

Objective:
To identify the primary health conditions that cause presenteeism, and to estimate the economic cost of lost productivity due to presenteeism in Japan.
Methods:
We conducted an Internet survey among 10,000 Japanese workers. Participants were asked to answer the health condition most affecting their work. Presenteeism was evaluated using the Quantity and Quality methods, and we estimated an annualized cost per capita and nation.
Results:
The common health conditions most interfering with work were neck pain or stiff shoulders, low back pain, and mental illnesses. The annualized costs of presenteeism per capita for each were $414.05, $407.59, and $469.67, respectively. The estimated national costs for each were all above $27 billion.
Conclusions:
Mental illnesses and musculoskeletal symptoms were the leading causes of presenteeism in Japan, and the economic burden of presenteeism was considerably large.
Keywords: cost, health, presenteeism, productivity, worker
Health problems among workers have a negative impact on work as well as their quality of life.1,2 Among the costs related to workers’ health, lost productivity costs are significantly greater than medical and pharmacy costs, and are on average, approximately 2.3 times higher.3 Workers’ lost productivity includes absenteeism (productivity loss that stems from being absent from work) and presenteeism (productivity loss that stems from being at work while ill and performing at a lower level than usual). In addition, presenteeism is a risk factor for subsequent absenteeism.4,5 Moreover, several studies have demonstrated that costs incurred from presenteeism are much larger than costs incurred from absenteeism,6–9 and accounted for the largest proportion of the total health-related costs.6–8 Therefore, to increase company productivity, it is important to identify and address the health issues that cause presenteeism.
Many studies have investigated the economic burden of presenteeism due to various health conditions.8,10–13 A recent U.S. large-scale study has indicated that musculoskeletal pain, mental illnesses, and headaches were the health conditions with the highest estimated cost of presenteeism.10 A previous study on employees at pharmaceutical companies in Japan revealed that the top five health conditions related to the economic costs of presenteeism were painful neck or stiff shoulders, insufficient sleep, back pain, eye problems, and depression.11 This study, however, was only conducted within one type of industry, which makes it difficult to compare with other industries and estimate the economic cost due to presenteeism for all Japanese workers. To our knowledge, as yet, there has been no large-scale nationwide study in Japan that has included workers from many different industries and with different occupations.
In promoting management to improve work productivity, it is essential to reveal the impact of health conditions on presenteeism in each industry including the aspect of economic burden in Japan. The present study aims to identify the primary health conditions that cause presenteeism by industry, and to estimate the economic cost of lost productivity due to presenteeism in Japan.
METHODS
We conducted an online survey on health conditions and work productivity during September and October 2019. Japanese workers aged between 20–69 years (n = 10,000) were included, and the participants were recruited by an Internet research company, hamon Co., Ltd. (Kanagawa, Japan), with approximately 1.58 million individuals across Japan registered voluntarily on their website. The volunteers were stratified by age and sex, and the participants were randomly selected according to the demographic distribution in Japan. Subsequently, 151,086 individuals were invited to participate in this study via an e-mail that contained a URL link to the survey. Among these individuals, the questionnaire screen was displayed only for those who understood the purpose of this study and provided their consent to participate.
The survey was closed when the number of respondents reached 10,000. All the participants completed the questionnaire without missing any data because the online survey was set to reject incomplete responses automatically. The participants received online shopping points as a reward. The study protocol was approved by the research ethics committee of the Graduate School of Medicine and Faculty of Medicine at the University of Tokyo (No. 2019147NI).
Assessment
Information on sex, age, body weight, height, marital status, education, type of employment, type of industry, size of the company, annual income, health conditions, and presenteeism were collected using the self-administered online survey. The Japanese Standard Industrial Classification developed by the Ministry of Internal Affairs and Communication14 was used to determine the type of industry. Then, these data were categorized into three groups: primary (agriculture, forestry, and fishery), secondary (mining, construction, and manufacture), and tertiary industries (other, mainly indoor types including wholesale or retail trade, medical, health care and welfare, and services). Company size was categorized into three groups: small (<100 employees), medium (100–999 employees), and large (1000 ≤ employees) according to the Basic Survey on Wage Structure conducted by the Ministry of Health, Labour and Welfare in Japan.15 The respondents were asked to choose one response for annual income (JPY) from the following options: less than 2 million, 2–4 million, 4–6 million, 6–8 million, 8–10 million, and 10 million JPY or more.
Presenteeism and Estimate Costs
We evaluated the degree of presenteeism and estimated its economic costs using the following procedure. First, we asked whether the participants had health problems in the past 4 weeks. Multiple answers were allowed among the following 14 health conditions that were chosen as they were used as highly prevalent symptoms in a previous study:16 allergies, skin disease/itchiness, infectious diseases, gastrointestinal disorders, painful or disabling arm and leg joints, low back pain, neck pain or stiff shoulders, headaches, tooth troubles, mental illnesses, sleep-related problems, weariness or fatigue, eye problems, and others. Second, if they responded that they had one or more health conditions, we asked which health condition out of the health issues they selected had the largest impact on their work. Third, the participants were asked how many days they had experienced the health condition with the largest over the past 4 weeks.
In addition, they were asked about the degree of presenteeism, that is, the extent to which the selected symptom affected the quantity and quality of their work. The respondents were asked to indicate in detail how much work they actually performed during regular hours when the symptoms were present and the quality of their work compared to when the symptoms were not present. The answers were scored on an 11-point numerical rating scale from 0 (no productivity) to 10 (regular productivity). This measurement, the Quantity and Quality method, has been adopted in previous studies,11,17,18 and the construct validity has been demonstrated previously.18
For income, we adopted the median value of the choices from the questionnaire (JPY) as follows: less than 2, 2–4, 4–6, 6–8, 8–10, and 10 million JPY or more were converted into 2, 3, 5, 7, 9, and 10 million JPY, respectively. We then calculated a daily wage by dividing the median by 240 (12 mo with 20 working d). The costs were then converted into US Dollar (USD) using the average exchange rate in February 2020 (1 USD = 109.9735 JPY). We then calculated the degree of presenteeism and estimated the monetary value of the productivity loss due to presenteeism per worker (hereinafter called per capita) using the following formula:
 |
Monetary value of the productivity loss due to presenteeism
 |
National cost estimates were calculated by multiplying the above monetary value of the productivity loss due to presenteeism per capita by the number of workers across Japan.19
Statistical Analysis
Data on the characteristics of the study participants were presented as number (percentage) for the categorical variables or as median (25th, 75th percentiles) for the continuous variables. Comparisons of the characteristics of workers with or without health-related symptoms were evaluated using a chi-squared test or Wilcoxon rank-sum test. A P value of less than 0.05 was considered statistically significant. Statistical analyses were performed using JMP® 14 (SAS Institute Inc., Cary, NC, USA).
RESULTS
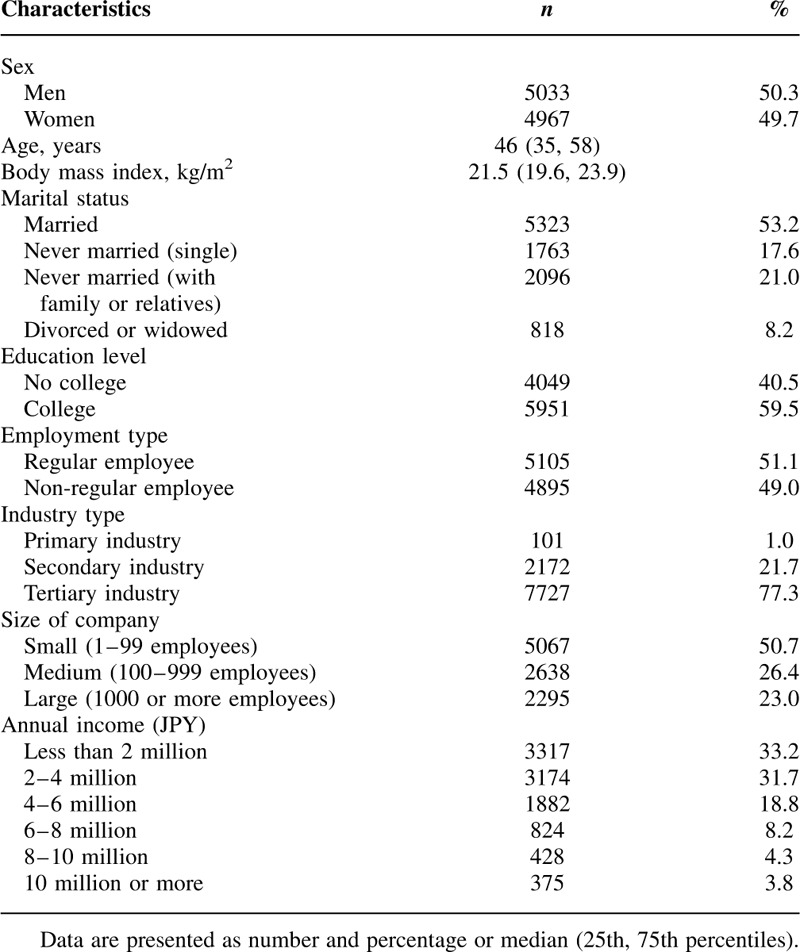
Table 1 shows the characteristics of the study participants. The median age of the participants in this study was 46 years, and 50.3% were men. The proportion of workers in the tertiary industry was the highest of the three industrial categories.
TABLE 1.
Characteristics of the Study Participants (n = 10,000)
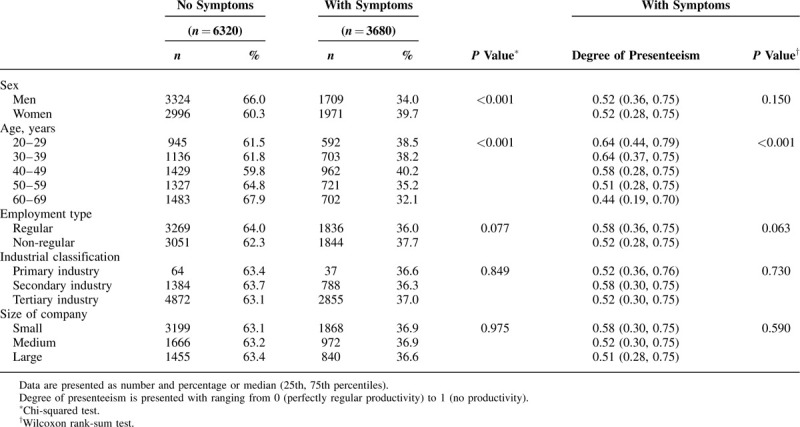
In total, 36.8% of the participants had a health problem that interfered with their work during the past 4 weeks. A comparison of the demographic distribution of workers with or without health-related symptoms affecting their work is shown in Table 2. Women with symptoms interfering with work were more frequent than men with symptoms, and workers aged 40 to 49 years had the highest prevalence of symptoms (40.2%). Younger workers tended to have high levels of presenteeism relative to older workers.
TABLE 2.
Comparison of the Characteristics of Workers With or Without Symptoms Affecting Work and the Degree of Presenteeism
Among the primary health conditions that interfered most with work, the symptoms selected the most were neck pain or stiff shoulders, low back pain, and mental illnesses (Fig. 1). The top symptom was low back pain for men, and neck pain or stiff shoulders for women. The number of men and women with mental illnesses and sleep-related problems was similar. However, headaches were more frequent among women than among men.
FIGURE 1.
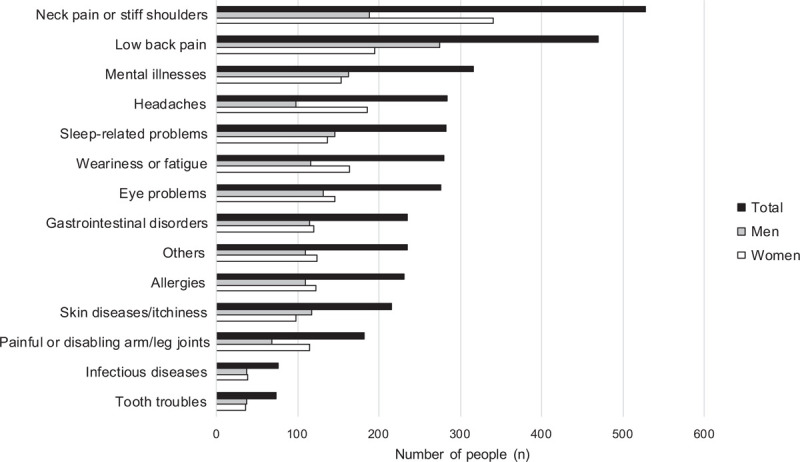
. Primary health conditions that interfered most with work.
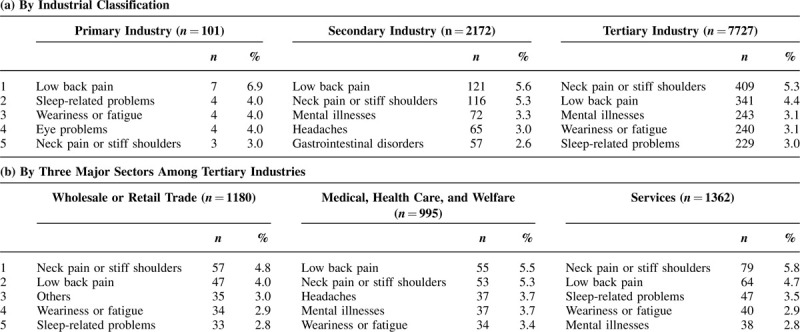
Table 3 presents the top five health conditions that have the largest impact on work by the industrial category, and demonstrates that low back pain was the leading symptom among workers in primary and secondary industries (a). The ranking of the health conditions in the three sectors with the highest number of employees among the tertiary industry (wholesale or retail trade/medical, healthcare, and welfare/services) are shown in b. Although there were some differences in the order of the primary health condition that caused presenteeism by industry sector, musculoskeletal pain, including neck pain and low back pain, was consistently the most common symptom.
TABLE 3.
Top Five Health Conditions That Have the Most Impact on Work by Industrial Classifications
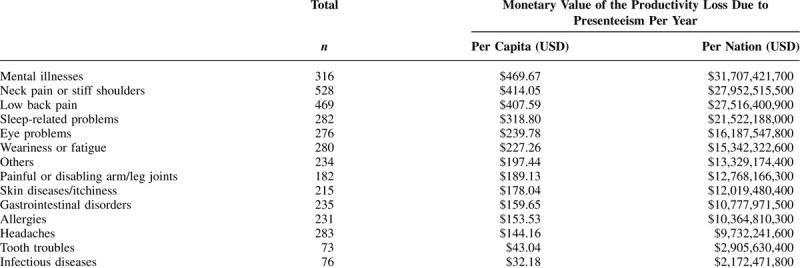
Estimates of the mean annualized costs of productivity loss due to presenteeism by each health condition are shown in Table 4. The primary health conditions with the highest cost per capita were mental illnesses (469.67 USD/capita), neck pain or stiff shoulders (414.05 USD), low back pain (407.59 USD), sleep-related problems (318.80 USD), and eye problems (239.78 USD). National cost estimates per year for the above symptoms, based on the total number of employees in Japan, were as follows: approximately 31.7 billion USD for mental illnesses, 28 billion USD for neck pain or stiff shoulders, 27.5 billion USD for low back pain, 21.5 billion USD for sleep-related problems, and 16.2 billion USD for eye problems.
TABLE 4.
Monetary Value of the Productivity Loss due to Presenteeism Per Year by Health Condition
DISCUSSION
This study aimed to determine the main health conditions that caused presenteeism, and estimate the economic impact of the loss of work productivity due to presenteeism in Japan. The primary health conditions that interfered the most with work were neck pain or stiff shoulders, low back pain, and mental illnesses. Moreover, the economic burden of presenteeism was considerably higher for mental illnesses and musculoskeletal symptoms, with estimated annualized costs of more than 400 USD per capita. This is the first study with a large sample to determine the economic impact of presenteeism across Japan.
We revealed that the main common health conditions interfering with work were neck pain or stiff shoulders, low back pain, mental illnesses, headaches, and sleep-related problems. The ranking of neck disorders and back pain by sex was similar to the results from the Comprehensive Survey of Living Conditions, the national survey that is conducted periodically to investigate basic information including health conditions for approximately 290,000 households in Japan.20 Mental illnesses21 such as depression or anxiety, headaches,22 and poor sleep23 have also been demonstrated to be the major causes of lost work productivity, which may be attributed to the high prevalence of these symptoms among workers. For example, the prevalence of migraine headaches is highest among workers aged between 25–44 years, which is the peak productivity age.24,25 This finding will need to be considered in health management initiatives.
We found that the degree of presenteeism in young to middle-aged workers tended to be higher than in other workers (Table 2). This was similar to a previous study among Canadians.26 Younger workers may attend work even when they feel unwell, presumably because of attendance requirements or career-related concerns. Our findings imply the significant impact of age on presenteeism.
We identified the common health conditions that caused presenteeism by the industrial category. In primary and secondary industries, the top health condition affecting work was low back pain. This may be due to the occupational, physical characteristics of these industries. Although neck pain or stiff shoulders was ranked first in the tertiary industries as a whole, low back pain was most frequent among workers in the medical, healthcare, and welfare. Indeed, many studies have indicated that healthcare workers, including nurses and caregivers, have a higher prevalence of low back pain than those with other occupations.27,28 We found that health conditions varied somewhat by industry, although musculoskeletal symptoms, including low back pain and neck pain, were consistently ranked the highest. These results may imply the importance of measures for the prevention/control of musculoskeletal symptoms throughout all the industries.29 Moreover, we used the Japanese Standard Industrial Classification in the present study, to demonstrate the list of primary health problems affecting work by industry. This classification is similar to the International Standards Industrial Classification of All Economic Activities (ISIC). To our knowledge, there are no studies that currently indicate the list of primary health conditions interfering with work by industry. A prospective study has demonstrated that changes in health status are strongly associated with improvement in productivity.30 Our results may help to formulate a strategy to improve productivity for workers in specific industries.
We estimated the economic impact of health conditions on the loss of work productivity due to presenteeism as a monetary value. The five health conditions with the highest economic costs due to presenteeism in our study were mental illnesses, neck pain or stiff shoulders, low back pain, sleep-related problems, and eye problems. Previous studies in Japan11,12 indicated that mental illnesses, including depression and anxiety, and musculoskeletal disorders such as back pain and neck pain account for a large portion of the economic burden of productivity loss due to presenteeism. These previous studies, however, were not on a sampling enough to estimate national figures. In addition, Loeppke et al13 investigated the costs of health-related presenteeism in U.S. companies, and indicated that the estimated costs of productivity loss were especially high for fatigue, depression, back/neck pain, and sleep problems. Our findings were similar to these results, although there was a slight disparity, probably because of the differences in method and the study population. In our study, combining low back pain and neck pain or stiff shoulders as musculoskeletal symptoms led to the highest productivity costs from presenteeism, which was the same as previous studies.11,12
Previous studies indicated that indirect costs (including absenteeism and presenteeism) accounted for 62%–75% of total health-related costs.11,31 In addition, Nagata et al reported that the proportion of the monetary value due to presenteeism was 64% among total costs, and that due to absenteeism was 11%.11 Indeed, a previous international and epidemiological study indicated that the proportion of absenteeism due to musculoskeletal conditions was much lower in Japan than in UK.28 In light of these findings, it is assumed that the economic burden of our estimated costs for presenteeism would be considerably large among total health-related costs.
In an Internet survey, a potential selection bias and representativeness of the sample are important issues. Although the sample in the present study was selected according to the demographic distribution in Japan (sex and age), the Internet research volunteers may differ from the general population in several aspects. Therefore, we need to be careful when interpreting the results of the present study. The annual income of the participants was relatively lower than that of the general working population investigated by the National Tax Agency in Japan,32 which may have caused us to underestimate economic costs in our study. In addition, compared to data from a national survey by the Japanese government,33 our sample had a slightly larger proportion of the tertiary industry (71% in the national survey vs. 77% in our study), which resulted in a small proportion of the primary industry in our study. Although three industry types (primary, secondary, and tertiary) did not show significant differences in the proportion of workers with symptoms affecting work and the degree of presenteeism in the present study (Table 2), the health conditions which caused presenteeism were different slightly by industry (Table 3). Therefore, the differences in characteristics between the included participants and the general population may have affected our results.
In addition to the points above, our study has other limitations. First, recall bias is an important issue in the present study. If the recall duration is shortened, there could be more accuracy in recalling the days on which participants experienced health problems. However, the influence of acute illnesses could be overestimated to approximate the situation for a year. We adopted the relatively widely-used 4-week period as the recall duration of presenteeism.34 However, it may have been challenging to remember the exact number of days in which participants suffered from health problems. Second, we conducted an online survey only once during the fall season. Seasonal symptoms may have affected our results, although chronic health problems would not have affected the findings. Third, we estimated the costs of presenteeism using the primary symptom that interferes with work for each participant. However, many workers may suffer multiple health problems. Therefore, the economic costs of presenteeism for each health condition may have been underestimated in the present study.
CONCLUSION
In summary, mental illnesses and musculoskeletal symptoms were the leading cause of presenteeism in workplaces in Japan, and the economic burden of productivity loss due to presenteeism was considerably large, especially for the above health conditions. Our findings on the link between health conditions and productivity loss due to presenteeism, including the economic impact, would provide an important perspective for managing the influence of poor health in the workplace.
Footnotes
This study protocol was approved by the research ethics committee of the Graduate School of Medicine and Faculty of Medicine at the University of Tokyo (No. 2019147NI).
This study was supported by a grant from the Ministry of Health, Labour and Welfare (No. 19FG1001) and Nippon Zoki Pharmaceutical Co. Ltd. These funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
All authors declare the following potential conflicts of interest: KM is a shareholder/adviser of Trunk Solution CO., Ltd. and received the following support: a research grant from the Ministry of Health, Labour and Welfare for the submitted work; grant support from Sumitomo Dainippon Pharma Co., Ltd. and Okamura Corporation; grant support, including lecture fees from AYUMI Pharmaceutical Corporation, Nippon Zoki Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., LTD., Eli Lilly Japan K.K., Astellas Pharma Inc., TOTO LTD., and Eisai Co., Ltd.; lecture fees from Pfizer Japan Inc., Hisamitsu Pharmaceutical Co., Inc., Janssen Pharmaceutical K.K., Kaken Pharmaceutical Co., LTD., and Teijin Pharma Limited; and lecture fees and advisory fees from Shionogi & Co., Ltd., MTG Co., Ltd., Sompo Holdings, Inc., NUVASIVE Japan, Murata Manufacturing Co., Ltd. outside the submitted work. HO received grants from Teijin Pharma Limited, Pfizer Inc., and Fujifilm Medical Co., Ltd.; grants and personal fees from AYUMI Pharmaceutical Corporation, Nippon Zoki Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., LTD. MTG Co., Ltd., Sompo Holdings, Inc., and NUVASIVE Japan; and grants from Eli Lilly Japan K.K. outside the submitted work. The other authors have no competing interests to report.
Clinical significance: Mental illnesses and musculoskeletal symptoms were the leading causes of presenteeism in the workplace, and the economic burden of productivity loss due to presenteeism was considerably large in Japan. Our findings may provide an important perspective for managing the impact of poor health in the workplace.
REFERENCES
- 1.Schultz AB, Edington DW. Employee health and presenteeism: a systematic review. J Occup Rehabil 2007; 17:547–579. [DOI] [PubMed] [Google Scholar]
- 2.Schwerha JJ. Occupational medicine forum. J Occup Environ Med 2006; 48:102–104. [DOI] [PubMed] [Google Scholar]
- 3.Loeppke R, Taitel M, Haufle V, Parry T, Kessler RC, Jinnett K. Health and productivity as a business strategy: a multiemployer study. J Occup Environ Med 2009; 51:411–428. [DOI] [PubMed] [Google Scholar]
- 4.Taloyan M, Aronsson G, Leineweber C, Magnusson Hanson L, Alexanderson K, Westerlund H. Sickness presenteeism predicts suboptimal self-rated health and sickness absence: a nationally representative study of the Swedish working population. PLoS One 2012; 7:e44721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Janssens H, Clays E, De Clercq B, De Bacquer D, Braeckman L. The relation between presenteeism and different types of future sickness absence. J Occup Health 2013; 55:132–141. [DOI] [PubMed] [Google Scholar]
- 6.Hemp P. Presenteeism: at work—but out of it. Harv Bus Rev 2004; 82:49–58. 155. [PubMed] [Google Scholar]
- 7.Collins JJ, Baase CM, Sharda CE, et al. The assessment of chronic health conditions on work performance, absence, and total economic impact for employers. J Occup Environ Med 2005; 47:547–557. [DOI] [PubMed] [Google Scholar]
- 8.Goetzel RZ, Long SR, Ozminkowski RJ, Hawkins K, Wang S, Lynch W. Health, absence, disability, and presenteeism cost estimates of certain physical and mental health conditions affecting U.S. employers. J Occup Environ Med 2004; 46:398–412. [DOI] [PubMed] [Google Scholar]
- 9.Iverson D, Lewis KL, Caputi P, Knospe S. The cumulative impact and associated costs of multiple health conditions on employee productivity. J Occup Environ Med 2010; 52:1206–1211. [DOI] [PubMed] [Google Scholar]
- 10.Allen D, Hines EW, Pazdernik V, Konecny LT, Breitenbach E. Four-year review of presenteeism data among employees of a large United States health care system: a retrospective prevalence study. Hum Resour Health 2018; 16:59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nagata T, Mori K, Ohtani M, et al. Total health-related costs due to absenteeism, presenteeism, and medical and pharmaceutical expenses in Japanese employers. J Occup Environ Med 2018; 60:e273–e280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wada K, Arakida M, Watanabe R, Negishi M, Sato J, Tsutsumi A. The economic impact of loss of performance due to absenteeism and presenteeism caused by depressive symptoms and comorbid health conditions among Japanese workers. Ind Health 2013; 51:482–489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Loeppke R, Taitel M, Richling D, et al. Health and productivity as a business strategy. J Occup Environ Med 2007; 49:712–721. [DOI] [PubMed] [Google Scholar]
- 14.Ministry of Internal Affairs and Communications. Japanese Standard Industrial Classification. Available at: https://www.soumu.go.jp/toukei_toukatsu/index/seido/sangyo/H25index.htm. Accessed June 1, 2020. [Google Scholar]
- 15.Ministry of Health, Labour and Welfare. Summary Report of Basic Survey on Wage Structure (Nationwide) 2012. Available at: https://www.mhlw.go.jp/english/database/db-l/dl/24gaikyo_zenkoku_Eng.pdf. Accessed June 1, 2020. [Google Scholar]
- 16.Chimed-Ochir O, Nagata T, Nagata M, Kajiki S, Mori K, Fujino Y. Potential work time lost due to sickness absence and presence among Japanese workers. J Occup Environ Med 2019; 61:682–688. [DOI] [PubMed] [Google Scholar]
- 17.Hoeijenbos M, Bekkering T, Lamers L, Hendriks E, van Tulder M, Koopmanschap M. Cost-effectiveness of an active implementation strategy for the Dutch physiotherapy guideline for low back pain. Health Policy 2005; 75:85–98. [DOI] [PubMed] [Google Scholar]
- 18.Brouwer WB, Koopmanschap MA, Rutten FF. Productivity losses without absence: measurement validation and empirical evidence. Health Policy 1999; 48:13–27. [DOI] [PubMed] [Google Scholar]
- 19.Statistics Bureau of Japan. Labour Force Survey (Survey date 2019 Aug). Available at: https://www.stat.go.jp/data/roudou/rireki/tsuki/pdf/201908.pdf (Japanese). Accessed June 1, 2020. [Google Scholar]
- 20.Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions 2016. Available at: https://www.mhlw.go.jp/toukei/list/dl/20-21-h28.pdf. Accessed June 1, 2020. [Google Scholar]
- 21.Stewart WF, Ricci JA, Chee E, Hahn SR, Morganstein D. Cost of lost productive work time among US workers with depression. Jama 2003; 289:3135–3144. [DOI] [PubMed] [Google Scholar]
- 22.Burton WN, Landy SH, Downs KE, Runken MC. The impact of migraine and the effect of migraine treatment on workplace productivity in the United States and suggestions for future research. Mayo Clin Proc 2009; 84:436–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Rosekind MR, Gregory KB, Mallis MM, Brandt SL, Seal B, Lerner D. The cost of poor sleep: workplace productivity loss and associated costs. J Occup Environ Med 2010; 52:91–98. [DOI] [PubMed] [Google Scholar]
- 24.Stewart WF, Lipton RB, Celentano DD, Reed ML. Prevalence of migraine headache in the United States. Relation to age, income, race, and other sociodemographic factors. JAMA 1992; 267:64–69. [PubMed] [Google Scholar]
- 25.Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies. Headache 2015; 55:21–34. [DOI] [PubMed] [Google Scholar]
- 26.Gosselin E, Lemyre L, Corneil W. Presenteeism and absenteeism: differentiated understanding of related phenomena. J Occup Health Psychol 2013; 18:75–86. [DOI] [PubMed] [Google Scholar]
- 27.Leighton DJ, Reilly T. Epidemiological aspects of back pain: the incidence and prevalence of back pain in nurses compared to the general population. Occup Med (Lond) 1995; 45:263–267. [DOI] [PubMed] [Google Scholar]
- 28.Matsudaira K, Palmer KT, Reading I, Hirai M, Yoshimura N, Coggon D. Prevalence and correlates of regional pain and associated disability in Japanese workers. Occup Environ Med 2011; 68:191–196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hagberg M, Violante FS, Bonfiglioli R, et al. Prevention of musculoskeletal disorders in workers: classification and health surveillance—statements of the Scientific Committee on Musculoskeletal Disorders of the International Commission on Occupational Health. BMC Musculoskelet Disord 2012; 13:109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Burton WN, Chen CY, Conti DJ, Schultz AB, Edington DW. The association between health risk change and presenteeism change. J Occup Environ Med 2006; 48:252–263. [DOI] [PubMed] [Google Scholar]
- 31.Sadosky AB, DiBonaventura M, Cappelleri JC, Ebata N, Fujii K. The association between lower back pain and health status, work productivity, and health care resource use in Japan. J Pain Res 2015; 8:119–130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.National Tax Agency. Statistical Survey of Actual Status for Salary in the Private Sector. Available at: https://www.nta.go.jp/publication/statistics/kokuzeicho/minkan2018/pdf/001.pdf (Japanese). Accessed June 1, 2020. [Google Scholar]
- 33.Statistics Bureau of Japan. Population Census. Available at: https://www.stat.go.jp/data/kokusei/2015/kekka/kihon2/pdf/gaiyou.pdf (Japanese). Accessed June 1, 2020. [Google Scholar]
- 34.Schultz AB, Chen CY, Edington DW. The cost and impact of health conditions on presenteeism to employers: a review of the literature. Pharmacoeconomics 2009; 27:365–378. [DOI] [PubMed] [Google Scholar]