

Background
Sometimes, unintended reduction of a strangulated hernia can occur intraoperatively, while manipulating the sac, leading to uncertainty about the viability of its contents.1 We describe a technique that helps to identify any possible ischaemic tissue after an accidental reduction of strangulated hernia.
Technique
Following accidental reduction of the sac contents of a strangulated hernia (Fig 1) into the abdominal cavity, a 10mm port is placed intra-abdominally via the open hernia sac (Fig 2) after inserting a pursestring suture, to prevent a leak of CO2. Alternatively, if the defect is small, a balloon port can be used. Pneumoperitoneum is established. A 10mm scope is used for laparoscopy of the abdominal cavity. The reduced contents are typically close to the port site. Nevertheless, a full laparoscopy and insertion of a 5mm port through the abdominal wall is recommended, in order to inspect as much of the bowel as possible.
Figure 1.
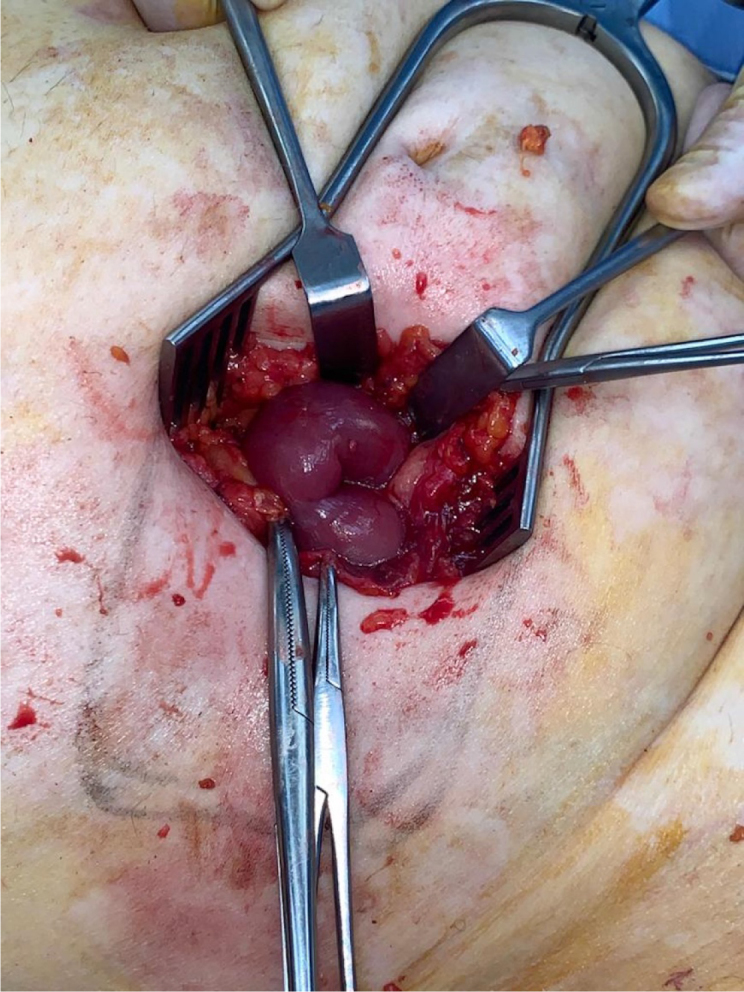
Strangulated abdominal hernia. Hernia sac was opened and bowel was visualised.
Figure 2.
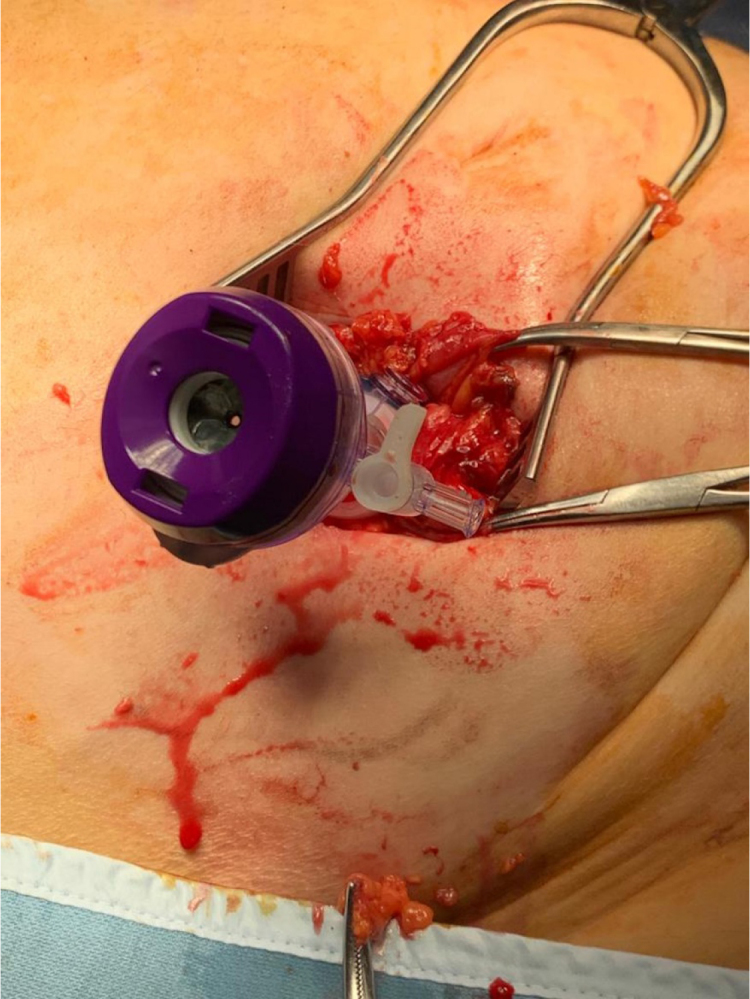
A 10mm port was inserted, via the hernia sac opening, in the peritoneal cavity
In case of finding ischaemic bowel, there are two options: 1) to guide the loop of bowel through the hernia defect, with the use of a laparoscopic atraumatic grasper via the 5mm abdominal port, or 2) to switch to a 5mm scope and with a Babcock forceps, via the hernia site, to externalise the bowel and perform a resection and anastomosis. Some extension of the original incision may be needed.
Discussion
This technique is safe and avoids unnecessary extensive laparotomies in case of accidental intraoperative reduction of a strangulated hernia content.
Reference
- 1.Yang GP. Laparoscopy in emergency hernia repair. Ann Laparosc Endosc Surg 2017; : 107. [Google Scholar]