

Abstract
BACKGROUND:
Coronary artery calcium (CAC) is a guideline recommended cardiovascular disease (CVD) risk stratification tool that increases with age and is associated with non-cardiovascular disease outcomes including cancer. We sought to define the age-specific change in the association between CAC and cause-specific mortality.
METHODS:
The Coronary Artery Calcium Consortium includes 59,502 asymptomatic patients age 40–75 without known CVD. Age-stratified mortality rates and parametric survival regression modeling was performed to estimate the age-specific CAC score at which CVD and cancer mortality risk were equal.
RESULTS:
The mean age was 54±8 years (67% men) and there were 2,423 deaths over a mean 12±3 years follow-up. Among individuals with CAC = 0, cancer was the leading cause of death, with low CVD mortality rates for both younger (40–54 years) 0.2/1,000 person-years and older participants (65–75 years) 1.3/1,000 person-years. When CAC ≥400, CVD was consistently the leading cause of death among younger (71% of deaths) and older participants (56% of deaths). The CAC score at which CVD overtook cancer as the leading cause of death increased exponentially with age and was approximately 115 at age 50 and 380 at age 65.
CONCLUSIONS:
Regardless of age, when CAC = 0 cancer was the leading cause of death and the cardiovascular disease mortality rate was low. Our age-specific estimate for the CAC score at which CVD overtakes cancer mortality allows for a more precise approach to synergistic prediction and prevention strategies for CVD and cancer.
Keywords: Age, Competing risk, Coronary artery calcium, Risk prediction
INTRODUCTION
Despite a significant decline in the rate of cardiovascular mortality, cardiovascular disease remains the leading cause of death worldwide, with mortality due to cancer as the second leading cause of death.1 However, cancer is projected to become the leading cause of death in the United States by as early as 2020, and is already the leading cause of death in 9 European countries and 22 of 50 states within the United States.2,3 Furthermore, cancer is the leading cause of death for adults aged between 45 and 64 years, whereas cardiovascular disease remains the leading cause of death for adults older than 65 years of age.4
Coronary artery calcium score is a measure of an individual’s burden of subclinical coronary atherosclerosis and is highly predictive for cardiovascular disease beyond traditional risk factors.5,6 It is also associated with other chronic diseases, including cancer, chronic kidney disease, and dementia.7–9 The association of coronary artery calcium with both cardiovascular disease and noncardiovascular disease is attributable to the many shared risk factors.10–15 In particular, hypertension, diabetes, tobacco use, poor diet, and low physical activity are risk factors for both cardiovascular disease and cancer.11–13,16,17 The coronary artery calcium score has the unique ability to integrate lifetime risk factor exposure and genetic susceptibility, both of which lead to small and large vessel vascular injury and subsequent cardiovascular disease events. Accordingly, coronary artery calcium score can be used as a representative measure of an individual’s overall health status and biological age.18–20
Dual screening for cardiovascular disease and cancer has been identified as a paradigm changing approach for the prevention of the 2 leading causes of death worldwide, and we have previously demonstrated the utility of the coronary artery calcium score for risk stratifying the relationship between cardiovascular disease and cancer mortality.9,21 However, the prevalence of coronary artery calcium increases with increasing age, and the rates of cardiovascular disease and cancer mortality also change with age, increasing the complexity of risk prediction.4,22,23 Therefore, a better understanding of how the relationships between coronary artery calcium and cardiovascular disease and coronary artery calcium and cancer mortality changes as a function of age is imperative in order to improve risk prediction for the 2 leading causes of death. This is especially important between the ages of 40 and 75 years, the ages for which coronary artery calcium score is recommended by cardiovascular disease guidelines as a risk stratification indicator.24,25
To address this knowledge gap, we used data from the Coronary Artery Calcium Consortium to perform novel competing risk analyses for cardiovascular disease vs cancer mortality as a function of age in order to more precisely determine the coronary artery calcium score at which cardiovascular disease overtakes cancer as the most likely cause of death.
METHODS
Study Design
The Coronary Artery Calcium Consortium is a retrospective cohort that consists of 66,636 patients who had undergone a clinically indicated coronary artery calcium scan at 1 of 4 contributing centers.26 The coronary artery calcium scans were performed for cardiovascular disease risk stratification between 1991 through 2010 using patients who were asymptomatic and without known cardiovascular disease. Individuals aged < 40 years (n = 4855) and ≥ 75 years (n = 2279) were excluded, leaving a total of 59,502 individual in this analysis.
Coronary Artery Calcium Measurement
Non-contrast, cardiac-gated computed tomography scans were performed using standardized protocols and primarily performed using electron beam tomography, which provides equivalent results compared with multi-detector computed tomography.26,27 The results were reported in Agatston units, and for this analysis, coronary artery calcium scores were categorized as 0, 1–99, 100–399, or ≥400.
Risk Factors
Individual patient demographics and cardiovascular disease risk factors were obtained by each site from referral visit information, during a semi-structured interview at the time of the coronary artery calcium scan, or both. Cardiovascular disease risk factors were reported as the following categorical variables: hypertension, dyslipidemia, diabetes, and current smoking. Three of the sites recorded a family history of coronary heart disease if a first-degree relative had a coronary heart disease event, and one site (Columbus, Ohio) recorded a premature family history of coronary heart disease (<55 for males and <65 for females).
Follow-Up and Cause-Specific Mortality Ascertainment
The follow-up and death matching algorithm have been described in detail elsewhere.28 Briefly, the Social Security Administration Death Master File was searched through June 2014 to ascertain patients’ mortality status. Subsequently, death certificates were obtained from the National Death Index, and cause of death was classified into common groups (such as cardiovascular disease, coronary heart disease, and cancer) using the underlying (primary) cause of death based on the codes of the ninth and tenth revisions of the International Classification of Diseases. Noncardiovascular disease was defined as total mortality minus cardiovascular disease mortality. The proportions of cardiovascular disease and cancer deaths in the Coronary Artery Calcium Consortium are similar to contemporary data from the United States Centers for Disease Control and American Cancer Society mortality data.29,30
Statistical Analysis
Total mortality and cause-specific mortality rates were calculated per 1000 person-years follow-up within each coronary artery calcium score and age group. Cox proportional hazard models overestimate the risk relationship when there are competing risks.31–34 Therefore, in order to more accurately account for the competing risk of cardiovascular disease and cancer mortality, we performed Fine and Gray subdistribution hazard modeling, which takes into account competing risks.35 These models were adjusted for age, sex, hypertension, hyperlipidemia, smoking, diabetes, and a family history of coronary heart disease.
We calculated the rates of incident cardiovascular disease and cancer as a function of coronary artery calcium score within the age groups fitted with a polynomial function. In order to more accurately describe the coronary artery calcium score at which cardiovascular disease mortality overtakes cancer mortality, we developed a calculator to determine the age-specific coronary artery calcium score at which the risk of death from cardiovascular disease and cancer were equal using parametric survival regression modeling and the log (coronary artery calcium score + 1). After equating the risk equations for cardiovascular disease and cancer, and solving for ln (coronary artery calcium score + 1), we obtained the following function for the age-specific coronary artery calcium score at which cardiovascular disease vs cancer mortality risk are equal, which we have graphically displayed and also used to create an online calculator.
RESULTS
The cohort had a mean age of 54.9 (±8.5) years. Sixty-six percent of the participants were male, and 89% were Caucasian. The percentage of participants with hypertension, hyperlipidemia, and diabetes increased with age, as did the mean atherosclerotic cardiovascular disease risk score (Table 1). Among individuals aged 40–54 years, only 6.7% had an atherosclerotic cardiovascular disease risk score ≥ 7.5%, whereas 43.7% had prevalent coronary artery calcium. Conversely, among individuals aged 65–75 years, 89.5% had an atherosclerotic cardiovascular disease risk score ≥ 7.5%, and 81.4% had prevalent coronary artery calcium. The median coronary artery calcium score for individuals aged 40–54 years was 0 Agatston units, whereas the median coronary artery calcium score for individuals aged 65–75 years was 110 Agatston units.
Table 1.
Participant Characteristics*
| Characteristic | Total Cohort (n = 59,502) | 40–54 Years (n = 31,033) | 55–64 Years (n = 19,747) | 65–75 Years (n = 8722) |
|---|---|---|---|---|
| Age | 54.9 (8.5) | 48.3 (4.2) | 59.2 (2.8) | 69.1 (2.9) |
| Male | 66.5 | 70.7 | 62.6 | 60.0 |
| Caucasian | 89.4 | 88.8 | 90.2 | 90.0 |
| Hypertension | 31.1 | 24.2 | 35.7 | 45.8 |
| Hyperlipidemia | 54.7 | 51.6 | 56.9 | 60.3 |
| Diabetes | 6.8 | 4.9 | 7.8 | 10.8 |
| Current smoking | 9.5 | 10.5 | 9.1 | 7.7 |
| Family history of CHD | 45.8 | 47.7 | 44.7 | 41.7 |
| 10-Year ASCVD risk | 6.8 | 3.3 | 7.9 | 17.0 |
| ASCVD category | ||||
| < 7.5% | 68.8 | 93.3 | 55.8 | 10.6 |
| 7.5%−19% | 26.0 | 6.5 | 41.5 | 60.1 |
| ≥ 20% | 5.3 | 0.2 | 2.7 | 29.4 |
| CAC >0 | 56.7 | 43.7 | 66.2 | 81.4 |
| CAC score† | 4 (0–96) | 0 (0–22) | 20 (0–163) | 110 (8–461) |
ASCVD = atherosclerotic cardiovascular disease; CAC = coronary artery calcium.
Values reported as mean (standard deviation) or percent unless otherwise noted.
median (interquartile range).
Over a mean follow-up of 12.3 years there were 2423 total deaths with 671 deaths due to cardiovascular disease (358 of those due to coronary heart disease) and 954 deaths due to cancer. Among individuals who died from cardiovascular disease, middle-aged adults (55–65 years) had a median coronary artery calcium score of 209, whereas older individuals (65–75 years) had a median coronary artery calcium score of 376. Among individuals who died from cancer, middle-aged adults had a median coronary artery calcium score of 44, whereas older adults had a median coronary artery calcium score of 140.
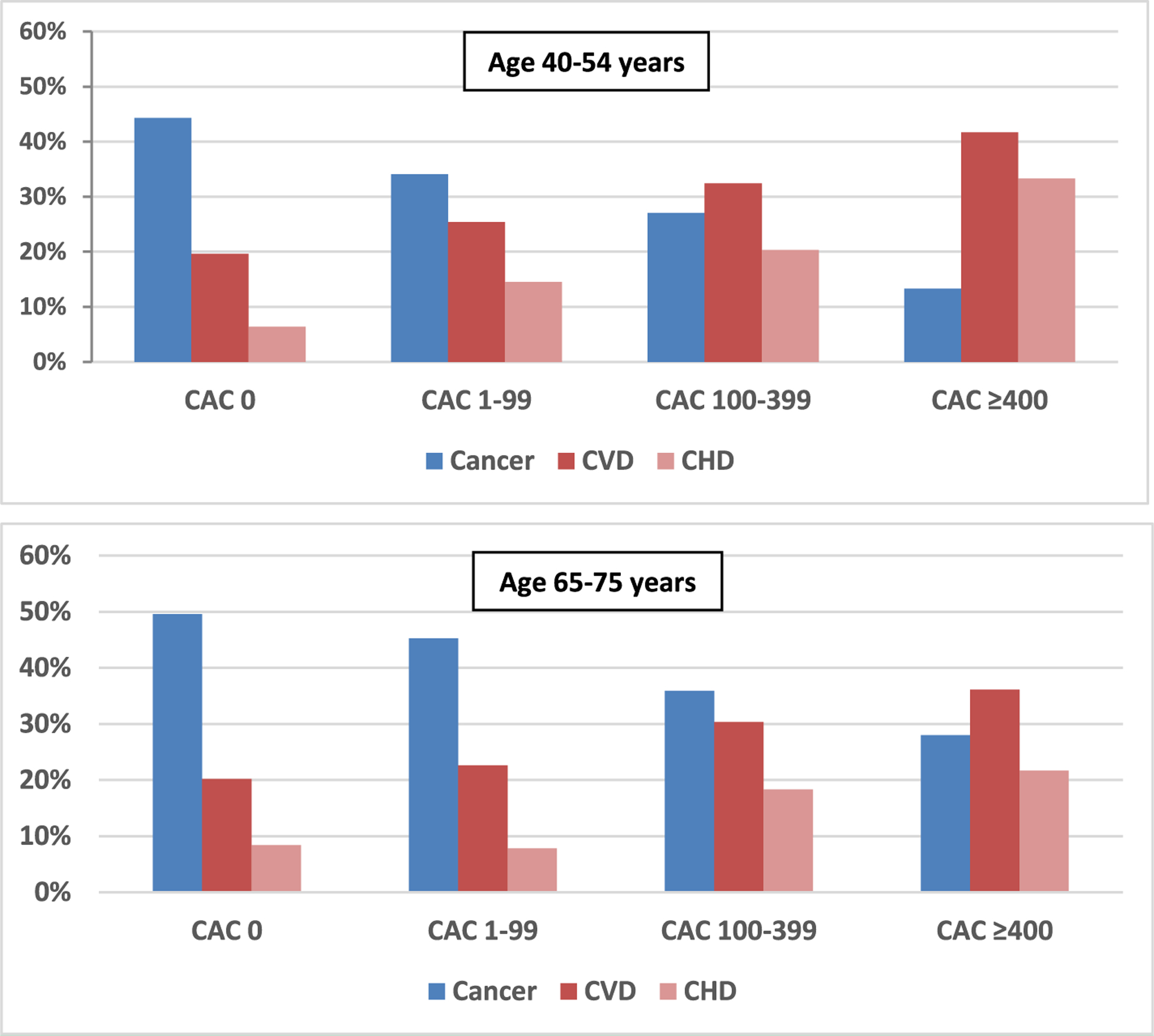
The rate of cardiovascular disease mortality increased with increasing coronary artery calcium score for all age groups (Table 2). However, the incidence rate of cancer mortality was relatively unchanged with increasing coronary artery calcium score for individuals aged < 55 years, but increased with an increasing coronary artery calcium score for individuals aged ≥ 55 years. For younger and older individuals, the proportion of death due to cardiovascular disease increased with coronary artery calcium, whereas the proportion of death due to cancer decreased with increasing coronary artery calcium score (Figure 1). The proportion of deaths due to cardiovascular disease was greater than deaths due to cancer when the coronary artery calcium score was ≥100 for younger individuals (40–54 years) and when the coronary artery calcium score was ≥ 400 for older individuals. When the coronary artery calcium score was 0, the proportion of deaths due to cardiovascular disease was similarly low for both younger and older individuals (Figure 2). When the coronary artery calcium score was ≥ 400, the proportion of deaths due to cardiovascular disease was greater than that of cancer for all age groups, but decreased with increasing age. The cancer mortality rate was relatively constant with increasing coronary artery calcium scores for younger individuals, and increased gradually for older individuals, whereas the rate of cardiovascular disease consistently increased with coronary artery calcium score for younger and older individuals (Figure 3).
Table 2.
Cause-Specific Mortality Rate per 1000 Person-Years, Stratified by Coronary Artery Calcium and Age
| CAC = 0 | CAC 1–99 | CAC 100–399 | CAC ≥ 400 | |
|---|---|---|---|---|
| Total | ||||
| 40–54 years | 1.0 | 1.4 | 2.2 | 4.1 |
| 55–64 years | 2.3 | 3.2 | 4.4 | 7.7 |
| 65–75 years | 6.2 | 7.5 | 10.2 | 15.0 |
| Coronary heart disease | ||||
| 40–54 years | 0.1 | 0.2 | 0.4 | 1.4 |
| 55–64 years | 0.2 | 0.3 | 0.6 | 1.7 |
| 65–75 years | 0.5 | 0.7 | 1.9 | 3.3 |
| Cardiovascular disease | ||||
| 40–54 years | 0.2 | 0.4 | 0.7 | 1.7 |
| 55–64 years | 0.4 | 0.7 | 1.3 | 2.9 |
| 65–75 years | 1.3 | 1.7 | 3.1 | 5.4 |
| Noncardiovascular disease | ||||
| 40–54 years | 0.8 | 1.0 | 1.5 | 2.4 |
| 55–64 years | 1.9 | 2.5 | 3.1 | 4.9 |
| 65–75 years | 5.0 | 5.8 | 7.1 | 9.6 |
| Cancer | ||||
| 40–54 years | 0.4 | 0.5 | 0.6 | 0.5 |
| 55–64 years | 1.4 | 1.5 | 1.9 | 2.7 |
| 65–75 years | 3.1 | 3.4 | 3.7 | 4.2 |
CAC = coronary artery calcium.
Figure 1.
Proportions of deaths due to cancer, cardiovascular disease, coronary heart disease, and non-coronary heart disease cardiovascular disease, stratified by age. CAC = coronary artery calcium; CHD = coronary heart disease CVD = cardiovascular disease.
Figure 2.

Proportions of cardiovascular and cancer deaths by coronary artery calcium group and age group. CAC = coronary artery calcium; CHD = coronary heart disease CVD = cardiovascular disease.
Figure 3.

Cardiovascular and cancer mortality rates per 1000 person-years follow-up as a function of coronary artery calcium score, stratified by age groups. CAC = coronary artery calcium; CHD = coronary heart disease CVD = cardiovascular disease.
Using the function we derived to calculate the age-specific coronary artery calcium score at which cardiovascular disease and cancer risk are equal, we obtained the following equation for our cardiovascular disease vs cancer mortality risk calculator:
Using this calculator, the coronary artery calcium score at which cardiovascular disease overtook cancer as the leading cause of death increased exponentially as a function of age corresponding to a coronary artery calcium score of approximately 115 at age 50 compared with 570 at age 70 (Figure 4).
Figure 4.

Coronary artery calcium score at which the rate of cardiovascaular disease and cancer mortality are equal.
Fine and Gray subdistribution hazard competing risk analyses showed that any coronary artery calcium score was significantly associated with cardiovascular disease across age groups. The strength of the association was attenuated with age, but remain significant for individuals 65–75 years old with coronary artery calcium scores ≥100 (Table 3). Overall, a coronary artery calcium score ≥ 400 was associated with a significantly increased competing risk for cancer (subdistribution hazard ratio 1.32, 95% confidence interval 1.07–1.64), although this was largely driven by a statistically significant result for individuals aged 55–64 years.
Table 3.
Fine and Gray Subdistribution Hazard of Cause-Specific Mortality by Coronary Artery Calcium Score and Age
| CAC = 0 | CAC 1–99 | CAC 100–399 | CAC ≥ 400 | |
|---|---|---|---|---|
| Coronary heart disease | ||||
| 40–54 years | Reference | 2.44(1.25–4.76) | 4.48 (2.06–9.72) | 11.78 (5.58–24.87) |
| 55–64 years | Reference | 1.40 (0.74–2.67) | 2.48 (1.28–4.78) | 6.12 (3.32–11.29) |
| 65–75 years | Reference | 0.94 (0.43–2.06) | 2.68 (1.31–5.50) | 3.76 (1.84–7.68) |
| Overall | Reference | 1.59 (1.06–2.39) | 3.35 (2.19–2.40) | 5.69 (3.78–8.58) |
| Cardiovascular disease | ||||
| 40–54 years | Reference | 1.55 (1.00–2.40) | 2.80 (1.64–4.77) | 5.90 (3.37–10.32) |
| 55–64 years | Reference | 1.66 (1.06–2.59) | 2.94 (1.84–4.67) | 5.70 (3.60–9.02) |
| 65–75 years | Reference | 1.22 (0.75–2.00) | 2.06 (1.27–3.33) | 3.12 (1.93–5.02) |
| Overall | Reference | 1.50 (1.15–1.95) | 2.59 (1.96–3.42) | 4.46 (3.36–5.93) |
| Noncardiovascular disease | ||||
| 40–54 years | Reference | 1.25 (0.99–1.58) | 1.64 (1.17–2.29) | 2.40 (1.62–3.53) |
| 55–64 years | Reference | 1.22 (0.98–1.52) | 1.44 (1.12–1.84) | 2.09 (1.63–2.67) |
| 65–75 years | Reference | 1.10 (0.86–1.42) | 1.27 (0.98–1.64) | 1.56 (1.20–2.01) |
| Overall | Reference | 1.20 (1.05–1.37) | 1.43 (1.23–1.66) | 1.90 (1.62–2.22) |
| Cancer | ||||
| Age 40–54 | Reference | 1.06 (0.75–1.48) | 1.21 (0.81–2.02) | 1.00 (0.48–2.10) |
| Age 55–64 | Reference | 1.00 (0.76–1.31) | 1.19 (0.87–1.61) | 1.58 (1.16–2.16) |
| Age 65–75 | Reference | 1.02 (0.73–1.41) | 1.03 (0.73–1.44) | 1.07 (0.75–1.51) |
| Overall | Reference | 1.03 (0.87–1.23) | 1.15 (0.94–1.41) | 1.32 (1.07–1.64) |
CAC = coronary artery calcium.
Adjusted for age, gender, hypertension, hyperlipidemia, smoking, diabetes, and family history of coronary heart disease.
DISCUSSION
Using cause-specific mortality data from the Coronary Artery Calcium Consortium, we describe how age impacts the relationship of coronary artery calcium with the 2 leading causes of death worldwide, cardiovascular disease and cancer. Although coronary artery calcium score is most strongly predictive of coronary heart disease and cardiovascular disease, its significant association with cancer mortality is attributable to the ability of the coronary artery calcium score to integrate the lifetime exposure to risk factors, many of which are shared between cardiovascular disease and cancer.7,9 However, although the prevalence of coronary artery calcium increases with age, the ratio of cancer to cardiovascular disease mortality is inversely related to age.4 To our knowledge, our results are the first to 1) demonstrate the utility of coronary artery calcium score for the synergistic risk stratification of cardiovascular disease and cancer mortality risk across the adult life course and 2) provide an estimator for the coronary artery calcium score at which cardiovascular disease mortality overtakes cancer as a function of age, which we demonstrate has an exponential relationship.
Prior reports have shown that a coronary artery calcium score of 0 is associated with a very low risk for incident cardiovascular disease events, but the association with cardiovascular disease mortality and cause-specific mortality data were unknown.36–38 Our results demonstrated that when the coronary artery calcium score is 0, regardless of age, cancer is the leading cause of death and the rate of cardiovascular disease mortality is low. We also showed that in young individuals 40–54 years of age, a coronary artery calcium score of 0 was associated with a very low absolute cancer and cardiovascular disease mortality rate, which is consistent with prior total mortality data. In our study, we observed that when the coronary artery calcium score was ≥ 400, there was a corresponding, but inverse relationship with a greater proportion of deaths due to cardiovascular disease compared with cancer across all age groups, even among individuals aged 65–75.
These results also underscore previous observations demonstrating that the prevalence of any coronary artery calcium at a young age (40–54 years) is premature, and even a low absolute coronary artery calcium score of 1–99 is associated with a greater than twofold relative increased risk of cardiovascular disease.38–40 However, we also demonstrated that among these young individuals with premature coronary artery calcium scores between 1 and 99, the absolute mortality rate was slightly higher for cancer (0.5/1,000 person-years) than for cardiovascular disease (0.4/1,000 person-years). This suggests that although cardiovascular disease preventive therapies to reduce the long-term cardiovascular disease risk for young persons with even minimal premature coronary artery calcium are important, age- and patient-specific cancer screening and preventive strategies should also be strongly emphasized.
Although an increasing coronary artery calcium score in this young age group was associated with a significantly increased rate of cardiovascular disease mortality, the cancer mortality rate was nearly the same for young individuals regardless of their coronary artery calcium score. However, for individuals aged ≥ 55 years, the mortality rate increased for both cancer and cardiovascular disease with increasing coronary artery calcium. This lack of association between the absolute cancer mortality rate and coronary artery calcium in young individuals may be attributable to a greater genetic contribution for cancer development at younger ages and a greater diet and lifestyle contribution at older ages. For instance, lung and bronchus cancer accounts for approximately 24% of cancer deaths for individuals aged 45–54 years compared with 34% for individuals aged 65–74 years.41
Our results have a number of implications for the development of cardiovascular disease primary prevention and population-based prevention strategies. This study adds further supporting evidence that a coronary artery calcium score of 0 is a marker for not only ideal cardiovascular disease health, but also for ideal overall health; regardless of age, individuals with a coronary artery calcium score of 0 were at a very low risk for cancer mortality and total mortality as well as for cardiovascular disease.
We also demonstrated that although any amount of coronary artery calcium is strongly associated with an increased risk of cardiovascular disease, there is an exponential relationship between age and coronary artery calcium score and risk of cardiovascular disease mortality. Furthermore, we developed a calculator to determine the age-specific coronary artery calcium score at which cardiovascular disease mortality overtakes cancer mortality as the leading cause of death, which has implications for the development of guidelines and prevention strategies. Therefore, these results add further evidence supporting the use of the coronary artery calcium score as a synergistic risk stratification indicator across the adult lifespan for both cardiovascular disease and cancer, and are in keeping with previously identified key public health priorities.21
Limitations of this analysis include that nearly all participants in the Coronary Artery Calcium Consortium were Caucasian, and about two-thirds of participants were male. For very young individuals (ie, < 40 years old) we expect that any coronary artery calcium (even a score of 1) would be associated with a higher risk of cardiovascular disease compared with cancer. Therefore, the utility of our age-specific coronary artery calcium score estimate at which the risk of cardiovascular disease and cancer are equal may be limited at very young ages, where the curve appears to flatten out before reaching a coronary artery calcium score of 0. A small number of deaths may not have been included in the data from the Coronary Artery Calcium Consortium, because our death ascertainment algorithm prioritized specificity over sensitivity when searching the national death database. In addition, there are well known limitations to the use of death certificates for ascertainment of cause of death. However, the death certificate data used for this analysis is the same data used by the Centers for Disease Control to track United States mortality trends and death certificates are also used to track worldwide mortality trends. Although we do not have information on downstream testing or procedures, an increase in cardiovascular disease medications/procedures among individuals with a higher coronary artery calcium score would bias our results toward the null hypothesis, and only coronary artery bypass surgery has been shown to reduce mortality.
CONCLUSIONS
Our study demonstrated that regardless of age, individuals with a coronary artery calcium score of 0 have a very low rate of cardiovascular disease mortality. In addition, for the first time, we also provide an age-based estimate of the coronary artery calcium score at which cardiovascular disease overtakes cancer as the leading cause of death. These results open the door to a synergistic cardiovascular disease and cancer prevention strategy for adults with an intermediate age-based coronary artery calcium score that may significantly reduce both cardiovascular disease and cancer mortality rates, the 2 leading causes of death worldwide.
CLINICAL SIGNIFICANCE.
Coronary artery calcium score can provide synergistic information for the prediction of both cardiovascular disease and cancer.
When the coronary artery calcium score was 0, cancer was the leading cause of death and the cardiovascular disease mortality rate was very low for both younger and older adults.
The coronary artery calcium score at which cardiovascular disease overtakes cancer as the leading cause of death increased exponentially with age.
Funding:
SPW was supported by the American Heart Association Mentored Clinical and Population Research Award (17MCPRP33660247) and the PJ Schafer Memorial Foundation.
Footnotes
Conflict of Interest: LJS has received grant support from the Antinori Foundation. MJ Budoff has received grant support from GE Healthcare. CHM has received grant support from Bristol Myers Squibb and travel support from DAVA Oncology. She also reports being a consultant for McGraw-Hill. All other authors have nothing to disclose.
References
- 1.Global Status Report on Noncommunicable Diseases. Geneva, Switzerland: World Health Organization; 2014. [Google Scholar]
- 2.Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. 2016;37(42):3232–45. [DOI] [PubMed] [Google Scholar]
- 3.Weir HK AR, Coleman King SM, Soman A, et al. Heart disease and cancer deaths - trends and projections in the United States, 1969–2020. Prev Chronic Dis. 2016;13:160211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Heron M Deaths: leading causes for 2016. Natl Vital Stat Rep. 2018;67(6). [PubMed] [Google Scholar]
- 5.Detrano R, Guerci AD, Carr JJ, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13):1336–45. [DOI] [PubMed] [Google Scholar]
- 6.Yeboah J, McClelland RL, Polonsky TS, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals. JAMA. 2012;308(8):788–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Handy CE, Desai CS, Dardari ZA, et al. The association of coronary artery calcium with noncardiovascular disease the Multi-Ethnic Study of Atherosclerosis. JACC Cardiovasc Imaging. 2016;9(5):568–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fujiyoshi A, Jacobs DR, Fitzpatrick AL, et al. Coronary artery calcium and risk of dementia in MESA (Multi-Ethnic Study of Atherosclerosis). Circ Cardiovasc Imaging 2017;10(5). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Whelton SP, Al Rifai M, Dardari Z, et al. Coronary artery calcium and the competing long-term risk of cardiovascular vs cancer mortality: the CAC Consortium. Eur Heart J Cardiovasc Imaging 2019;20 (4):389–95. [DOI] [PubMed] [Google Scholar]
- 10.Eyre H, Kahn R, Robertson RM, et al. Preventing cancer, cardiovascular disease, and diabetes: a common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Circulation. 2004;109(25):3244–55. [DOI] [PubMed] [Google Scholar]
- 11.Carter BD, Abnet CC, Feskanich D, et al. Smoking and mortality - beyond established causes. N Engl J Med. 2015;372(7):631–40. [DOI] [PubMed] [Google Scholar]
- 12.Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of US adults. N Engl J Med. 2003;348(17):1625–38. [DOI] [PubMed] [Google Scholar]
- 13.Giovannucci E, Harlan DM, Archer MC, et al. Diabetes and cancer: a consensus report. Diabetes Care. 2010;33(7):1674–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schmid D, Leitzmann MF. Television viewing and time spent sedentary in relation to cancer risk: a meta-analysis. J Natl Cancer Inst 2014;106(7). [DOI] [PubMed] [Google Scholar]
- 15.Whelton SP, Al Rifai M, Dardari Z, et al. Coronary artery calcium and the competing long-term risk of cardiovascular vs. cancer mortality: the CAC Consortium. Eur Heart J Cardiovasc Imaging 2019;20 (4):389–95. [DOI] [PubMed] [Google Scholar]
- 16.Eyre H, Kahn R, Robertson RM, et al. Preventing cancer, cardiovascular disease, and diabetes: a common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Stroke. 2004;35(8):1999–2010. [DOI] [PubMed] [Google Scholar]
- 17.Schmid D, Leitzmann MF. Television viewing and time spent sedentary in relation to cancer risk: a meta-analysis. Asia-Pacific Journal of Clinical Oncology. 2014;10:244–5. [DOI] [PubMed] [Google Scholar]
- 18.McClelland RL, Nasir K, Budoff M, Blumenthal RS, Kronmal RA. Arterial age as a function of coronary artery calcium (from the Multi-Ethnic Study of Atherosclerosis [MESA]). Am J Cardiol. 2009;103 (1):59–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shaw LJ, Raggi P, Berman DS, Callister TQ. Coronary artery calcium as a measure of biologic age. Atherosclerosis. 2006;188(1):112–9. [DOI] [PubMed] [Google Scholar]
- 20.Whelton S, Silverman M, McEvoy J, et al. The long-term non-development of coronary artery calcium as a marker of healthy arterial aging in the Multi Ethnic Study of Atherosclerosis (MESA). J Am Coll Cardiol. 2014;63(12):A1388. [Google Scholar]
- 21.Handy CE, Quispe R, Pinto X, et al. Synergistic opportunities in the interplay between cancer screening and cardiovascular disease risk assessment: together we are stronger. Circulation. 2018;138(7):727–34. [DOI] [PubMed] [Google Scholar]
- 22.McClelland RL, Chung HJ, Detrano R, Post W, Kronmal RA. Distribution of coronary artery calcium by race, gender, and age: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2006;113(1):30–7. [DOI] [PubMed] [Google Scholar]
- 23.Nakanishi R, Li D, Blaha MJ, et al. All-cause mortality by age and gender based on coronary artery calcium scores. Eur Heart J Cardiovasc Imaging 2016;17(11):1305–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Catapano AL, Graham I, De Backer G, et al. 2016 ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J. 2016;37 (39):2999–3058. [DOI] [PubMed] [Google Scholar]
- 25.Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2019;73(24):e285–350. [DOI] [PubMed] [Google Scholar]
- 26.Blaha MJ, Whelton SP, Al Rifai M, et al. Rationale and design of the coronary artery calcium consortium: a multicenter cohort study. Journal of Cardiovascular Computed Tomography. 2017;11(1):54–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Mao SS, Pal RS, McKay CR, et al. Comparison of coronary artery calcium scores between electron beam computed tomography and 64-multidetector computed tomographic scanner. J Comput Assist Tomogr. 2009;33(2):175–8. [DOI] [PubMed] [Google Scholar]
- 28.Al-Mallah MH, Keteyian SJ, Brawner CA, Whelton S, Blaha MJ. Rationale and design of the Henry Ford Exercise Testing Project (The FIT Project). Clin Cardiol. 2014;37(8):456–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Heron M Deaths: leading causes for 2014. Natl Vital Stat Rep. 2015;65(5):1–96. [PubMed] [Google Scholar]
- 30.American Cancer Society. Cancer facts and figures. 2014. Atlanta: American Cancer Society; 2014. https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2014.html. [Google Scholar]
- 31.Austin PC, Lee DS, Fine JP. Introduction to the analysis of survival data in the presence of competing risks. Circulation. 2016;133 (6):601–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 1999;18(6):695–706. [DOI] [PubMed] [Google Scholar]
- 33.Lau B, Cole SR, Gange SJ. Competing risk regression models for epidemiologic data. Am J Epidemiol. 2009;170(2):244–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kim HT. Cumulative incidence in competing risks data and competing risks regression analysis. Clin Cancer Res. 2007;13(2): 559–65. [DOI] [PubMed] [Google Scholar]
- 35.Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94(446):496–509. [Google Scholar]
- 36.Blaha MJ, Cainzos-Achirica M, Greenland P, et al. Role of coronary artery calcium score of zero and other negative risk markers for cardiovascular disease the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2016;133(9):849–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Blaha M, Budoff MJ, Shaw LJ, et al. Absence of coronary artery calcification and all-cause mortality. JACC Cardiovasc Imaging. 2009;2 (6):692–700. [DOI] [PubMed] [Google Scholar]
- 38.Budoff MJ, McClelland RL, Nasir K, et al. Cardiovascular events with absent or minimal coronary calcification: the Multi-Ethnic Study of Atherosclerosis (MESA). Am Heart J. 2009;158(4):554–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Tota-Maharaj R, Blaha MJ, Blankstein R, et al. Association of coronary artery calcium and coronary heart disease events in young and elderly participants in the Multi-Ethnic Study of Atherosclerosis: a secondary analysis of a prospective, population-based cohort. Mayo Clin Proc. 2014;89(10):1350–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Carr JJ, Jacobs DR Jr, Terry JG, et al. Association of coronary artery calcium in adults aged 32 to 46 years with incident coronary heart disease and death. JAMA Cardiol. 2017;2(4):391–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Howlader N, Noone AM, Krapcho M, et al. (eds). SEER Cancer Statistics Review, 1975–2012, National Cancer Institute. Bethesda, MD: https://seer.cancer.gov/archive/csr/1975_2012/. Accessed July 22, 2019. [Google Scholar]