

Abstract
Background:
Brachial plexus and axillary nerve injuries often result in paralysis of the deltoid muscle. This can be functionally debilitating for patients and have a negative impact on their activities of daily living. In these settings, transferring the branch of the radial nerve innervating the triceps to the axillary nerve is a viable treatment option. Additional nerve transfers may be warranted. This study sought to determine the efficacy of nerve transfer procedures in the setting of brachial plexus and axillary nerve injuries and factors affecting clinical outcomes.
Methods:
The U.S. National Library of Medicine’s website “PubMed” was queried for “radial to axillary nerve transfer” and “brachial plexus nerve transfer.” An initial review by two authors was performed to identify relevant articles followed by a third author validation utilizing inclusion and exclusion criteria. Individual patient outcomes were recorded and pooled for final analysis.
Results:
Of the 80 patients, 66 (82.5%) had clinical improvement after surgical nerve transfer procedures. Significant difference in clinical improvement following nerve transfer procedures was correlated with patient age, mechanism of injury, brachial plexus vs isolated axillary nerve injuries, multiple nerve transfers vs single nerve transfers, and surgery within the first 7 months of injury. The branch of the radial nerve supplying the triceps long head showed improved clinical results compared with the branch of the radial nerve supplying the triceps medial head and anconeus.
Conclusion:
Nerve transfers have been shown to be effective in restoring shoulder abduction in both isolated axillary nerve injuries and brachial plexus injuries.
INTRODUCTION
Brachial plexus injuries often result in permanent neurological deficits. Regardless of surgical intervention, the anatomic location, mechanism, and initial severity of the injury dictates expected outcomes.1 Axillary nerve injuries resulting in paralysis of the deltoid muscle can limit shoulder abduction especially when combined with brachial plexus injuries that incur additional muscle involvement.2–5 Axillary nerve injuries typically occur during traumatic events, resulting in closed stretch or blunt direct trauma to the nerve, but can also follow penetrating injuries, iatrogenic causes, and quadrilateral space syndrome.6–12 Upper brachial plexus injuries with C5/C6 root involvement often occur after motorcycle or motor vehicle accidents, resulting in avulsion or rupture of the nerve roots.1,8,13–16
Treatment options for axillary and brachial plexus injuries predominantly involved isolated tendon transfers or shoulder arthrodesis. However, surgical advances have shifted mainstay treatments toward nerve transfers.5 Favorable outcomes are seen when utilizing a donor nerve that is expendable, has pure motor function, many axons, good size match, and has a neuromuscular junction in close proximity to the targeted muscle.17,18 Early nerve transfers for the restoration of shoulder abduction in the setting of brachial plexopathy included using the phrenic nerve, spinal accessory nerve, or intercostal nerve.19,20
Leechavengvongs et al advocated transferring the radial nerve branch to the long head of the triceps to the axillary nerve utilizing a posterior approach for C5/C6 root avulsion injuries.8 The branch of the radial nerve to the long head of the triceps is expendable, has pure motor function, contains many axons, and is synergistic to the deltoid muscle.21 Early reports demonstrated that patients had M4 recovery of muscle strength and functional range of motion.22,23 Since Leechavengvongs’ original study in 2003, there have been multiple independent case series confirming the optimistic outcomes of transferring a branch of the radial nerve to the axillary nerve in the setting of brachial plexus or isolated axillary nerve injuries. The purpose of this study was to perform a systematic review using the patient data in these independent studies and determine factors that affect clinical outcomes.
MATERIALS AND METHODS
Literature Search
Institutional Review Board approval was obtained before initiating analysis or data collection. A retrospective review was conducted utilizing The U.S. National Library of Medicine’s National Center for Biotechnology Information’s website “PubMed.” The search terms were “radial to axillary nerve transfer” and “brachial plexus nerve transfer.” Utilizing titles and abstracts of each article, an initial review by two authors was performed to identify potentially relevant articles for review of the full text. The reference lists were compared and discussed with a third author, leading to secondary review exclusion of articles. The full articles of the final list were reviewed in the scope of the inclusion and exclusion criteria, resulting in the final list of articles used for analysis (Fig. 1).
Fig. 1.
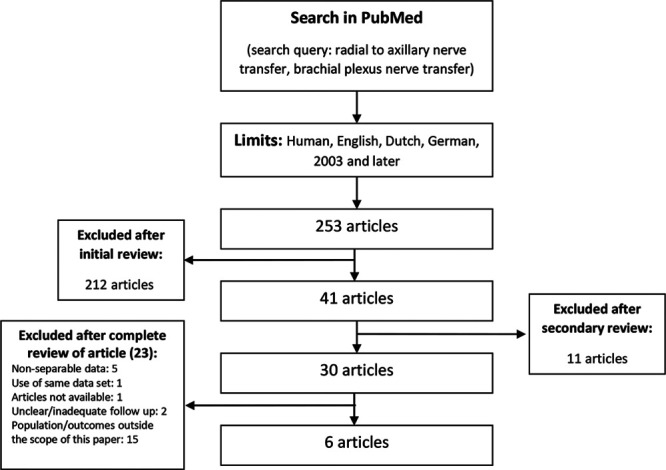
Flow diagram of study selection and stages of exclusion.
Inclusion and Exclusion Criteria
The included articles presented original data on individual patients who had undergone a radial to axillary nerve transfer, had a minimum of 6 months follow up, and reported changes in abduction range of motion or strength level. Studies on staged nerve transfer procedures, procedures in the setting of obstetric brachial plexopathy procedures, and procedures performed in the setting of partial amputations were excluded. Isolated lower brachial plexus injuries were excluded as the upper brachial plexus supplies the axillary nerve. Brachial plexus injuries with complete avulsion injuries were excluded, as these patients did not have nerve roots that could be appropriately used as grafts. Articles that reported only on surgical techniques or anatomic studies were excluded.
Defining Clinical Improvement
Approximately 130 degrees of abduction is required for ipsilateral overhead activities required to perform basic activities of daily living such as brushing one’s hair.24 In the setting of restricted joint motion, compensatory movements such as contralateral side bending to assist with ipsilateral shoulder abduction deficits are utilized to overcome loss in range of motion. Khadlikar et al. showed that certain activities of living, such as opening a door, opening/closing jars, and reaching behind one’s back, require less than 40 degrees of abduction.25 The most commonly accepted method of evaluating muscle strength is the Medical Research Council Manual Muscle Testing Scale (MRC; Fig. 2).22 Utilizing these parameters, clinical improvement in shoulder abduction was defined as an increased range of motion of ≥40 degrees of abduction or MRC grade of ≥3 after surgical intervention.
Fig. 2.
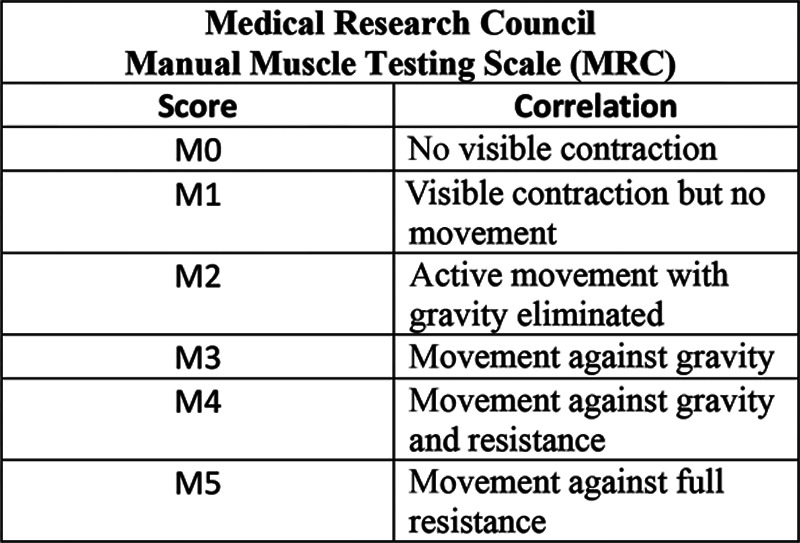
Muscle strength grading and clinical evaluation.
Data Extraction
After the final list of articles was established, two reviewers extracted data and compared outcomes to ensure correct reporting. The objective was to determine the expected outcomes in deltoid function and abduction after radial to axillary nerve transfer procedures. Both brachial plexus injuries and isolated axillary nerve injuries treated with nerve transfers described at the individual patient level were included in this study. Single nerve transfers included single radial nerve branch transfers to the axillary nerve. Multiple nerve transfers were defined as separate, individual nerve transfers performed during the same operation (ie, radial to axillary nerve transfer with additional ulnar to musculocutaneous nerve transfer and/or spinal accessory to suprascapular nerve transfer). Whether treated with single nerve transfers or multiple nerve transfers, all patients received a radial to axillary nerve transfer. Demographic, surgical, and outcome variables were collected, including age of patient, gender, type of injury, interval between injury and surgery, nerve transfer procedure performed, interval between surgery and follow up, MRC shoulder abduction strength before and after surgery, abduction range of motion of the shoulder before and after surgery, and the MRC strength of the triceps before and after surgery. High-energy mechanisms included motor vehicle accidents and motorcycle collisions. Low-energy mechanisms of injury included sport injuries, ground level falls, iatrogenic surgical injuries, and Parsonage-Turner syndrome.
Data and Statistical Analysis
Descriptive statistics were used to report basic measures such as number, mean (± SD), range, and median. Pairwise comparisons of continues variables were performed using a two-tailed paired student’s t-test. Pairwise comparisons of categorical variables were performed using a chi-squared analysis. Binary logistics regressions were used to calculate odds ratios. Multivariate binary logistic regression was attempted for all significant variables. Small group sizes (n < 5) utilized during analysis were compared using Fisher’s Exact Test. Alpha value of 0.05 was considered to be statistically significant throughout all data analysis. The statistical analysis operations were performed utilizing the IBM SPSS software platform.
RESULTS
The literature search returned 253 articles, 6 of which met the inclusion and exclusion criteria.1,8,16,26–28 A total of 80 patients were included with an average age of 30 ± 13 years, an average time from injury to surgery of 6.2 ± 2.3 months, and an average follow up of 27.2 ± 10 months. Of the 80 patients, 66 (82.5%) had clinical improvement after surgical nerve transfer procedures. No patients were reported to have a loss in triceps strength on follow up. Reported complications were limited to unsuccessful nerve transfer outcomes in 14 patients (17.5%). No other complications were reported.
Significant difference in clinical improvement following neurotization procedures were correlated with age (27.2 ± 9 versus 43.4 ± 19 years, n = 80, P = 0.007), caused by high energy mechanism of injury (86.1% versus 22.2%, n = 45, P < 0.001) and brachial plexus injuries vs isolated axillary nerve injuries (96% versus 60%, n = 80, P < 0.001) (Table 1). Significant difference in clinical improvement following neurotization procedures were also correlated with multiple nerve transfers vs single nerve transfers (95.6% versus 65.7%, n = 80, P = 0.001) and surgery within the first 7 months of injury (5.97 ± 2 versus 7.71 ± 3 months, n = 80, P = 0.008) (Table 2). Among those who underwent isolated radial to axillary neurotization for isolated axillary nerve injuries, the branch of the radial nerve supplying the triceps long head showed improved clinical results compared with the branch of the radial nerve supplying the triceps medial head and anconeus (76.2% versus 22.2%, n = 30, P = 0.013) (Table 2). There was no difference in outcomes between gender, time to follow up, nor incomplete versus complete brachial plexus injuries. However, after multivariate regression to correct for age, high energy mechanism, nerve injured, and interval between injury and surgery only high energy mechanism was a significant predictor of successful nerve transfer, with high energy mechanisms being 21.7 times more likely to show clinical improvement.
Table 1.
Demographic Information and Injury Characteristics Observed in Neurotization Procedures
| n | Clinical Improvement | No Clinical Improvement | P | OR (CI) | |
|---|---|---|---|---|---|
| Age (±SD) | 30 ± 13 | 27.2 ± 9 | 43.4 ± 19 | 0.007* | 0.92 (0.56–0.94) |
| Gender | |||||
| Male | 53 | 46 (86.8%) | 7 (13.2%) | 0.58 | |
| Female | 4 | 4 (100%) | 0 (0%) | ||
| Mechanism of injury | |||||
| High energy Motor vehicle collision Motorcycle collision |
36 | 31 (86.1%) | 5 (13.9%) | <0.001† | 21.7 (3.5–135.7) |
| Low energy Sports injury Ground-level fall Iatrogenic (surgical) Parsonage Turner syndrome |
9 | 2 (22.2%) | 7 (77.8%) | ||
| Nerve injury type | |||||
| Isolated axillary | 30 | 18 (60%) | 12 (40%) | <0.001† | 16 (3.3–78.7) |
| Brachial plexus | 50 | 48 (96%) | 2 (4%) | ||
Significance through student t test for independent variables assuming unequal variances.
†Significant through χ: 2 analysis.
CI, confidence interval; OR, odds ratio.
Table 2.
Factors and Related Outcomes after Nerve Neurotization Procedures
| n | Clinical Improvement | No Clinical Improvement | P | OR (CI) | ||
|---|---|---|---|---|---|---|
| Interval between injury and surgery, mo | 6.2 ± 2.3 | 5.97 ± 2 | 7.71 ± 3 | 0.008* | 0.72 (0.56–0.94) | |
| Time to follow-up, mo | 27.2 ± 10 | 26.6 ± 10 | 30.0 ± 11 | 0.28 | ||
| Type of nerve transfer | ||||||
| Single Radial → axillary |
35 | 23 (65.7%) | 12 (34.2%) | 0.001† | 11.2 (2.3–54.5) | |
| Multiple Radial → axillary + ulnar → musculocutaneous + spinal accessory → suprascapular |
45 | 43 (95.6%) | 2 (4.5%) | |||
| Brachial plexus injuries | ||||||
| Incomplete (C5–C6) | 34 | 34 (100%) | 0 (0%) | 0.098 | ||
| Complete (C5–T1) | 18 | 14 (87.5%) | 2 (12.5%) | |||
| Isolated axillary nerve injury with neurotization procedure | ||||||
| Nerve to triceps long head | 21 | 16 (76.2%) | 5 (23.8%) | 0.013† | ||
| Nerve to triceps medial head/anconeus | 9 | 2 (22.2%) | 7 (77.8%) | |||
*Significant through the χ: 2 analysis.
Significant difference using the Fisher exact test.
CI, confidence interval; OR, odds ratio.
DISCUSSION
In the setting of axillary nerve injuries, radial nerve transfers have been shown to be an effective treatment option. Patients with concomitant radial nerve injuries or below M4 strength of their triceps should be considered for other surgical options.
Brachial Plexus Injuries
Patient age was found to be a predictive factor for determining success rates in nerve transfer procedures, which was consistent with previous analysis. In a retrospective review of 21 patients undergoing radial nerve transfer for isolated axillary nerve injuries with mean follow up of 21 months, Lee et al. determined that increasing age was related to a decreased pre-injury conditioning of the deltoid in individuals.27 Bonnard et al. had similar findings, citing decreased capacity for nerve regeneration in older patients.29 These conclusions are consistent with the present findings; however, when controlling for the mechanism of injury, age was no longer considered a significant predictor of successful surgical outcomes. In this analysis, there was an observed correlation that patients who sustained higher energy mechanisms of injury had brachial plexus injuries, received multiple neurotizations, and showed an increased rate of clinical improvement. Although increasing age was associated with a higher risk for failed improvement in shoulder abduction, patients as old as 62 years still benefited from combined nerve transfer procedures. Therefore, a lower threshold for neurotization procedures should be considered in the setting of brachial plexopathy, regardless of age.
Axillary Nerve Injuries
Patients with isolated axillary nerve injuries demonstrated a clinically significant improvement less often than brachial plexus injuries (60% versus 96%; P < 0.05). This is likely due to the parameters set for clinical improvement in this study, and had more stringent clinical improvement criteria been chosen, these groups would have shown similar outcomes. The radial nerve branch to the triceps long head was a more efficacious (76%) donor than the nerve branch to the triceps medial head/anconeous (22.2%). Patients older than 45 years with an axillary nerve injury consistently failed to show clinically significant improvement in abduction strength and range of motion regardless of the radial nerve branch utilized for donation.
Surgical Timing and Electrodiagnostic Testing
In this analysis there was a significant difference in outcomes when time to surgery was before or after 7 months from the date of injury. This was confirmed through binary logistic regression suggesting surgery performed within 7 months from the date of injury led to superior clinical outcomes. We recommend discussing surgical intervention with patients who lack clinical signs of improvement confirmed by electrodiagnostic testing at 3–4 months after date of injury. This would allow adequate time for surgical planning and medical optimization.
Many patients who present with acute neuropraxia injuries will recover without surgical intervention and can initially be observed with efforts focused on maintaining full shoulder range of motion through conservative treatments.9,11 Wallerian degeneration can take up to 10 days to occur at which point nerve conduction studies can help differentiate between neurapraxia and axonotmesis based on the amplitude of the compound muscle action potential.30 Patients should be considered for electrodiagnostic testing between 1 and 3 months after injury to evaluate nerve continuity and deltoid innervation.31 Recently an electrodiagnostic parameter for the detection of axillary motor nerve injury was determined by comparing a conduction study of the contralateral limb; however, it has not been shown to be a prognostic factor in treatment outcomes.32 On the other hand, brachial plexus injuries without or with minimal voluntary motor unit potentials at 2–4 months are suggestive of poor outcomes.31 Therefore, the authors recommend electrodiagnostic testing for diagnosis confirmation after 1 month of conservative management followed by repeated electrodiagnostic testing at 2–4 months to project expected outcomes with continued conservative management versus surgical neurotization. If the patient does not show improvement on the second electrodiagnostic testing, most authors would suggest surgical intervention within six months from the date of injury.29,33
Other Considerations
Mechanism of injury was correlated with the type of nerve injury sustained in which higher energy mechanisms more often lead to brachial plexus injuries. These patients were more likely to undergo multiple nerve transfer procedures; however, some still received isolated single nerve transfers. This article showed that patients were more likely to show clinical improvement if they were younger, were involved in a high energy mechanism of injury, sustained a brachial plexus injury, and underwent multiple nerve transfers within 6 months of injury. These findings can be explained by brachial plexus injuries resulting in more debilitating functional outcomes and a greater capacity for clinical improvement when compared with isolated axillary nerve injuries alone. Shoulder abduction is a complex upper extremity function necessitating the actions of the scapulothoracic and glenohumeral muscles.34–37 The majority of shoulder abduction occurs at the glenohumeral joint with the deltoid serving as the primary abductor. However, there is obligatory scapulothoracic joint involvement in a 2:1 ratio of glenohumeral to scapulothoracic contribution, requiring recruitment of surrounding musculature.38–42 The contribution of additional musculature in performing shoulder abduction likely contributes to the greater improvement in shoulder abduction in brachial plexus patients receiving multiple nerve transfers.
Limitations
There were limitations of this study to include retrospective analysis and relatively small sample size contributing to notably larger odds ratios. Clinical assessment of deltoid abduction strength contribution has often been debated, given the complexity of the abduction movement and the multiple muscles involved.28,34–36,43 Lastly, this analysis used a relatively low threshold for clinical improvement. As discussed, certain activities of living require less than 40 degrees of abduction.25 In this study of 80 patients, 64 had a pre-operative shoulder abduction MRC strength of 0 or had an inability to abduct their shoulder entirely. While approximately 130 degrees of abduction is required for ipsilateral overhead activities,24 the authors considered a post-operative improvement of abduction MRC strength to ≥3 or ≥40 degrees of improved abduction to be clinically significant. More stringent parameters for clinical improvement could affect reported outcomes.
CONCLUSIONS
Radial nerve transfers have been shown to be effective in restoring shoulder abduction in both isolated axillary nerve injuries and brachial plexus injuries. Surgical intervention should be performed within the first 6–7 months after injury and the branch of the radial nerve supplying the long head of the triceps may be utilized. Clinical improvement has been noted as early as 3 months post operatively; however, a long-term follow up is indicated for rehabilitation.
ACKNOWLEDGMENT
The opinions or assertions contained herein are the private views of the authors and are not to be construed as reflecting the official position or views of the Department of the Army, the Department of Defense, or the U.S. Government.
Footnotes
Published online 23 September 2020.
Disclosure: Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, and patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article.
REFERENCES
- 1.Bertelli JA, Ghizoni MF.Transfer of the accessory nerve to the suprascapular nerve in brachial plexus reconstruction. J Hand Surg Am. 2007;32:989. [DOI] [PubMed] [Google Scholar]
- 2.Alnot JY.[Paralytic shoulder secondary to post-traumatic peripheral nerve lesions in the adult]. Acta Orthop Belg. 1999;65:10–22. [PubMed] [Google Scholar]
- 3.Bentolila V, Nizard R, Bizot P, et al. Complete traumatic brachial plexus palsy. Treatment and outcome after repair. J Bone Joint Surg Am. 1999;81:20–28. [DOI] [PubMed] [Google Scholar]
- 4.Azze RJ, Mattar Júnior J, Ferreira MC, et al. Extraplexual neurotization of brachial plexus. Microsurgery. 1994;15:28–32. [DOI] [PubMed] [Google Scholar]
- 5.Terzis JK, Kostas I, Soucacos PN.Restoration of shoulder function with nerve transfers in traumatic brachial plexus palsy patients. Microsurgery. 2006;26:316–324. [DOI] [PubMed] [Google Scholar]
- 6.Bertelli JA, Kechele PR, Santos MA, et al. Axillary nerve repair by triceps motor branch transfer through an axillary access: anatomical basis and clinical results. J Neurosurg. 2007;107:370–377. [DOI] [PubMed] [Google Scholar]
- 7.Lee S, Saetia K, Saha S, et al. Axillary nerve injury associated with sports. Neurosurg Focus. 2011;31:E10. [DOI] [PubMed] [Google Scholar]
- 8.Leechavengvongs S, Witoonchart K, Uerpairojkit C, et al. Nerve transfer to deltoid muscle using the nerve to the long head of the triceps, part II: a report of 7 cases. J Hand Surg Am. 2003;28:633–638. [DOI] [PubMed] [Google Scholar]
- 9.Safran MR.Nerve injury about the shoulder in athletes, part 1: suprascapular nerve and axillary nerve. Am J Sports Med. 2004;32:803–819. [DOI] [PubMed] [Google Scholar]
- 10.Terzis JK, Barmpitsioti A.Axillary nerve reconstruction in 176 posttraumatic plexopathy patients. Plast Reconstr Surg. 2010;125:233–247. [DOI] [PubMed] [Google Scholar]
- 11.Visser CP, Coene LN, Brand R, et al. The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery. A prospective clinical and EMG study. J Bone Joint Surg Br. 1999;81:679–685. [DOI] [PubMed] [Google Scholar]
- 12.Lädermann A, Lübbeke A, Mélis B, et al. Prevalence of neurologic lesions after total shoulder arthroplasty. J Bone Joint Surg Am. 2011;93:1288–1293. [DOI] [PubMed] [Google Scholar]
- 13.Limthongthang R, Bachoura A, Songcharoen P, et al. Adult brachial plexus injury: evaluation and management. Orthop Clin North Am. 2013;44:591–603. [DOI] [PubMed] [Google Scholar]
- 14.Rasulić L, Savić A, Lepić M, et al. Viable C5 and C6 proximal stump use in reconstructive surgery of the adult brachial plexus traction injuries. Neurosurgery. 2020;86:400–409. [DOI] [PubMed] [Google Scholar]
- 15.Acharya AM, Cherian BS, Bhat AK.Diagnostic accuracy of MRI for traumatic adult brachial plexus injury: a comparison study with surgical findings. J Orthop. 2020;17:53–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Leechavengvongs S, Witoonchart K, Uerpairojkit C, et al. Combined nerve transfers for C5 and C6 brachial plexus avulsion injury. J Hand Surg Am. 2006;31:183–189. [DOI] [PubMed] [Google Scholar]
- 17.Nath RK, Mackinnon SE.Nerve transfers in the upper extremity. Hand Clin. 2000;16:131, ix–9, ix. [PubMed] [Google Scholar]
- 18.Mackinnon SE, Novak CB.Nerve transfers. New options for reconstruction following nerve injury. Hand Clin. 1999;15:643, ix–66, ix. [PubMed] [Google Scholar]
- 19.Samardzic M, Grujicic D, Antunovic V.Nerve transfer in brachial plexus traction injuries. J Neurosurg. 1992;76:191–197. [DOI] [PubMed] [Google Scholar]
- 20.Merrell GA, Barrie KA, Katz DL, et al. Results of nerve transfer techniques for restoration of shoulder and elbow function in the context of a meta-analysis of the English literature. J Hand Surg Am. 2001;26:303–314. [DOI] [PubMed] [Google Scholar]
- 21.Witoonchart K, Leechavengvongs S, Uerpairojkit C, et al. Nerve transfer to deltoid muscle using the nerve to the long head of the triceps, part I: an anatomic feasibility study. J Hand Surg Am. 2003;28:628–632. [DOI] [PubMed] [Google Scholar]
- 22.Compston A.Aids to the investigation of peripheral nerve injuries. Medical Research Council: Nerve Injuries Research Committee. His Majesty’s Stationery Office: 1942; pp. 48 (iii) and 74 figures and 7 diagrams; with aids to the examination of the peripheral nervous system. By Michael O’Brien for the Guarantors of Brain. Saunders Elsevier: 2010; pp. [8] 64 and 94 Figures. Brain. 2010;133:2838–2844. [DOI] [PubMed] [Google Scholar]
- 23.James MA.Use of the medical research council muscle strength grading system in the upper extremity. J Hand Surg Am. 2007;32:154–156. [DOI] [PubMed] [Google Scholar]
- 24.Namdari S, Yagnik G, Ebaugh DD, et al. Defining functional shoulder range of motion for activities of daily living. J Shoulder Elbow Surg. 2012;21:1177–1183. [DOI] [PubMed] [Google Scholar]
- 25.Khadilkar L, MacDermid JC, Sinden KE, et al. An analysis of functional shoulder movements during task performance using Dartfish movement analysis software. Int J Shoulder Surg. 2014;8:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Uerpairojkit C, Leechavengvongs S, Witoonchart K, et al. Nerve transfer to serratus anterior muscle using the thoracodorsal nerve for winged scapula in C5 and C6 brachial plexus root avulsions. J Hand Surg Am. 2009;34:74–78. [DOI] [PubMed] [Google Scholar]
- 27.Lee JY, Kircher MF, Spinner RJ, et al. Factors affecting outcome of triceps motor branch transfer for isolated axillary nerve injury. J Hand Surg Am. 2012;37:2350–2356. [DOI] [PubMed] [Google Scholar]
- 28.Bertelli JA, Ghizoni MF.Nerve transfer from triceps medial head and anconeus to deltoid for axillary nerve palsy. J Hand Surg Am. 2014;39:940–947. [DOI] [PubMed] [Google Scholar]
- 29.Bonnard C, Anastakis DJ, van Melle G, et al. Isolated and combined lesions of the axillary nerve. A review of 146 cases. J Bone Joint Surg Br. 1999;81:212–217. [DOI] [PubMed] [Google Scholar]
- 30.Robinson LR.Traumatic injury to peripheral nerves. Muscle Nerve. 2000;23:863–873. [DOI] [PubMed] [Google Scholar]
- 31.Impastato DM, Impastato KA, Dabestani P, et al. Prognostic value of needle electromyography in traumatic brachial plexus injury. Muscle Nerve. 2019;60:595–597. [DOI] [PubMed] [Google Scholar]
- 32.Zis P, Hadjivassiliou M, Rao DG.Axillary motor nerve conduction study: description of technique and provision of normative data. J Electromyogr Kinesiol. 2018;39:95–98. [DOI] [PubMed] [Google Scholar]
- 33.Moor BK, Haefeli M, Bouaicha S, et al. Results after delayed axillary nerve reconstruction with interposition of sural nerve grafts. J Shoulder Elbow Surg. 2010;19:461–466. [DOI] [PubMed] [Google Scholar]
- 34.Paletta GA, Jr, Warner JJ, Warren RF, et al. Shoulder kinematics with two-plane x-ray evaluation in patients with anterior instability or rotator cuff tearing. J Shoulder Elbow Surg. 1997;6:516–527. [DOI] [PubMed] [Google Scholar]
- 35.Keener JD, Chalmers PN, Yamaguchi K.The humeral implant in shoulder arthroplasty. J Am Acad Orthop Surg. 2017;25:427–438. [DOI] [PubMed] [Google Scholar]
- 36.Amin NH, Ryan J, Fening SD, et al. The relationship between glenohumeral internal rotational deficits, total range of motion, and shoulder strength in professional baseball pitchers. J Am Acad Orthop Surg. 2015;23:789–796. [DOI] [PubMed] [Google Scholar]
- 37.Kibler WB, Sciascia A, Wilkes T.Scapular dyskinesis and its relation to shoulder injury. J Am Acad Orthop Surg. 2012;20:364–372. [DOI] [PubMed] [Google Scholar]
- 38.Poppen NK, Walker PS.Forces at the glenohumeral joint in abduction. Clin Orthop Relat Res. 1978;135:165–170. [PubMed] [Google Scholar]
- 39.Terzis JK, Papakonstantinou KC.The surgical treatment of brachial plexus injuries in adults. Plast Reconstr Surg. 2000;106:1097–1122; quiz 1123. [DOI] [PubMed] [Google Scholar]
- 40.Hippensteel KJ, Brophy R, Smith MV, et al. Comprehensive review of provocative and instability physical examination tests of the shoulder. J Am Acad Orthop Surg. 2019;27:395–404. [DOI] [PubMed] [Google Scholar]
- 41.Cvetanovich GL, Waterman BR, Verma NN, et al. Management of the irreparable rotator cuff tear. J Am Acad Orthop Surg. 2019;27:909–917. [DOI] [PubMed] [Google Scholar]
- 42.Burnier M, Elhassan BT, Sanchez-Sotelo J.Surgical management of irreparable rotator cuff tears: what works, what does not, and what is coming. J Bone Joint Surg Am. 2019;101:1603–1612. [DOI] [PubMed] [Google Scholar]
- 43.Okazaki M, Al-Shawi A, Gschwind CR, et al. Outcome of axillary nerve injuries treated with nerve grafts. J Hand Surg Eur Vol. 2011;36:535–540. [DOI] [PubMed] [Google Scholar]