

Abstract
Aim
To review the literature of existing survey instruments used to measure the occurrence of staff‐to‐resident elder abuse in residential care settings.
Methods
A comprehensive literature search during May 2017 produced 2,037 records. Two authors independently reviewed these records for inclusion, where a total of 17 studies met eligibility criteria. Descriptive information of all identified survey instruments is provided.
Results
This literature review reveals a diversity of survey instruments used to measure staff‐to‐resident abuse in residential care settings. The survey instruments varied greatly, where most instruments were self‐developed by the authors and provided none or limited information on psychometric properties. Most studies were conducted in high‐income countries and many of them in the United States.
Keywords: elder abuse, long‐term care settings, occurrence, prevalence, residential care settings, staff survey, staff‐to‐resident abuse, survey instruments
1. INTRODUCTION
Elder abuse is a major public health problem that may create serious health consequences for the victims, including increased risk of morbidity, mortality, institutionalisation and hospital admission (Baker, 2007; Dong & Simon, 2013; Lachs, Williams, O'Brien, Pillemer, & Charlson, 1998). The World Health Organization (WHO, 2002) defines elder abuse as “a single or repeated act, or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person.” It can be of various forms: physical, psychological/emotional, sexual and financial/material or simply reflect intentional or unintentional neglect.
Elder abuse occurs in all settings, among home‐dwelling older adults as well as residents in institutional care facilities. A review by Yon, Mikton, Gassoumis, and Wilber (2017) showed that the overall prevalence of abuse among community‐dwelling older persons was 15.7%, while another review by Yon, Ramiro‐Gonzalez, Mikton, Huber, and Sethi (2019) found that 64.2% of staff in institutional settings admitted to elder abuse in the past year. In institutional care, older adults may be exposed to abuse, neglect and mistreatment not only from staff, but also from co‐residents and relatives. This review focuses on instruments used to measure the occurrence of staff‐to‐resident abuse in residential care settings, such as nursing homes, assisted living facilities and other long‐term care facilities.
2. BACKGROUND
2.1. Residential care settings
Different factors contribute to an older person's vulnerability to abuse; these risk factors include old age, cognitive decline/dementia, mental illness, physical impairment, being dependent on help and care and being socially isolated (Lachs & Pillemer, 2004; McDonald et al., 2012; Pillemer, Burnes, Riffin, & Lachs, 2016). A large proportion of older adults in residential care settings are cognitively and physically impaired, and thus, they are more vulnerable and at a higher risk of being abused than others. Nevertheless, only a limited number of studies have focused on the occurrence of elder abuse in residential care settings. Studies from the USA (Pillemer & Moore, 1989), Canada (Hirst, 2002), Sweden (Saveman, Astrom, Bucht, & Norberg, 1999), Finland (Isola, Backman, Voutilainen, & Rautsiala, 2003), Germany (Goergen, 2004), Norway (Malmedal, Ingebrigtsen, & Saveman, 2009) and Ireland (Drennan et al., 2012) have shown that nursing home staff have observed acts of abuse and even admitted committing such acts themselves. The most observed acts were of negligent and of psychological character, often related to care activities such as unnecessarily leaving older residents alone or omitting to change wet incontinence pads (Isola et al., 2003; Malmedal et al., 2009), ignoring residents (Drennan et al., 2012; Malmedal et al., 2009; Wierucka & Goodridge, 1996), restraining a resident beyond what was needed (Drennan et al., 2012; Malmedal et al., 2009), omitting preventive measures with regard to pressure sores for residents confined to their beds (Goergen, 2001) or neglecting oral care (Malmedal et al., 2009). The findings from a systematic review and meta‐analysis (Yon et al., 2019) show the magnitude of the problem. The prevalence estimates reported by older residents were highest for psychological abuse (33.4%), followed by physical (14.1%), financial (13.8%), neglect (11.6%) and sexual abuse (1.9%). In addition, the review shows that data based on staff self‐reports indicated that 64.2% of staff admitted committing one or more acts of elder abuse in the past twelve months. The problems with reporting global prevalence based on the existing studies will be addressed in this article.
2.2. Measuring elder abuse in residential care settings
According to the WHO (2014), elder abuse has not been studied to the same extent as other types of violence and mistreatment in institutions may be more extensive than generally believed. In studies of vulnerable older persons (for example, those suffering from dementia or living in a residential institution for older adults), nearly 25% reported significant levels of psychological abuse (De Donder et al., 2011). The recent systematic review and meta‐analysis in institutional care demonstrated differences in overall prevalence estimates, ranging from 53.3%–73.9% (Yon et al., 2019). However, differences in the definition and choice of the measurement instrument can influence the prevalence rates of elder mistreatment (De Donder et al., 2011), where it was found that operationalization and items included in the survey instruments varied greatly, depending on the researchers’ concepts and definitions. Different cut‐off points for responses were also used; for example, either a single (unrepeated) episode or a single form that occurred repeatedly before it was categorised as abuse. The same review revealed that most studies self‐designed questions and did not appear to have (or did not report that they had) validated their measurement instruments. Fifteen out of nineteen studies used their own questions, only one provided information on face validity and none of them reported information on reliability or validity (De Donder et al., 2011).
It is possible to ask some residents about abuse, but when taking the frailty of most nursing home residents into consideration, one can understand that this is challenging. Only a few of the residents would be able to take part in such studies. Other reasons why the residents are unwilling to report abuse may be due to fear of speaking up, they can be afraid of revenge, or they do not want to be a complaining person. Researchers measuring elder abuse in institutional settings have therefore often chosen to conduct surveys among staff. Even though this is also a limitation, for example, one can expect underestimates of abuse (Castle, 2012), this seems to be the preferred design. As there is no gold standard available, researchers tend to create their own study‐specific instruments, which makes it impossible to compare results across studies. To capture and summarise the different instruments used to measure institutional elder abuse, we undertook a literature review of existing elder abuse prevalence studies using staff‐reported instruments from around the world.
2.3. Objectives
The objectives of this review were as follows: (a) to identify studies using staff surveys to measure the occurrence of observed and/or perpetrated staff‐to‐resident abuse in residential care settings for older people and (b) to provide a description of these survey instruments.
3. THE STUDY
3.1. Design
A comprehensive literature review.
3.2. Search strategy
A comprehensive literature search was conducted by an experienced librarian in May 2017. The search strategy was executed in the following databases: Medline, Cinahl, Cochrane Library, Embase, PsycINFO and SveMed+. No specific time frame was indicated; we wanted to find relevant articles regardless of year of publication. The search was based on a combination of MeSH‐terms and keywords. The following search terms were used, combined with adequate Boolean operators: older persons, older adults, residents, patients, seniors, elders/elderly, aged, nursing homes, long‐term care facilities, residential care settings, residential care institutions, residential aged care facility, residential facilities, care homes, nursing residence, homes for the aged, neglect, violence, aggression, mistreatment, maltreatment, inadequate care, ill‐treatment, restraints, coercion, duress, abuse, physical abuse, physical aggression, psychological abuse, material/financial abuse, material/financial exploitation, sexual abuse, sexual aggression, patient abuse, verbal abuse, verbal aggression, emotional abuse, elder abuse, elder mistreatment, elder maltreatment, prevalence, incidence, occurrence, screening, frequency and correlation. We also conducted a secondary hand‐search of selected journals and screened references cited in included articles and previous literature reviews. Alert services were set up, and we received notifications of new records in selected databases, up to December 2019.
3.3. Eligibility criteria
A set of inclusion and exclusion criteria were used for selecting the studies:
Inclusion criteria were as follows: (a) studies which addressed elder abuse of older persons (65 years and more) in residential care settings with estimates, frequencies, prevalence, incidence rates etc.; (b) studies based on quantitative healthcare staff surveys; (c) only original peer‐reviewed studies; (d) written in English or any Scandinavian language; and (5) published in scientific journals.
Exclusion criteria were as follows: (a) studies of elder abuse in the community; (b) studies of elder abuse of persons under 65 years of age; (c) studies concerning self‐neglect, restraints or homicide; (d) studies with solely a qualitative design; and (e) reviews, conference proceedings, editorial commentaries or letters.
3.4. Data extraction and analysis
Two of the authors independently reviewed studies identified in the literature search. After duplicates were removed, the title and/or abstract of the records were screened independently by the two authors. The full text of the remaining studies was then assessed for eligibility by the same authors to find the final studies to be included. Any discrepancies were discussed in meetings with all the authors. To describe the methodological quality of the survey instruments, we considered using the COSMIN risk of bias checklist (Mokkink et al., 2018). However, after using the checklist on some of the articles, we found that COSMIN was not a suitable tool for this purpose. The articles did not contain enough information about the survey instruments to make a proper assessment, according to COSMIN. Therefore, we chose to go through the articles and describe the survey instruments more thoroughly. The following data on the survey instruments were extracted: main author and year of publication, country of origin, observed/perpetrated abuse, types of abuse measured, respondents, timeframe, number of items, measurement scale, instrument‐description, reliability and validity. In studies where the survey instrument was not thoroughly described, the corresponding authors were contacted to get a copy of the instruments (Table 1).
TABLE 1.
Survey instruments measuring staff‐to‐resident abuse in residential care settings
| Author (year), country | Type of abuse | Design and data collection | Respondents (response rate if specified) and setting | Time frame | Number of items | Scoring scale | Instrument development | Reliability | Validity | Language | Availability of instrument |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Moore (2017), United Kingdom | Witnessed/suspected psychological, physical, sexual, financial, neglect and other |
Questionnaire pen‐and‐paper survey Postage‐paid return envelope |
N = 156 nursing and care staff (rr = 75.4%) from five convenient independent‐sector nursing homes for older people | Past year, 1–3 years or > 3 years ago | Not specified | Once or repeatedly. | Not specified | Not specified | Not specified | English | Not found online |
| Blumenfeld Arens et al. (2017), Switzerland | Observed emotional, physical and neglect. | Secondary analysis of SHURP (cross‐sectional multicenter study) | N = 4,599 care workers from 156 randomly selected nursing homes | Past 4 weeks | 5 | 4‐point Likert scale, from “never” to “more than once a week” | Investigator‐constructed instrument derived from Malmedal et al. (2009) | Neglect sum index; Cronbach's alpha 0.78 | Not specified | German, French | |
| Neuberg et al. (2017), Croatia | Observed psychological, physical, sexual, financial and neglect. | Cross‐sectional survey | N = 171 nurses (rr = 85.5%) from four NHs and two extended care units at the hospital | Past year | 25 | Never, once, 2–10 times, more than 10 times | 20 items from Drennan et al. (2012) + 5 study‐specific items self‐developed by the authors | Analysis included only items with Cronbach's alpha > 0.7 | Pretested in a validation pilot study. Only behaviours observed by more than 10% of respondents were recorded | Croatian | Not found online, available from author |
| Drennan et al. (2012), Ireland | Observed/perpetrated psychological, physical, sexual, financial and neglect |
National cross‐sectional pen‐and‐paper survey Postage‐paid return envelope |
N = 1,316 nurses and healthcare assistants (rr = 43%) from 64 randomly selected residential care settings | Past year | 20 | Never, once, 2–10 times, more than 10 times | Modified version of the conflict tactics scale to measure psychological (5 items) and physical abuse (6 items), single item from Harris and Benson (1998) to measure financial abuse, one study‐specific single item to measure sexual abuse, study‐specific items (N = 7) to measure neglect | Not specified | Not specified | English | Not found online, not available form author |
| Castle (2013), United States | Perceptions of verbal, psychological, physical, caregiving, medication, sexual and material exploitation |
Cross‐sectional survey Postage‐paid return envelope |
N = 12,555 direct care workers (rr = 81%) from 1,500 assisted living facilities | Past 3 months | 28 | Never, once, 2–3 times, 4–5 times, 5–6 times, other (#) | Previously used questionnaire (Castle, 2011–2012) | Reported missing items, floor‐ceiling, item‐scale correlations (>r = 0.50) and Cronbach's alpha > 0.70 | Face and content validity described. Used Fleisch–Kinkaid Scale | English | Not found online, available from author |
| Castle (2012), United States | Perceptions of verbal, psychological, physical, caregiving, medication, sexual and material exploitation |
Cross‐sectional survey Postage‐paid return envelope |
N = 4,451 nurse aides (rr = 64%) working in NHs and registered in the Pennsylvania nurse aide registry | Past 3 months (in a prior facility) | 31 |
Observed or have evidence that this happened; the resident told you this happened; someone other than the resident told you this happened; you suspect that this happened |
Self‐developed study‐specific questionnaire | Not specified | Face and content validity described. Used Fleisch–Kinkaid Scale | English | Not found online, available from author |
| Castle and Beach (2011), United States | Observed verbal, psychological, physical, caregiving, medication, sexual and material exploitation |
Cross‐sectional survey Mail survey |
N = 855 nurse aides working in assisted living facilities and registered in the Pennsylvania nurse aide registry | Past 3 months | 28 | Never, once, 2–3 times, 4–5 times, 5–6 times, other # | Self‐developed study‐specific questionnaire | Not specified | Face and content validity described. Used Fleisch–Kinkaid Scale | English | https://www.icpsr.umich.edu/icpsrweb/NACJD/studies/34575/datadocumentation# |
| Buzgova and Ivanova (2011), The Czech Republic | Observed/perpetrated psychological, physical, financial, sexual and neglect |
Quantitative pen‐and‐paper survey Sealed collection boxes |
N = 454 direct care employees (rr = 64%) from 12 randomly selected senior homes | Past year | 40 | Never, once, repeatedly | Self‐developed study‐specific questionnaire | Not specified | Clarity and comprehensibility of questions reviewed in a preliminary survey in 2007 | Czech | Not found online, available from author |
| Natan, Lowenstein, and Eisikovits (2010), Israel | Observed/perpetrated physical violence, mental abuse, physical neglect, mental neglect, sexual violence and financial exploitation | Quantitative pen‐and‐paper survey | N = 510 healthcare staff (85%) from 22 randomly selected long‐term nursing homes | Past year | Not specified | Not specified | Iowa Dependent Adult Abuse Nursing Home Questionnaire designed by Daly and Jogerst (2005) | Not specified | Not specified | Hebrew | Not found online, available from author |
| Malmedal et al. (2009), Norway | Observed/perpetrated physical, emotional and neglect |
Cross‐sectional pen‐and‐paper survey Sealed envelopes collected by a “coordinator” |
N = 616 nursing staff (rr = 79%) from 16 nursing homes | During the entire work carrier | 21 | Never, once a month or rarer, once a week or rarer, more than once a week | Self‐developed study‐specific questionnaire inspired by Pillemer and Moore (1989), Goergen (2004) and Saveman et al. (1999) | Cronbach's alpha; physical 0.57; emotional 0.43; neglect 0.78 | Focus group and two pilot studies. | Norwegian | https://core.ac.uk/download/pdf/52109553.pdf |
| McCool et al. (2009), United States | Observed/suspected physical, emotional, sexual, financial and neglect |
Questionnaire pen‐and‐paper survey Return envelope |
N = 49 nursing staff (rr = 15%) from two nursing homes | Suspected abuse in their current facility | 5 | Not specified | “The Nursing Home Questionnaire” based on a former study by Clark‐Daniels, Daniels, and Baumhover, (1990) was revised for nursing home employees and Iowa laws | Not specified | Not specified | English | Not found online |
| Wang (2005), Taiwan | Observed psychological |
Cross‐sectional survey Structured face‐to‐face administration of survey instruments |
N = 114 caregivers from several long‐term elderly care facilities | Past 6 months | 20 | 4 point Likert scale from “never” to “often” | Caregiver Psychological Elder Abuse Behavior (CPEAB) Scale (previously validated by Wang, 2004) | Cronbach's alpha 0.85 | Content validity index 0.95 |
Mandarin English (translation not described) |
Not found online, available from author |
| Goergen (2004), Germany | Observed/perpetrated psychological, physical, sexual, neglect and inappropriate use of restraints | Questionnaire survey | N = 361 nursing staff (rr = 36%) from 27 nursing homes | Past year | 46 | Yes, #__ times and No | Instrument previously used in the pilot study of Goergen (2001) | Not specified | Not specified | German | Not found online, available from author |
| Goergen (2001), Germany | Observed/perpetrated psychological, physical, sexual, neglect and inappropriate use of restraints |
Questionnaire survey Returned individually by mail |
N = 79 nursing staff (rr = 20.4%) from 9 convenient sampled nursing homes | Past year | 45 | Yes, #__ times and No | Self‐developed study‐specific questionnaire inspired by the conflict tactics scale and Pillemer and Moore (1989) | Not specified | Not specified | German | Not found online, available from author |
| Harris and Benson (1999), United States | Observed/perpetrated financial/theft |
National survey Postage‐paid return envelope |
N = 1,116 nursing staff (rr = 22%) from 47 randomly selected nursing homes | Past year | Not specified | If they had taken, and the number of times | Self‐developed study‐specific questionnaire | Not specified | Not specified | English | Not found online |
| Saveman et al. (1999), Sweden | Observed/perpetrated psychological physical, sexual, financial and neglect. |
Quantitative and qualitative survey. Questionnaires collected and sent to researchers |
N = 499 nursing staff (rr = 78%) working in residential settings in one area in Umeå and Kalmar | Past year | Not specified | Never, sometimes per month, at least once a week, weekly, daily | Self‐developed sudy‐specific instrument containing multiple‐choice and open‐ended questions | Not specified | Not specified | Swedish | Not found online |
| Pillemer and Moore (1989), United States | Observed/perpetrated physical and psychological | Telephone survey | N = 577 staff (rr = 85%) from 31 nursing homes | Past year | 11 | Never, once, 2–10 times, more than 10 times | Self‐developed study‐specific questionnaire based on the conflict tactics scale | Not specified | Not specified | English | Not found online |
3.5. Ethics
Ethical approval was not required.
4. RESULTS
A total of 2,037 records were identified from the comprehensive literature search, and an additional nine records were identified through a secondary search. After removing duplicates, screening and assessing full‐text documents a total of 17 studies were included in this review. See Figure 1 for an overview of the selection process. All included studies reported the occurrence of staff‐to‐resident abuse in residential care settings measured by staff surveys.
FIGURE 1.
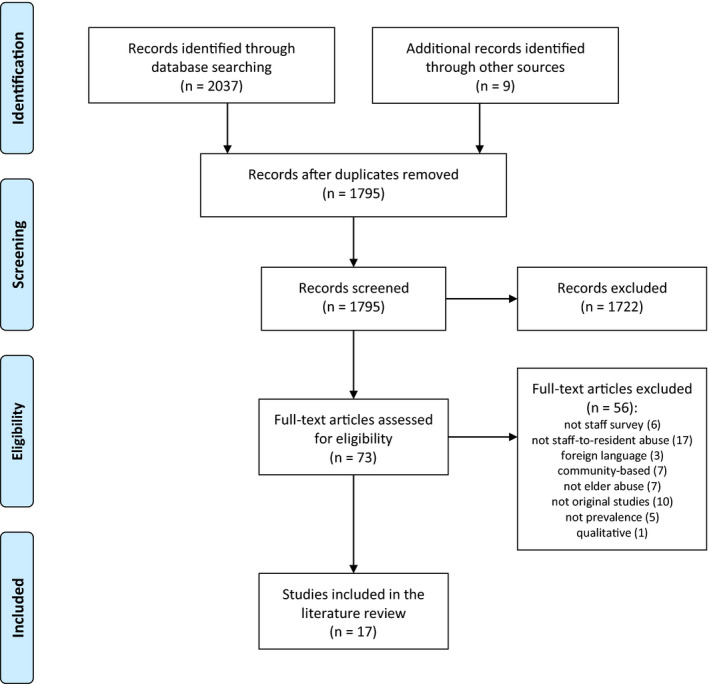
Flow diagram of the literature search and review
4.1. Characteristics of studies using staff survey instruments
The 17 studies identified in the literature review came from the USA, UK, Sweden, Norway, Germany, Ireland, Croatia, Israel, Taiwan, Switzerland and the Czech Republic, and they were all published between 1989–2017. Most studies were conducted in high‐income countries and many of them in the USA. Two studies were completed in assisted living facilities (Castle, 2013; Castle & Beach, 2011) and the rest in nursing homes/long‐term care units. In all surveys, healthcare staff were the respondents and the number of respondents ranged widely from 49 (McCool, Jogerst, Daly, & Xu, 2009)–12,555 (Castle, 2013). Likewise, the response rate ranged widely from 15.0% (McCool et al., 2009)–85.5% (Neuberg, Zeleznik, Mestrovic, Ribic, & Kozina, 2017). Fifteen studies used pen‐and‐paper questionnaires, one study used a face‐to‐face administration of study instruments (Wang, 2005) and one study used a telephone survey (Pillemer & Moore, 1989). Three studies were conducted nationally with a representative sample (Blumenfeld Arens, Fierz, & Zuniga, 2017; Drennan et al., 2012; Harris & Benson, 1999).
4.2. Descriptive information of survey instruments
Table 1 shows that only one study used a previously validated instrument to measure psychological abuse (Wang, 2005); the rest of studies developed their own study‐specific survey instruments to measure staff‐to‐resident abuse. Eight studies measured only observed/witnessed/suspected abuse, while nine studies measured both observed and perpetrated abuse. Ten studies measured all types of abuse (psychological, physical, financial/material, sexual and neglect). One study was solely on financial abuse/theft (Harris & Benson, 1999), and one study was solely on psychological abuse (Wang, 2005). The rest of the studies did not include sexual abuse, financial/material abuse and/or neglect. The number of items used to measure staff‐to‐resident abuse differed from 5–46, where four studies did not specify the number of items. Ten studies used a timeframe of the past year, where the rest of the studies used a timeframe ranging from four weeks to the entire lifetime. Only one study described psychometric properties of the instrument thoroughly (Wang, 2005), while four studies reported Cronbach's alpha values (Blumenfeld Arens et al., 2017; Drennan et al., 2012; Malmedal et al., 2009; Neuberg et al., 2017) and one study reported missing, floor‐ceiling effects and item‐scale correlations (Castle, 2013). Seven studies described the survey questionnaire development with a pilot study testing face/content validity. Nine studies were either originally in English language or translated by the authors (translation not described).
5. DISCUSSION
To the best of our knowledge, this is the first literature review of studies using staff surveys to measure the occurrence of staff‐to‐resident abuse in residential care settings. In this review, we examined 17 studies that provided information about their survey instruments. Our results show that there exists a great variety of survey instrument used to measure staff‐to‐resident abuse in residential care settings, which makes it difficult to compare the occurrence of elder abuse across studies and nations.
5.1. Data collection methods
Most survey instruments were completed with pen and paper, and we did not identify any web‐based or electronic staff surveys. Pillemer and Moore (1989) used a telephone survey and argue that compared with face‐to‐face interviews, telephone surveys encourage more honest responses because respondents feel less self‐conscious. Thus, paper surveys may provide even more anonymity and perhaps more honest responses than telephone and face‐to‐face surveys, due to respondents' social desirability to answer more positively in direct settings of contact. However, telephone and face‐to‐face surveys may be more expensive than mailed paper surveys. We found that the paper questionnaires were either returned by prepaid return envelopes, collected and returned by study “coordinators,” or the questionnaires were self‐dropped in sealed collection boxes at the facilities. Future studies should consider whether prepaid return envelopes encourage more honest responses than on‐site sealed collection boxes, but this is also a matter of cost, because prepaid return envelopes may be more expensive than sending or collecting sealed return boxes.
5.2. Study samples
One issue of concern in studies with a cross‐sectional design is the representativeness of nursing staff selected to respond in the survey. We found that only three studies had randomly selected institutions to participate. In Switzerland, a multicenter cross‐sectional study employed a stratified sampling method to include a representative sample of nursing homes (Blumenfeld Arens et al., 2017). In the USA, Harris and Benson (1999) used a multi‐stage stratified cluster sampling technique to draw the nursing home population. In Ireland, all residential care homes were stratified in four geographical clusters and the institutions were weighted by the number of beds before randomisation (Drennan et al., 2012). In Norway, Malmedal et al. (2009) stratified nursing homes into small/large sizes in rural/urban locations, but the nursing homes were only selected from one out of 19 counties in Norway. The rest of the studies used either a convenient sample of nursing homes or nursing homes located in smaller regional areas. Such differences in sampling techniques may influence the survey results and occurrence rates. The survey instruments varied widely regarding the number of participating nursing staff and response rates. One limitation of conducting surveys in residential care settings is low response rates, which might be caused by the high workload nursing staff experience and their low motivation to participate and one may speculate whether nursing staff who do not want to participate exhibit more acts of abuse. In our review, we found that response rates varied considerably from 15%–85.5%, but surprisingly nine out of 17 studies reported response rates above 60% (Table 1). Furthermore, since most studies were conducted in high‐income countries and many of them in the USA, the instruments found in this review may not be transferrable to low‐income countries.
5.3. Survey instrument content
The survey instruments varied widely in how they were developed, type of abuse measured, the number of items used and the timeframe used to measure the occurrence of staff‐to‐resident abuse. However, many of the instruments were inspired by the conflict tactics scale (CTS) developed by Straus (1979). The CTS is the most widely used instrument to measure domestic violence, and it has been translated and used in several countries worldwide. Pillemer and Moore (1989) conducted one of the first surveys of elder abuse in nursing homes and used CTS when designing the abuse measurement instrument. One disadvantage with CTS is that it does not measure financial/material abuse nor neglect. To measure these subtypes of abuse, researchers self‐developed their own survey questions. In addition, the number of items used to measure staff‐to‐resident abuse varied greatly. One may assume that short questionnaires are more useful than extensive and detailed instruments and may increase the response rate. However, the study of McCool et al. (2009) used five items to measure abuse and reported a considerably lower response rate than Buzgova and Ivanova (2011) that used 40 items.
Most studies used a timeframe of the past year, but some studies used much shorter timeframes. There may be limitations of both long and short timeframes to measure the occurrence of abuse. Too extensive timeframes may lead to recall bias, because nursing staff may not remember the accurate number of incidents one year back in time, but both short and long timeframes may limit the pool of respondents because they may not have been employed during the entire reference period (Castle, 2013). Castle (2012) found that nurse aides believed they could provide accurate responses if a timeframe of three months was used. Nevertheless, the use of different timeframes makes it difficult to compare prevalence estimates across studies and nations and future studies should consider a consensus on the reference period.
5.4. Survey instrument reliability and validity
As Table 1 shows, only one study used a validated instrument to measure abuse (Wang, 2005), but this instrument only measured psychological abuse and not the other subtypes.
Some studies reported Cronbach's alpha values, but most studies did not provide thoroughly information regarding the instruments' basic psychometric properties. Some researchers did, however, describe how face and content validity had been pretested in pilot studies with open‐ended measures, focus‐groups and/or cognitive interviews of staff. Testing both the reliability and validity of a survey instrument is important to ensure both consistency and accuracy of a measure. The instrument by Dr. Nicholas Castle in the USA was the only instrument measuring all types of staff‐to‐resident abuse with several items on each subtype. The author did also report a thoroughly description on how the instrument was developed with cognitive interviews, face and content validity, use of the Fleisch–Kinkaid scale and some psychometric properties such as missing items, floor‐ceiling categories, item‐scale correlation and Cronbach's alpha coefficients. The instrument had also been used in three large staff surveys measuring staff‐to‐resident abuse in both nursing homes and assisted living facilities. Nevertheless, further psychometric properties such as a factor analyses should be conducted to assess the dimensions of abuse and appropriateness for use across studies.
5.5. Strengths and limitations
There are some limitations in this review that should be noted. First, only studies published in English or Scandinavian were included, which limits the selection. Although all studies were published in English, several of the questionnaires had not been translated into English, which made them difficult to compare. The lack of description of the development of survey instruments made it impossible to evaluate the questionnaires with COSMIN. The strengths of this review are the comprehensive literature search made by an experienced librarian and the thorough review by researchers. Further, to the best of our knowledge, this is the first literature review addressing these measurement instruments. The unique contribution of this study is that it provides necessary knowledge on the diversity of the measurement instruments used on staff‐to‐resident abuse. This diversity was perhaps welcomed in early times of establishing and developing the research field, but now it hinders the opportunity to fully compare prevalence across countries and makes it more difficult to develop effective preventive measures.
6. CONCLUSIONS
Our comprehensive literature review shows that there exists a variety of survey instruments used to measure staff‐to‐resident abuse in residential care settings, where most of the studies are conducted in high‐income countries. This variety makes it difficult to compare the occurrence of elder abuse across studies and borders. A standardised survey instrument suitable for both high‐ and low‐income countries would be valuable, and it may also be beneficial to standardise the sampling procedures and data collection methods.
Is it possible to single out one survey questionnaire that can be used as a gold standard to measure elder abuse across studies and nations? We suggest that one first important step is to make a clear description of how instruments are made and make the instrument available to other researchers. If this becomes standard procedure, it may provide a better basis for establishing a kind of gold standard. Even after several decades of studies on elder abuse in residential care facilities, we have not reached a consensus regarding survey instruments. The conflict tactics scale is a possible instrument to agree on, but CTS needs to be developed further and should include all subtypes of elder abuse, including financial/material abuse, as well as neglect. The instrument developed by Dr. Castle is a promising tool measuring all types of staff‐to‐resident abuse in both nursing homes and assisted living facilities, and it has already been used in several large US surveys of staff. However, the psychometric properties and user‐evaluation of this instrument should be further assessed.
CONFLICTS OF INTEREST
There is no conflict of interest.
PATIENT CONSENT
No patient consent was needed for this study.
Malmedal W, Kilvik A, Steinsheim G, Botngård A. A literature review of survey instruments used to measure staff‐to‐resident elder abuse in residential care settings. Nursing Open. 2020;7:1650–1660. 10.1002/nop2.573
Funding information
The study was funded by Norwegian Research Council.
REFERENCES
- Baker, M. (2007). Elder mistreatment: Risk, vulnerability and early mortality. Journal of American Psychiatric Nurses Association, 12, 313–321. 10.1177/1078390306297519 [DOI] [Google Scholar]
- Blumenfeld Arens, O. , Fierz, K. , & Zuniga, F. (2017). Elder abuse in nursing homes: Do special care units make a difference? A secondary data analysis of the Swiss Nursing Homes Human Resources Project. Gerontology, 63(2), 169–179. 10.1159/000450787 [DOI] [PubMed] [Google Scholar]
- Buzgova, R. , & Ivanova, K. (2011). Violation of ethical principles in institutional care for older people. Nursing Ethics, 18(1), 64–78. 10.1177/0969733010385529 [DOI] [PubMed] [Google Scholar]
- Castle, N. (2012). Nurse aides' reports of resident abuse in nursing homes. Journal of Applied Gerontology, 31(3), 402–422. 10.1177/0733464810389174 [DOI] [Google Scholar]
- Castle, N. (2013). An examination of resident abuse in assisted living facilities. Retrieved from US: https://www.ncjrs.gov/pdffiles1/nij/grants/241611.pdf [Google Scholar]
- Castle, N. , & Beach, S. (2011). Elder abuse in assisted living. Journal of Applied Gerontology, 32(2), 248–267. 10.1177/0733464811418094 [DOI] [PubMed] [Google Scholar]
- Clark‐Daniels, C. L. , Daniels, R. S. , & Baumhover, L. A. (1990). Physicians' and nurses' responses to abuse of the elderly: A comparative study of two surveys in Alabama. Journal of Elder Abuse & Neglect, 1(4), 57–72. [Google Scholar]
- Daly, J. M. , & Jogerst, G. J. (2005). Association of knowledge of adult protective services legislation with rates of reporting of abuse in Iowa nursing homes. Journal of the American Medical Directors Association, 6(2), 113–120. [DOI] [PubMed] [Google Scholar]
- De Donder, L. , Luoma, M.‐L. , Penhale, B. , Lang, G. , Santos, A. J. , Tamutiene, I. , … Verté, D. (2011). European map of prevalence rates of elder abuse and its impact for future research. European Journal of Ageing, 8(2), 129 10.1007/s10433-011-0187-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dong, X. , & Simon, M. A. (2013). Elder abuse as a risk factor for hospitalization in older persons. JAMA Internal Medicine, 173(10), 911–917. 10.1001/jamainternmed.2013.238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Drennan, J. , Lafferty, A. , Treacy, P. , Fealy, G. , Phelan, A. , Lyons, I. , & Hall, P. (2012). Older people in residential care settings: Results of a National Survey of Staff‐Resident Interactions and Conflicts. Retrieved from University College Dublin: https://www.rte.ie/documents/news/elderlyreport.pdf [Google Scholar]
- Goergen, T. (2001). Stress, conflict, elder abuse and neglect in German nursing homes: A pilot study among professional caregivers. Journal of Elder Abuse & Neglect, 13(1), 1–26. 10.1300/J084v13n01_01 [DOI] [Google Scholar]
- Goergen, T. (2004). A multi‐method study on elder abuse and neglect in nursing homes. Journal of Adult Protection, 6(3), 15–25. 10.1108/14668203200400016 [DOI] [Google Scholar]
- Harris, D. K. , & Benson, M. L. (1998). Nursing home theft: The hidden problem. Journal of Aging Studies, 12(1), 57–67. [Google Scholar]
- Harris, D. K. , & Benson, M. L. (1999). Theft in nursing homes: An overlooked form of elder abuse. Journal of Elder Abuse & Neglect, 11(3), 73–90. 10.1300/J084v11n03_05 [DOI] [Google Scholar]
- Hirst, S. P. (2002). Defining resident abuse within the culture of long‐term care institutions. Clinical Nursing Research, 11(3), 267–284. 10.1177/10573802011003004 [DOI] [PubMed] [Google Scholar]
- Isola, A. , Backman, K. , Voutilainen, P. , & Rautsiala, T. (2003). Family members' experiences of the quality of geriatric care. Scandinavian Journal of Caring Sciences, 17(4), 399–408. 10.1046/j.0283-9318.2003.00246.x [DOI] [PubMed] [Google Scholar]
- Lachs, M. S. , & Pillemer, K. (2004). Elder abuse. Lancet, 364(9441), 1263–1272. 10.1016/S0140-6736(04)17144-4 [DOI] [PubMed] [Google Scholar]
- Lachs, M. S. , Williams, C. S. , O'Brien, S. , Pillemer, K. A. , & Charlson, M. E. (1998). The mortality of elder mistreatment. Journal of the American Medical Association, 280(5), 428–432. 10.1001/jama.280.5.428 [DOI] [PubMed] [Google Scholar]
- Malmedal, W. , Ingebrigtsen, O. , & Saveman, B. I. (2009). Inadequate care in Norwegian nursing homes – As reported by nursing staff. Scandinavian Journal of Caring Sciences, 23(2), 231–242. 10.1111/j.1471-6712.2008.00611.x [DOI] [PubMed] [Google Scholar]
- McCool, J. J. , Jogerst, G. J. , Daly, J. M. , & Xu, Y. (2009). Multidisciplinary reports of nursing home mistreatment. Journal of the American Medical Directors Association, 10(3), 174–180. 10.1016/j.jamda.2008.09.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDonald, L. , Beaulieu, M. , Harbison, J. , Hirst, S. , Lowenstein, A. , Podnieks, E. , & Wahl, J. (2012). Institutional abuse of older adults: What we know, what we need to know. Journal of Elder Abuse & Neglect, 24(2), 138–160. 10.1080/08946566.2011.646512 [DOI] [PubMed] [Google Scholar]
- Mokkink, L. B. , de Vet, H. C. W. , Prinsen, C. A. C. , Patrick, D. L. , Alonso, J. , Bouter, L. M. , & Terwee, C. B. (2018). COSMIN Risk of bias checklist for systematic reviews of patient‐reported outcome measures. Quality of Life Research, 27(5), 1171–1179. 10.1007/s11136-017-1765-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore, S. (2017). Abuse of residents in nursing homes: results of a staff questionnaire. Nursing Times, 113(2), 29–33. [Google Scholar]
- Natan, M. B. , Lowenstein, A. , & Eisikovits, Z. (2010). Psycho‐social factors affecting elders' maltreatment in long‐term care facilities. International Nursing Review, 57, 113–120. 10.1111/j.1466-7657.2009.00771.x [DOI] [PubMed] [Google Scholar]
- Neuberg, M. , Zeleznik, D. , Mestrovic, T. , Ribic, R. , & Kozina, G. (2017). Is the burnout syndrome associated with elder mistreatment in nursing homes: Results of a cross‐sectional study among nurses. Arhiv Za Higijenu Rada I Toksikologiju, 68(3), 190–197. 10.1515/aiht-2017-68-2982 [DOI] [PubMed] [Google Scholar]
- Pillemer, K. , Burnes, D. , Riffin, C. , & Lachs, M. S. (2016). Elder abuse: global situation, risk factors and prevention strategies. Gerontologist, 56(Suppl 2), 194–205. 10.1093/geront/gnw004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pillemer, K. , & Moore, D. W. (1989). Abuse of patients in nursing‐homes – Findings from a survey of staff. Gerontologist, 29(3), 314–320. 10.1093/geront/29.3.314 [DOI] [PubMed] [Google Scholar]
- Saveman, B. I. , Astrom, S. , Bucht, G. , & Norberg, A. (1999). Elder abuse in residential settings in Sweden. Journal of Elder Abuse & Neglect, 10(1–2), 43–60. 10.1300/J084v10n01_04 [DOI] [Google Scholar]
- Straus, M. A. (1979). Measuring intra‐family conflict and violence – Conflict tactics (Ct) scales. Journal of Marriage and the Family, 41(1), 75–88. 10.2307/351733 [DOI] [Google Scholar]
- Wang, J. (2004, October 31). Subtle psychological abuse of elderly in Taiwan. Annual report to National Science Council of Taiwan. Retrieved November 30, 2005, from http://nscnt13.nsc.gov.tw/NT56DOC/report/91/B/912314B242005.pdf
- Wang, J. J. (2005). Psychological abuse behavior exhibited by caregivers in the care of the elderly and correlated factors in long‐term care facilities in Taiwan. Journal of Nursing Research, 13(4), 271–280. 10.1097/01.JNR.0000387550.50458.bc [DOI] [PubMed] [Google Scholar]
- Wierucka, D. , & Goodridge, D. (1996). Vulnerable in a safe place: Institutional elder abuse. Canadian Journal of Nursing Administration, 9(3), 82–104. [PubMed] [Google Scholar]
- World Health Organization (2002). The Toronto Declaration on the global prevention of elder abuse. Retrieved from http://www.who.int/ageing/publications/toronto_declaration/en/ [Google Scholar]
- World Health Organization (2014). Global status report on violence prevention 2014. Retrieved from Geneva: https://www.who.int/violence_injury_prevention/violence/status_report/2014/en/ [Google Scholar]
- Yon, Y. , Mikton, C. R. , Gassoumis, Z. D. , & Wilber, K. H. (2017). Elder abuse prevalence in community settings: A systematic review and meta‐analysis. Lancet Global Health, 5(2), e147–e156. 10.1016/S2214-109X(17)30006-2 [DOI] [PubMed] [Google Scholar]
- Yon, Y. , Ramiro‐Gonzalez, M. , Mikton, C. R. , Huber, M. , & Sethi, D. (2019). The prevalence of elder abuse in institutional settings: A systematic review and meta‐analysis. European Journal of Public Health, 29(1), 58–67. 10.1093/eurpub/cky093 [DOI] [PMC free article] [PubMed] [Google Scholar]