

Dear Sir,
Lithopedion is a very rare condition and refers to an ectopic pregnancy that evolves to fetal death and calcification.[1] Most patients are asymptomatic and diagnosis is usually made incidentally on imaging studies.
We report a case of 80-year-old female who was presented with the complaint of right hip pain after a ground level fall. The pelvis radiograph demonstrated a right basicervical femoral neck fracture and incidentally showed a large abdominopelvic calcified mass. The abdominal radiograph AP view revealed a large irregular calcified mass with heterogeneous density and bony structures [Figure 1]. Abdominal and pelvic computed tomography (CT) revealed a mummified fetus, depicting in great detail the fetal anatomy [Figure 2]. The calcified mass was in close contact with abdominal organs, showing adherences to the bladder wall. It was 19 × 17 × 10 cm in size and femur length was 6.7 cm, with an estimated gestational age of 34–35 weeks.
Figure 1.

Abdominal radiograph AP view depicts a large calcified heterogeneous mass in the lower abdominal region, corresponding to a lithopedion, whose maximum length was 19 cm. A right basicervical femoral fracture is also visible
Figure 2.
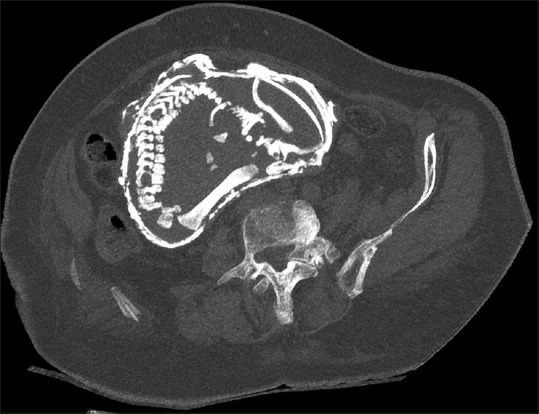
CT MIP reconstructions reveal the fetal anatomy in great detail, showing the calcified shell and fetus’ spine
Owing to the advanced age of the patient and because she was asymptomatic, it was decided that the calcified fetus should be left in place and no further surgery would be recommended. Subsequently, a total right hip arthroplasty was performed.
Lithopedion, from the Greek words lithos (stone) and paedion (child), is the term used to describe an abdominal ectopic pregnancy in which the fetus dies but cannot be reabsorbed by the mother's body. The dead fetus is retained in the abdominal cavity, forming a calcium shell around it. It is a very infrequent condition and occurs in only 0.0054% of all gestations.[2] This rare condition was first described in the 10th century[3] and there are only about 330 reported cases in medical literature.[4]
Lithopedion has been described in women ranging in age from 23 to 100 years old, with two thirds of them being over 40 years old. The period of fetus retention was from 4 to 60 years.[1] In this case, the exact retention period is unknown, but it is reasonable to think that it could be at least 40 years.
Most cases remain asymptomatic and represent incidental findings on imaging studies, surgery or necropsy.[3] An abdominal radiograph is useful to suggest or confirm diagnosis. Computed tomography and magnetic resonance imaging are able to reach a conclusive diagnosis[5] and allow further characterization of the mass, help the diagnosis of adherence, define the involvement of adjacent structures and estimate the fetal gestational age by measuring the femoral length.
In this clinical case, computed tomography allowed us to confirm the diagnosis, providing a clear visualization of the fetal anatomy, size and estimated gestational age. It also showed adherences between the calcified fetus and bladder wall.
Treatment of these patients should be individualized, considering patient age, comorbidities, symptoms, and imaging findings like size, location, and possible adherences to adjacent structures. It is necessary to evaluate the risk/benefit relationship of an operative approach in these cases. In this particular case, it was considered that the risk of excision overcame its benefits, so the lithopedion was left in place.
Lithopedion is really rare nowadays, due to medical and pre-natal care becoming more accessible to the population, with the possibility of early diagnosis and treatment of the pathology.[5] This case reflects the precarious medical attention in vulnerable populations.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Misra P, Bastia BK, Deep N, Rao M, Jena SK. Lithopaedion evolution of an abdominal siamese twin pregnancy-a rare case report. Indian J Radiol Imaging. 2006;16:813–4. [Google Scholar]
- 2.Medhi R, Nath B, Mallick MP. Lithopedion diagnosed during infertility workup: A case report. Springerplus. 2014;3:151. doi: 10.1186/2193-1801-3-151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lachman N, Satyapal KS, Kalideen JM, Moodley TR. Lithopedion: A case report. Clin Anatomy. 2001;14:52–4. doi: 10.1002/1098-2353(200101)14:1<52::AID-CA1009>3.0.CO;2-H. [DOI] [PubMed] [Google Scholar]
- 4.Rutten C, Khadam L, Picamoles P, Fokou-soh RM, Alperin E, Belaidi N. Lithopedion developed in a non-communicating rudimentary uterine horn: CT features. Diagn Interv Imaging. 2017;98:817–8. doi: 10.1016/j.diii.2017.04.007. [DOI] [PubMed] [Google Scholar]
- 5.Ramos-Andrade D, Ruivo C, Portilha MA, Brito JB, Caseiro-Alves F, Curvo-Semedo L. An unusual cause of intra-abdominal calcification: A lithopedion. Eur J Radiol Open. 2014;1:60–3. doi: 10.1016/j.ejro.2014.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]