

Abstract
Objective
To evaluate the clinical efficacy of combining electroacupuncture with auricular point pressing in improving quality of life of individuals with heroin use disorder undergoing methadone maintenance treatment.
Design
A randomized controlled crossover trial.
Subjects
50 participants were recruited from Taipei City Hospital, Linsen Chinese Medicine and Kunming branches, and randomly allocated to treatment groups.
Method
The 36-Item Short Form Health Survey (SF-36) was used. Group A received electroacupuncture at the Hegu (LI4) and Zusanli (ST36) and auricular point pressing on Ear Shenmen, and Group B received only auricular point pressing on Ear Shenmen biweekly for 4 weeks. After a 1-week washout period, crossover of the groups was performed.
Results
The SF-36 mental component scores of the combined treatment group improved relative to the single treatment group (11.09 vs. 10.33, p=0.023). Methadone dosage was reduced in both groups (combined therapy group: 8.58 ± 4.17/7.76 ± 4.11 (baseline/posttreatment) vs. single therapy group: 8.36 ± 4.20/8.30 ± .28, p=0.001).
Conclusion
Combined therapy of high-frequency electroacupuncture with auricular point pressing had better efficacy in enhancing quality of life, especially for mental well-being, and in gradually reducing methadone dosage.
1. Introduction
Heroin use disorder is a prominent public health problem worldwide and a chronic medical illness. This disorder is associated with not only spreading of infectious diseases, such as HIV and hepatitis B and C, but also loss of productivity, disruption of personal relationships, crime, and violence [1]. However, opiate use disorders cause multiple types of damage to the normal functioning of individuals and thus require a multiaspect approach to the treatment process to improve their quality of life [2].
Treatment and prevention of heroin use disorder are a substantial public health concern [3]. Methadone and buprenorphine/naloxone are considered not only first-line treatments for heroin use disorder but also opioid substitution treatments. They can both alleviate opioid withdrawal symptoms and reduce opioid cravings, drug use, and mortality by reducing opioid use and improving quality of life [4, 5].
In 2006, an HIV/AIDS outbreak among people who use heroin intravenously in Taiwan had a considerable nationwide effect regarding heroin use and infectious disease control, and methadone maintenance treatment (MMT) was introduced [6, 7]. However, a multidisciplinary approach toward methadone must consider related clinical scenarios. Constipation, dizziness, drowsiness, headache, sweating, itchy skin, nausea, vomiting, and weakness are potential adverse effects of methadone [8].
Above all else, opiate use disorder is significantly associated with poor quality of life [2]. Individuals undergoing MMT may have poorer physical and psychological health than the general population, with a mental status similar to that of clinically depressed patients [9]. Approaches to improving the quality of life of individuals should include physiology and psychology [10, 11]. Low quality of life can easily lead to nonadherence to MMT [12].
The application of acupuncture has proven significant clinical effects on anxiety and depression, both physiologically and psychologically [13]. Patients undergoing MMT who received acupuncture treatment experienced significant improvement in quality of life, [14, 15] especially with treatment by biweekly application of electroacupuncture at Hegu on the hand, Zusanli on the leg, and Shenmen on the ear. With electroacupuncture as an adjunctive treatment for their withdrawal syndrome, these patients were able to reduce their methadone dosage [16, 17].
Electroacupuncture alleviates opioid withdrawal syndrome by releasing endogenous opioid neurotransmitters to relieve pain, along with exerting psychological effects after receptor binding [18, 19]. Electroacupuncture can stimulate neurotransmitters to bind with receptors, creating a cascade for a series of chemical reactions. However, low-frequency electroacupuncture (2 Hz) differs from high-frequency electroacupuncture (100 Hz) by stimulating the release of β-endorphin, endomorphins, and encephalins, which then interact with µ-opioid receptors and delta-opioid receptors. High-frequency electroacupuncture can accelerate the release of dynorphins, which bind to κ-opioid receptors [19–23].
Auricular point pressing treatment, an alternative to electroacupuncture, is an easily accessible adjunct therapeutic method for treating withdrawal symptoms during opiate detoxification. This treatment is beneficial in MMT for managing disorders related to drug use and follows theories and principles of Traditional Chinese Medicine (TCM) [24–27].
Reduction in quality of life related to poor physical and psychological health is closely associated with sleep quality in individuals who are dependent on heroin [28, 29].
In the treatment of individuals with opiate use disorders, improved quality of life is among the efficacies associated with both acupuncture and auricular point pressing. However, the efficacy of a combination treatment of electroacupuncture and auricular point pressing is unknown. Hence, the aim of this study was to evaluate the clinical efficacy of combined electroacupuncture and auricular point pressing in improving the quality of life of individuals with heroin use disorder undergoing MMT.
2. Materials and Methods
2.1. Study Participants
The study was conducted from June 23, 2017, to December 28, 2018. We invited 72 individuals in clinics of the Linsen Chinese Medicine and Kunming branches of Taipei City Hospital (Taipei, Taiwan), which offers standard methadone therapy, to participate.
Inclusion criteria were as follows: (1) the participant was between 20 and 65 years of age and (2) received a diagnosis of heroin disorder based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Exclusion criteria involved the following: (1) pregnancy, (2) refusal to receive electroacupuncture or auricular point pressing treatment, (3) appearance of major physical or mental disorders, and (4) apparently irregular or fluctuating dosage of methadone or apparent morphine withdrawal syndrome. During their first clinic visit, participants were interviewed by a research assistant and signed informed consent forms approved by the Research Ethics Committee of Taipei City Hospital (IRB number: TCHIRB-10601106). Baseline assessments were conducted in Taipei City Hospital, Linsen Chinese Medicine and Kunming branches, clinics. The trial was registered with ClinicalTrials.gov (Identifier: NCT03881618).
2.2. Randomization
After completion of the baseline assessment, all eligible participants received a sealed envelope containing a computer-generated random number collected by the author who did not have direct contact with participants. Allocation was concealed until completion of all baseline assessments. Participants were randomly allocated to one of the two groups in a 1 : 1 ratio (Group A, n = 25 and Group B, n = 25) and started receiving treatment according to their assignment.
2.3. Interventions
Acupuncture points for the electroacupuncture intervention were selected on the basis of studies examining the efficacy of acupuncture for the treatment of opioid addiction [13, 16, 17, 30–33]. Hegu and Zusanli were chosen as two acupoints. They consisted of four bilateral acupuncture points on the hands and legs, and electroacupuncture was administered using an electroacupuncture machine (Model D0310K, Ching Ming Medical Device Co. Ltd., Taiwan) delivering a frequency of 100 Hz (dense and disperse, DD). Electroacupuncture was dispersed at automatic 2-second intervals for 20 minutes to lead to “DeQi” (revealed as numbness, soreness, and heaviness), with increasing 1 mA increments of intensity to the maximum tolerable intensity as reported by the participant. In addition, bilateral Shenmen auricular acupoints were fixed with cowherb seed by a breathable tape and stimulated by manual pressing every five minutes for a total of 20 minutes, in accordance with relevant research [24–26]. All TCM interventions and care were provided in quiet, private clinics of the Linsen Chinese Medicine and Kunming branches of Taipei City Hospital, Taipei, Taiwan, by the same attending clinician with 10 years of acupuncture experience, and all interventions were performed in the evening (between 5:00 and 8:00 pm). The needles and cowherb seeds were removed immediately afterward by the same clinician after intervention.
2.4. Study Process
After the exclusion of ineligible individuals, 50 (69%) patients aged between 20 and 65 years were included in the parallel intervention. Group A received combined therapy (electroacupuncture at the Hegu (LI4) and Zusanli (ST36) and auricular point press on Ear Shenmen), whereas Group B received a single therapy (auricular point press on Ear Shenmen). The intervention was performed biweekly for 4 weeks (Stage I treatment, days 1–28). After a 1-week washout period (days 29–35), a crossover of the groups was performed (Stage II treatment, days 36–64). During both treatments, all participants received treatment biweekly for 4 weeks continually and without interruption.
2.5. Outcome Measurement
Outcome measurements of the treatments on days 1, 28, 36, and 64 were made using the Taiwanese version of the 36-Item Short Form Health Survey (SF-36) to evaluate quality of life at the completion of treatment courses. The Taiwanese version of the instrument demonstrated validity similar to that of other language versions [34]. To evaluate quality of life, eight domains are assessed: physical functioning (PF), role limitations due to physical problems (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and general mental health (MH) [35]. Five of the scales (PF, RP, BP, SF, and RE) describe limitations or disability, with the remaining three (GH, VT, and MH) denoting a state of welfare where midrange scores indicate no limitations or disabilities. For this study, items in each domain were aggregated and transformed into a scale from 0 to 100, with higher scores indicating better health status [34–36]. Moreover, two distinct concepts are measured by the SF-36: a physical dimension, represented by a physical component summary (PCS) containing PF, RP, BP, and GH scores, and a mental dimension, represented by a mental component summary (MCS) [37] containing VT, SF, RE, and MH scores.
In methadone maintenance treatment, opioid withdrawal syndrome may be observed among patients with irregular adherence, causing poor quality of life. Therefore, a gradual and smooth methadone dosage tapering without heroin relapse is inevitably a vivid goal for individuals with heroin use disorder.
2.6. Sample Size
Sample size was calculated using the following input parameters: two tails, an error probability = 0.05, and power (1 − b error probability) = 0.8. The required size was calculated to be 35. With a 20% dropout rate, approximately 44 participants were required.
2.7. Statistical Analysis
Statistical analysis was performed by another researcher who was unaware of treatment allocation. Demographic and other data for age, sex, occupation, marital status, and history of methadone use, hepatitis B, hepatitis C, HIV, and syphilis were collected and analyzed using SPSS (version 22.0). The demographic characteristics were first analyzed using descriptive statistics, including the mean, standard deviation, and percentage. Inferential statistics, including the independent t-test, were used to verify homogeneity and the effect of electroacupuncture among groups. The paired t-test was used to evaluate within-group differences. Statistical significance was set at a p value of 0.05, two-tailed.
3. Results
Figure 1 presents the study flowchart. Among 72 eligible participants, 22 were excluded as they did not wish to try acupuncture. In total, 50 participants were enrolled, of whom 37 completed both stages of the study. During the study period, five participants (20%) in Group A dropped out. Four were afraid of needle treatment in Stage I and one participant was unwilling to accept Stage II treatment. Eight participants in Group B (32%) dropped out (three because they were unwilling to complete the questionnaire at Stage I and five because they were afraid of needle treatment at Stage II). Demographic data revealed no significant differences between these groups (Table 1).
Figure 1.
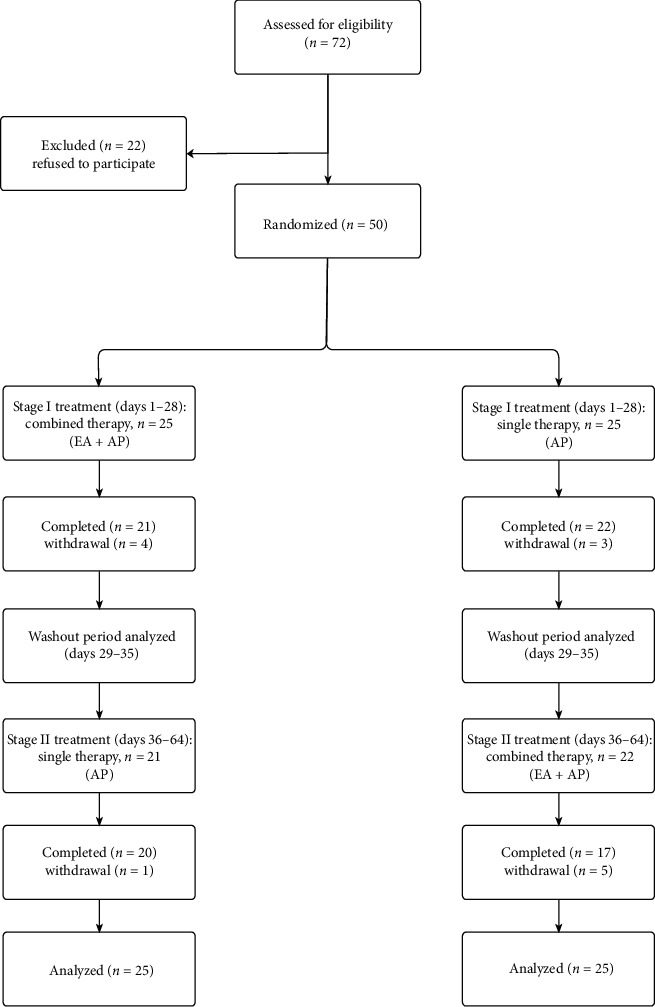
Participant flowchart.
Table 1.
Demographic and clinical characteristics of participants.
| Variable definition | Group A (n = 25) | Group B (n = 25) | Total (n = 50) | p value |
|---|---|---|---|---|
| Age (years) | 46.20 ± 8.09 | 45.47 ± 7.85 | 45.99 ± 7.83 | 0.783 |
| Sex | 0.508 | |||
| Male | 18 (72.0) | 16 (64.0) 9 (36.0) | 34 (68.0) | |
| Female | 7 (28.0) | 16 (32.0) | ||
| Occupation | 0.970 | |||
| Employed | 18 (72.0) | 17 (68.0) | 35 (70.0) | |
| Unemployed | 7 (28.0) | 8 (32.0) | 15 (30.0) | |
| History of methadone use (years) | 6.70 ± 3.21 | 7.18 ± 3.09 | 6.94 ± 3.12 | 0.650 |
| Hepatitis B | 0.860 | |||
| Positive | 5 (20.0) | 4 (16.0) | 9 (18.0) | |
| Negative | 20 (80.0) | 21 (84.0) | 41 (82.0) | |
| Hepatitis C | 0.868 | |||
| Positive | 23 (92.0) | 22 (88.0) | 45 (90.0) | |
| Negative | 2 (8.0) | 3 (12.0) | 5 (10.0) | |
| HIV | 0.228 | |||
| Positive | 2 (8.0) | 5 (20.0) | 7 (14.0) | |
| Negative | 23 (92.0) | 20 (80.0) | 43 (86.0) | |
| Syphilis | 0.284 | |||
| Positive | 0 (0.0) | 2 (8.0) | 2 (4.0) | |
| Negative | 25 (100.0) | 23 (92.0) | 48 (96.0) | |
| Marital status | 0.463 | |||
| Never married | 9 (36.0) | 9 (36.0) | 18 (36.0) | |
| Married/cohabiting | 9 (36.0) | 15 (60.0) | 24 (48.0) | |
| Divorced/widowed | 7 (28.0) | 1 (4.0) | 8 (16.0) |
3.1. Treatment Outcome on Quality of Life
Sizeable treatment outcomes were noted in Group A (n = 25)/Stage I and Group B (n = 25)/Stage II. A significant improvement through combined therapy was observed in the RP (Group B/Stage I and Group B/Stage II), BP (Group A/Stage I and Group B/Stage I), VT (Group A/Stage I and Group B/Stage I), RE (Group B/Stage II), and MH (Group B/Stage II) subscales (Table 2).
Table 2.
SF-36 results at Stage I and Stage II.
| Measurements | Stage | Days | Group A mean (SD) |
Group B mean (SD) |
p value |
|---|---|---|---|---|---|
| SF-36 | |||||
| Physical functioning (PF) | I | 0 | 29.15 (2.36) | 28.29 (2.97) | |
| I | 28 | 29.25 (2.35) | 28.58 (2.95) | 0.610 | |
| p value for paired t-test | 0.163 | 0.236 | |||
| II | 36 | 29.15 (2.34) | 28.52 (2.60) | ||
| II | 64 | 29.20 (2.30) | 28.35 (2.59) | 0.433 | |
| p value for paired t-test | 0.330 | 0.332 | |||
| Role limitation due to physical problems (RP) | I | 0 | 7.30 (1.34) | 7.00 (1.65) | |
| I | 28 | 7.75 (0.71) | 7.76 (0.97) | 0.854 | |
| p value for paired t-test | 0.095 | 0.049∗ | |||
| II | 36 | 7.50 (1.14) | 6.58 (1.58) | ||
| II | 64 | 7.65 (0.93) | 7.52 (0.94) | 0.826 | |
| p value for paired t-test | 0.186 | 0.013∗ | |||
| Bodily pain (BP) | I | 0 | 9.45 (1.98) | 8.58 (2.29) | |
| I | 28 | 10.10 (1.29) | 9.58 (1.46) | 0.496 | |
| p value for paired t-test | 0.015∗ | 0.036∗ | |||
| II | 36 | 9.40 (1.69) | 8.52 (1.66) | ||
| II | 64 | 9.35 (1.66) | 8.88 (1.69) | 0.574 | |
| p value for paired t-test | 0.863 | 0.138 | |||
| General health (GH) | I | 0 | 15.70 (0.97) | 15.05 (0.82) | |
| I | 28 | 16.10 (0.71) | 15.55 (0.62) | 0.511 | |
| p value for paired t-test | 0.189 | 0.120 | |||
| II | 36 | 15.75 (0.71) | 15.52 (1.00) | ||
| II | 64 | 15.55 (0.94) | 15.52 (0.71) | 1.000 | |
| p value for paired t-test | 0.479 | 1.000 | |||
| Vitality (VT) | I | 0 | 12.60 (1.95) | 11.52 (2.57) | |
| I | 28 | 14.25 (1.86) | 12.88 (2.11) | 0.018∗ | |
| p value for paired t-test | 0.002∗ | 0.030∗ | |||
| II | 36 | 12.00 (2.07) | 11.29 (1.61) | ||
| II | 64 | 12.25 (1.99) | 12.17 (2.35) | 0.586 | |
| p value for paired t-test | 0.096 | 0.060 | |||
| Social function (SF) | I | 0 | 6.95 (1.39) | 6.64 (1.45) | |
| I | 28 | 7.25 (1.61) | 6.88 (1.49) | 0.459 | |
| p value for paired t-test | 0.527 | 0.637 | |||
| II | 36 | 7.00 (1.25) | 7.00 (1.45) | ||
| II | 64 | 7.20 (1.39) | 7.05 (1.43) | 0.569 | |
| p value for paired t-test | 0.494 | 0.896 | |||
| Role limitation due to emotional problems (RE) | I | 0 | 4.60 (1.09) | 4.41 (1.00) | |
| I | 28 | 5.00 (0.72) | 4.64 (0.93) | 0.231 | |
| p value for paired t-test | 0.202 | 0.482 | |||
| II | 36 | 4.65 (0.48) | 4.29 (0.58) | ||
| II | 64 | 4.70 (0.65) | 4.94 (0.55) | 0.455 | |
| p value for paired t-test | 0.772 | 0.002∗∗ | |||
| Mental health (MH) | I | 0 | 20.50 (1.82) | 17.23 (1.56) | |
| I | 28 | 19.95 (1.27) | 17.58 (1.46) | <0.001∗∗∗ | |
| p value for paired t-test | 0.290 | 0.269 | |||
| II | 36 | 17.70 (2.07) | 20.17 (1.70) | ||
| II | 64 | 17.85 (2.10) | 18.94 (1.29) | 0.256 | |
| p value for paired t-test | 0.697 | 0.012∗ |
Note. SF-36 = 36-Item Short Form Health Survey; ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
We divided data for treatment groups for comparison (Table 3). Significant differences in vitality (VT: p = 0.012) and mental health (MH: p < 0.001) subscales were observed.
Table 3.
SF-36 results at baseline and posttreatment (electroacupuncture plus auricular point pressing vs. auricular point pressing alone).
| Electroacupuncture + auricular point pressing | Auricular point pressing | p value | |||
|---|---|---|---|---|---|
| Mean (SD) | Paired t-test p value | Mean (SD) | Paired t-test p value | ||
| Physical functioning (PF) | |||||
| Baseline | 28.86 (2.46) | 0.768 | 28.75 (2.65) | 0.160 | 0.975 |
| Posttreatment | 28.83 (2.47) | 28.91 (2.60) | |||
| Role limitations of physical problems (RP) | |||||
| Baseline | 6.97 (1.48) | 0.003∗∗ | 7.27 (1.40) | 0.021∗ | 0.358 |
| Posttreatment | 7.64 (0.82) | 7.70 (0.93) | |||
| Bodily pain (BP) | |||||
| Baseline | 9.02 (1.87) | 0.004∗∗ | 9.02 (2.00) | 0.111 | 0.893 |
| Posttreatment | 9.54 (1.59) | 9.45 (1.55) | |||
| General health (GH) | |||||
| Baseline | 15.48 (1.04) | 0.026∗∗ | 15.37 (1.08) | 0.044∗ | 0.846 |
| Posttreatment | 16.08 (1.21) | 15.91 (1.11) | |||
| Vitality (VT) | |||||
| Baseline | 12.00 (1.90) | <0.001∗∗∗ | 11.78 (2.29) | 0.011∗∗ | 0.012∗∗ |
| Posttreatment | 13.29 (2.31) | 12.54 (2.04) | |||
| Social function (SF) | |||||
| Baseline | 6.97 (1.40) | 0.557 | 6.83 (1.34) | 0.427 | 0.611 |
| Posttreatment | 7.16 (1.51) | 7.05 (1.43) | |||
| Role limitations due to emotional problems (RE) | |||||
| Baseline | 4.45 (0.90) | 0.007∗∗ | 4.54 (0.76) | 0.442 | 0.437 |
| Posttreatment | 4.97 (0.64) | 4.67 (0.78) | |||
| Mental health (MH) | |||||
| Baseline | 20.35 (1.75) | 0.015∗ | 17.48 (1.85) | 0.330 | <0.001∗∗∗ |
| Posttreatment | 19.48 (1.36) | 17.72 (1.82) | |||
Note. ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Data collected using the SF-36 were also analyzed by the physical component score (PCS) and mental component score (MCS) for evaluation. We uncovered a significantly higher percentage of improvement in the MCS score of the combined treatment group vs. the single treatment group (11.09 vs. 10.33, p = .023; Figure 2).
Figure 2.
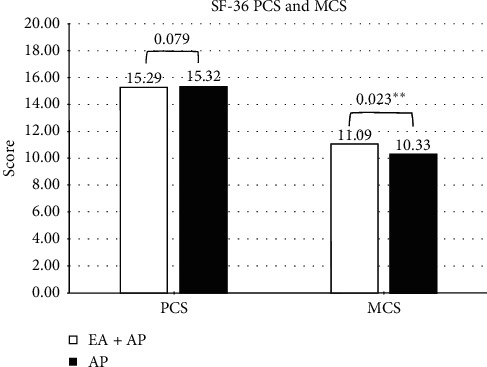
Physicalcomponentscore (PCS) and mental component score (MCS) of combined therapy group and single therapy group. Note: ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
3.2. Methadone Dosage of Participants
We closely monitored methadone dosage among participants (Table 4). Dosage significantly decreased in both the combined (baseline vs. posttreatment: 8.32 ± 4.11 vs. 7.56 ± 3.91, p = 0.002) and single (8.27 ± 3.97 vs. 7.97 ± 4.15, p = .027) treatment groups.
Table 4.
Methadone dosage at baseline and posttreatment (electroacupuncture plus auricular point pressing vs. acupressure point pressing alone).
| Electroacupuncture + auricular point pressing | Auricular point pressing | |||||
|---|---|---|---|---|---|---|
| Mean (SD) | Paired t-test p value | Mean (SD) | Paired t-test p value | p value | ||
| Dosage | ||||||
| Baseline (mg/day) | 8.32 (4.11) | 0.002∗∗ | 8.27 (3.97) | 0.027∗ | 0.001∗∗∗ | |
| Posttreatment (mg/day) | 7.56 (3.91) | 7.97 (4.15) | ||||
|
| ||||||
| Mean (SD) | Mean (SD) | p value | Mean difference (95% CI) | |||
|
| ||||||
| Posttreatment-baseline (mg/day) | −0.75 (4.01) | −0.30 (4.06) | 0.043∗∗ | −0.83, −0.27 | ||
Note. ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
3.3. Adverse Reactions
One participant presented with mild bleeding at the acupuncture point after Group B Stage II treatments. Another participant reported a feeling of dizziness after Group A Stage I treatments. Immediate supportive medical treatments were provided and followed to conclusion.
4. Discussion
Individuals with heroin use disorder may experience heroin relapse. Therefore, relapse prevention approaches that improve the physical and mental health and well-being of individuals with heroin use disorder are vital during recovery. A low quality of life during MMT may be a latent risk factor for relapse [3]. Furthermore, the larger the amount of opiate used during MMT, the more severe the withdrawal syndrome symptoms are—especially its psychological symptoms [9]. A goal of improvement in client quality of life is decreased methadone dosage. When dosage is reduced gradually, withdrawal is less severe, creating a virtuous cycle with improved quality of life [3].
Our results indicate that combined therapy resulted in a larger decline in dosages (Table 4), which would also indirectly reduce the incidence of withdrawal syndrome through improving quality of life [38]. This improvement was more evident in MCS scores (combined therapy: 11.09 vs. single therapy: 10.33, p = 0.023) than in PCS scores (combined therapy: 15.29 vs. single therapy: 15.32, p = 0.079; Figure 2). The largest effects were observed in VT (combined therapy baseline : posttreatment (12.00 ± 1.90 : 13.29 ± 2.31) vs. single therapy baseline : posttreatment (11.78 ± 2.29 : 12.54 ± 2.04), p = .012) and RE (combined therapy: 4.45 ± 0.90 vs. single therapy: 4.97 ± 0.64, p = 0.007) subscales.
The mechanism of electroacupuncture has been revealed to be associated with opioid receptors (kappa, delta, and mu) in brain regions known to interact with endogenous opioids and that are believed to play an essential role in life quality [39, 40]. Exogenous opioids, such as morphine, bind to the same sites as endogenous opioids, suppressing the production of endogenous opioids. Withdrawal syndrome may appear when morphine exposure is suddenly stopped [41, 42]. Acupuncture can compensate for the lack of a chemical cascade from neurotransmitters.
Auricular point pressing and electroacupuncture treatment follow theories and principles of TCM to improve Chi circulation [43]. Auricular point pressing was included in the design of both interventions because it is convenient and accessible at home by clients themselves, whereas invasive treatment must be executed at a clinic.
A partially single adjunct therapeutic method to treat withdrawal symptoms during opiate detoxification has been beneficial in MMT in managing related disorders [23–26]. A daily practice of appropriate auricular point pressing may also strengthen efficacy for improving RP (single therapy, baseline: 7.27 ± 1.40 vs. posttreatment: 7.70 ± 0.93, p = 0.021), GH (single therapy, baseline: 15.37 ± 1.08 vs. posttreatment: 15.91 ± 1.11, p = 0.044), and VT (single therapy, baseline: 11.78 ± 2.29 vs. posttreatment: 12.54 ± 2.04, p = 0.011; Table 3) subscales. Adding electroacupuncture also added efficacy according to MCS results (combined therapy: 11.09 vs. single therapy: 10.33, p = 0.023). Maintaining mental health is the most difficult challenging aspect of MMT for individuals with heroin disorder [9].
Little research has been conducted to study the clinical effect of high-frequency electroacupuncture. All that is known is that 100 Hz was more effective than 2 Hz in an animal study, owing to the promotion of endogenous opioids, such as dynorphin, which binds to kappa opioid receptors to ameliorate withdrawal syndrome. We demonstrated that high-frequency electroacupuncture reduced withdrawal syndrome among clients undergoing MMT as measured by SF-36, especially its mental domains. Furthermore, it may result in declining methadone dosage (Table 4).
Because auricular point pressing is a noninvasive, evidence-based, access-friendly TCM treatment, the related treatment program should be addressed by addiction specialists. TCM treatments are widely accepted in Taiwanese and Chinese culture, whether electroacupuncture or auricular point pressing. Auricular point pressing in a TCM clinic with adequate supervision by trained TCM clinicians improves quality of life, and combining it with high-frequency electroacupuncture further improves outcomes. Finally, for ethical reasons, we did not include a sham treatment [24–26] for participants.
The clinical impact of the study is in its demonstration that TCM treatments, especially electroacupuncture with auricular point pressing, can be introduced as a routine facilitating treatment for patients undergoing MMT.
4.1. Limitations
This study has several limitations. First, it included a small number of participants. However, through a randomized crossover controlled design, we could gather data with sufficient statistical power. Second, this was an open-label study and thus lacked blinding. Third, the washout period was short, largely because participants undergoing MMT belonged to a particular ethnic group, making tracing and evaluation with a longer washout period too risky.
5. Conclusion
A combined therapy of electroacupuncture and auricular point pressing is more effective than only auricular point pressing in improving the quality of life of individuals with heroin use disorder undergoing MMT. TCM treatments, particularly electroacupuncture with auricular point pressing, can be introduced as a routine adjunctive treatment.
Acknowledgments
We honor Dr. Yuh-Hsiang Yeh, a previous team member, who left us quietly and peacefully in August 2019. He was an excellent researcher, a caring doctor, and a warm colleague. May he rest in peace. This study was funded by the Taipei City Government, Department of Health (H9B8A1), and the “Yin Yen-Liang Foundation Development and Construction Plan” of the School of Medicine, National Yang-Ming University (107F-M01).
Abbreviations
- MMT:
Methadone maintenance treatment
- TCM:
Traditional Chinese Medicine
- MCS:
Mental component summary of the SF-36
- PCS:
Physical component summary of the SF-36
- PF:
Physical functioning
- RP:
Role limitation due to physical problems
- BP:
Bodily pain
- GH:
General health
- VT:
Vitality
- SF:
Social function
- RE:
Role limitation due to emotional problems
- MH:
Mental health.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
Data collection was approved by the Institutional Review Board of Taipei City Hospital (IRB number: TCHIRB-10601106; ClinicalTrials.gov Identifier: NCT03881618).
Disclosure
The funding sources had no role in any process of the study.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors' Contributions
Kai-Chiang Yu and Han-Ting Wei analyzed and interpreted patient data. Shang-Chih Chang collected patient data and designed the study. Prof. Chung-Hua Hsu led the TCM treatment team and constructed treatment protocols. All authors read and approved the manuscript.
References
- 1.Zhu J. W., Liu F. L., Mu D., Deng D. Y., Zheng Y. T. Heroin use is associated with lower levels of restriction factors and type I interferon expression and facilitates HIV-1 replication. Microbes Infect. 2017;19(4-5):288–294. doi: 10.1016/j.micinf.2017.01.002. [DOI] [PubMed] [Google Scholar]
- 2.Petrov S. V., Orbetzova M. M., Iliev Y. T., Boyadzhiev D. T. Chronic treatment with opiate agonists in Bulgaria - assessing the quality of life using SF 36 v. 2. Folia Medica. 2016;58(2):115–121. doi: 10.1515/folmed-2016-0019. [DOI] [PubMed] [Google Scholar]
- 3.Yu K. C., Hsu C. H. Research for the role of Chinese medicine in heroin detoxification. Journal of Traditional Chinese Internal Medicine. 2017;15(1):28–39. [Google Scholar]
- 4.Hser Y. I., Evans E., Huang D., et al. Long–term outcomes after randomization to buprenorphine/naloxone versus methadone in a multi–site trial. Addiction. 2016;111(4):695–705. doi: 10.1111/add.13238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pihkala H., Sandlund M. Parenthood and opioid dependence. Substance Abuse and Rehabilitation. 2015;6:33–40. doi: 10.2147/sar.s75796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tang Y.-l., Zhao D., Zhao C., Cubells J. F. Opiate addiction in China: current situation and treatments. Addiction. 2006;101(5):657–665. doi: 10.1111/j.1360-0443.2006.01367.x. [DOI] [PubMed] [Google Scholar]
- 7.Lyu S.-Y., Su L.-W., Chen Y.-M. A. Effects of education on harm-reduction programmes. The Lancet. 2012;379(9814):e28–30. doi: 10.1016/s0140-6736(11)60786-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Deering D., Frampton C., Horn J., Sellman D., Adamson S., Potiki T. Health status of clients receiving methadone maintenance treatment using the SF-36 health survey questionnaire. Drug and Alcohol Review. 2004;23(3):273–280. doi: 10.1080/09595230412331289428. [DOI] [PubMed] [Google Scholar]
- 9.Ryan C. F., White J. M. Health status at entry to methadone maintenance treatment using the SF-36 health survey questionnaire. Addiction. 1996;91(1):39–45. doi: 10.1046/j.1360-0443.1996.911397.x. [DOI] [PubMed] [Google Scholar]
- 10.Rounsaville B. J., Weissman M. M., Kleber H., Wilber C. Heterogeneity of psychiatric diagnosis in treated opiate addicts. Archives of General Psychiatry. 1982;39(2):161–168. doi: 10.1001/archpsyc.1982.04290020027006. [DOI] [PubMed] [Google Scholar]
- 11.Darke S., Swift W., Hall W. Prevalence, severity and correlates of psychological morbidity among methadone maintenance clients. Addiction. 1994;89(2):211–217. doi: 10.1111/j.1360-0443.1994.tb00880.x. [DOI] [PubMed] [Google Scholar]
- 12.Kurth M. E., Sharkey K. M., Millman R. P., Corso R. P., Stein M. D. Insomnia among methadone-maintained individuals: the feasibility of collecting home polysomnographic recordings. Journal of Addictive Diseases. 2009;28(3):219–225. doi: 10.1080/10550880903014155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Boyuan Z., Yang C., Ke C., Xueyong S., Sheng L. Efficacy of acupuncture for psychological symptoms associated with opioid addiction: a systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine. 2014;2014:13. doi: 10.1155/2014/313549.313549 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Norliza C., Norni A., Anandjit S., Mohd Fazli M. I. A review of substance abuse research in Malaysia. Medical Journal of Malaysia. 2014;69:55–58. [PubMed] [Google Scholar]
- 15.Wu S. L., Leung A. W., Yew D. T. Acupuncture for detoxification in treatment of opioid addiction. East Asian Archives of Psychiatry: Official Journal of the Hong Kong College of Psychiatrists = Dong Ya Jing Shen Ke Xue Zhi: Xianggang Jing Shen Ke Yi Xue Yuan Qi Kan. 2016;26(2):70–76. [PubMed] [Google Scholar]
- 16.Chen Z., Wang Y., Wang R., Xie J., Ren Y. Efficacy of acupuncture for treating opioid use disorder in adults: a systematic review and meta-analysis. Evidence-Based Complementary and Alternative Medicine. 2018;2018:15. doi: 10.1155/2018/3724708.3724708 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lin J. G., Chan Y. Y., Chen Y. H. Acupuncture for the treatment of opiate addiction. Evidence-Based Complementary and Alternative Medicine. 2012;2012:10. doi: 10.1155/2012/739045.739045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Chan Y.-Y., Lo W.-Y., Li T.-C., et al. Clinical efficacy of acupuncture as an adjunct to methadone treatment services for heroin addicts: a randomized controlled trial. The American Journal of Chinese Medicine. 2014;42(3):569–586. doi: 10.1142/s0192415x14500372. [DOI] [PubMed] [Google Scholar]
- 19.Han J. S. Acupuncture and endorphins. Neuroscience Letters. 2004;361(1-3):258–261. doi: 10.1016/j.neulet.2003.12.019. [DOI] [PubMed] [Google Scholar]
- 20.Han J. S., Ding X. Z., Fan S. G. Frequency as the cardinal determinant for electroacupuncture analgesia to be reversed by opioid antagonists. Sheng Li Xue Bao. 1986;38(5):475–482. [PubMed] [Google Scholar]
- 21.Han J. S., Chen X. H., Sun S. L., et al. Effect of low- and high-frequency TENS on Met-enkephalin-Arg-Phe and dynorphin A immunoreactivity in human lumbar CSF. Pain. 1991;47(3):295–298. doi: 10.1016/0304-3959(91)90218-m. [DOI] [PubMed] [Google Scholar]
- 22.Han J.-S. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends in Neurosciences. 2003;26(1):17–22. doi: 10.1016/s0166-2236(02)00006-1. [DOI] [PubMed] [Google Scholar]
- 23.Li Y. J., Zhong F., Yu P., Han J. S., Cui C. L., Wu L. Z. Electroacupuncture treatment normalized sleep disturbance in morphine withdrawal rats. Evidence-Based Complementary and Alternative Medicine. 2011;2011 doi: 10.1093/ecam/nep133.361054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bearn J., Swami A., Stewart D., Atnas C., Giotto L., Gossop M. Auricular acupuncture as an adjunct to opiate detoxification treatment: effects on withdrawal symptoms. Journal of Substance Abuse Treatment. 2009;36(3):345–349. doi: 10.1016/j.jsat.2008.08.002. [DOI] [PubMed] [Google Scholar]
- 25.Lua P. L., Talib N. S. Auricular acupuncture for drug dependence: an open-label randomized investigation on clinical outcomes, health-related quality of life, and patient acceptability. Alternative Therapies in Health and Medicine. 2013;19(4):28–42. [PubMed] [Google Scholar]
- 26.Lua P. L., Talib N. S., Ismail Z. Methadone maintenance treatment versus methadone maintenance treatment plus auricular acupuncture. Journal of Pharmacy Practice. 2013;26(6):541–550. doi: 10.1177/0897190013489574. [DOI] [PubMed] [Google Scholar]
- 27.Baker T. E., Chang G. The use of auricular acupuncture in opioid use disorder: a systematic literature review. The American Journal on Addictions. 2016;25(8):592–602. doi: 10.1111/ajad.12453. [DOI] [PubMed] [Google Scholar]
- 28.Chen V. C., Ting H., Wu M. H., Lin T. Y., Gossop M. Sleep disturbance and its associations with severity of dependence, depression and quality of life among heroin-dependent patients: a cross-sectional descriptive study. Substance Abuse Treatment, Prevention, and Policy. 2017;12(1):p. 16. doi: 10.1186/s13011-017-0101-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chen Y. Z., Huang W. L., Shan J. C., Lin Y. H., Chang H. C., Chang L. R. Self-reported psychopathology and health-related quality of life in heroin users treated with methadone. Neuropsychiatric Disease and Treatment. 2013;9:41–48. doi: 10.2147/ndt.s37284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Chiu J. H., Chung M. S., Cheng H. C., et al. Different central manifestations in response to electroacupuncture at analgesic and nonanalgesic acupoints in rats: a manganese-enhanced functional magnetic resonance imaging study. Canadian Journal of Veterinary Research. 2003;67(2):94–101. [PMC free article] [PubMed] [Google Scholar]
- 31.Xu H., Shi Y., Xiao Y., et al. Efficacy comparison of different acupuncture treatments for primary insomnia: a bayesian analysis. Evidence-Based Complementary and Alternative Medicine. 2019;2019:13. doi: 10.1155/2019/8961748.8961748 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Yeung W. F., Chung K. F., Poon M. M., et al. Prescription of Chinese herbal medicine and selection of acupoints in pattern-based traditional Chinese medicine treatment for insomnia: a systematic review. Evidence-Based Complementary and Alternative Medicine. 2012;2012:16. doi: 10.1155/2012/902578.902578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Yeung W.-F., Chung K.-F., Poon M. M.-K., et al. Acupressure, reflexology, and auricular acupressure for insomnia: a systematic review of randomized controlled trials. Sleep Medicine. 2012;13(8):971–984. doi: 10.1016/j.sleep.2012.06.003. [DOI] [PubMed] [Google Scholar]
- 34.Tseng H.-M., Lu J.-f., Gandek B. Cultural issues in using the SF-36 health survey in asia: results from Taiwan. Health and Quality of Life Outcomes. 2003;1(1):p. 72. doi: 10.1186/1477-7525-1-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ware J. E., Jr., Sherbourne C. D. The MOS 36-ltem short-form health survey (SF-36) Medical Care. 1992;30(6):473–483. doi: 10.1097/00005650-199206000-00002. [DOI] [PubMed] [Google Scholar]
- 36.Ware J. E., Jr., Kosinski M., Bayliss M. S., McHorney C. A., Rogers W. H., Raczek A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the medical outcomes study. Medical Care. 1995;33(4 Suppl):264–279. [PubMed] [Google Scholar]
- 37.Lins L., Carvalho F. M. SF-36 total score as a single measure of health-related quality of life: scoping review. SAGE Open Medicine. 2016;4 doi: 10.1177/2050312116671725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Chen Y. L., Lee T. C., Chen Y. T., Lo L. C., Hsu W. Y., Ouyang W. C. Efficacy of electroacupuncture combined with methadone maintenance therapy: a case-control study. Evidence-Based Complementary and Alternative Medicine. 2019;2019:7. doi: 10.1155/2019/7032581.7032581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Greco M.-A., Fuller P. M., Jhou T. C., et al. Opioidergic projections to sleep-active neurons in the ventrolateral preoptic nucleus. Brain Research. 2008;1245:96–107. doi: 10.1016/j.brainres.2008.09.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Wang D., Teichtahl H. Opioids, sleep architecture and sleep-disordered breathing. Sleep Medicine Reviews. 2007;11(1):35–46. doi: 10.1016/j.smrv.2006.03.006. [DOI] [PubMed] [Google Scholar]
- 41.Rasmussen K., Beitner-Johnson D., Krystal J., Aghajanian G., Nestler E. Opiate withdrawal and the rat locus coeruleus: behavioral, electrophysiological, and biochemical correlates. The Journal of Neuroscience. 1990;10(7):2308–2317. doi: 10.1523/jneurosci.10-07-02308.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Van Bockstaele E. J., Peoples J., Menko A. S., McHugh K., Drolet G. Decreases in endogenous opioid peptides in the rat medullo-coerulear pathway after chronic morphine treatment. The Journal of Neuroscience. 2000;20(23):8659–8666. doi: 10.1523/jneurosci.20-23-08659.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Yao W., Yang H., Ding G. Mechanisms of Qi-blood circulation and Qi deficiency syndrome in view of blood and interstitial fluid circulation. Journal of Traditional Chinese Medicine. 2013;33(4):538–544. doi: 10.1016/s0254-6272(13)60162-4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used to support the findings of this study are available from the corresponding author upon request.