

Late 2019, a novel coronavirus causing coronavirus disease (COVID-19) emerged in Wuhan, China, and rapidly spread globally.1 Iran reported the first confirmed cases of COVID-19 on 19 February 2020 in Qom2 which is located about 150 km to the south of Tehran. The outbreak then quickly moved to other parts of Iran. The aim of this study was to describe the epidemic curve and estimate the reproduction number of COVID-19 in Iran. For this purpose, the SIR (Susceptible–Infected–Removed)3 epidemic model was used to fit the reported data.
The differential equations of the SIR model are given as:
 |
(1) |
where  ,
,  and
and  are the number of susceptible, infected and removed people.
are the number of susceptible, infected and removed people.  is the infection rate, and
is the infection rate, and  is the remove rate which is the inverse of infectious period. The basic reproduction number,
is the remove rate which is the inverse of infectious period. The basic reproduction number,  , is the average number of the secondary individuals in a complete susceptible population infected by a single infected person during its spreading life. When
, is the average number of the secondary individuals in a complete susceptible population infected by a single infected person during its spreading life. When  , the virus spreads through the population, and when
, the virus spreads through the population, and when  the outbreak will stop due to decreasing the number of new cases.
the outbreak will stop due to decreasing the number of new cases.  can be calculated as the following:
can be calculated as the following:
 |
(2) |
N is assumed to be the population of Iran 81 800 269 in 2018 (https://data.worldbank.org).
We model epidemic spreading in the period from 21 February 2020 to 2 May 2020 using reported data by MoHME.2 The Runge–Kutta method is used to solve the ordinary differential equations in MATLAB. As shown in Figure 1, we estimated the  to be 4.86 in the first week of the outbreak which is significantly higher than that reported for many other regions.4 Iran suffered from inadequate testing kits in the early stages and had to conduct tests in a few laboratories in Tehran. Hence obtaining the test results was delayed. However, as of 28 March 2020, 90 labs were capable of conducting tests every day.5
to be 4.86 in the first week of the outbreak which is significantly higher than that reported for many other regions.4 Iran suffered from inadequate testing kits in the early stages and had to conduct tests in a few laboratories in Tehran. Hence obtaining the test results was delayed. However, as of 28 March 2020, 90 labs were capable of conducting tests every day.5
Figure 1.
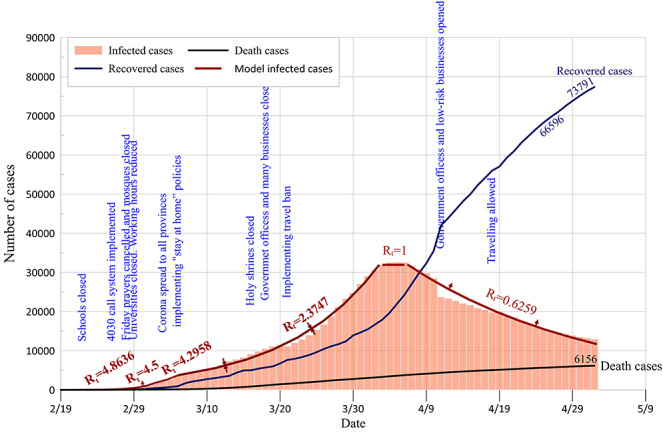
Epidemic curve and estimated reproduction number of COVID-19 in Iran during different time periods
In response to the exponential increase in cases, the Iranian government closed all schools in the first week. By the end of the first week, Friday prayers were cancelled and all mosques were closed. In the second week, universities were closed and the government reduced the working hours. However, by the end of the second week, the virus spread to all provinces in Iran. The government then implemented ‘stay at home’ policies. Social network users created campaigns and public messaging to stay at home and do social distancing. In the second week,  reduced from 4.86 to 4.5 and then to 4.29 in the third week. Figure 1 illustrated the decline of the effective reproduction number over time as increasingly nonpharmaceutical interventions. The effective reproduction number further decreased to 2.37 between 6 March 2020 and 3 April 2020, most likely due to increasingly stringent measures for social distancing, and ‘stay at home’ policies, but also the enforcement of quarantine of household and other contacts of confirmed cases.
reduced from 4.86 to 4.5 and then to 4.29 in the third week. Figure 1 illustrated the decline of the effective reproduction number over time as increasingly nonpharmaceutical interventions. The effective reproduction number further decreased to 2.37 between 6 March 2020 and 3 April 2020, most likely due to increasingly stringent measures for social distancing, and ‘stay at home’ policies, but also the enforcement of quarantine of household and other contacts of confirmed cases.
As Nowruz, Persian New Year, arrived on 20 March 2020, many businesses as well as government offices closed, and the government restricted travelling between provinces for almost 4 weeks. As a result, as shown in Figure 1, the effective reproduction number further declined to 1 between 4 April and 6 April 2020. It can be seen that the reproduction number has been less than 1 since 7 April 2020, indicating that the epidemic has been curbed.
Previous studies showed that the basic reproduction number of COVID-19 was estimated to range from 2.24 to 3.58 during the early outbreak in Wuhan City, China.6 In Iran, the reproduction number was likely higher due to high social mixing during social events. The beginning of the outbreak coincided with the beginning of the new semester for universities when students travelled from their hometowns to their universities. Many students live in dormitories where the risk of spreading was high due to close social intermixing.
The closure of universities, discontinuation of religious gatherings and prohibition of social events and increasingly additional public health interventions including contact tracing, quarantine and travel restrictions within the country led to a decline of the effective reproduction number to below 1. Unless mitigation strategies continue, COVID-19 will resurge in Iran. Social distancing, active case detection, prompt isolation of all cases, contact tracing and quarantining of contacts will need to be maintained until an effective and safe vaccine becomes available. COVID-19 poses a tremendous burden on Iran’s health care system, economy and society, especially at a time of US sanctions.7
Authors’ contributions
E.S. conducted the simulation experiments, analysed the results and wrote the manuscript; S.S. collected the reported case data and revised and edited the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no specific funding for this work.
Conflict of interest
The authors declare that they have no competing interests.
References
- 1. Bogoch II, Watts A, Thomas-Bachli A, Huber C, Kraemer MUG, Khan K. Potential for global spread of a novel coronavirus from China. J Travel Med 2020; 27:1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ministry of Health and Medical Education (MoHME) http://ird.behdasht.gov.ir/.
- 3. Kermack WO, McKendrick AG. A contributions to the mathematical theory of epidemics. Proc R Soc Lond 1927; 115:700–21. [Google Scholar]
- 4. Liu Y, Gayle A, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med 2020; 27:4–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Raoofi A, Takian A, Akbari Sari A, Olyaeemanesh A, Haghighi H, Aarabi M. COVID-19 pandemic and comparative health policy learning in Iran. Arch Iran Med 2020; 23:220–34. [DOI] [PubMed] [Google Scholar]
- 6. Zhao S, Lin Q, Ran J et al. . Preliminary estimation of the basic reproduction number of novel coronavirus (2019-nCoV) in China, from 2019 to 2020: a data-driven analysis in the early phase of the outbreak. Int J Infect Dis 2020; 92:214–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Takian A, Raoofi A, Kazempour-Ardebili S. COVID-19 battle during the toughest sanctions against Iran. Lancet 2020; 395:1035–6. [DOI] [PMC free article] [PubMed] [Google Scholar]