zero or few people. Older age was also associated with a higher perception of severity, more trust in the authorities, and hearing more about COVID‐19 and protective behaviour from authorities, and less from lay people. The number of cases in the country was not significantly associated with any of our measures, while the number of face‐to‐face contacts with other people was notably negatively associated with self‐efficacy of performing protective behaviours, and actual control.
TABLE 2.
Correlations between Socio‐Demographic Variables and Beliefs
| Sex (men = 1, women = 2) | Educational level | Number of people living with the respondent | Age | Number of cases in the country | Number of social contacts | |
|---|---|---|---|---|---|---|
| Beliefs towards C19 and PB | ||||||
| Susceptibility to catching C19 | .010 | .01 | .03 | .05 | .01 | .09* |
| Severity of C19 | .010 | −.06 | −.11* | .29* | .01 | −.11* |
| Self‐OE of PB for protecting oneself | .04 | −.01 | .05 | −.08 | .03 | −.04 |
| Self‐efficacy to perform PB | .09* | −.03 | .01 | .08 | −.01 | −.16* |
| Actual control to perform PB | .05 | .01 | .02 | .04 | −.02 | −.16* |
| Subjective norm about PB | .04 | −.01 | .02 | .08 | −.07 | −.06 |
| Trust in the authorities | −.02 | −.12* | .04 | .14* | .05 | −.07 |
| Beliefs towards SARS‐CoV‐2 transmission | ||||||
| Likelihood of transmitting SARS‐CoV‐2 | .08 | .09* | −.02 | .00 | −.08 | −.01 |
| Self‐OE of PB for limiting SARS‐CoV‐2 transmission | .06 | .08* | .02 | .00 | .03 | −.11* |
| Self‐OE of PB for reducing the epidemic | .06 | .05 | .03 | −.04 | .03 | −.06 |
| Social dilemma variables | ||||||
| Collective OE of PB for reducing the epidemic | .06 | .05 | .03 | −.05 | .00 | −.05 |
| Collective‐efficacy to perform PB | .06 | −.08 | .05 | .06 | −.01 | −.06 |
| Descriptive norm about PB | −.09* | −.05 | .02 | .10* | −.07 | −.08* |
| Social dilemma beliefs about PB | −.11* | −.05 | .07 | −.11* | .04 | .05 |
| Drop‐in‐the‐bucket belief about PB reducing the epidemic | −.12* | −.06 | .00 | −.04 | −.02 | .01 |
| Perceived external cues | ||||||
| Hearing about C19 from lay people | .08 | .10* | .02 | −.09* | .01 | .06 |
| Hearing about C19 from authorities | −.01 | .04 | −.05 | .16* | .03 | −.02 |
| Hearing about PB from lay people | .07 | .11* | .06 | −.14* | .03 | .06 |
| Hearing about PB from authorities | .00 | .04 | −.07 | .17* | −.02 | −.09* |
| Incentive in the environment to follow PB | .00 | .02 | −.02 | .01 | −.01 | .02 |
| Knowledge of cases in the county | .01 | .04 | .01 | −.01 | .00 | .05 |
| Score of protective behaviours before outbreak | .08 | −.07 | −.01 | .04 | .02 | −.03 |
Benjamini‐Hochberg correction was applied and resulted in a significance threshold of .008. Correlations whose p‐value is equal or below this threshold are indicated in bold with an*.
Abbreviations: PB = protective behaviours. C19 = COVID‐19. OE = outcome expectancy. SARS‐CoV‐2 = severe acute respiratory syndrome coronavirus 2.
Association between Beliefs and Protective Behaviour
Confidence Interval‐Based Estimation of Relevance (CIBER) (Crutzen & Peters, 2019; Jamovi Project, 2019; R Core Team, 2018) was used to analyse the association between beliefs and protective behaviour. What can be concluded from the CIBER plot (Figure 3) is that respondents already scored high on a number of variables: beliefs towards SARS‐CoV‐2 transmission, subjective norm, and external cues from authorities. Variables with low association with behaviour (thus not useful to target) were susceptibility, severity, self‐outcome expectancy for protecting oneself from COVID‐19, trust in the authorities, and cues from lay people. Potentially interesting variables (i.e. broad distributions and/or non‐negligible association with behaviour) were: self‐ and collective‐efficacy to perform protective behaviours, action control to perform protective behaviours, and social dilemma and drop‐in‐the‐bucket beliefs.
We also performed a multiple linear regression to estimate the unique relationships between the beliefs measures and the current protective behaviours, as CIBER analysis only provides bivariate estimates. The multicollinearity and homoscedasticity assumptions were verified. No outliers were detected by examining studentised residuals and leverage (Stevens, 1984). The Benjamini‐Hochberg correction for multiple comparison test indicates that only p‐values less than or equal to .003 could be considered significant. The results showed that self‐outcome expectancy of protective behaviours for limiting SARS‐CoV‐2 transmission (b = .13, t(904) = 3.54, p < .001), social dilemma beliefs (b = −.09, t(904) = −3.87, p < .001), and score of protective behaviours before the outbreak (b = .40, t(904) = 16.98, p < .001) were related to current protective behaviours (b = .40, t(904) = 16.98, p < .001) (see the Supporting Information Appendix F for full results table).
Mediation Analysis
We performed single linear regressions to estimate the bivariate relationships between the demographic variables and current protective behaviours. Sex and frequency of social contacts were the only variables significantly associated with current protective behaviours (b = .188, t(1002) = 5.42, p < .001, and b = −.06, t(1006) = −3.71, p < .001, respectively) (beta coefficients reported are unstandardised. For results of other variables, see the Supporting Information Appendix G Table S4). These variables were thus selected for two parallel mediation analyses, with, as mediators, the variables significantly associated with each of them as shown in Table 2. Mediations were run in SPSS, using PROCESS macro (Hayes, 2018). Coefficients are reported in the Supporting Information (Appendix G, Tables S5 and S6). Figure 4 presents two mediation models (one for the mediation of the effect of sex on protective behaviour, and the other for the mediation of the effect of frequency of social contact on protective behaviour), that were tested separately. The effect of sex on protective behaviours might be mediated by self‐efficacy, descriptive norm, social dilemma variables, and drop‐in‐the‐bucket beliefs. The effect of frequency of social contact might be mediated by severity, self‐efficacy, self‐outcome expectancy for limiting SARS‐CoV‐2 transmission, and actual control (for indirect effects, see the Supporting Information Appendix G).
FIGURE 4.
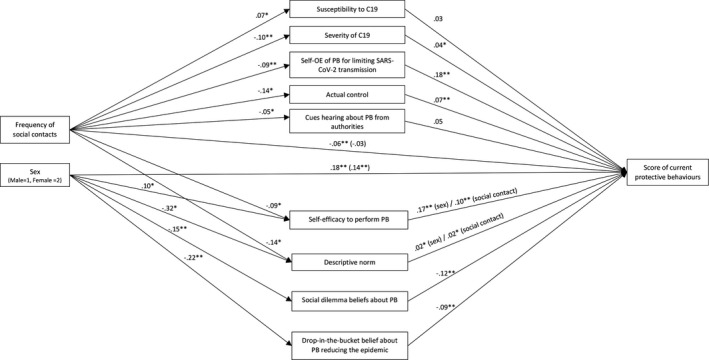
Unstandardised regression coefficients for the relationship between socio‐demographic variables (sex and frequency of social contacts), mediators, and score of current protective behaviours. The regression coefficients between socio‐demographic variables and score of current protective behaviours, controlling for the mediators, are in parentheses. *p < .05, **p < .001. Note: Sex and frequency of contacts are presented on the same figure for simplification, but two separate mediation analyses were run. Abbreviations: PB = protective behaviours. C19 = COVID‐19. OE = outcome expectancy.
DISCUSSION
The present study sought to assess people’s protective behaviour, the extent to which it has changed, socio‐demographic and beliefs correlates, and the relationships between these variables. Data collected on a large nationally representative sample of UK respondents provided insightful information about these factors.
Two weeks after the first cases of COVID‐19 surge in the UK, we can see a marked increase in people following recommended protective behaviour. This is consistent with the UK and US data collected in February–March 2020, showing that most respondents knew that washing hands, avoiding close contact with people who are sick, and avoiding touching one’s eyes, nose and mouth with unwashed hands were effective measures for preventing infection (Geldsetzer, 2020). As has been observed during the HIV epidemic (Anderson et al., 1999), this confirms that, in the face of a serious and probable risk, a large part of the population is able to change quickly and without resistance. However, it is likely that a communication effort directed at a minority of those resistant to change will still be necessary. Apart from sex and number of social contacts, our results show little variability in protective behaviours as a function of socio‐demographic variables. Given the scale of the crisis, it seems that the entire population has changed its habits, even in regions that are still little affected or amongst the least vulnerable populations. The adoption of some protective behaviours increased more than others. This may be attributed to a lower level of practice of certain behaviours before the crisis (e.g. avoiding touching one’s face with unwashed hands) compared to behaviours that were already widely adopted (e.g. covering one’s mouth and nose with a tissue or sleeve when coughing/sneezing). Thus, if prioritisation is needed, communication efforts could be directed at the behaviours that are not already part of people’s habits. Two behaviours had lower levels of adoption than others, and could therefore be targeted in future interventions: working from home, and using public transport only if necessary. However, because of the way the questions were formulated, it is possible that responses to these questions reflect the general extent to which people work from home or take public transport. Future research might confirm whether or not people were reluctant to work from home and reduce their use of public transport even if they could.
In our sample, men were less likely to follow protective measures than women (a similar pattern was found by Armitage et al., 2020), and the mediation analyses suggested possible explanations for this finding. Relative to women, men were: more likely to think that their own individual action would not make a difference in reducing the COVID‐19 epidemic (i.e. drop‐in‐the‐bucket beliefs); tended to agree with social dilemma beliefs to a greater extent; tended to have a lower level of self‐efficacy beliefs. Men tended also to have a higher perception of descriptive norm. These findings build on recent research evidencing sex differences (for instance, Galasso et al., 2020), and provide insights into how these differences may effectively be tackled, by identifying modifiable determinants of behaviour.
The second result of the mediation analysis was that people with prior higher frequency of social contacts engaged in fewer protective behaviours. In our data, possible explanations for this effect were that, relative to people with fewer social contacts, people with more contacts: had a lower perception of severity; were less likely to believe that following the protective measures would decrease their chances of transmitting the coronavirus to other people; had a lower level of actual control; tended to have a lower level of self‐efficacy beliefs. Thus, people with high frequency of social contacts can be encouraged to adopt protective measures by increasing perceived severity, actual control, and their perception that following the protective measures will decrease their chances of transmitting the coronavirus to other people. It is important to note that some confidence intervals testing the indirect effects were close to including zero (e.g. indirect effect of sex on protective behaviours via descriptive norm, and indirect effect of frequency of social contact on protective behaviours via severity). Future research would be necessary to confirm the replicability of those results.
Our findings suggest that the variables featured in the Health Belief Model may not play as strong a role in the adoption of protective behaviours during the COVID‐19 pandemic as other factors. Further research, notably the results of the COVID‐19 Psychological Research Consortium Study (McBride et al., 2020), may shed further light on this matter. Beyond the Health Belief Model predictors, the present research highlights the role played by social dilemma‐related beliefs. While recent work has theorised that the social dilemma perspective has much to contribute to the understanding of behaviour during the present pandemic (see Ling Hoh Teck & Chyong, 2020), to our knowledge, there has not yet been a direct investigation of people’s social dilemma beliefs and how these relate to the adoption of protective behaviours. Our results confirm the importance of taking these variables into consideration in collective situations. In particular, social dilemma beliefs (free‐riding and sucker effect) were predictors of protective behaviours adoption when other predictors were controlled for.
A simple parallel mediation structure (Figure 1) has been chosen to meet the main aim of the paper: allowing the identification of modifiable determinants in case variations in adoption of protective behaviours according to socio‐demographic variables are observed. However, more complex links between beliefs can be anticipated and were seen in the bivariate correlations (Table S2, Supporting Information file). For example, actual control and self‐efficacy could had been hypothesised as being linked, as the latter is sometimes used as a proxy for the former (Ajzen, 2002), and were indeed statistically associated. Self‐outcome expectancy and collective outcome expectancy are part of the same taxonomy (Koletsou & Mancy, 2011), and thus could be more closely related than with other variables. Social dilemma variables could also be expected to be associated with one another, and correlations showed statistically significant association, although of small to moderate sizes.
CIBER analysis highlights several variables with potential to further increase the following of protective measures. Confirming the importance of studying them separately, beliefs about self‐protection, beliefs about the spread of the virus, and social dilemma beliefs all play a role in motivating the adoption of behavioural recommendations. Thus, we would recommend that health communication should go beyond merely informing people about the severity of the virus, and aim to induce a stronger perception of efficacy to perform protective behaviours, both at the individual and collective levels, and strengthen action control. For example, drop‐in‐the‐bucket beliefs can be increased by directing the focus to concrete goals (Moussaoui & Desrichard, 2016), or by combining information on social norms and increasing subjective proximity (Soliman et al., 2018). Collective efficacy and social dilemma beliefs are more difficult to address in real life, notably because techniques such as onymity (Wang et al., 2017) or providing feedback which have been shown to promote cooperation in lab studies can be hard to use in real‐life large‐scale situations (Biel, 2000). Injunctive norms, dividing the objectives into sub‐goals (geographically or temporally), presenting examples of past success, persuading people that others will contribute, and that success is possible are suggestions (Biel, 2000; Klandermans, 1992) that would need empirical validation.
One limitation of the study is that a number of items showed unsatisfactory internal consistency. As pre‐registered, we removed items with low face validity, resulting in single‐item measures. Single‐item measures are problematic because of measurement error; thus future studies should aim for improvement in the measurement of those concepts. Another limitation of the study is its transversal design. Measuring at the same time beliefs and behaviour can be problematic for several reasons, one of them being compromised construct validity. Conway and Lance (2010) gave examples of a priori consideration of common method bias, among which the following had been used in this study: ensuring participants’ anonymity and counterbalancing question order. Another suggestion by the same authors to ensure construct validity is using validated scales; however, this was impossible as the area of research is new (for an exception see Ahorsu et al., 2020). Another flaw of transversal design is preclusion of drawing conclusions regarding causality. This issue has been discussed in particular for mediation analysis (Antonakis et al., 2010). Assumptions for making inferences from mediation include: having established the causal order of variables, ensuring there are no omitted variables in the analysis, and that the variables are measured without error (Shrout, 2011). In our case, causal order of variables can only be questioned in the sense that adoption of protective behaviour could lead to change in beliefs (rather than our supposed model beliefs affecting behaviour), but socio‐demographic variables cannot be anything other than predictors. It is not possible to rule out external variables which could correlate both with socio‐demographic characteristics and the mediators; thus this remains a potential flaw of the study. Error measurement is also a potential issue, notably with single items. Shrout (2011) argues that cross‐sectional correlations could still reveal possible causal mechanisms, for example, when well‐founded theories describe the direction of the process. In the case of the Health Belief Model, according to Jones et al. (2015), “The HBM is one of the most widely utilized and heavily studied theories in public health. … yet variables ordering remains a relatively understudied topic” (p. 13). The authors tested three plausible models (parallel, serial, and moderated mediation), but in all cases beliefs were the mediators of external variables’ effect on behaviour. Because the internal structure of the HBM lacks strong empirical evidence, and considering the methodological design used, we were not in the situation of a clear established causal model, and in this regard our results were discussed cautiously and without implied causality.
Despite those limitations, this study provides a preliminary overview of the adoption of protective behaviours and associated variables at an early stage of the COVID‐19 epidemic. Conclusions are of course tied to the political context, which varies across countries, as well as to the rapidly evolving temporal circumstances.
Future research could leverage other theoretical frameworks, particularly geared towards behaviour change, as for instance Gibson Miller and colleagues have done in their work on hygiene practices using the Capability, Opportunity, Motivation‐Behaviour (COM‐B) model (Gibson Miller et al., 2020). Future studies could also include additional socio‐demographic variables (e.g. sexual orientation; Ko et al., 2020).
Conflict of interest
The authors declare having no conflict of interest related to this work.
Supporting information
Appendix A. Method: Participants representativeness.
Appendix B. Method: Sample size determination.
Appendix C. Method: Beliefs measures.
Appendix D. Results: Temporal evolution of protective behaviours.
Appendix E. Results: Association between beliefs.
Appendix F. Results: Association between beliefs and protective behaviour
Appendix G. Results: Mediation analysis.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are openly available in Open Science Framework at https://osf.io/67bk5/?view_only=1d102f1b47a041ce8c272a4daa8ad786
REFERENCES
- Ahorsu, D.K. , Lin, C.‐Y. , Imani, V. , Saffari, M. , Griffiths, M.D. , & Pakpour, A.H. (2020). The Fear of COVID‐19 Scale: Development and initial validation. International Journal of Mental Health and Addiction, 10.1007/s11469-020-00270-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ajzen, I. (2002). Perceived behavioral control, self‐efficacy, locus of control, and the theory of planned behavior. Journal of Applied Social Psychology, 32(4), 665–683. 10.1111/j.1559-1816.2002.tb00236.x. [DOI] [Google Scholar]
- Ajzen, I. (2011). The theory of planned behaviour: Reactions and reflections. Psychology & Health, 26(9), 1113–1127. 10.1080/08870446.2011.613995. [DOI] [PubMed] [Google Scholar]
- Anderson, J.E. , Wilson, R. , Doll, L. , Jones, T.S. , & Barker, P. (1999). Condom use and HIV risk behaviors among US adults: Data from a national survey. Family Planning Perspectives, 31, 24–28. [PubMed] [Google Scholar]
- Antonakis, J. , Bendahan, S. , Jacquart, P. , & Lalive, R. (2010). On making causal claims: A review and recommendations. Leadership Quarterly, 21(6), 1086–1120. 10.1016/j.leaqua.2010.10.010. [DOI] [Google Scholar]
- Arden, M.A. , & Chilcot, J. (2020). Health psychology and the coronavirus (COVID‐19) global pandemic: A call for research. British Journal of Health Psychology, 25(2), 231–232. 10.1111/bjhp.12414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armitage, C. , Keyworth, C. , Leather, J. , Byrne‐Davis, L. , & Epton, T. (2020). Identifying targets for interventions to support public adherence to government COVID‐19‐related instructions [Preprint]. PsyArXiv. 10.31234/osf.io/8gfvb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Attari, S.Z. , Krantz, D.H. , & Weber, E.U. (2014). Reasons for cooperation and defection in real‐world social dilemmas. Judgement and Decision Making, 9(4), 316–334. [Google Scholar]
- Benjamini, Y. , & Hochberg, Y. (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B (Methodological), 57(1), 289–300. 10.1111/j.2517-6161.1995.tb02031.x. [DOI] [Google Scholar]
- Betsch, C. , Böhm, R. , & Korn, L. (2013). Inviting free‐riders or appealing to prosocial behavior? Game‐theoretical reflections on communicating herd immunity in vaccine advocacy. Health Psychology, 32(9), 978–985. 10.1037/a0031590. [DOI] [PubMed] [Google Scholar]
- BFPG (2020). British Foreign Policy Group. https://bfpg.co.uk/2020/04/covid‐19‐timeline/. [Google Scholar]
- Biel, A. (2000). Factors promoting cooperation in the laboratory, in common pool resource dilemmas, and in large‐scale dilemmas. In Van Vugt M., Snyder M., Tyler, T.R. & Biel A. (Eds.), Cooperation in modern society: Promoting the welfare of communities, states and organizations (pp. 25–41). New York, NY: Routledge. [Google Scholar]
- Bish, A. , & Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. British Journal of Health Psychology, 15(4), 797–824. 10.1348/135910710X485826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bish, A. , & Michie, S. (2011). Demographic and attitudinal determinants of protective behaviours during a pandemic. Departement of Health: UK Pandemic Influenza Preparedness Team. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/215674/dh_125324.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bonniface, L. , & Henley, N. (2008). ‘A drop in the bucket‘: Collective efficacy perceptions and environmental behaviour. Australian Journal of Social Issues, 43(3), 345–358. 10.1002/j.1839-4655.2008.tb00107.x. [DOI] [Google Scholar]
- Cialdini, R.B. , Reno, R.R. , & Kallgren, C.A. (1990). A focus theory of normative conduct: Recycling the concept of norms to reduce littering in public places. Journal of Personality and Social Psychology, 58, 1015–1026. [Google Scholar]
- Conway, J.M. , & Lance, C.E. (2010). What reviewers should expect from authors regarding common method bias in organizational research. Journal of Business and Psychology, 25(3), 325–334. 10.1007/s10869-010-9181-6. [DOI] [Google Scholar]
- Crutzen, R. , & Peters, G.‐J.Y. (2019). The book of behavior change (1st edn.). https://bookofbehaviorchange.com. [Google Scholar]
- Desrichard, O. , Roché, S. , & Bègue, L. (2007). The theory of planned behavior as mediator of the effect of parental supervision: A study of intentions to violate driving rules in a representative sample of adolescents. Journal of Safety Research, 38(4), 447–452. 10.1016/j.jsr.2007.01.012. [DOI] [PubMed] [Google Scholar]
- Faggiano, F. , Allara, E. , Giannotta, F. , Molinar, R. , Sumnall, H. , Wiers, R. , … Conrod, P. (2014). Europe needs a central, transparent, and evidence‐based approval process for behavioural prevention interventions. PLoS Med, 11(10), e1001740. 10.1371/journal.pmed.1001740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galasso, V. , Pons, V. , Profeta, P. , Becher, M. , Brouard, S. , & Foucault, M. (2020). Gender differences in COVID‐19 related attitudes and behavior: Evidence from a panel survey in eight OECD countries (No. w27359; p. w27359). National Bureau of Economic Research. 10.3386/w27359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geldsetzer, P. (2020). Use of rapid online surveys to assess people’s perceptions during infectious disease outbreaks: A cross‐sectional survey on COVID‐19. Journal of Medical Internet Research, 22(4), e18790. 10.2196/18790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson Miller, J. , Hartman, T.K. , Levita, L. , Martinez, A.P. , Mason, L. , McBride, O. , … Bentall, R.P. (2020). Capability, opportunity, and motivation to enact hygienic practices in the early stages of the COVID‐19 outbreak in the United Kingdom. British Journal of Health Psychology, bjhp.12426, 10.1111/bjhp.12426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hallsworth, M. (2020, 4 March). Handwashing can stop a virus: So why don’t we do it? Behavioral Scientist. https://behavioralscientist.org/handwashing‐can‐stop‐a‐virus‐so‐why‐dont‐we‐do‐it‐coronavirus‐covid‐19/. [Google Scholar]
- Hayes, A.F. (2018). Introduction to mediation, moderation, and conditional process analysis: A regression‐based approach (2nd edn.). New York: Guilford Press. [Google Scholar]
- Ibuka, Y. , Li, M. , Vietri, J. , Chapman, G.B. , & Galvani, A.P. (2014). Free‐riding behavior in vaccination decisions: An experimental study. PLoS One, 9(1), e87164. 10.1371/journal.pone.0087164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jamovi Project . (2019). Jamovi (1.0) [Computer software]. https://www.jamovi.org. [Google Scholar]
- Jones, C.L. , Jensen, J.D. , Scherr, C.L. , Brown, N.R. , Christy, K. , & Weaver, J. (2015). The health belief model as an explanatory framework in communication research: Exploring parallel, serial, and moderated mediation. Health Communication, 30(6), 566–576. 10.1080/10410236.2013.873363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerr, N.L. (1983). Motivation losses in small groups: A social dilemma analysis. Journal of Personality and Social Psychology, 45(4), 819–828. [Google Scholar]
- Klandermans, B. (1992). Persuasive communication: Measures to overcome real‐life social dilemmas. In Liebrand W.B.G., Messick D.M., Wilke H.A.M., Liebrand W.B.G., Messick D.M., & Wilke H.A.M. (Eds.), Social dilemmas: Theoretical issues and research findings (1993–98342‐016; pp. 307–318). Elmsford, NY: Pergamon Press; psyh. http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=1993‐98342‐016&site=ehost‐live. [Google Scholar]
- Ko, N.‐Y. , Lu, W.‐H. , Chen, Y.‐L. , Li, D.‐J. , Chang, Y.‐P. , Wang, P.‐W. , & Yen, C.‐F. (2020). Cognitive, affective, and behavioral constructs of COVID‐19 health beliefs: A comparison between sexual minority and heterosexual individuals in Taiwan. International Journal of Environmental Research and Public Health, 17(12), 4282. 10.3390/ijerph17124282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koletsou, A. , & Mancy, R. (2011). Which efficacy constructs for large‐scale social dilemma problems? Individual and collective forms of efficacy and outcome expectancies in the context of climate change mitigation. Risk Management, 13(4), 184–208. 10.1057/rm.2011.12. [DOI] [Google Scholar]
- Ling Hoh Teck, G. , & Chyong, C. (2020). Effects of the coronavirus (COVID‐19) pandemic on social behaviours: From a social dilemma perspective. Technium Social Sciences Journal, 7, 312–320. [Google Scholar]
- Luttrell, A. , & Petty, R. (2020). Evaluations of self‐focused versus other‐focused arguments for social distancing: An extension of moral matching effects [Preprint]. PsyArXiv. 10.31234/osf.io/t5srq. [DOI] [Google Scholar]
- McBride, O. , Murphy, J. , Shevlin, M. , Gibson‐Miller, J. , Hartman, T.K. , Hyland, P. , … Bentall, R.P. (2020). An overview of the context, design and conduct of the first two waves of the COVID‐19 Psychological Research Consortium (C19PRC) Study. PsyArXiv, https://psyarxiv.com/z3q5p/. [Google Scholar]
- McDonald, J.H. (2009). Handbook of biological statistics (Vol. 2), Baltimore, MA: Sparky House Publishing. [Google Scholar]
- Michie, S. , West, R. , Amlôt, R. , & Rubin, G.J. (2020). Slowing down the covid‐19 outbreak: Changing behaviour by understanding it. BMJ Opinion. https://blogs.bmj.com/bmj/2020/03/11/slowing‐down‐the‐covid‐19‐outbreak‐changing‐behaviour‐by‐understanding‐it/. [Google Scholar]
- Moussaoui, L.S. , & Desrichard, O. (2016). Act local but don’t think too global: The impact of ecological goal level on behaviour. Journal of Social Psychology, 156, 536–552. 10.1080/00224545.2015.1135780. [DOI] [PubMed] [Google Scholar]
- Noble, W.S. (2009). How does multiple testing correction work? Nature Biotechnology, 27(12), 1135–1137. 10.1038/nbt1209-1135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Orbell, J. , & Dawes, R. (1981). Social dilemmas. In Stephenson G.M. & Davis J.M. (Eds.), Progress in applied social psychology (Vol. 1, pp. 37–65). New York, NY: John Wiley & Sons. [Google Scholar]
- Ouellette, J.A. , & Wood, W. (1998). Habit and intention in everyday life: The multiple processes by which past behavior predicts future behavior. Psychological Bulletin, 124(1), 54–74. 10.1037/0033-2909.124.1.54. [DOI] [Google Scholar]
- R Core Team (2018). R: A language and environment for statistical computing . [Computer software]. https://cran.r‐project.org/. [Google Scholar]
- Rosenstock, I.M. (1974). The health belief model and preventive health behavior. Health Education Monographs, 2(4), 354–386. 10.1177/109019817400200405. [DOI] [PubMed] [Google Scholar]
- Shrout, P.E. (2011). Commentary: Mediation analysis, causal process, and cross‐sectional data. Multivariate Behavioral Research, 46(5), 852–860. 10.1080/00273171.2011.606718. [DOI] [PubMed] [Google Scholar]
- Soliman, M. , Alisat, S. , Bashir, N.Y. , & Wilson, A.E. (2018). Wrinkles in time and drops in the bucket: Circumventing temporal and social barriers to pro‐environmental behavior. SAGE Open, 8(2), 215824401877482. 10.1177/2158244018774826. [DOI] [Google Scholar]
- Stevens, J.P. (1984). Outliers and influential data points in regression analysis. Psychological Bulletin, 95, 334–344. [Google Scholar]
- Van Lange, P.A.M. , Joireman, J. , Parks, C.D. , & Van Dijk, E. (2013). The psychology of social dilemmas: A review. Organizational Behavior and Human Decision Processes, 120(2), 125–141. 10.1016/j.obhdp.2012.11.003. [DOI] [Google Scholar]
- Wang, Z. , Jusup, M. , Wang, R.‐W. , Shi, L. , Iwasa, Y. , Moreno, Y. , & Kurths, J. (2017). Onymity promotes cooperation in social dilemma experiments. Science Advances, 3(3), e1601444. 10.1126/sciadv.1601444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO (2020). Coronavirus disease (COVID‐19) pandemic. World Health Organization. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019. [Google Scholar]
- Wilson, T.D. , & Juarez, L.P. (2015). Intuition is not evidence: Prescriptions for behavioral interventions from social psychology. Behavioral Science & Policy, 1, 13–20. [Google Scholar]
- Wolf, M.S. , Serper, M. , Opsasnick, L. , O’Conor, R.M. , Curtis, L.M. , Benavente, J.Y. , … Bailey, S.C. (2020). Awareness, attitudes, and actions related to COVID‐19 among adults with chronic conditions at the onset of the US outbreak: A cross‐sectional survey. Annals of Internal Medicine, 173(2), 100–109. 10.7326/M20-1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix A. Method: Participants representativeness.
Appendix B. Method: Sample size determination.
Appendix C. Method: Beliefs measures.
Appendix D. Results: Temporal evolution of protective behaviours.
Appendix E. Results: Association between beliefs.
Appendix F. Results: Association between beliefs and protective behaviour
Appendix G. Results: Mediation analysis.
Data Availability Statement
The data that support the findings of this study are openly available in Open Science Framework at https://osf.io/67bk5/?view_only=1d102f1b47a041ce8c272a4daa8ad786