

Abstract
Alpha-fetoprotein (AFP)-producing gastric cancer (AFPGC) is a relatively rare type of gastric cancer (GC). To improve the early diagnosis and treatment of AFPGC, we thoroughly investigated the clinicopathological features and prognosis of AFPGC. 139 GC patients who had received treatment from January 2013 to March 2016 in Jinan Central Hospital were included in this study. Blood samples for the pretreatment AFP examinations were collected. The relationship between the serum AFP and the clinicopathological features and prognosis were analyzed. Among the 139 GC cases, 16 cases (11.5%) were AFPGC patients. Compared with the AFP-negative (non-AFPGC) group, the AFPGC patients were prone to have distant metastasis (P=0.029), particularly in the liver, and the abdominal metastasis accounted for 79.4% (27/34). AFPGC patients’ cancer is clearly prone to occur in the upper third of the stomach (P=0.008) and among younger (≤60 years old) patients (P=0.044). Furthermore, among the young and middle-aged (≤60 years old) patients, there were no significant differences in the serum carcinoembryonic antigen (CEA), the cancer antigen 19-9 (CA19-9), or the combined (CEA+CA19-9) positive rate between the AFPGC and the non-AFPGC patients. A Kaplan-Meier survival analysis showed that the median overall survival (mOS) of patients with AFPGC was significantly less than it was among the non-AFPGC patients (P=0.042). The serum AFP level (<100 ng/ml vs ≥100 ng/ml) is a prognostic factor for overall survival in AFPGC patients (P=0.041). In conclusion, the real-time examination of serum AFP has great diagnostic and prognostic value for managing AFPGC, especially for young and middle-aged patients.
Keywords: Gastric cancer, α-fetoprotein, pathological features, prognosis
Introduction
Alpha-fetoprotein (AFP) is a glycoprotein produced and secreted during the prenatal period by the liver, yolk sac, and gastrointestinal (GI) tract [1,2]. In clinical practice, AFP commonly serves as an important tumor marker for hepatocellular carcinoma (HCC) or yolk sac tumors. However, some diseases other than HCC and yolk sac tumors are also associated with high serum levels of AFP, among which gastric cancer is the most common [3,4]. AFP-producing gastric cancer (AFPGC) was first described by Bourreille et al. [5] in 1970, and gastric cancer with a high level of AFP is termed AFPGC [6]. AFPGC is a relatively rare type of malignancy, which comprises 2.7-8% of all GCs [7].
AFPGC is characterized by a high incidence of metastases to the liver and lymph nodes, and a poor prognosis [6,8,9]. However, there is still no standardized process for the treatment of patients with AFPGC. Thus, it is necessary and valuable to pay attention to the clinical observations of AFPGC. Currently, there are few published studies on the clinicopathology or prognosis of AFPGC, and most previous studies are case reports. Moreover, the main possible pathway for liver metastasis of gastric cancer is unclear.
On the basis of the considerations mentioned above, in this study, we retrospectively reviewed the clinicopathologic features of AFPGC patients in the Jinan Central Hospital and investigated the prognostic factors. Furthermore, we suggest that AFPGC is clearly prone to occur in the upper third of the stomach, in younger (≤60 years old) patients, and to have distant metastasis. Meanwhile, in this study, among the younger patients (≤60 years old), there were no differences in their serum CEA, cancer antigen 19-9 (CA19-9), or their combined (CEA+CA19-9) positive rates between the AFPGC and non-AFPGC patients, suggesting that an examination of the serum CEA, CA199, or the combined (CEA+CA19-9) in young and middle-aged patients is not conducive to the early diagnosis of AFPGC. A survival analysis of the AFPGC patients showed that the serum AFP level (<100 ng/ml vs ≥100 ng/ml) is a prognostic factor for overall survival. Finally, we conclude that a real-time examination of the serum AFP levels has a great diagnostic and prognostic value for managing AFPGC, especially for young and middle-aged patients.
Materials and methods
Patients and data
269 patients with primary gastric adenocarcinoma were diagnosed and treated in the Jinan Central Hospital from January 2013 to March 2016. The inclusion criteria were as follows: 1. Primary diagnosis of GC or at the first treatment after a diagnosis of GC, aged 20-86; 2. Determined the pathological tissue through fiberoptic endoscopy, spiral CT, or other methods before surgery; 3. The cardiopulmonary function of the patient is generally normal, the cardiac function test and ECG results are within the normal range, and no history of serious cardiopulmonary disease; 4. No chemoradiotherapy was performed before the surgery; 5. Have complete clinical data such as a clear clinical stage and basic personal information. Meanwhile, the exclusion criteria were as follows: 1. Underwent chemoradiotherapy before the surgery; 2. Poor physical condition; 3. GC is not the primary lesion; 4. Have multiple diseases, including acute or chronic hepatitis, cirrhosis, fatty liver, alcoholic liver, or primary liver cancer when admitted to the hospital; 5. Have incomplete clinical data. The serum AFP, CEA, and CA19-9 levels were determined using enzyme immunoassays (EIA), and concentrations greater than 10 ng/ml, 6 ng/ml, 37 U/ml were considered elevated. According to the above criteria, a total of 139 patients were enrolled in the present study, and 16 of these patients were confirmed to have AFPGC. Immunohistochemistry was used to further confirm the positive expression of AFP in the gastric tissues of the 16 patients. This study was approved by the Ethical Committee of Jinan Central Hospital, and a written informed consent was obtained from all the patients.
Among the 139 patients, a curative proximal, distal, or total gastrectomy with a combined standardized lymph node dissection was performed according to the Japanese Classification of Gastric Carcinoma standard. The patients received follow-up to determine their survival by telephone or a subsequent consultation with a cut-off date of December 2017.
The clinicopathological characteristics, including age, gender, tumor size, tumor location, histological differentiation, depth of invasion, serum AFP level, peripheral lymph node invasion, surgical approach, distant metastasis, clinical stage, and Helicobacter pylori infection were recorded. The tumors were staged according to the seventh edition of the American Joint Committee on Cancer Tumor Node Metastasis (TNM) classification [10]. All the pathological data of the enrolled patients were reviewed independently by two experienced pathologists for the histopathological classification.
Immunohistochemistry
The immunohistochemistry involved the use of biotin-streptavidin-per-oxidase with a Vectastain ABC kit (Vector Laboratories, CA, USA). Simply put, tissue sections (4 μm) were prepared from the paraffin-embedded tissue specimens. The sections were deparaffinized with xylene followed by dehydration in graded alcohol. We heated the sections in a microwave for 2 min at 900 W to retrieve the antigen, and then incubated them with a 0.3% H2O2 solution in methanol for 30 min to block the endogenous peroxidase. After 3 washes with phosphate buffered saline (PBS), the slides were incubated with 10% normal horse serum to block the nonspecific background staining, then they were incubated with primary antibodies rabbit anti-AFP (1:300 dilution, Proteintech, China) in a humid chamber at 4°C overnight. After a washing with PBS, the sections were incubated with biotinylated-horse anti-mouse antibodies for 30 min, washed 3 times with PBS, and incubated with streptavidin-conjugated peroxidase for 30 min. We visualized the sections by incubation with 3,3’-diaminobenzidine solution (0.3% H2O2 and 0.05% 3,3’-diaminobenzidine) and counterstained them with hematoxylin. The omission of the primary antibody was a negative control. Every run included a positive control and a negative control. For the negative control, the primary antibody was replaced with PBS.
Statistical analysis
The statistical analysis was done using SPSS 20.0 (IBM, Armonk, NY, USA). Chi-squared tests or Fisher’s exact tests were used to assess the significant differences in the clinicopathological characteristics. The overall survival (OS) was measured from the time of the resection until death or the last follow-up. The clinicopathologic factors were analyzed using the Kaplan-Meier method and compared using log-rank tests. All the tests were two-sided. A P value <0.05 was considered statistically significant.
Results
General characteristics
Among the 139 GC patients in the study cohort, 103 were male and 36 were female, with a median age of 65.8 years (range, 24-86 years). Regarding the surgical treatment, 75 patients underwent radical or palliative surgery, and 27 patients were transferred or discharged automatically. There were 11 patients who refused the surgery, 19 patients who had no surgical indications for radiotherapy or chemotherapy, and 7 patients who underwent thoracic or abdominal exploration and endoscopic ESD. These patients, including the 16 study patients with AFPGC, had elevated serum AFP levels and positive expressions of AFP in their tissues (Figure 1). The general characteristics are shown in Table 1.
Figure 1.

Representative immunohistochemical staining in the AFPGC tissue and its adjacent tissue (magnification ×200). A. Immunostaining for AFP in AFPGC. B. Immunostaining for AFP in the adjacent tissue.
Table 1.
The clinicopathological features of the AFPGC and non-AFPGC gastric cancer patients
| Characteristics | Total number | AFPGC number (%) | Non-AFPGC number (%) | Chi-square | P value |
|---|---|---|---|---|---|
| Age | 4.067 | 0.044 | |||
| >60 | 92 | 7 (43.75) | 85 (69.11) | ||
| ≤60 | 47 | 9 (56.25) | 38 (30.89) | ||
| Total | 139 | 16 (100) | 123 (100) | ||
| Gender | 1.692 | 0.240 | |||
| female | 36 | 2 (12.50) | 34 (27.64) | ||
| male | 103 | 14 (87.50) | 89 (72.36) | ||
| Total | 139 | 16 (100) | 123 (100) | ||
| Distant metastasis | 5.430 | 0.029 | |||
| yes | 34 | 8 (57.14) | 26 (26.53) | ||
| no | 78 | 6 (42.86) | 72 (73.47) | ||
| Total | 112 | 14 (100) | 98 (100) | ||
| Clinical stage | 7.842 | 0.125 | |||
| 0 | 6 | 0 (0.00) | 6 (6.38) | ||
| I | 13 | 0 (0.00) | 13 (13.83) | ||
| II | 17 | 3 (21.43) | 14 (14.89) | ||
| III | 39 | 3 (21.43) | 36 (38.30) | ||
| IV | 33 | 8 (57.14) | 25 (26.60) | ||
| Total | 108 | 14 (100) | 94 (100) | ||
| Surgical approach | 4.915 | 0.209 | |||
| cardiectomy | 6 | 2 (28.57) | 4 (5.88) | ||
| distal gastrectomy | 47 | 3 (42.86) | 44 (64.71) | ||
| proximal gastrectomy | 3 | 0 (0.00) | 3 (4.41) | ||
| palliative gastrectomy | 9 | 1 (14.29) | 8 (11.76) | ||
| total gastrectomy | 10 | 1 (14.29) | 9 (13.24) | ||
| Total | 75 | 7 (100) | 68 (100) | ||
| Helicobacter pylori infection | 0.061 | 1.000 | |||
| positive | 9 | 1 (8.33) | 8 (10.67) | ||
| negative | 78 | 11 (91.67) | 67 (89.33) | ||
| Total | 87 | 12 (100) | 75 (100) | ||
| Tumor location | 10.319 | 0.008 | |||
| Upper third of stomach | 65 | 4 (25.00) | 61 (52.14) | ||
| Middle third of stomach | 46 | 5 (31.25) | 41 (35.04) | ||
| Distal third of stomach | 22 | 7 (43.75) | 15 (12.82) | ||
| Total | 133 | 16 (100) | 117 (100) | ||
| Tumor size | 1.312 | 0.414 | |||
| ≤5 cm | 49 | 3 (42.86) | 46 (64.79) | ||
| >5 cm | 29 | 4 (57.14) | 25 (35.21) | ||
| Total | 78 | 7 (100) | 71 (100) | ||
| Lymph node metastasis | 0.056 | 1.000 | |||
| Yes | 57 | 5 (62.50) | 52 (66.67) | ||
| No | 29 | 3 (37.50) | 26 (33.33) | ||
| Total | 86 | 8 (100) | 78 (100) | ||
| Infiltration depth | 1.741 | 0.705 | |||
| T1 | 15 | 0 (0.00) | 15 (20.00) | ||
| T2 | 14 | 1 (16.67) | 13 (17.33) | ||
| T3 | 35 | 3 (50.00) | 32 (42.67) | ||
| T4 | 17 | 2 (33.33) | 15 (20.00) | ||
| Total | 81 | 6 (100) | 75 (100) | ||
| Differentiation degree | 1.995 | 0.565 | |||
| high-grade intraepithelial neoplasia | 7 | 0 (0.00) | 7 (8.64) | ||
| Poorly differentiated | 46 | 3 (42.86) | 43 (53.09) | ||
| Moderately and poorly differentiated | 23 | 2 (28.57) | 21 (25.93) | ||
| Moderately and well differentiated | 12 | 2 (28.57) | 10 (12.35) | ||
| Total | 88 | 7 (100) | 81 (100) |
The correlation analysis between the preoperative serum AFP positive rate and the clinicopathological features
As presented in Table 1, the preoperative serum AFP positive rate showed no significant association with gender, tumor size, peripheral lymph node metastasis, clinical stage, differentiation degree, infiltration degree, surgical methods, or Helicobacter pylori infection between the AFPGC and non-AFPGC patients. However, there was a significant correlation between the serum AFP positive rate and age, tumor sites, distant metastasis, and clinical stage. In detail, the positive rate of serum AFP in the ≤60 years old patients was significantly higher than it was in the >60 years old patients (19.1% vs 7.6%, P=0.044), and the incidence of AFPGC in the patients ≤60 years old was higher than it was in the non-AFPGC patients (56.3% vs 30.9%). Regarding the tumor locations, the positive rate of serum AFP in the patients with tumors in the upper third of the stomach was significantly higher than it was in the patients with tumors in the middle and distal thirds of the stomach (31.8% vs 10.9% vs 6.2%, P=0.008). Furthermore, the incidence of distant metastasis was significantly higher in the AFPGC patients than it was in the non-AFPGC patients (57.1% vs 26.5%), indicating that the serum AFP positive rate is significantly associated with distant metastasis (P=0.029). In addition, after we excluded the patients with incomplete clinical data, 13 patients with liver metastases or peritoneal metastases all had peripheral lymph node metastasis, so we speculated that the abdominal and liver metastasis pathways may occur through the lymph node metastasis.
Serum CEA and CA19-9 levels in the young and middle-aged patients
As shown in Table 1, the positive rate of serum AFP in the ≤60 years old patients was significantly higher than it was in the >60 years old patients. Therefore, it is necessary to explore whether there is a difference in the serum CEA and CA19-9 positive rates between the AFPGC and non-AFPGC patients. As shown in Table 2, in the 47 young and middle-aged patients, there was no significant difference in the serum CEA or CA19-9 levels, and the combined (CEA+CA19-9) positive rate between the AFPGC and non-AFPGC patients (P>0.05). The results may suggest that an examination of the serum CEA and CA19-9 levels or their combined (CEA+CA19-9) levels in the young and middle-aged patients is not conducive to an early diagnosis of AFPGC.
Table 2.
Serum CEA and CA19-9 levels in the 47 young and middle-aged patients
| Tumor marker | AFPGC (n=9) | Non-AFPGC (n=38) | Chi-square | P value |
|---|---|---|---|---|
| CEA | 1.489 | 0.222 | ||
| Positive | 4 (44.44%) | 7 (18.42%) | ||
| Negative | 5 (55.56%) | 31 (81.58%) | ||
| CA19-9 | 0.460 | 0.498 | ||
| Positive | 1 (11.11%) | 11 (28.95%) | ||
| Negative | 8 (88.89%) | 27 (71.05%) | ||
| CEA+CA19-9 | 2.452 | 0.117 | ||
| Positive | 6 (66.67%) | 12 (31.58%) | ||
| Negative | 3 (33.33%) | 26 (68.42%) |
Survival analysis
Although all the patients received follow-up, 59 patients (42.4%) were lost to the follow-up. As shown in Figure 2, the Kaplan-Meier survival analyses showed that the median overall survival (mOS) times of the non-AFPGC patents were significantly higher than they were among the AFPGC patients in the remaining 80 patients (55 months vs 40 months, P=0.042). Furthermore, in this study, four significant different characteristics including age, tumor location, serum AFP level, and distant metastasis in the AFPGC and non-AFPGC groups were selected for a survival analysis in the AFPGC patients. The Kaplan-Meier analysis and the log-rank test for the AFPGC patients showed that the serum AFP level (<100 ng/ml vs ≥100 ng/ml) is a prognostic factor for overall survival (P=0.041), but age, tumor location and distant metastasis are not (Table 3).
Figure 2.
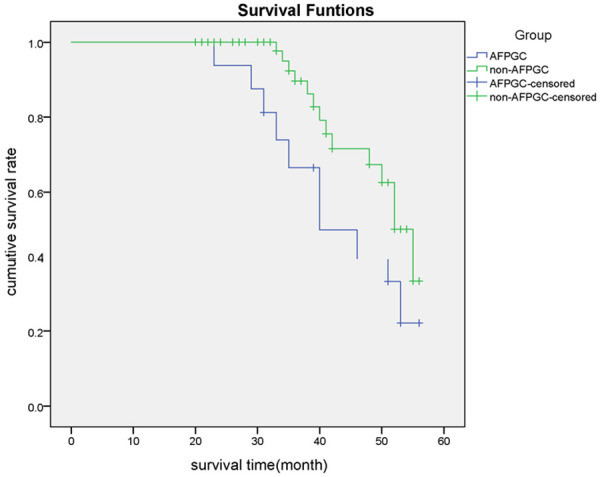
Comparison of the overall survival between the AFPGC and non-AFPGC patients.
Table 3.
A survival analysis of the AFPGC patients using the Kaplan-Meier method
| Characteristics | Median OS time Estimate (month) | Chi-square | P value |
|---|---|---|---|
| Tumor location | 0.490 | 0.484 | |
| Not upper third of stomach | 46 | ||
| Upper third of stomach | 40 | ||
| Age | 2.183 | 0.140 | |
| ≤60 | 40 | ||
| >60 | 33 | ||
| Serum AFP level | 4.189 | 0.041 | |
| <100 ng/ml | 51 | ||
| ≥100 ng/ml | 33 | ||
| Distant metastasis | 1.297 | 0.255 | |
| Yes | 35 | ||
| No | 40 |
Discussion
Gastric cancer is the fourth most common cancer in the world and the second most common cancer in China [11,12]. Among the various subtypes, AFPGC is recognized as one of the most aggressive, for it has a high propensity for liver metastasis and a subsequent poor prognosis compared with other GC subtypes, and its clinical features and prognosis are rarely reported.
In the present study AFPGC accounted for approximately 11.5% of all gastric cancers, a rate similar to those found in previous studies. Currently, there is controversy about the abnormal increase of AFP in GC patients. Some scholars believe that this type of tumor is a re-emergence of digestive system embryo development because the stomach and liver tissue are similar in their embryonic origin. Another view says that AFP is produced during the process of proliferation and regeneration of the liver cells around the liver metastasis sites of GC. Liver metastasis is a characteristic feature of AFPGC, occurring in 33%-72% of all AFPGC cases. Similarly, Liu et al. [13] suggested that there was a significantly higher incidence of vascular invasion, lymph node metastasis, and liver metastasis in the AFP positive group than in the negative group. Consistent with previous reports, AFPGC patients are more likely to have distant metastases, higher rates of peripheral lymph node metastasis, and advanced stages compared to the non-AFPGC patients in our study. These observations indicated that AFPGC has a more aggressive behavior than common GCs. Liu et al. [13] found that more than 40% of the AFPGC cases developed in the antrum of the stomach, suggesting the importance of measuring the AFP levels in GC at the antrum. However, He et al. [14] found that 31 cases (38.75%) had tumors in the upper third of the stomach among 80 AFPGC patients, but 22 cases (27.5%) had tumors in the distal third. Moreover, previous reports indicated that most AFPGC cases were elderly males and their gross types were mostly Borrmann II and Borrmann III [14]. However, in this study, the AFPGC cases were more concentrated in the younger patient group (≤60 years, 56.25%) and the upper third of the stomach group (43.75%). Importantly, this study suggests that young patients and patients with tumors occurring in the upper third of the stomach need more clinical attention and need to have their r serum AFP tested. Tumor markers, such as CEA and CA19-9, have been widely used for the diagnosis of different types of cancers, including gastric cancer [15]. Therefore, because it’s necessary to evaluate whether CEA and CA19-9 provide information about the early diagnosis of AFPGC, we compared the differences in the CEA and CA19-9 levels and their combined (CEA+CA19-9) levels between the AFPGC and the non-AFPGC patients. However, the results suggested that an examination of the serum CEA and CA19-9 levels or their combined (CEA+CA19-9) levels in young and middle-aged patients are not conducive to an early diagnosis of AFPGC. Thus, we suppose that an examination of the preoperative serum AFP could provide important clinical value in the proper early identification and treatment of AFPGC for young and middle-aged patients.
There is very limited information on the cellular or molecular characteristics of AFPGC that might explain this aggressive behavior. Some previous studies showed that the integrity of hepatocyte growth factor (HGF) receptor (c-Met) and ligand as HGF could regulate cell proliferation and migration. Amemiya et al. [16] found that c-Met is over-expressed more frequently in AFPGC than in stage-matched non-AFPGC. Moreover, the regulation of cancer cells by the HGF/c-Met system has been found in GC cell lines [17]. Kaji et al. [18] reported an inhibition of the growth and migration of the gastric cancer cell line when treated with an antisense c-Met oligonucleotide. These results suggest that the aggressive behavior of AFPGC may be associated with over-expressed c-Met. In this study, the main approach to AFPGC liver metastasis and peritoneal metastasis was analyzed from a clinical perspective, and the results showed that lymph node metastasis may be the main pathway.
AFPGC has been considered to have an unfavorable long-term survival rate, mainly due to the higher incidence of liver metastasis and lymphovascular invasion [6,7]. Lew et al. [19] suggested that the median survival length was shorter in the AFPGC group than in the non-AFPGC group (P=0.004). Consistent with previous reports, our results suggested that the mOS time was significantly lower in AFPGC group than in the non-AFPGC group (40 months vs 55 months, P=0.042). Furthermore, Tatli et al. [20] indicated that the AFP levels are a better indicator than CEA for the early response and diagnosis to ensure the early start of treatment and patient follow-up. In this study, the serum AFP level (<100 ng/ml vs ≥100 ng/ml) was found to be a prognostic factor for overall survival (P=0.041).
There are limitations to our study, as follows. First, as a single hospital-based design, inevitably, this study might have led to an uncertain amount of selection bias. Second, this was a retrospective analysis, and a well-designed randomized clinical trial should be conducted to avoid statistical bias in the future. Third, not all of the patients enrolled in our study were followed up due because contact was lost in some cases.
Conclusions
AFPGC is a rare subtype of GC with a high risk of distant metastasis and rapid progression. Its proper identification and treatment remain a challenge. In this study, we suggest that the real-time examination of serum AFP has great diagnostic and prognostic value for managing AFPGC, especially with young and middle-aged patients.
Acknowledgements
This study was financially supported by the National Natural Science Foundation of China (Nos. 31671468 and 81602593), the Academic promotion programme of Shandong First Medical University (No. 2019QL024), the Shandong Provincial Natural Science Foundation of China (Nos. ZR2016HM15, ZR2015HM018, ZR2017MH071, and ZR2018MH021), and the Shandong Provincial Postdoctoral Innovation Project (201702047).
Disclosure of conflict of interest
None.
References
- 1.Alpert E. Human alpha1-fetoprotein (AFP): developmental biology and clinical significance. Prog Liver Dis. 1976;5:337–349. [PubMed] [Google Scholar]
- 2.Gitlin D, Perricelli A, Gitlin GM. Synthesis of -fetoprotein by liver, yolk sac, and gastrointestinal tract of the human conceptus. Cancer Res. 1972;32:979–982. [PubMed] [Google Scholar]
- 3.El-Bahrawy M. Alpha-fetoprotein-producing non-germ cell tumours of the female genital tract. Eur J Cancer. 2010;46:1317–1322. doi: 10.1016/j.ejca.2010.01.028. [DOI] [PubMed] [Google Scholar]
- 4.Ishikura H, Fukasawa Y, Ogasawara K, Natori T, Tsukada Y, Aizawa M. An AFP-producing gastric carcinoma with features of hepatic differentiation. A case report. Cancer. 1985;56:840–848. doi: 10.1002/1097-0142(19850815)56:4<840::aid-cncr2820560423>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 5.Bourreille J, Metayer P, Sauger F, Matray F, Fondimare A. Existence of alpha feto protein during gastric-origin secondary cancer of the liver. Presse Med. 1970;78:1277–1278. [PubMed] [Google Scholar]
- 6.Li XD, Wu CP, Ji M, Wu J, Lu B, Shi HB, Jiang JT. Characteristic analysis of alpha-fetoprotein-producing gastric carcinoma in China. World J Surg Oncol. 2013;11:246. doi: 10.1186/1477-7819-11-246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shibata Y, Sato K, Kodama M, Nanjyo H. Alpha-fetoprotein-producing early gastric cancer of the remnant stomach: report of a case. Surg Today. 2007;37:995–999. doi: 10.1007/s00595-007-3501-0. [DOI] [PubMed] [Google Scholar]
- 8.He L, Ye F, Qu L, Wang D, Cui M, Wei C, Xing Y, Lee P, Suo J, Zhang DY. Protein profiling of alpha-fetoprotein producing gastric adenocarcinoma. Oncotarget. 2016;7:28448–28459. doi: 10.18632/oncotarget.8571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wang D, Li C, Xu Y, Xing Y, Qu L, Guo Y, Zhang Y, Sun X, Suo J. Clinicopathological characteristics and prognosis of alpha-fetoprotein positive gastric cancer in Chinese patients. Int J Clin Exp Pathol. 2015;8:6345–6355. [PMC free article] [PubMed] [Google Scholar]
- 10.Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17:1471–1474. doi: 10.1245/s10434-010-0985-4. [DOI] [PubMed] [Google Scholar]
- 11.Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. doi: 10.3322/caac.21262. [DOI] [PubMed] [Google Scholar]
- 12.Liu S, Feng F, Xu G, Liu Z, Tian Y, Guo M, Lian X, Cai L, Fan D, Zhang H. Clinicopathological features and prognosis of gastric cancer in young patients. BMC Cancer. 2016;16:478. doi: 10.1186/s12885-016-2489-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Liu X, Cheng Y, Sheng W, Lu H, Xu Y, Long Z, Zhu H, Wang Y. Clinicopathologic features and prognostic factors in alpha-fetoprotein-producing gastric cancers: analysis of 104 cases. J Surg Oncol. 2010;102:249–255. doi: 10.1002/jso.21624. [DOI] [PubMed] [Google Scholar]
- 14.He R, Yang Q, Dong X, Wang Y, Zhang W, Shen L, Zhang Z. Clinicopathologic and prognostic characteristics of alpha-fetoprotein-producing gastric cancer. Oncotarget. 2017;8:23817–23830. doi: 10.18632/oncotarget.15909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Huang ZB, Zhou X, Xu J, Du YP, Zhu W, Wang J, Shu YQ, Liu P. Prognostic value of preoperative serum tumor markers in gastric cancer. World J Clin Oncol. 2014;5:170–176. doi: 10.5306/wjco.v5.i2.170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Amemiya H, Kono K, Mori Y, Takahashi A, Ichihara F, Iizuka H, Sekikawa T, Matsumoto Y. High frequency of c-Met expression in gastric cancers producing alpha- fetoprotein. Oncology. 2000;59:145–151. doi: 10.1159/000012152. [DOI] [PubMed] [Google Scholar]
- 17.Ponzetto C, Giordano S, Peverali F, Della Valle G, Abate ML, Vaula G, Comoglio PM. c-met is amplified but not mutated in a cell line with an activated met tyrosine kinase. Oncogene. 1991;6:553–559. [PubMed] [Google Scholar]
- 18.Kaji M, Yonemura Y, Harada S, Liu X, Terada I, Yamamoto H. Participation of c-met in the progression of human gastric cancers: anti-c-met oligonucleotides inhibit proliferation or invasiveness of gastric cancer cells. Cancer Gene Ther. 1996;3:393–404. [PubMed] [Google Scholar]
- 19.Lew DH, Jung WT, Kim HJ, Min HJ, Ha CY, Kim HJ, Kim TH, Ko GH. Clinicopathological characteristics and prognosis of alpha-fetoprotein producing gastric cancer. Korean J Gastroenterol. 2013;62:327–335. doi: 10.4166/kjg.2013.62.6.327. [DOI] [PubMed] [Google Scholar]
- 20.Tatli AM, Urakci Z, Kalender ME, Arslan H, Tastekin D, Kaplan MA. Alpha-fetoprotein (AFP) elevation gastric adenocarcinoma and importance of AFP change in tumor response evaluation. Asian Pac J Cancer Prev. 2015;16:2003–2007. doi: 10.7314/apjcp.2015.16.5.2003. [DOI] [PubMed] [Google Scholar]