

Summary:
Despite medical advances, the mortality rate associated with Fournier gangrene has remained largely unchanged and extremely high. In addition, conventional surgical treatment of Fournier gangrene of the scrotum requires excision of the testicles in some cases, which can result in loss of fertility. We report herein the favorable results of reconstruction of the scrotum following Fournier gangrene, using the hydrosurgery system and pedicled deep inferior epigastric perforator flap. A 60-year-old male patient was urgently transported to our hospital for fever, lower abdominal pain, and scrotal pain for several days. He was diagnosed with Fournier gangrene and underwent an emergency debridement procedure on the same day. Later, we performed a 2-phase reconstruction with a hydrosurgery system and pedicled deep inferior epigastric perforator flap under general anesthesia for the postoperative tissue defect. At 6 months postoperatively, there was no ulceration or scar contracture, and the results were aesthetically pleasing. There are no reported cases of reconstruction of the scrotum following Fournier gangrene using this procedure, and it might be an effective treatment option.
INTRODUCTION
Fournier gangrene is a necrotizing soft-tissue infection that occurs in the external genitalia and lower gastrointestinal tract. Despite medical advances, the mortality rate associated with necrotizing soft-tissue infection has remained largely unchanged over the past 30 years, and is as high as 25%–35%. The mortality rate is directly proportional to the time to medical intervention. Both aerobic and anaerobic bacteria cause Fournier gangrene, and sometimes, mixed infections occur. The gangrene progresses rapidly, causing multiple organ failure and, in some cases, death. Multidisciplinary treatment such as surgical debridement, antimicrobial administration, and hyperbaric oxygen therapy are required for life support.1,2
Herein, we report the favorable results of scrotal reconstruction following Fournier gangrene, using the hydrosurgery system (HS) and a pedicled deep inferior epigastric perforator (DIEP) flap.
CASE REPORT
A 60-year-old man presented with fever, lower abdominal pain, and scrotal pain for several days and was urgently transported to our hospital. The diagnosis was Fournier gangrene of the scrotum.3 An emergency debridement was performed under general anesthesia. The black necrotic skin and subcutaneous tissue from the scrotum to the perineum were excised, and the perineum was excised from the anus up to 2 cm anteriorly. Both testes and spermatic cords were spared (Fig. 1). Subsequently, his general condition improved with a multidisciplinary treatment, and 20 days after the initial debridement, he underwent secondary scrotal reconstruction with HS and pedicled DIEP flap, under general anesthesia. A hydraulic debridement was performed using hydrosurgery (VERSAJET II, Smith & Nephew, Watford, UK) until a good bleeding point was located. The remaining necrotic tissue was then removed to freshen the superficial tissue (Figs. 2 and 3).
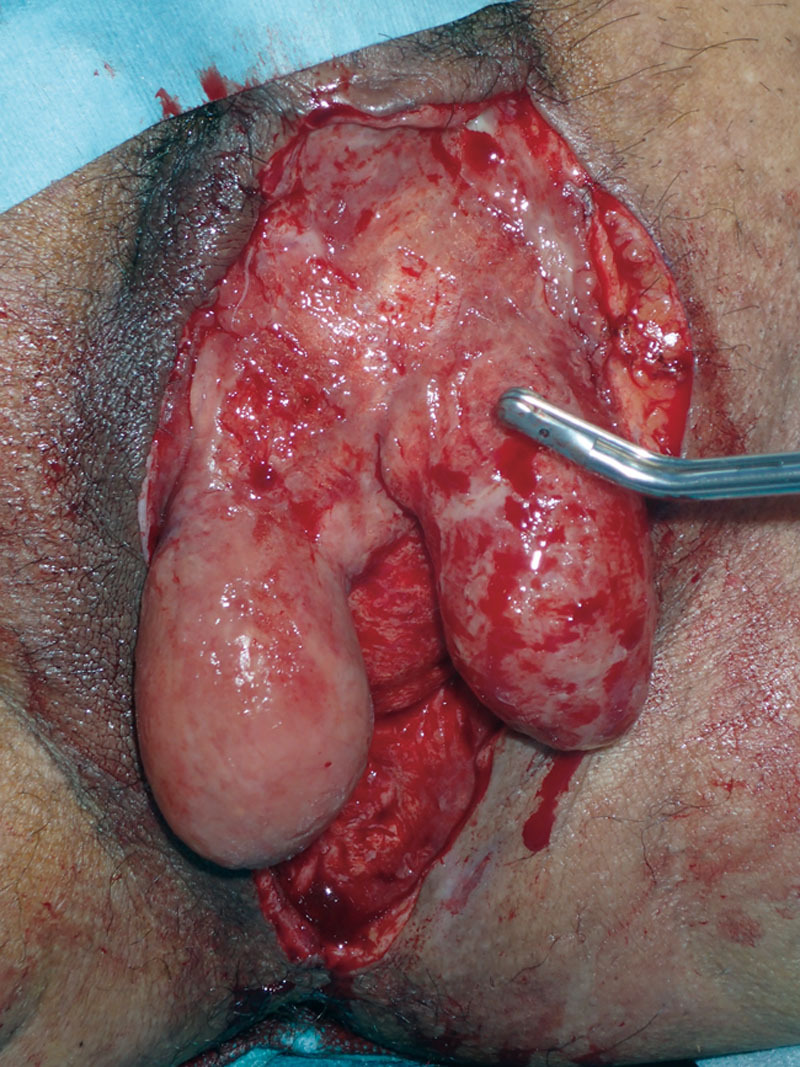
Fig. 1.

Appearance of Fournier gangrene of the scrotum during the emergency debridement. The black necrotic skin and subcutaneous tissue from the scrotum to the perineum were excised, and the perineum was excised from the anus up to 2 cm anteriorly.
Fig. 2.
Intraoperative findings of debridement using hydrosurgery. A hydraulic debridement was performed until a good bleeding point was located using HS.
Fig. 3.

Intraoperative findings of hydrosurgery. The remaining necrotic tissue was then removed to freshen the superficial tissue.
Next, a 15 × 8 cm pedicled DIEP flap was designed, and elevated from the left abdomen, with DIEP branching out from the medial side branch of the left deep inferior epigastric artery (DIEA) as the vascular pedicle. The vascular pedicle was dissected to the main trunk of the DIEA, so that the entire width of the muscle could be conserved. After elevation of the flap, the fat tissue beneath the superficial fascia was removed and thinning of the flap was performed. Next, a subcutaneous tunnel was created over the fascia of the left groin. The flap was transferred through the tunnel to the scrotal tissue defect and sutured (Fig. 4). A 15-Fr J-VAC Drainage System (Ethicon, Inc., Somerville, N.J.) was implanted in both the donor and recipient sites. Both were extracted on postoperative day 6.
Fig. 4.

Intraoperative findings of a DIEP flap reconstruction of scrotal tissue defects. A 15 × 8 cm pedicled DIEP flap from the left side of the abdomen was elevated and transferred through a subcutaneous tunnel into the scrotal tissue defect.
After ambulation on the 10th postoperative day, there were no complications such as infection, skin necrosis, wound dissection, or deep vein thrombosis (DVT). He was transferred to the rehabilitation center on the 40th postoperative day. At 6 months postoperatively, there was no ulceration or scar contracture, and the results were aesthetically pleasing (Fig. 5).
Fig. 5.

Scrotal findings at 6 months after reconstructive surgery. There was no ulceration or scar contracture, and the results were aesthetically pleasing.
DISCUSSION
In this case, we performed successful scrotal reconstruction using HS and pedicled DIEP flap for the treatment of Fournier gangrene of the scrotum. The first advantage of using the HS is that the handpiece is easy to handle. It is effective on areas with complex anatomy such as the face and limbs, which are difficult to approach with conventional surgical debridement.4,5 In this case, HS was remarkably effective for scrotal debridement, which has a complex anatomical structure. The second advantage is the high tissue selectivity. It is easy to adjust the thickness of the tissue to be removed by adjusting the water flow, thereby minimizing the invasion of normal tissue. Hence, selective debridement of the necrotic tissue can be performed to preserve more of the normal tissue.4,6 Conventional surgical treatment of Fournier gangrene of the scrotum requires excision of the testicles in some cases, which results in loss of fertility. However, in the present case, loss of fertility was prevented due to the high tissue selectivity. A third advantage is that the risk of postoperative infection can be reduced by washing the tissue with a large volume of saline solution during debridement. We previously reported the use of normal saline in debridement before flap reconstruction for pressure injuries of the trunk with wound infection, and no postoperative wound infection was seen in any of the cases.7 In this case too, normal saline was used to wash the scrotal infection, followed by flap reconstruction, and there was no postoperative wound infection.8
The DIEP flap is commonly used in breast reconstructive surgery. However, its use as a pedicle DIEP flap to fill a scrotal skin defect is rare.9 In general, split-thickness skin grafting is usually used for wound closure after surgical debridement for Fournier gangrene of the scrotum. Karian et al. suggested that the skin flaps could be used if the defect exceeds 50% of the scrotal surface area.10 In addition, if skin grafting is performed, the fixation period is longer (which delays ambulation) and there is a risk of DVT.9 In this case, the scrotal skin defect was reconstructed using the pedicled DIEP flap, no postoperative DVT was observed, and the patient was transferred to the rehabilitation center early. The scrotal skin protects spermatogenesis by radiating heat. Therefore, when the testicular and epididymal temperatures increase due to inhibition of heat dissipation, spermatogenesis is inhibited and the percentage of sperms with morphological abnormalities increases.11 Hence, if a thick pedicled DIEP flap is used for scrotal reconstruction, it might interfere with heat dissipation and inhibit spermatogenesis. Hence, we removed the fat and thinned the flap as much as possible.
CONCLUSION
We encountered a case of Fournier gangrene of the scrotum and performed scrotal reconstruction using HS and pedicled DIEP flap without postoperative infection or recurrence of ulcer formation.
Footnotes
Published online 23 September 2020.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Products and Drugs Used: VERSAJET II hydrosurgery debridement system [Product N. 6680039] (Smith & Nephew, Watford, UK), J-VAC Drainage System (Ethicon, Inc., Somerville, N.J.).
REFERENCES
- 1.Sarani B, Strong M, Pascual J, et al. Necrotizing fasciitis: current concepts and review of the literature. J Am Coll Surg. 2009;208:279. [DOI] [PubMed] [Google Scholar]
- 2.Thwaini A, Khan A, Malik A, et al. Fournier’s gangrene and its emergency management. Postgrad Med J. 2006;82:516–519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wong CH, Khin LW, Heng KS, et al. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004;32:1535–1541. [DOI] [PubMed] [Google Scholar]
- 4.Vanwijck R, Kaba L, Boland S, et al. Immediate skin grafting of sub-acute and chronic wounds debrided by hydrosurgery. J Plast Reconstr Aesthet Surg. 2010;63:544–549. [DOI] [PubMed] [Google Scholar]
- 5.Klein MB, Hunter S, Heimbach DM, et al. The versajet??? Water dissector: a new tool for tangential excision. J Burn Care Res. 2005;26:483–487. [DOI] [PubMed] [Google Scholar]
- 6.Gravante G, Delogu D, Esposito G, et al. Versajet hydrosurgery versus classic escharectomy for burn débridment: a prospective randomized trial. J Burn Care Res. 2007;28:720–724. [DOI] [PubMed] [Google Scholar]
- 7.Matsumine H, Giatsidis G, Takagi M, et al. Hydrosurgical debridement allows low-invasive and effective wound bed preparation of truncal pressure injuries before flap repair: a prospective uncontrolled case series. PRSGO. 2020;8:e2921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chammas MF, Jr, Gurunluoglu R, Carlsen SN, et al. Surgical debridement of mineral pitch and nonviable penile tissue using water-jet power: a preliminary report. BJU Int. 2009;103:974–976. [DOI] [PubMed] [Google Scholar]
- 9.Zeng A, Xu J, Yan X, et al. Pedicled deep inferior epigastric perforator flap: an alternative method to repair groin and scrotal defects. Ann Plast Surg. 2006;57:285–288. [DOI] [PubMed] [Google Scholar]
- 10.Karian LS, Chung SY, Lee ES.Reconstruction of defects after Fournier gangrene: a systematic review. Eplasty. 2015;15:e18. [PMC free article] [PubMed] [Google Scholar]
- 11.Abdelhamid MHM, Walschaerts M, Ahmad G, et al. Mild experimental increase in testis and epididymis temperature in men: effects on sperm morphology according to spermatogenesis stages. Transl Androl Urol. 2019;8:651–665. [DOI] [PMC free article] [PubMed] [Google Scholar]