

Abstract
Purpose:
Modified ride-on cars have emerged as an early powered mobility option for young children with disabilities. The purpose of this study was to identify, extract, and synthesize perceived barriers of modified ride-on car use reported in previous studies.
Methods:
This study was descriptive using a qualitative content analysis of previously published studies identified from a systematic literature search.
Results:
Categories of perceived barriers were identified: device, environmental, child-related perceived barriers regarding health, tolerance, and abilities, and caregiver-related perceived barriers regarding physical requirements, time, and motivation. Device and environmental perceived barriers were the most reported.
Conclusions:
Pediatric physical therapists play a critical role in working with families to promote their self-efficacy for using the modified ride-on car, and their capacity for overcoming the inherent difficulties associated with use. Most of the reported perceived barriers are modifiable, at least to some degree, with likely impacts on modified ride-on car use.
Introduction
The U.S. Department of Health and Human Services estimates that 7% of children ages 3 to 17 experience developmental disabilities.1 Many conditions, such as spina bifida, Down syndrome, and cerebral palsy, affect children’s ability to move and engage in self-directed mobility. Self-directed mobility is defined as mobility that is controlled by an individual and may include (a) ambulation (e.g., crawling, walking), (b) use of non-powered technology (e.g., prosthetics, walking aids, manual wheelchairs), or (c) use of powered technology (e.g., motorized wheelchairs, battery-powered ride-on toy cars).2 The use of battery-powered modified ride-on cars is an example of the recent advances in powered mobility technology that supports the engagement of children with developmental disabilities in self-directed mobility and social play.3–14 Families engage in a wide variety of amounts of car use, and a large range of adherence to recommended use. 2,5,6,11 There is a critical need to understand the reasons why modified ride-car use and adherence are varied and low compared to recommended levels. This study will address this critical need through identifying, extracting, and synthesizing perceived barriers of modified ride-on car use reported in previous studies.
Environmental inaccessibility and device characteristics of motorized wheelchairs are two of the most frequently reported barriers to use by children and families.15–17 Environmental inaccessibility includes inadequate space within the home and community settings, such as narrow store aisles or inaccessible bathrooms, lack of curb cuts on sidewalks, and rough and uneven outdoor surfaces.16 Device characteristics of motorized wheelchairs have been reported to include high cost, large size, and transportation requirements, as well as the inability of the device to navigate or handle varying terrain.15, 16 For example, Berry and colleagues (1996) examined use of motorized wheelchairs by 36 children aged 5-years and older, and found that only 57% of families had a van to transport the chair, and not all of the vans had a lift for ease of use.17 Furthermore, 9% of children never used the chairs. Similarly, Østensjø et al. (2005) reported that 9% of assistive devices owned by 96 children with cerebral palsy were not used at all.18 Researchers also report ongoing stigma associated with motorized wheelchairs, and in some cases children cite bullying and physical aggression from peers.18–20 A new and/or improved solution is needed in order for powered mobility devices to be effectively used by young children with developmental disabilities in their homes and communities.
Modified ride-on cars may address some of the previously reported barriers of environmental inaccessibility, financial burden, and device characteristics (e.g., large size and transportation requirements) of motorized wheelchairs. Commercially available, battery-powered, ride-on cars are modified by installing a large, accessible activation switch on the steering wheel. Common materials, such as polyvinyl chloride (PVC) pipe, swimming kickboards, and Velcro, are used to build a customized seating system for support (Figure 1). Modified ride-on cars are lower cost (between $70-$400), lighter, and easier to transport than motorized wheelchairs.15 Further, modified ride-on cars are a feasible and fun option to facilitate positive outcomes and behaviors for young children with developmental disabilities.2–8,11–14
Figure 1.

Example of a child using a modified ride-on car.
It is important that young children with developmental disabilities are provided access to modified ride-on cars in order to potentially experience advances in development. However, assessment of intervention effectiveness has been limited by low fidelity to the intervention protocol, prompting a need to better understand perceived barriers associated with modified ride-on car use. Interventions prescribing 20-minutes of use per day, for 5 days a week, over a 3-month period (i.e. 1,200 minutes of total use), indicated a wide variety of total use (range: 120-2,210 minutes) and adherence rates (10-100%).2,5,6 Additionally, a sit-to-stand modified ride-on car intervention that recommended at least 8 minutes per day, 5 days per week of use over a nine-month intervention (i.e. 1,440 minutes total use), also reported a wide variety of total use (range: 31-1,156 minutes) and adherence rates (2-64%), despite a lower recommended dosage.11
Because appropriate and impactful dosage of mobility interventions is key to providing optimal and evidence-based care, it is important to understand perceived barriers to modified ride-on car use in the home and community. This is especially important given the increasingly resource-limited environment of contemporary clinical practice. No previous studies have examined in detail the perceived barriers to modified ride-on car use of young children with developmental disabilities. The purpose of this study was to identify, extract, and synthesize perceived barriers of modified ride-on car use reported in previous studies. This work will inform future research and may have an impact on clinical practice given the role that pediatric physical therapists play in the provision of powered mobility devices, including modified ride-on cars. An understanding of perceived barriers may facilitate the development of specific strategies that pediatric physical therapists can implement to support families upon receipt of a modified ride-on car.
Method
Research Design
This study was descriptive using a qualitative content analysis of previously published studies identified from a systematic literature search to achieve the purpose of the study. 21–23
Sampling Strategy & Data Collection
We conducted a systematic search of literature to identify previously reported perceived barriers to modified ride-on car use. Key search terms included: ‘child’, ‘ride on car’, and ‘toy car’. The following databases were searched for relevant articles: Academic Search Premier, PubMed, and Web of Science. The first 100 results of each search were reviewed. Relevant journals and article reference lists were manually searched. The literature search was completed on April 22nd, 2019. Articles were included if they met the following criteria: (1) Full-text available in English; (2) a powered, toy-based ride-on car was provided to children of any age; (3) published in a peer-reviewed journal; (4) empirical data were collected (i.e. technical reports, commentaries, or reviews were not included); and (5) at least one perceived barrier of modified ride-on car use was reported. Articles were reviewed for relevance and consensus by the first and second authors. There were 11 studies that met the inclusion criteria and were included for analysis (Figure 2).
Figure 2.
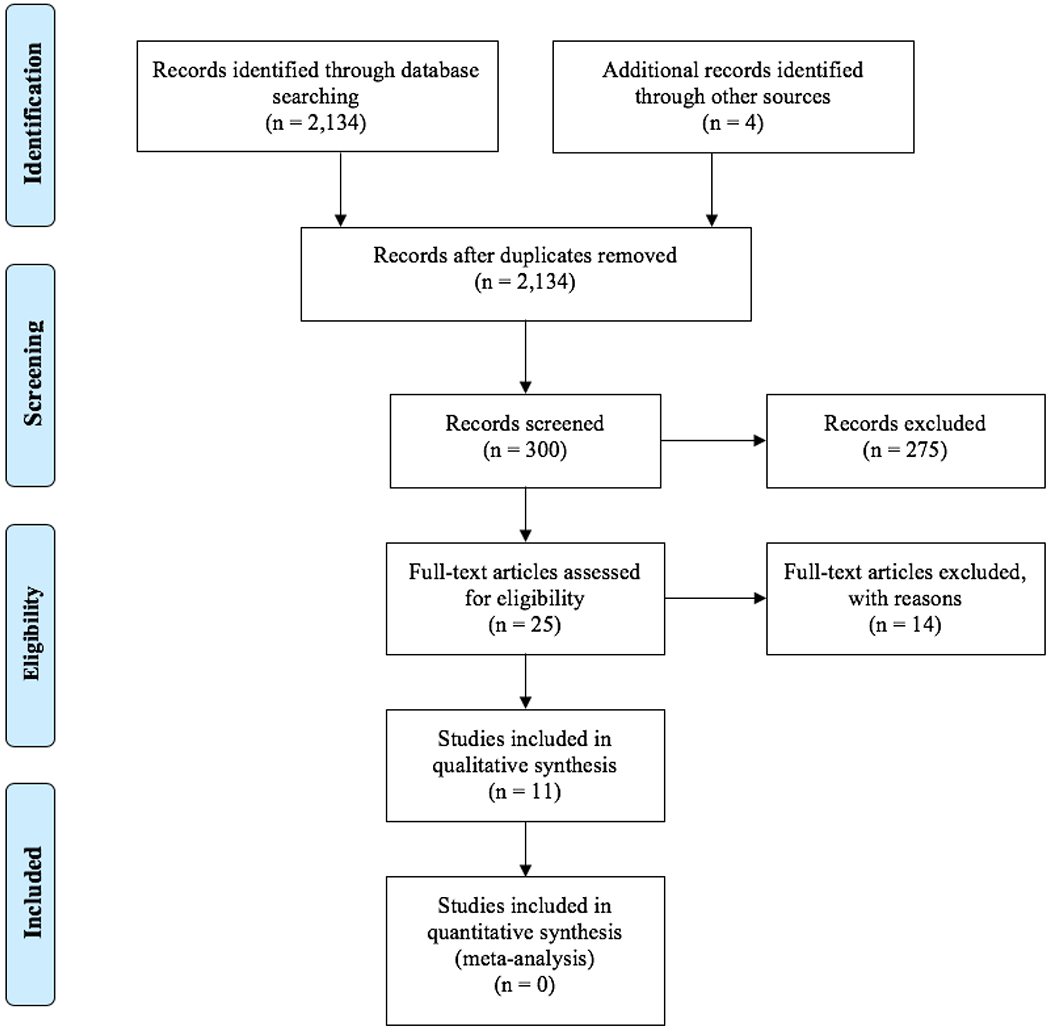
Results of systematic literature search based on PRISMA statement.
Data Analysis
A content analysis was completed to determine frequencies and percentages of perceived barriers of modified ride-on car use reported in previously published research studies. This was an iterative process as recommended for descriptive studies.23 Our description of data analysis is based on the work of Bradley, Curry, and Devers (2007).24
Reading for overall understanding. The first and second authors independently read through the 11 of the included studies in order to gain a deeper understanding of the participants’ experience with modified ride-on cars. Developing the code structure. This process was an iterative and inductive. The first and second authors independently identified and extracted perceived barriers reported in previous studies and drafted an initial code structure. The first and second authors collaboratively examined their code structures and revised based on discussion. This process was repeated until 100% agreement was obtained for the identification and definition of conceptual codes and subcodes (Table 1). Applying the finalized code structure. The first and second authors re-reviewed the 11 studies and systematically identified and extracted perceived barriers to ensure that all data was captured. Initial comparison resulted in >95% agreement of identification and extraction of perceived barriers. Disagreements were resolved via discussion until 100% of agreement was reached. The first, second, and sixth authors applied the final code structure to the extracted perceived barriers. Initial comparison resulted in >95% agreement of coding the extracted perceived barriers based on conceptual codes and subcodes. Disagreements were resolved via discussion until 100% of agreement was reached.
Table 1.
Definitions of Conceptual Codes and Subcodes of Perceived Barriers of Modified Ride-on Car Usage.
| Conceptual Codes | Definitions and Subcodes |
|---|---|
| Environmental | Any perceived barrier related to the environment. This may include the weather or the physical space. |
| Caregiver (includes families and clinicians) |
Subcode: Physical Requirements.
Any perceived barrier related to the physical effort or demand required
to transition a child in/out of the ride-on car, provide arm’s
length supervision, or assist with
steering. Subcode: Motivation. Any perceived barrier related to the caregiver’s decreased motivation to provide their child with opportunities to use a modified ride-on car. Subcode: Time. Any perceived barrier related to the lack of time to provide their child with opportunities to use a modified ride-on car. |
| Child |
Subcode: Health. Any perceived
barrier related to a child’s health that prevents them having
opportunities to use a modified ride-on car. Examples include sickness,
general fatigue, or recovery from surgery. Subcode: Tolerance. Any perceived barrier related to a child’s tolerance to using a modified ride-on car. Examples include child’s willingness, lack of enjoyment, negative responses to movement or the sound/acceleration of the modified ride-on car. Subcode: Ability. Any perceived barrier related to a child’s physical or cognitive ability to using modified ride-on car. Examples include a lack of trunk control, inability to steer, low vision, lack of understanding cause and effect. |
| Device | Any perceived barrier related to the characteristics of the modified ride-on car. Examples include size of steering wheel, size of the ride-on car, loud sound, duration of battery, or quick acceleration. |
Results
Content analysis identified a total of 43 perceived barriers reported in previous research studies (Table 2). The number and percent of perceived barriers in each category is in Figure 3. Device (25%) and environmental (19%) perceived barriers were the most frequently reported, followed by caregiver-related perceived barriers regarding: physical requirements (12%), time (9%), and motivation (9%), and child-related perceived barriers regarding: health (12%), tolerance (9%), and abilities (5%).
Table 2.
Extraction and Coding of Perceived Barriers from Previously Published Research Studies of Modified Ride-On Cars.
| Reference | Perceived Barriers | Assigned Code of Perceived Barrier |
|---|---|---|
| Chiulli (1988) | • Initial ‘lurch’ with activation | • Device |
| Deitz (2002) | • Family vacation • Child’s health • Loud • Disruptive when used indoors • Difficulty driving on rough surfaces • Large turning radius • Experienced frequent but solvable break downs • Impracticality of use in small classrooms/crowded spaces |
• Caregiver: Time • Child: Health • Device • Device • Device • Device • Device • Environmental |
| Huang, Ragonesi, Stoner, Peffley, & Galloway (2014) | • Weather • Child’s tolerance • Inability to install joystick to teach child to steer • Child’s health |
• Environmental • Child: Tolerance • Device • Child: Health |
| Logan, Huang, Stahlin, & Galloway (2014) | • Weather • Child’s tolerance • Child’s health (sickness, tired from multiple medical appointments, recovering from surgery) |
• Environmental • Child: Tolerance • Child: Health |
| Logan, Feldner, Galloway, & Huang (2016) | • Physical effort of clinical staff
involved in transition children in and out of ride-on
car • Physical exertion required for arm’s length supervision for safety • Physical demand required to assist with driving and positioning since car is low to the ground • Increased personnel demand to supervise car play sessions when researcher not present • Child’s health • Possible that cognitive delay contributed to requiring assistance to learn to drive independently • Difficulty in transferring children into appropriate modified ride-on cars to accommodate size, weight, and operational needs of the child’s ventilator |
• Caregiver:
Physical • Caregiver: Physical • Caregiver: Physical • Caregiver: Physical • Child: Health • Child: Abilities • Device |
| Ross et al. (2017) | • Steering was
difficult • Refusal of child • Adult supervision required for steering, transferring child in and out of device, avoiding obstacles • Disinterest, fatigue, and request to get out of device |
• Child: Ability • Child: Tolerance • Caregiver: Physical • Child: Tolerance |
| Feldner, 2018 | • Lack of space in
classroom • Noisy/disruptive in classroom • Expensive as out-of-pocket item • Large size • Family/therapist priority for child to walk as primary mode of mobility • Process of choosing a ride-on car • Community-based, decentralized process of modified ride-on car provision was frustrating at times |
• Environmental • Device • Device • Device • Caregiver: Motivation • Caregiver: Motivation • Caregiver: Motivation |
| Feldner, Logan, Galloway (2018) | • Difficult to use on playground woodchips | • Environmental |
| Huang, Chen, Huang, Shih, Hsieh, & Chen (2018) | • Child’s health
(sickness) • Family vacation |
• Child: Health • Caregiver: Time |
| Logan, Hospodar, Feldner, Huang, & Galloway (2018) | • Lack of space • Lack of time |
• Environmental • Caregiver: Time |
| Logan, Catena, Sabet, Hospodar, Yohn, Govindan, & Galloway, 2019 | • Weather • Lack of space • Lack of time • Decreased motivation for their child to drive once competence in switch activation was demonstrated |
• Environmental • Environmental • Caregiver: Time • Caregiver: Motivation |
Figure 3.
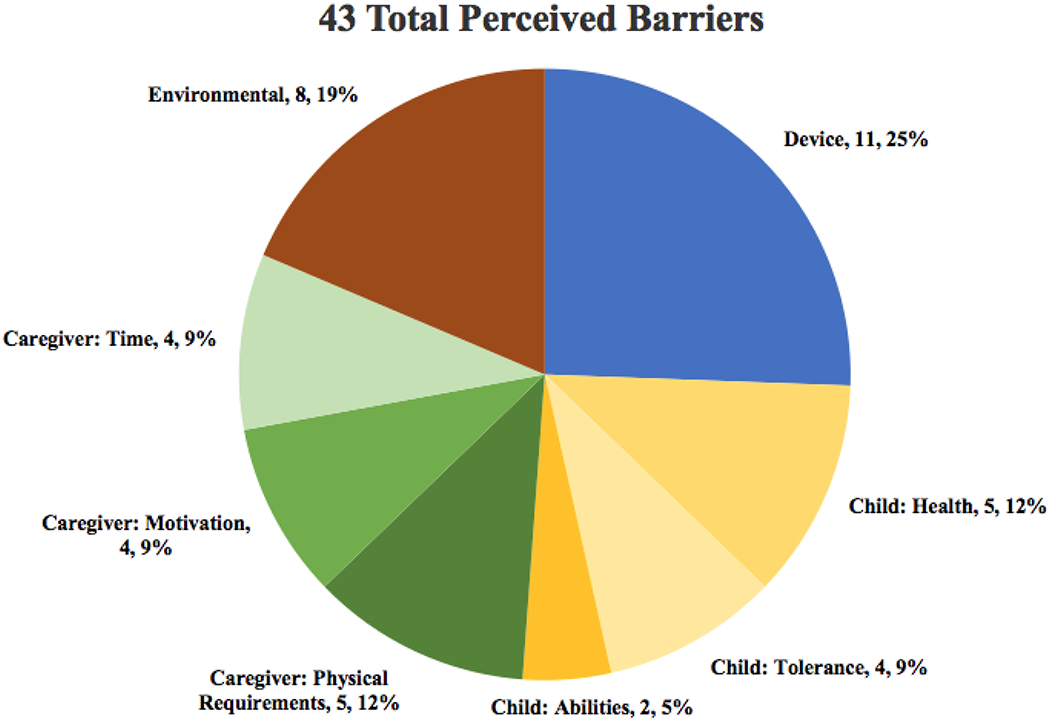
Visual representation of categorized perceived barriers of previously published research on modified ride-on cars. Frequencies and percentages reported for each category of perceived barrier.
Discussion
The purpose of this study was to identify, extract, and synthesize perceived barriers of modified ride-on car use reported in previous studies. The final coding structure in Table 1 may have broader implications beyond modified ride-on cars, and may be applied to other powered mobility devices, such as motorized wheelchairs and may be useful in clinical practice. We suggest that, with the exception of the child’s health, all of the perceived barriers outlined in Table 1 are modifiable, at least to some degree, with likely impacts on modified ride-on car use. For example, social cognitive theorists posit a bi-directional causality between the person, behavior, and environment, whereby influencing one determinant will influence the others.25 Applying this knowledge to modified ride-on car use, strategies to change the environmental context in which children use the technology (e.g., covered playgrounds, industrial/wholesale grocery stores) might help ameliorate identified barriers (e.g., weather), thereby producing positive behavioral (e.g. increased modified ride-on car use) and developmental outcomes for children.
Device and environmental perceived barriers were the most commonly reported perceived barriers for use of modified ride-on cars, and it is likely that these perceived barriers are interrelated. For example, 50% of the environmental perceived barriers were related to lack of space. Modified ride-on cars may be difficult to use within the living spaces and hallways of most homes. From a clinical perspective, modified ride-on car use within a home, despite limited space for exploration depending upon the home, could still be important for a child, as it may yield developmental benefits.2–12 However, families may have reported space as a barrier if they preferred a wide-open area for modified ride-on car use, or if they perceived the scuffs and nicks that may occur from bumping into walls within the home as undesirable. It may be helpful to discuss with parents that while using modified ride-on cars for open exploration is important, there are other play-based activities involving goal-directed driving that may also be beneficial and feasible within the home.
Results of the current study align with previous research that reported device and environmental factors as common barriers to use of motorized wheelchairs.15–17 The specific perceived barriers of motorized wheelchairs and modified ride-on cars may be different depending upon design and function of each type of device. Modified ride-on cars are lightweight (typically less than 10 pounds) and do not require a van or specialized vehicle for transportation. Despite the portability of modified ride-on cars, it still requires effort from the family to transport the car from home to a community space, and there are no guarantees that the community space will be accessible for the car. Ride-on cars are typically modified with an easy-to-press activation switch installed on the steering wheel. This modification promotes easier activation of the ride-on car to make it ‘go’, but this type of switch activation does not improve the turning radius of the ride-on car, which is often quite wide and not highly compatible with small indoor living spaces. Motorized wheelchairs are typically activated via a proportional speed-control joystick that provides 360 degrees of turning radius and an ability to easily move in and out of small spaces, which may be more compatible with most indoor living spaces. Further, the intent of each device is unique, with modified ride-on cars serving as an early or transitional device, while a motorized wheelchair is typically a more permanent mobility solution. Therefore, while modified ride-on cars and motorized wheelchairs both provide access to self-directed mobility, each device may present unique perceived barriers based on design and function.
Several of the categories of perceived barriers, such as a child’s tolerance and ability, may be modifiable through interventions and education delivered by pediatric physical therapists. Pediatric physical therapists could address the family’s capacity for overcoming the inherent difficulties associated with a child’s tolerance to use the modified ride-on car. For example, due to the noise and quick acceleration of the modified ride-on car, there are often initial, negative reactions from children such as crying or frustration. These initial and negative reactions may lead families to subsequently provide their child with less access to the modified ride-on car. Pediatric physical therapists can reassure families that these initial negative reactions happen frequently and does not mean that their child will never enjoy using a modified ride-on car. Pediatric physical therapists can offer valuable insight regarding expectation setting and contingency planning for how to continue use of the modified ride-on car while experiencing these perceived barriers. Another perceived barrier that may be modifiable includes a child’s abilities. Pediatric physical therapists are experts in providing optimal seating support in a modified ride-on car. This may address one aspect of a child’s ability level as a perceived barrier (i.e. lack of trunk control). Pediatric physical therapists and families can collaborate to brainstorm new and interesting activities for the child to engage in that may elicit an understanding of cause and effect that was not previously demonstrated. Pediatric physical therapists can provide valuable learning strategies to families regarding how to scaffold their child’s learning to activate the modified ride-on car and transition from open exploration to goal-directed driving based on each child’s ability level.
Pediatric physical therapists could address some of the caregiver-related perceived barriers through promoting their self-efficacy for using the modified ride-on car, and their capacity for overcoming the inherent difficulties associated with modified ride-on car use. For example, supplementary modifications to the ride-on car such as addition of a PVC handle on the back of the car can provide caregivers with a means to assist with steering to address the caregiver-related perceived barrier of physical requirements. This modification is simple and would decrease the physical requirement of a caregiver constantly bending down to assist with steering. An example of addressing the caregiver-related perceived barrier of time includes providing families with a gradual goal setting plan that increases over time. Families and pediatric physical therapists can work together to create an initial weekly goal of how much to use the modified ride-on car during the first week of use. This goal should be attainable in order to begin to facilitate self-efficacy for the caregivers that they are able to provide opportunities for the child to use the modified ride-on car. Over time, the weekly goal of modified ride-on car use can increase gradually. This type of goal setting is more likely to promote self-efficacy and continued use of the modified ride-on car, as opposed to setting unrealistic initial expectations that lead to eventual abandonment of the car. Lastly, an example to address the caregiver-related perceived barrier of motivation may include education. Education could include discussion of the relevant research related to the potential benefits of modified ride-on car use for young children with developmental disabilities. Exposure to the available clinical evidence may motivate families to provide their child with more opportunities to use the modified ride-on car.
There were strengths and limitations of the current study. A strength is that this is the first study to synthesize previous literature on perceived barriers of modified ride-on cars. Another strength is the development of a coding structure to identify and define perceived barriers related to modified ride-on car use (Table 1). This coding structure presents an opportunity for future work to potentially intervene upon perceived barriers. For example, an intervention could be developed that includes parent education and training about strategies to overcome commonly reported perceived barriers. Weather and inadequate space are often reported as environmental perceived barriers. Parents could be provided with information of covered playgrounds and indoor community spaces where modified ride-on cars could be used more easily than in a family’s home or outside during inclement weather. Another example are the reported perceived barriers of a child’s inability to steer or the caregiver’s physical effort required to assist with steering. An additional modification includes making the ride-on car controllable via a remote control. This would assist both the caregiver and the child with steering. Our lab is currently developing an intervention to address perceived barriers of modified ride-on car use. This is important because adherence to the recommended levels of modified ride-on car use is critical in order to examine dose/response relationships between car use and developmental outcomes, which will further inform evidence-based clinical practice.
A limitation of the current study is that none of the included studies specifically assessed perceived barriers to modified ride-on car use. This may have prevented a deeper analysis of the perceived barriers to develop themes around participants’ experiences. For example, it is unclear the relationship between environmental perceived barriers. It is likely that an apartment or small home (inadequate space) in combination with living in an area with frequent inclement weather (i.e. extreme temperatures, rainy, etc.) results in less modified ride-on car use compared to other families without these circumstances. It remains unknown the relationship between the different types of perceived barriers identified and defined in the coding structure. It is also possible that families experienced other perceived barriers that were not reported in previous studies. Future research could examine families’ perceived barriers to modified ride-on car use before and after obtaining a car for their child. This information would be useful in understanding how perceived barriers may change over time.
What this case adds to evidence-based practice
It is important for pediatric physical therapists to be aware of the potential perceived barriers that families may experience in regard to young children with developmental disabilities using modified ride-on cars or other powered mobility devices, such as motorized wheelchairs. Pediatric physical therapists play a critical role in working with families and children upon initial receipt of a modified ride-on car to ensure the family is educated about recommended driving dosage, mitigation of commonly identified barriers, and the varied responses children may exhibit upon their first or several initial driving sessions. Pediatric physical therapists may promote greater use of devices if perceived barriers are known and addressed through education, when possible.
Footnotes
Conflicts of Interest and Sources of Funding:
The authors declare no conflict of interest. This work was supported by the John C. Erkkila, M.D. Endowment for Health and Human Performance, Corvallis, Oregon; and Oregon State University’s Joint Interdisciplinary Research Program, Corvallis, Oregon. Additionally, Dr. Feldner's time was supported by the NIH National Center for Advancing Translational Science KL2 TR002317. The funding sources were not involved in the study design, data collection, analyses and interpretation of data, the writing of the report, nor the decision to submit the article for potential publication.
References
- 1.Zablotsky B, Black LI, Blumberg SJ. Estimated prevalence of children with diagnosed developmental disabilities in the United States, 2014–2016 NCHS Data Brief, no 291 Hyattsville, MD: National Center for Health Statistics; 2017. Retrieved from https://www.cdc.gov/nchs/data/databriefs/db291.pdf [PubMed] [Google Scholar]
- 2.Logan SW, Hospodar CM, Feldner HA, Huang H-H, Galloway JC. Modified ride-on car use by young children with disabilities: Pediatr Phys Ther. 2018;30(1):50–56. doi: 10.1097/PEP.0000000000000468. [DOI] [PubMed] [Google Scholar]
- 3.Huang HH, Chen CL. The use of modified ride-on cars to maximize mobility and improve socialization-a group design. Res Dev Disabil. 2017;61:172–180. doi: 10.1016/j.ridd.2017.01.002. [DOI] [PubMed] [Google Scholar]
- 4.Huang H-H, Chen Y-M, Huang H-W, Shih M-K, Hsieh Y-H, Chen C-L. Modified ride-on cars and young children with disabilities: effects of combining mobility and social training. Front Pediatr. 2018;5. doi: 10.3389/fped.2017.00299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Huang HH, Ragonesi CB, Stoner T, Peffley T, Galloway JC. Modified toy cars for mobility and socialization: case report of a child with cerebral palsy. Pediatr Phys Ther. 2014;26(1):76–84. doi: 10.1097/PEP.0000000000000001. [DOI] [PubMed] [Google Scholar]
- 6.Logan SW, Huang H-H, Stahlin K, Galloway JC. Modified ride-on car for mobility and socialization: single-case study of an infant with down syndrome. Pediatr Phys Ther. 2014;26(4):418–426. doi: 10.1097/PEP.0000000000000070. [DOI] [PubMed] [Google Scholar]
- 7.Logan SW, Feldner HA, Galloway JC, Huang H-H. Modified ride-on car use by children with complex medical needs. Pediatr Phys Ther. 2016;28(1):100–107. doi: 10.1097/PEP.0000000000000210 [DOI] [PubMed] [Google Scholar]
- 8.Ross SM, Catena M, Twardzik E, et al. Feasibility of a modified ride-on car intervention on play behaviors during an inclusive playgroup. Phys Occup Ther Pediatr. 2018;38(5):493–509 doi: 10.1080/01942638.2017.1400491. [DOI] [PubMed] [Google Scholar]
- 9.Feldner H Impacts of early powered mobility provision on disability identity: A case study. Rehabil Psychol. 2018. doi: 10.1037/rep0000259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Feldner HA, Logan SW, Galloway JC. Mobility in pictures: a participatory photovoice narrative study exploring powered mobility provision for children and families. Disabil Rehabil Assist Technol. 2018;1–11. doi: 10.1080/17483107.2018.1447606. [DOI] [PubMed] [Google Scholar]
- 11.Logan SW, Catena MA, Sabet A, Hospodar CM, Yohn H, Govindan A, Galloway JC. Standing tall: feasibility of a modified ride-on car that encourages standing. Pediatr Phys Ther. 2019;31(1):E6–E13. doi: 10.1097/PEP.0000000000000568. [DOI] [PubMed] [Google Scholar]
- 12.Logan SW, Lobo MA, Feldner HA, et al. Power-up: exploration and play in a novel modified ride-on car for standing. Pediatr Phys Ther. 2017;29(1):30–37. doi: 10.1097/PEP.0000000000000336. [DOI] [PubMed] [Google Scholar]
- 13.Chiulli C, Corradi-Scalise D, Donatelli-Schultheiss L. Powered mobility vehicles as aids in independent locomotion for young children: Suggestions from the field. Phys Ther, 1988;68(6):997–999. [DOI] [PubMed] [Google Scholar]
- 14.Deitz J, Swinth Y, White O. Powered mobility and preschoolers with complex developmental delays. Am J Occup Ther. 2002;56(1):86–96. doi: 10.5014/ajot.56.1.86. [DOI] [PubMed] [Google Scholar]
- 15.Feldner HA, Logan SW, Galloway JC. Why the time is right for a radical paradigm shift in early powered mobility: the role of powered mobility technology devices, policy and stakeholders. Disabil Rehabil Assist Technol. 2016;11(2):89–102. doi: 10.3109/17483107.2015.1079651. [DOI] [PubMed] [Google Scholar]
- 16.Jones MA, McEwen IR, Neas BR. Effects of power wheelchairs on the development and function of young children with severe motor impairments. Pediatr Phys Ther. 2012;24(2):131–140. doi: 10.1097/PEP.0b013e31824c5fdc. [DOI] [PubMed] [Google Scholar]
- 17.Berry ET, McLaurin SU, & Sparling JW. Parent/caregiver perspectives on the use of power wheelchairs. Pediatr Phys Ther. 1996;8:146–150. [Google Scholar]
- 18.Østensjø S, Carlberg EB, Vøllestad NK. The use and impact of assistive devices and other environmental modifications on everyday activities and care in young children with cerebral palsy. Disabil Rehabil. 2005;27(14):849–861. doi: 10.1080/09638280400018619. [DOI] [PubMed] [Google Scholar]
- 19.Gudgeon S, Kirk S. Living with a powered wheelchair: exploring children’s and young people’s experiences. Disabil Rehabil Assist Technol. 2015;10(2):118–125. doi: 10.3109/17483107.2013.870609. [DOI] [PubMed] [Google Scholar]
- 20.McMaugh A En/countering disablement in school life in Australia: children talk about peer relations and living with illness and disability. Disabil Soc. 2011;26(7):853–866. doi: 10.1080/09687599.2011.618740. [DOI] [Google Scholar]
- 21.Knafl KA, Webster DC. Managing and analyzing qualitative data. A description of tasks, techniques and materials. Western J Nurs Res. 1988;10:195–218. [DOI] [PubMed] [Google Scholar]
- 22.Thorne S Interpretive description (1st ed.). 2008. Walnut Creek, CA: Left Coast Press. [Google Scholar]
- 23.Thorne S, Kirkham SR, MacDonald-Emes J. Interpretive description: A noncategorical qualitative alternative for developing nursing knowledge. Res Nurs & Health. 1997;20(2):169–177. [DOI] [PubMed] [Google Scholar]
- 24.Bradley EH, Curry LA, Devers KJ. Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Res Edu Trust. 2007;42(4):1758–1772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bandura A Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall; 1986. [Google Scholar]