

Abstract
Background
Anxiety and depressive disorders are prevalent in adolescents and young adults. However, most young people with mental health problems do not receive treatment. Computerized cognitive behavior therapy (cCBT) may provide an accessible alternative to face-to-face treatment, but the evidence base in young people is limited.
Objective
The objective was to perform an up-to-date comprehensive systematic review and meta-analysis of the effectiveness of cCBT in treating anxiety and depression in adolescents and young adults compared with active treatment and passive controls. We aimed to examine posttreatment and follow-up effects and explore the moderators of treatment effects.
Methods
We conducted systematic searches in the following six electronic databases: PubMed, EMBASE, PsycINFO, CINAHL, Web of Science, and Cochrane Central Register of Controlled Trials. We included randomized controlled trials comparing cCBT with any control group in adolescents or young adults (age 12-25 years) with anxiety or depressive symptoms. The quality of included studies was assessed using the Cochrane risk-of-bias tool for randomized trials, version 2.0. Overall quality of evidence for each outcome was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Posttreatment means and SDs were compared between intervention and control groups, and pooled effect sizes (Hedges g) were calculated. Random-effects meta-analyses were conducted using Comprehensive Meta-Analysis software. Subgroup analyses and meta-regression analyses were conducted to explore whether age, guidance level, and adherence rate were associated with treatment outcome.
Results
The search identified 7670 papers, of which 24 studies met the inclusion criteria. Most included studies (22/24) had a high risk of bias owing to self-report measures and/or inappropriate handling of missing data. Compared with passive controls, cCBT yielded small to medium posttreatment pooled effect sizes regarding depressive symptoms (g=0.51, 95% CI 0.30-0.72, number needed to treat [NNT]=3.55) and anxiety symptoms (g=0.44, 95% CI 0.23-0.65, NNT=4.10). cCBT yielded effects similar to those of active treatment controls regarding anxiety symptoms (g=0.04, 95% CI −0.23 to 0.31). For depressive symptoms, the nonsignificant pooled effect size favored active treatment controls (g=−0.70, 95% CI −1.51 to 0.11, P=.09), but heterogeneity was very high (I2=90.63%). No moderators of treatment effects were identified. At long-term follow-up, cCBT yielded a small pooled effect size regarding depressive symptoms compared with passive controls (g=0.27, 95% CI 0.09-0.45, NNT=6.58). No other follow-up effects were found; however, power was limited owing to the small number of studies.
Conclusions
cCBT is beneficial for reducing posttreatment anxiety and depressive symptoms in adolescents and young adults compared with passive controls. Compared with active treatment controls, cCBT yielded similar effects regarding anxiety symptoms. Regarding depressive symptoms, however, the results remain unclear. More high-quality research involving active controls and long-term follow-up assessments is needed in this population.
Trial Registration
PROSPERO CRD42019119725; https://tinyurl.com/y5acfgd9.
Keywords: cognitive behavior therapy, internet, anxiety, depression, youth, meta-analysis
Introduction
Anxiety and depressive disorders are common in children and adolescents [1,2]. Symptoms of anxiety and depression in childhood and adolescence predict a range of mental health problems later in life, including adult anxiety and depressive disorders and substance use disorders [3-8]. Moreover, anxiety and depressive disorders in young people are associated with an increased risk of self-harm and suicide [5,9], the second most common cause of death among youth aged between 10 and 24 years [10].
Among children and adolescents aged up to 18 years, global prevalence rates are estimated at 6.5% for anxiety disorders and 2.6% for depressive disorders [11]. The prevalence of mental disorders increases during the transition from childhood to adolescence [12,13], with prevalence rates in adolescents (ie, age 12-19 years) estimated at 10.7% for anxiety disorders and 6.1% for depressive disorders [13]. The incidence of most anxiety disorders peaks during adolescence, whereas the incidence of depressive disorders starts to rise during adolescence [14] and peaks in young adulthood (ie, age 19-25 years) [15-17]. Given the high incidence and burden of anxiety and depressive disorders in young people, early intervention in both adolescents and young adults is of utmost importance.
Adolescents and young adults with anxiety or depressive disorders are commonly treated with cognitive behavioral therapy (CBT), which is a widely-used treatment that has been proven to be effective in this population [18-21]. However, the majority of adolescents and young adults with mental health problems do not receive treatment [22-25]. Among their reasons for low treatment utilization are limited availability of youth mental health services, perceived stigma associated with mental illness, perceived lack of time or resources, and preference for self-help [24,26,27]. These barriers to treatment utilization may partly be overcome by computerized mental health interventions involving psychological treatment delivered via the internet and/or digital devices. Compared with face-to-face treatment, computerized interventions may provide more flexible access in terms of time, location, and availability; greater privacy and anonymity; and more independence [28,29]. The internet is ubiquitous in the lives of young people, who have shown positive attitudes toward computerized mental health interventions [30]. Therefore, computerized treatment provides an accessible and feasible alternative to face-to-face treatment for this group [31,32].
Numerous randomized controlled trials (RCTs) and meta-analyses in adult populations with anxiety and depressive disorders have shown that CBT may be effectively delivered via the internet or digital devices [33,34]. The effects of these so-called computerized CBT (cCBT) interventions have been demonstrated to be comparable to the effects of face-to-face CBT in adults [35]. In children and young people, cCBT has been found to be effective in treating mental health problems as well [36-42]. Despite these promising results, however, the evidence base on cCBT in young people remains limited compared with research in adults. The number of studies is still small, and the quality of RCTs is often low [39].
To date, three meta-analyses have shown cCBT [36,37] and internet-based mental health interventions [43] to be effective in reducing anxiety and depressive symptoms in young people aged 12 to 25 years. Ebert et al [36] found cCBT to be superior to passive control conditions for both anxiety (g=0.68, 95% CI 0.45-0.92, P<.001; k=7) and depression (g=0.76, 95% CI 0.23-2.66, P<.001; k=4). Active control conditions were not included in their meta-analysis. Similarly, Pennant et al [37] found positive effects of cCBT on both anxiety (standardized mean difference [SMD]=−0.77, 95% CI −1.45 to −0.09, k=6) and depression (SMD=−0.62, 95% CI −1.13 to −0.11, k=7) compared with passive controls. Compared with face-to-face CBT, their meta-analysis showed similar effects for cCBT on anxiety (SMD=−0.04, 95% CI −0.36 to 0.28, P=.89; k=3), but a large effect in favor of face-to-face CBT on depression (SMD=1.65, 95% CI 0.88-2.41, P<.001; k=2). However, these meta-analyses included only a small number of studies that were all published up to 2013. A more recent meta-analysis in children and adolescents up to 18 years with depressive and/or anxiety symptoms showed that cCBT interventions yielded a medium effect size compared with waiting list controls (g=0.66, 95% CI 0.42-0.90, P<.001, k=17) [44]. This study reported neither separate effects of cCBT on depression and anxiety symptoms nor effects of cCBT compared with face-to-face CBT. Importantly, none of these meta-analyses reported mid-term or long-term effects [36,37,44].
To our knowledge, the study of Välimäki et al [43] is the only meta-analysis that not only reported posttreatment effects, but also described short-term and long-term follow-up effects. Posttreatment effects showed the positive effects of internet-based interventions on depressive symptoms (P=.02, median=1.68, 95% CI 0.25-3.11, k=10) and anxiety symptoms (P=.001, median=1.47, 95% CI 0.59-2.36, k=8) compared with any control group. The authors found significant long-term effects of internet-based interventions aimed at reducing depressive symptoms 6 months after treatment (P=.01, median=1.78, 95% CI 0.37-3.20, k=3), but no mid-term effects (ie, 3-5 months after treatment). Regarding anxiety symptoms, they found no mid-term effects in the only two available studies, and no study reported long-term results on anxiety [43]. However, their meta-analysis included both cCBT and various other internet-based mental health interventions (eg, positive psychology), and did not specifically analyze the effects of cCBT. Furthermore, the effects of internet-based interventions were not reported separately compared with active treatment controls and passive controls. In addition, the authors used a narrow search string, which did not include anxiety disorders or interventions aimed at decreasing anxiety symptoms. Hence, it remains unclear whether cCBT is effective in treating young people with anxiety and depressive disorders in the long term, compared with active treatment and passive controls.
In adults, individual participant data meta-analyses on internet-based interventions have demonstrated several predictors of better treatment outcomes, among which are older age [45] and higher treatment adherence [33]. In addition, level of guidance (ie, the level of therapist support provided during cCBT) appears to be associated with larger treatment effects in adults, as studies on guided internet-based interventions have generally demonstrated larger effect sizes than studies on unguided interventions [33,45,46]. Although previous meta-analyses on cCBT in children and young people have attempted to identify moderators of treatment effects, the results remain mixed. Some found evidence for a moderating role of age [36,37,42], whereas others did not [38,44]. With regard to guidance, evidence remains mixed as well [37,42,44]. To our knowledge, previous meta-analyses in young people did not examine whether treatment adherence is associated with cCBT effect sizes.
Research on cCBT in young people with anxiety or depressive symptoms is a rapidly developing field, and all previous meta-analyses are limited to studies of at least 2 years old [36-38,43,44]. In addition, the most recent meta-analyses focused on other age groups [38,41,42,44] or did not separately report effects for either anxiety and depressive disorders [38,44] or cCBT [43]. Moreover, the follow-up effects of cCBT remain largely unknown. Lastly, since most previous meta-analyses in young people did not separately compare cCBT to active treatment and passive controls [36,43], it remains unclear whether cCBT provides an effective alternative to face-to-face treatment in this group. Therefore, our objective was to provide an up-to-date comprehensive systematic review and meta-analysis of the effectiveness of cCBT in treating anxiety and depressive symptoms in adolescents and young adults compared with active treatment and passive control groups, differentiating between posttreatment, short-term follow-up, and long-term follow-up. Furthermore, we aimed to explore whether age, guidance level, and treatment adherence are associated with treatment outcome by conducting subgroup analyses and meta-regression analyses.
Methods
Design
This study was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement for reporting systematic reviews and meta-analyses [47]. The systematic review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO, registration number: CRD42019119725).
Search Strategy
We conducted a comprehensive literature search in the following six electronic databases from database inception to September 13, 2019: PubMed, EMBASE, PsycINFO, CINAHL, Web of Science, and Cochrane Central Register of Controlled Trials (CENTRAL). An information specialist was consulted for the search. The search strategy included combinations of relevant medical subject headings and text-based search terms covering computerized (or internet, digital, eHealth, online, smartphone, or web-based), CBT (or cognitive, behavior, therapy, treatment, or intervention), and adolescent (or child, young person, teenager, or youth). The complete search strings are documented in Multimedia Appendix 1. In addition, we manually searched reference lists of included studies and relevant previous reviews, and searched international trial registers for eligible studies, which resulted in one additional record.
Study Selection
We included RCTs in which computer-based, internet-based, or smartphone-based cognitive behavioral therapy targeting anxiety, depression, or both was compared to an active treatment control condition or passive control condition. The study population involved adolescents or young adults with a mean age between 12 and 25 years and elevated symptoms of anxiety or depressive disorder (ie, either a formal diagnosis or an elevated score on a standardized self-report measure representing at least a mild-to-moderate symptom level). We only included studies with an English abstract available, those that were published in peer-reviewed journals or were PhD theses, and those that contained outcome data on a continuous anxiety or depressive symptom measure that allowed for calculation of effect sizes. If effect sizes could not be calculated, authors were contacted to retrieve the necessary information.
The intervention needed to be primarily delivered via technology (ie, computer, internet, or smartphone). Interventions were categorized as CBT if (1) they were explicitly described as such by the authors of the article and we found no reason to disagree or (2) all authors of this review agreed that the description of the main intervention components could be regarded as CBT. The control condition was defined as active treatment control (ie, face-to-face CBT or treatment as usual [TAU]) or passive control (ie, waiting list/no treatment or information control). Studies in which the control condition involved an active self-help website (ie, including both psychoeducation and exercises) focused specifically on anxiety or depression were excluded. Studies in which the control condition involved a monitoring control website that did not include active self-help content were included. Comorbid psychiatric or medical disorders were not used as an exclusion criterion.
Two authors (CC and MS) conducted the study selection in a stepwise manner. First, titles and abstracts of all studies were independently screened for potential eligibility. Any disagreements were discussed until consensus was reached. Second, the full papers of all included abstracts were independently screened according to the inclusion and exclusion criteria. In case of discrepancy or uncertainty regarding inclusion, a third author (MB) was consulted until consensus was reached.
Data Extraction
Information on study characteristics, participant characteristics, and mental health outcomes was extracted from each study and included in an Excel spreadsheet. Data extraction was conducted by one reviewer (CC) and checked by a second reviewer (MS). Study characteristics included authors, country, year of publication, study design, recruitment setting (ie, clinical, general population, or schools), inclusion and exclusion criteria, primary outcome measures, and descriptions of the experimental intervention and comparator, including focus of the intervention, information on guidance, number of treatment modules, and adherence rates. Participant characteristics included sample size, mean age, gender, primary diagnostic type (ie, anxiety, depression, or both; either based on diagnosis or an elevated symptom level), and baseline symptom levels. Means and SDs of the outcome measures of anxiety and depressive symptoms at posttreatment assessment were extracted. If available, means and SDs at short-term follow-up (ie, 1-5 months) and long-term follow-up (ie, 6-12 months) were extracted as well.
If possible, we utilized effect sizes of the intention-to-treat sample; if these were not available, we used effect sizes of the completer sample. In case of multiple outcome measures of anxiety and depressive symptoms, we selected the primary outcome measure as stated by the authors. If the authors did not specify any primary outcome measure of anxiety or depressive symptoms, we selected a well-validated and widely-used outcome measure of these symptoms that was used at every time point of the study (ie, both at posttest and follow-up, if applicable). If both an active treatment control and passive control were utilized in a single RCT, outcomes from both conditions were extracted. Our main meta-analyses were conducted separately for active treatment control (ie, face-to-face CBT or face-to-face TAU) and passive control (ie, waiting list, information control, or no treatment). In our subgroup analyses, data from all control groups per study were included. As the inclusion of multiple comparisons of one study in a meta-analysis violates the assumption of independence, we divided the n of the intervention group evenly across comparators, which is a procedure recommended by the Cochrane guidelines [48].
Quality Assessment
The quality of each included study was assessed following the guidelines provided by the Cochrane risk-of-bias tool for randomized trials, version 2.0 (RoB 2) [49]. Risk of bias was examined in the following five domains: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) missing outcome data; (4) bias in measurement of the outcome; and (5) bias in selection of the reported result. Each domain was rated as either low risk of bias, some concerns, or high risk of bias. A total score was calculated for each study by adding up the following values for each domain: “0” for low risk of bias, “1” for some concerns, and “2” for high risk of bias.
The overall quality of the evidence for each outcome was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [50]. The quality of each outcome was assessed for the following domains: (1) risk of bias; (2) inconsistency of results (ie, heterogeneity); (3) indirectness of evidence; (4) imprecision of results; and (5) suspected publication bias. In case of limitations in one domain, the evidence for each outcome was downgraded by one or two levels. Subsequently, the overall evidence for each outcome across domains was categorized as high, moderate, low, or very low, representing the level of certainty of the effect estimates. Both RoB 2 and GRADE assessments were conducted independently by two reviewers (CC and MS), and any disagreements were resolved by discussion until consensus was reached. Cohen κ coefficients were calculated to determine the interrater reliability.
Statistical Analysis
A random-effects meta-analysis was conducted with the Comprehensive Meta-Analysis software (CMA version 3), using the SMD to calculate pooled mean effect sizes (Hedges g). Effect sizes were calculated by subtracting the mean posttest score of the treatment group from the mean score of the comparison group, and dividing the result by the pooled standard deviation of the two groups. Posttreatment means and SDs were compared between the intervention and control groups. Effect sizes of 0.2, 0.5, and 0.8 are considered to be small, medium, and large, respectively [51]. In addition, we calculated the number needed to treat (NNT), using the Kraemer & Kupfer [52] formula. The NNT indicates the total number of patients who need to be treated in order to achieve one additional positive outcome [53].
Heterogeneity was assessed by calculating the I2 statistic, which indicates how much overall variance should be attributed to between-study variance, with a value of 25% representing low heterogeneity, 50% representing moderate heterogeneity, and 75% representing high heterogeneity. In addition, we calculated the 95% CIs around I2 by using the noncentral chi-square approach in the “heterogi” module of STATA [54,55].
Subgroup analyses were conducted to examine the influence on the difference between intervention and control conditions for (1) the diagnostic focus of the intervention (ie, anxiety, depression, or both); (2) age group (ie, adolescents with mean age ≤18 years or young adults with mean age >18 years); (3) the level of guidance (ie, guided or self-guided); (4) the adherence rate, defined as the percentage of participants in the intervention group who completed all treatment modules at posttreatment (ie, low, defined as ≤50%, or high, defined as >50%); (5) recruitment type (ie, clinical, community, or university/school); and (6) the number of treatment modules (ie, <5, 5-9, or 10-14 modules). Subgroup analyses were conducted across studies with interventions focused on anxiety, depression, or both, with multiple control groups per study included. Subgroup analyses were conducted using the mixed-effects model, in which the effect sizes within the subgroups are pooled with the random-effects model, whereas the fixed-effects model is used to test for significant differences between the subgroups. Subgroup analyses involving age, guidance level, and adherence rates were planned a priori based on the literature. In addition, a subgroup analysis on the diagnostic focus of the intervention was planned a priori to test whether it was justified to conduct all subgroup analyses on the total set of studies, including interventions aimed at anxiety, depression, or both. Recruitment type and number of treatment modules were examined post-hoc as these reflect potential sources of heterogeneity. For all six subgroup analyses, a Bonferroni-corrected α level of P<.008 was used to account for multiple testing. In addition, bivariate meta-regression analyses were conducted to explore the associations of the mean age of study participants, adherence rate, and risk of bias with effect sizes. Analyses with age and adherence rate were planned a priori, whereas risk of bias level was included post-hoc.
Publication bias was examined as follows. First, the funnel plot of effect sizes was visually inspected. Second, the Duval and Tweedie trim and fill procedure was used to calculate an adjusted pooled effect size that accounts for missing studies due to publication bias [56]. Third, the Egger test was used to quantify the bias captured by the funnel plot [57]. In accordance with the Cochrane guidelines [48], publication bias was only examined in meta-analyses with at least 10 studies.
Results
Systematic Review
Included Studies
The database search resulted in 7670 articles, of which we retrieved the full text of 240 articles. Twenty-four studies met all inclusion criteria and were included in the systematic review and meta-analysis (Figure 1). Interrater agreement of inclusion was strong (98.3%; Cohen κ=0.90, P<.001). The included studies were published between 2009 and September 2019. Most were conducted in Australia (n=5) and the United Kingdom (n=4). All studies reported posttreatment effects, whereas short-term and long-term follow-up data of both intervention and control conditions were only reported in three and five studies, respectively. The sample sizes of the RCTs ranged from 19 to 257 (mean 92.75, median 70). Twelve studies were primarily aimed at adolescents (age 12-19 years), eight studies were aimed at young adults (age 19-25 years), and four studies had a mixed sample. The mean age varied between 13.31 [58] and 24.40 years [59]. Most studies were conducted in samples of university students (n=8) or community samples (n=7), whereas four studies were conducted in clinical samples, four studies in secondary schools or educational programs, and one study in a mixed sample [60]. Studies targeted participants with a diagnosis or elevated symptoms of depressive disorder (n=10), participants with a diagnosis or elevated symptoms of anxiety disorder (n=8), or participants with elevated symptoms of depressive and/or anxiety disorder (n=6). In total, 19 studies compared cCBT to a waiting list or no treatment control condition, of which five studies also included a face-to-face CBT control condition. Four studies compared cCBT to a placebo condition (information control or attention control), and one study compared cCBT to TAU. Selected characteristics of the included studies are presented in Multimedia Appendix 2.
Figure 1.
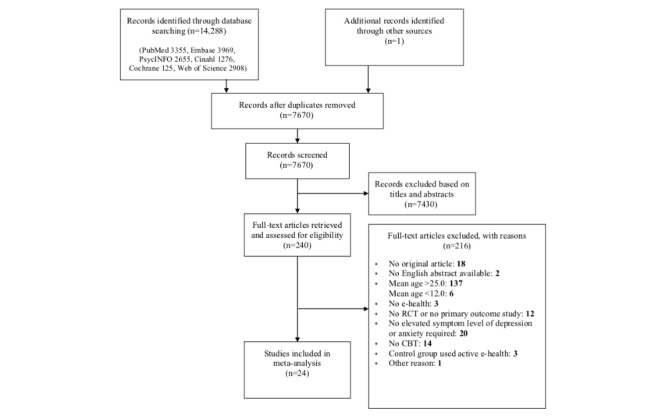
Flow chart.
Description of the Interventions
Seventeen studies investigated cCBT programs delivered via the internet (also known as iCBT), such as MoodGym [60-62] and BRAVE [63,64]. Of these interventions, most were completed at the respondent’s home (n=12), whereas five were completed at a treatment or research site. Seven studies investigated cCBT programs delivered via a computer program or CD-ROM, such as SPARX [65-67], Woebot [68], and Stressbusters [58]. Of these interventions, four were completed at the respondent’s home (n=4) and three were completed at school or a treatment site. The regular treatment components of cCBT were psychoeducation, behavioral activation, cognitive restructuring, exposure, problem-solving, and homework assignments.
Treatment Duration and Intensity
The number of treatment modules ranged from 3 to 12 in 21 included studies (mean 7.1, median 7). Two studies did not report the exact number of modules [59,69]. One study examined the Woebot intervention [68], which does not consist of different modules, but delivers cCBT by 1 to 20 (median 12) automated conversations and mood tracking in an instant messenger app. The 24 included interventions were completed over a period of 2 to 16 weeks (mean 7.5, median 7).
Guidance
In 14 studies, participants were guided through the intervention by a therapist or researcher. The other 10 interventions were self-guided (ie, unguided) [58,59,65-72]. Guidance was provided through telephone and/or email contact [63,64,73-78], chat sessions [79], or face-to-face guidance during the participant’s completion of the modules [60-62,80,81]. In general, guidance consisted of monitoring progress and providing support, encouragement, and clarification. In nine studies, guidance additionally included providing personalized feedback on completed exercises [63,64,74-80].
Adherence
Adherence rates were reported in 19 studies. Only 10 studies reported the most common measure of adherence (ie, the number of completed sessions divided by the maximum number of sessions). In these studies, adherence ranged from 32.2% to 100% (mean 76.91%, median 78%). An alternative measure of adherence, namely the percentage of participants in the intervention group who completed all treatment modules, was reported in 19 studies, with adherence rates ranging from 0% to 100% (mean 57.12%, median 60%). Adherence rates for each study are presented in Multimedia Appendix 3.
Quality of Evidence
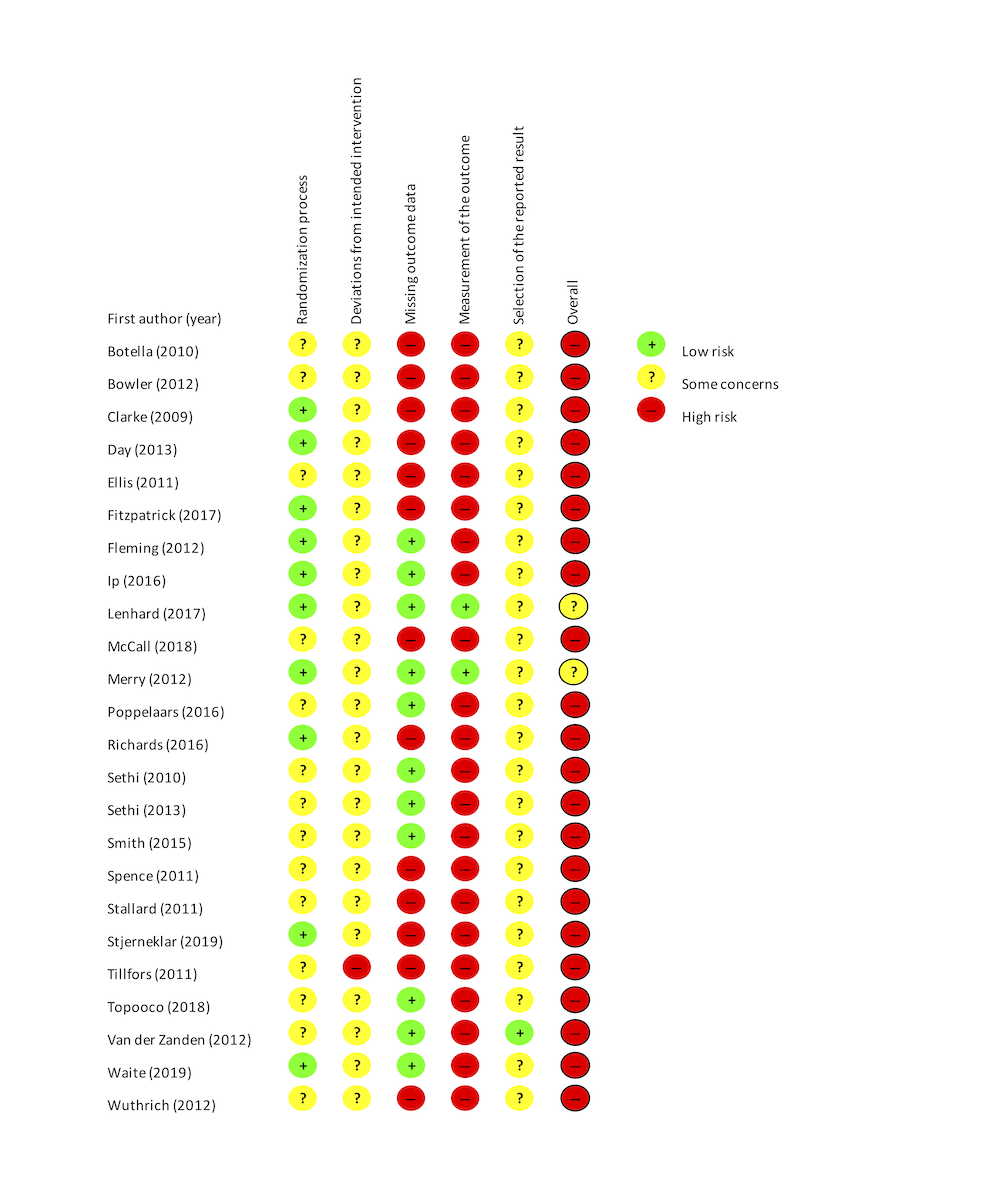
Based on the Cochrane RoB 2 tool [49], 22 out of 24 studies had an overall high risk of bias, and the remaining two studies were rated as “some concerns.” The overall high risk of bias in this vast majority of included studies was mainly due to an increased risk of bias in the measurement of the outcome, caused by the use of self-report measures or the unblinded use of observer-rated measures. Furthermore, 13 out of 24 studies also had an increased risk of bias due to missing outcome data, since >5% of their data were missing and no sufficiently appropriate analysis (eg, multiple imputation) was used to handle the missing data. Lastly, one study was rated as having an increased risk of bias due to deviations from the intended intervention [77]. Interrater reliability for the risk of bias was very good (κ=0.89, P<.001). Figure 2 demonstrates the authors’ conclusions regarding the risk of bias across studies. Multimedia Appendix 4 presents the risk of bias classifications per domain assigned to each study. It should be noted that self-report measures are widely used in psychological treatment studies, especially in studies on computerized treatment. Therefore, the current rating may be too strict. Without taking into account the risk of bias in the measurement of the outcome, 13 out of 24 studies had an overall high risk of bias.
Figure 2.
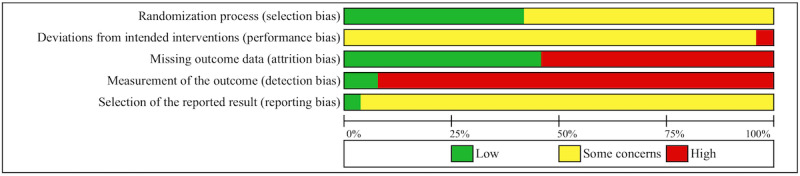
Risk of bias graph.
The overall quality of the evidence for each outcome was assessed using the GRADE approach [50]. The quality rate for each outcome is shown in Tables 1-3. In summary, although the overall quality of some outcomes was moderate, the overall quality of most outcomes was low. Since almost all studies were associated with a high risk of bias based on the RoB tool, all outcomes were downgraded one level for this domain. Many outcomes were downgraded one additional level for inconsistency, because of substantial heterogeneity in the meta-analysis. One outcome was downgraded one additional level for imprecision of results due to a small sample size. Interrater reliability for the quality of evidence was very good (κ=0.87, P<.001).
Table 1.
Effect sizes regarding depressive symptoms in the meta-analysis of studies comparing computerized cognitive behavior therapy in adolescents and young adults with active treatment and passive controls at posttreatment.
| Variable | Ncoma | Nparb | Effect size | Heterogeneity | Gradec | NNTd | ||||
| g | 95% CI | I 2 | 95% CI | |||||||
| All studies |
|
|
|
|
|
|
|
|
||
|
|
Active treatment controls | 5 | 403 | −0.55 | −1.18 to 0.08 | 87.52 | 73 to 94 | ++ | 3.31 | |
|
|
Passive controls | 20 | 1604 | 0.52e | 0.33 to 0.71 | 68.69 | 50 to 80 | ++ | 3.5 | |
|
|
|
One outlier removedf | 19 | 1558 | 0.46e | 0.29 to 0.63 | 58.49 | 31 to 75 | +++ | 3.91 |
| Studies aimed at depression |
|
|
|
|
|
|
|
|
||
|
|
Active treatment controls | 4 | 351 | −0.70 | −1.51 to 0.11 | 90.63 | 79 to 96 | + | 2.63 | |
|
|
Passive controls | 13 | 1162 | 0.60e | 0.35 to 0.85 | 73.27 | 54 to 85 | ++ | 3.05 | |
|
|
|
One outlier removedf | 12 | 1116 | 0.51e | 0.30 to 0.72 | 61.76 | 28 to 80 | ++ | 3.55 |
aNcom: number of comparisons.
bNpar: number of participants.
c+: very low quality; ++: low quality; +++: moderate quality.
dNNT: number needed to treat.
eP<.001.
fOutlier Sethi (2013) excluded.
Table 3.
Bivariate meta-regression analyses regarding depressive symptoms in studies comparing computerized cognitive behavior therapy in adolescents and young adults with active treatment and passive controls at posttreatment.
| Variable | Ncoma | b | 95% CI | P | |
| Mean ageb |
|
|
|
|
|
|
|
Intercept | 21 | 0.14 | −0.55 to 0.84 | .69 |
|
|
Mean age | 21 | 0.01 | −0.02 to 0.05 | .44 |
| Adherenceb |
|
|
|
|
|
|
|
Intercept | 16 | 0.39 | −0.02 to 0.79 | .06 |
|
|
Adherence | 16 | 0.01 | −0.01 to 0.01 | .75 |
| Risk of biasb |
|
|
|
|
|
|
|
Intercept | 21 | −0.07 | −0.68 to 0.53 | .81 |
|
|
Risk of bias | 21 | 0.11 | −0.01 to 0.23 | .08 |
aNcom: number of comparisons.
bOutliers Sethi (2010) and Sethi (2013) excluded.
Meta-Analysis
Effects of cCBT on Depressive Symptoms at Posttreatment
The pooled effect size of cCBT for depressive disorders, anxiety disorders, or both regarding depressive symptoms at posttreatment compared with active treatment controls was g=−0.55 (95% CI −1.18 to 0.08, P=.09, k=5; Table 1), and heterogeneity was high (I2=87.52%, 95% CI 73-94). Compared with passive controls, the pooled effect size of cCBT was g=0.52 (95% CI 0.33-0.71, P<.001, k=20), and heterogeneity was moderate (I2=68.69%, 95% CI 50-80). Removing one extreme outlier with an effect size of g=1.93 [60] resulted in a somewhat smaller mean effect size of g=0.46 (95% CI 0.29-0.63, P<.001, k=19), with a lower, though still moderate, heterogeneity (I2=58.49%, 95% CI 31-75).
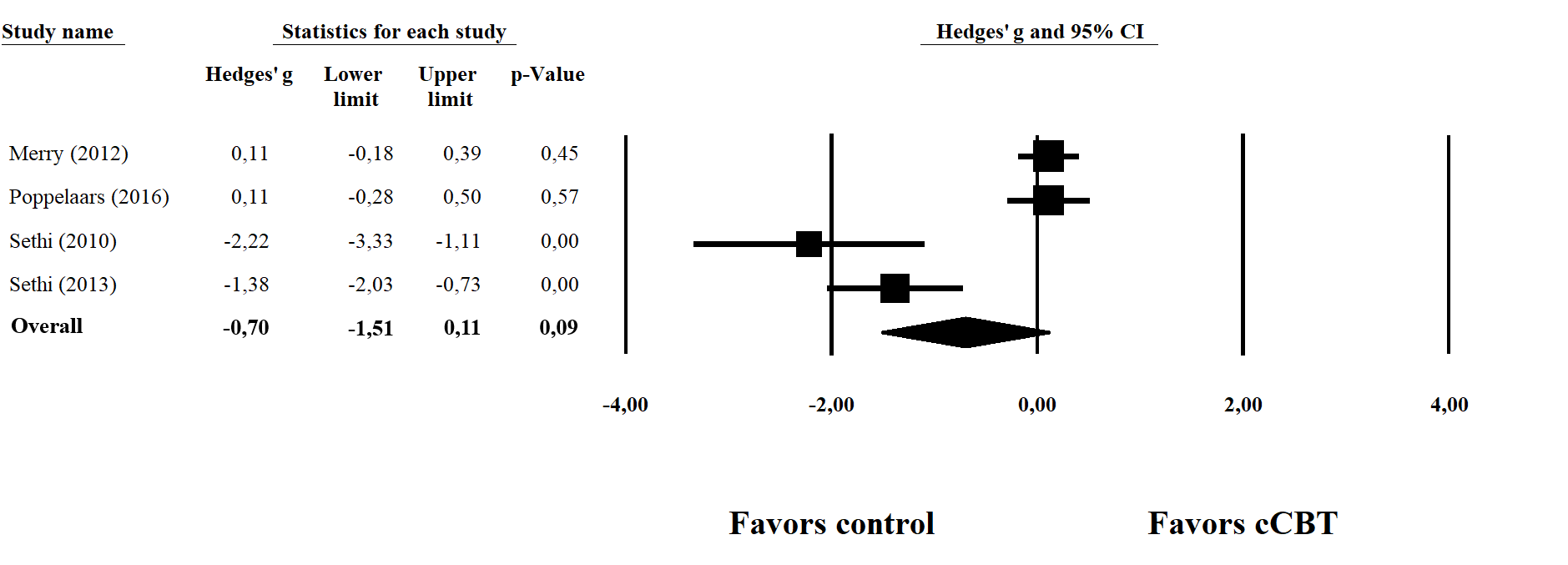
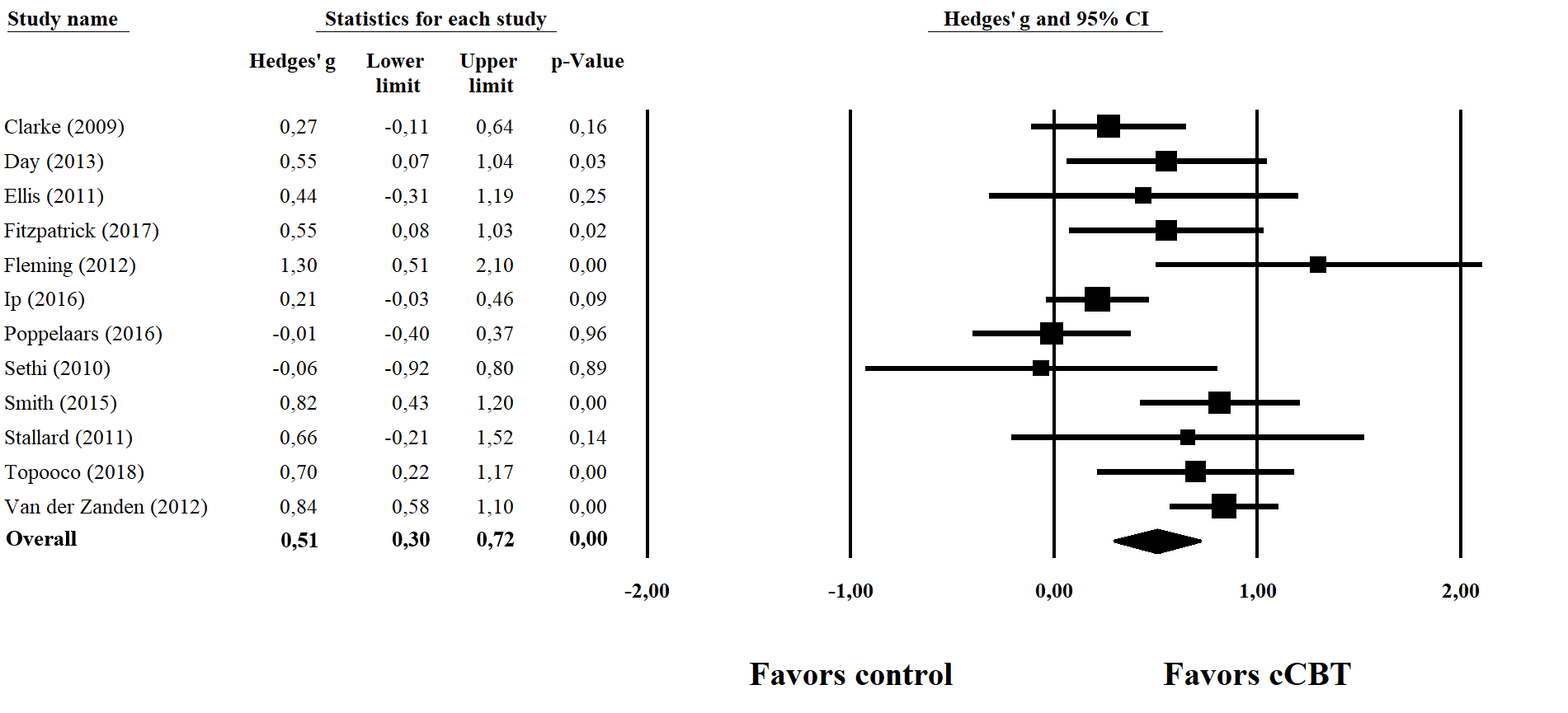
In studies aimed specifically at depressive disorders or both depressive and anxiety disorders, the nonsignificant pooled effect size of cCBT compared with active treatment controls regarding depressive symptoms was g=−0.70 (95% CI −1.51 to 0.11, P=.09, k=4), corresponding to an NNT of 2.63 in favor of active treatment controls. Heterogeneity was very high (I2=90.63%, 95% CI 79-96). When compared with passive controls, cCBT yielded a significant medium effect size of g=0.60 (95% CI 0.35-0.85, P<.001, k=13), corresponding to an NNT of 3.05. Heterogeneity was moderate to high (I2=73.27, 95% CI 54-85). Removing the extreme outlier [60] again resulted in a somewhat smaller mean effect size of g=0.51 (95% CI 0.30-0.72, P<.001, k=12), with a lower, though still moderate, heterogeneity (I2=61.76, 95% CI 28-80) and a corresponding NNT of 3.55. Inspection of the funnel plot and the Duval and Tweedie trim and fill procedure showed no indication of publication bias, and the Egger test of the intercept was not significant (P=.74), indicating no need to adjust for missing studies. Multimedia Appendix 5 and Multimedia Appendix 6 provide forest plots of effect sizes regarding depressive symptoms for active treatment controls and passive controls, respectively.
A series of subgroup analyses (Table 2) was conducted across studies focused on depression, anxiety, or both, with multiple control groups per study included and two extreme outliers excluded [60,62]. Heterogeneity remained moderate in most subgroups. Effects in all but two subgroups were significantly different from zero, and all were in favor of cCBT. We found no indication that the diagnostic focus of the intervention, age group, level of guidance, adherence rate, type of recruitment, or number of treatment modules was associated with differential effect sizes. Lastly, bivariate meta-regression analyses (Table 3) showed no significant association of the mean age of study participants (b=0.01; 95% CI −0.02 to 0.05, P=.44), adherence (b=0.01; 95% CI −0.01 to 0.01, P=.74), or risk of bias (b=0.11; 95% CI −0.01 to 0.23, P=.08) with effect size regarding depressive symptoms.
Table 2.
Effect sizes regarding depressive symptoms in the subgroup analyses of studies comparing computerized cognitive behavior therapy in adolescents and young adults with active treatment and passive controls at posttreatment.
| Variable | Ncoma | Nparb | Effect size | Heterogeneity | P | NNTc | |||
| g | 95% CI | I 2 | 95% CI | ||||||
| Diagnostic focusd |
|
|
|
|
|
|
.63 |
|
|
|
|
Anxiety | 8 | 464 | 0.32e | 0.04 to 0.60 | 50.78 | 0 to 78 |
|
5.56 |
|
|
Depression | 9 | 1152 | 0.44f | 0.21 to 0.67 | 75.44 | 53 to 87 | 4.1 | |
|
|
Both | 4 | 182 | 0.55e | 0.13 to 0.96 | 0 | 0 to 85 |
|
3.31 |
| Age groupd |
|
|
|
|
|
|
.29 |
|
|
|
|
Adolescents | 12 | 1027 | 0.34g | 0.14 to 0.54 | 61.51 | 28 to 79 |
|
5.26 |
|
|
Young adults | 9 | 771 | 0.50f | 0.28 to 0.73 | 39.7 | 0 to 72 |
|
3.62 |
| Guidanced |
|
|
|
|
|
|
.56 |
|
|
|
|
Guided | 10 | 771 | 0.46f | 0.23 to 0.70 | 56.96 | 13 to 79 |
|
3.91 |
|
|
Self-guided | 11 | 1027 | 0.37g | 0.16 to 0.58 | 58.97 | 20 to 79 |
|
4.85 |
| Adherenced |
|
|
|
|
|
|
.77 |
|
|
|
|
Low | 6 | 779 | 0.39e | 0.09 to 0.69 | 77.56 | 50 to 90 |
|
4.59 |
|
|
High | 10 | 737 | 0.48f | 0.23 to 0.72 | 62.06 | 25 to 81 |
|
3.76 |
| Recruitment typed |
|
|
|
|
|
|
.53 |
|
|
|
|
Clinical | 4 | 376 | 0.24 | −0.11 to 0.59 | 0 | 0 to 85 |
|
7.46 |
|
|
Community | 5 | 462 | 0.50g | 0.18 to 0.82 | 78.12 | 47 to 91 |
|
3.62 |
|
|
University/school | 12 | 960 | 0.44f | 0.23 to 0.65 | 50.27 | 3 to 74 |
|
4.1 |
| Number of modulesd |
|
|
|
|
|
|
.21 |
|
|
|
|
<5 | 3 | 138 | 0.65g | 0.20 to 1.11 | 0 | 0 to 90 |
|
2.82 |
|
|
5-9 | 12 | 1097 | 0.49f | 0.29 to 0.69 | 69.11 | 44 to 83 |
|
3.68 |
|
|
10-14 | 3 | 377 | 0.14 | −0.23 to 0.52 | 0 | 0 to 90 |
|
12.82 |
aNcom: number of comparisons.
bNpar: number of participants.
cNNT: number needed to treat.
dOutliers Sethi (2010) and Sethi (2013) excluded.
eP<.05.
fP<.001.
gP<.01.
Effects of cCBT on Anxiety Symptoms at Posttreatment
Regarding anxiety symptoms at posttreatment, the pooled effect size of cCBT for anxiety disorders, depressive disorders, or both compared with active treatment controls was g=0.06 (95% CI −0.13 to 0.26, P=.53, k=5; Table 4). Heterogeneity was low, although the wide 95% CI indicated some uncertainty regarding the exact level of heterogeneity (I2=0.00%, 95% CI 0-79). Compared with passive controls, cCBT yielded a significant pooled effect size of g=0.49 (95% CI 0.29-0.68, P<.001, k=21), and heterogeneity was moderate (I2=68.17%, 95% CI 50-80). Removing one extreme outlier with an effect size of g=1.94 [60] resulted in a slightly smaller mean effect size of g=0.42 (95% CI 0.25-0.59, P<.001, k=20), with a lower, though still moderate, heterogeneity (I2=57.42%, 95% CI 30-74).
Table 4.
Effect sizes regarding anxiety symptoms in the meta-analysis of studies comparing computerized cognitive behavior therapy in adolescents and young adults with active treatment and passive controls at posttreatment.
| Variable | Ncoma | Nparb | Effect size | Heterogeneity | Gradec | NNTd | ||||||||||||
| g | 95% CI | I 2 | 95% CI |
|
|
|||||||||||||
| All studies |
|
|
|
|
|
|
|
|
||||||||||
|
|
Active treatment controls | 5 | 390 | 0.06 | −0.13 to 0.26 | 0 | 0 to 79 | ++ | 29.41 | |||||||||
|
|
Passive controls | 21 | 1570 | 0.49e | 0.29 to 0.68 | 68.17 | 50 to 80 | ++ | 3.68 | |||||||||
|
|
|
One outlier removedf | 20 | 1524 | 0.42e | 0.25 to 0.59 | 57.42 | 30 to 74 | +++ | 4.27 | ||||||||
| Studies aimed at anxiety |
|
|
|
|
|
|
|
|
||||||||||
|
|
Active treatment controls | 4 | 203 | 0.04 | −0.23 to 0.31 | 0 | 0 to 85 | ++ | 45.45 | |||||||||
|
|
Passive controls | 16 | 868 | 0.59e | 0.34 to 0.84 | 67.83 | 46 to 81 | ++ | 3.09 | |||||||||
|
|
|
One outlier removedf | 15 | 822 | 0.50e | 0.29 to 0.71 | 52.57 | 15 to 74 | +++ | 3.62 | ||||||||
|
|
|
Trim and fill adjusted values |
|
0.44 | 0.23 to 0.65 |
|
|
|
4.1 | |||||||||
aNcom: number of comparisons.
bNpar: number of participants.
c++: low quality; +++: moderate quality.
dNNT: number needed to treat.
eP<.001.
fOutlier Sethi (2013) excluded.
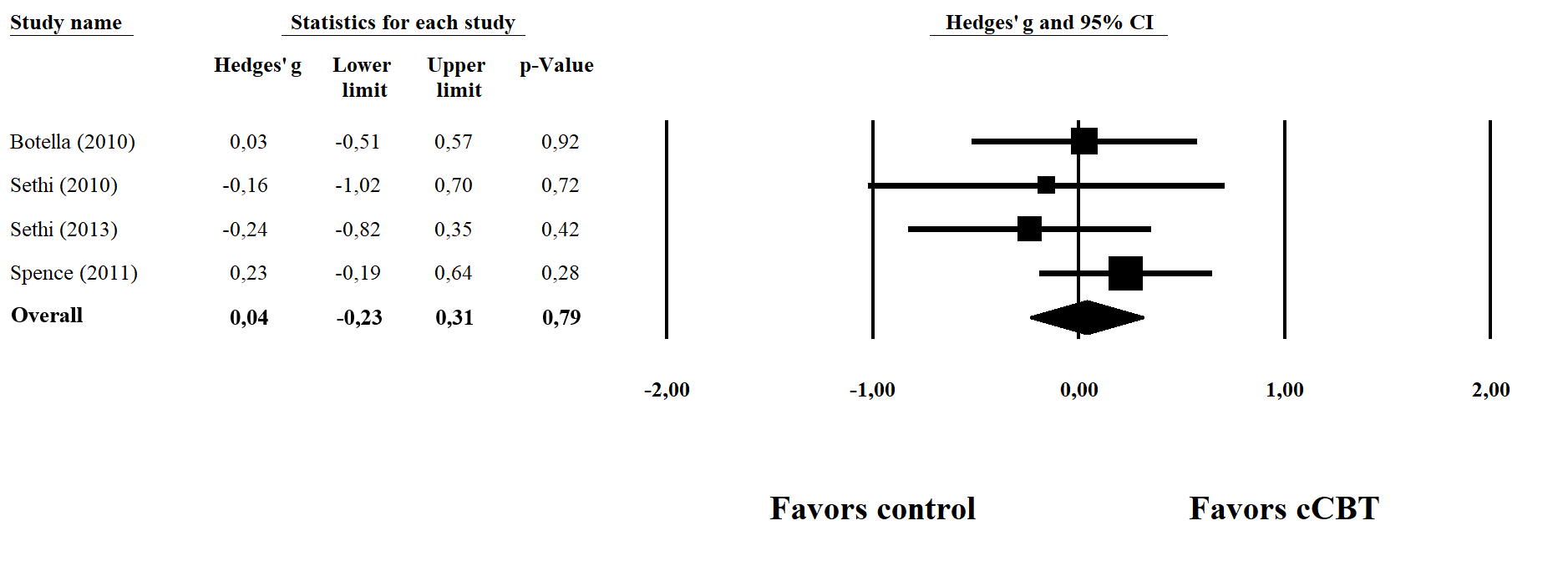
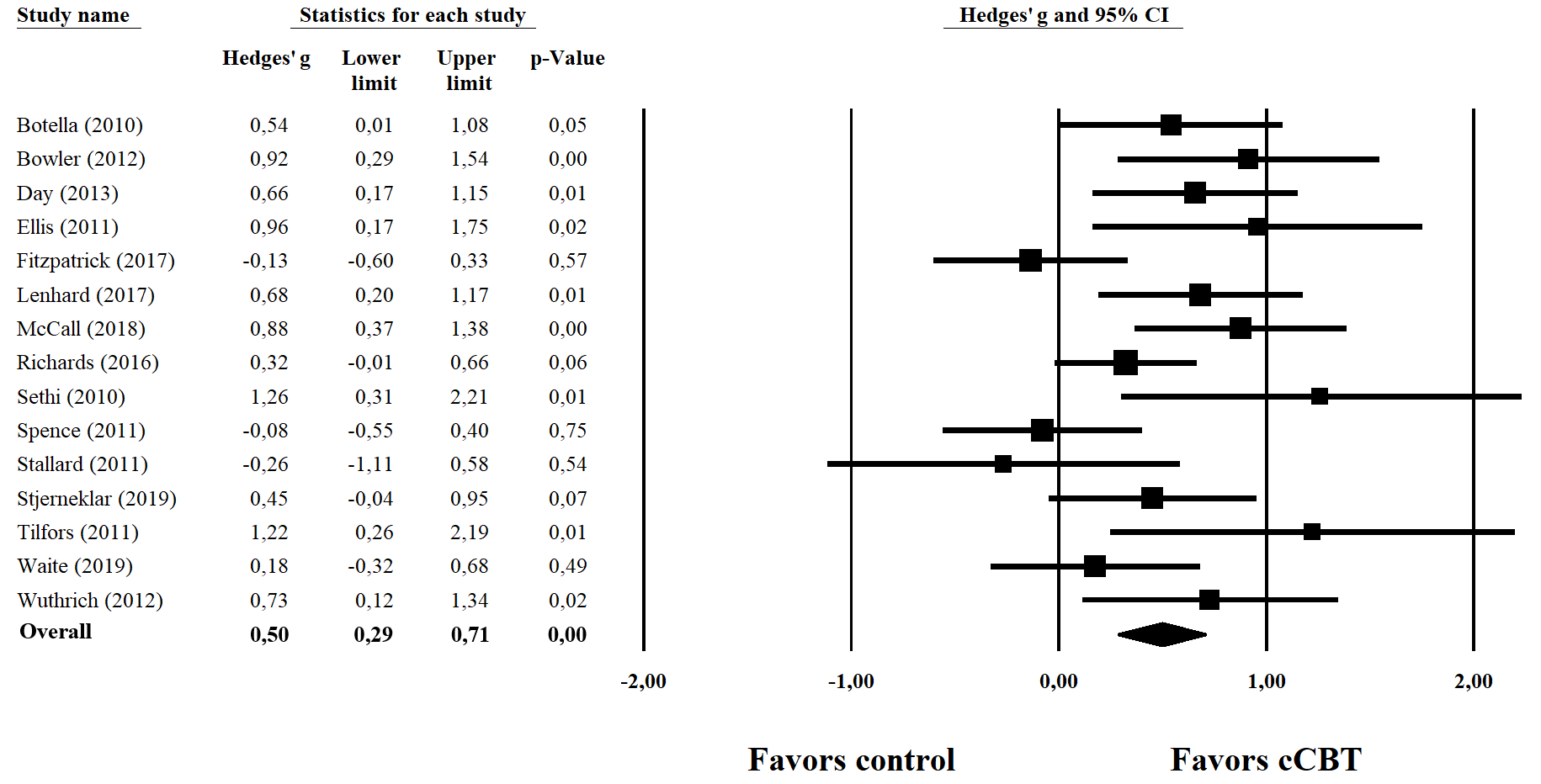
When only including studies with cCBT aimed specifically at anxiety disorders or at both anxiety and depressive disorders, the nonsignificant pooled effect size regarding anxiety symptoms compared with active treatment controls remained similar (g=0.04, 95% CI −0.23 to 0.31, P=.79, k=4). Heterogeneity was low, although the wide 95% CI again indicated uncertainty regarding the exact level of heterogeneity (I2=0.00%, 95% CI 0-85). Compared with passive controls, cCBT yielded a pooled effect size of g=0.59 (95% CI 0.34-0.84, P<.001, k=16), corresponding to an NNT of 3.09, and heterogeneity was moderate (I2=67.83%, 95% CI 46-81). Again, removing the extreme outlier [60] resulted in a smaller mean effect size of g=0.50 (95% CI 0.29-0.71, P<.001, k=15), with an NNT of 3.62 and a lower, though still moderate, heterogeneity (I2=52.57%, 95% CI 15-74). Inspection of the funnel plot and the Duval and Tweedie trim and fill procedure showed a minor indication of publication bias, but the Egger test of the intercept was not significant (P=.11). Adjusting for missing studies using the Duval and Tweedie trim and fill procedure resulted in a slightly smaller overall effect size of g=0.44 (95% CI 0.23-0.65), corresponding to an NNT of 4.10. Multimedia Appendix 7 and Multimedia Appendix 8 provide forest plots of effect sizes regarding anxiety symptoms for active treatment and passive control conditions, respectively.
A series of subgroup analyses were conducted across studies focused on anxiety, depression, or both, with multiple comparators per study included and one outlier excluded [60]. Heterogeneity was moderate in most subgroups (Table 5). Effects in most subgroups were different from zero, and all were in favor of cCBT. We found no indication that the diagnostic focus of the intervention, age group, type of guidance, adherence rate, type of recruitment, or number of treatment modules was associated with differential effect sizes. Lastly, bivariate meta-regression analyses (Table 6) showed no significant association of the mean age of study participants (b=0.02; 95% CI −0.01 to 0.06, P=.21), adherence (b=0.00; 95% CI −0.01 to 0.00, P=.65), or risk of bias (b=0.04; 95% CI −0.05 to 0.13, P=.36) with effect size regarding anxiety symptoms.
Table 5.
Effect sizes regarding anxiety symptoms in the subgroup analyses of studies comparing computerized cognitive behavior therapy in adolescents and young adults with active treatment and passive controls at posttreatment.
| Variable | Ncoma | Nparb | Effect size | Heterogeneity | P | NNTc | |||
| g | 95% CI | I 2 | 95% CI | ||||||
| Diagnostic focusd |
|
|
|
|
|
|
|
|
|
|
|
Anxiety | 12 | 687 | 0.47e | 0.25 to 0.69 | 34.28 | 0 to 67 | .39 | 3.85 |
|
|
Depression | 6 | 889 | 0.23 | −0.03 to 0.50 | 71.68 | 34 to 88 |
|
7.69 |
|
|
Both | 6 | 211 | 0.33 | −0.04 to 0.69 | 61.89 | 7 to 84 |
|
5.43 |
| Age groupd |
|
|
|
|
|
|
|
|
|
|
|
Adolescents | 13 | 1031 | 0.25f | 0.06 to 0.44 | 44.27 | 0 to 71 | .08 | 7.14 |
|
|
Young adults | 11 | 756 | 0.51e | 0.29 to 0.73 | 51.47 | 3 to 76 |
|
3.55 |
| Guidanced |
|
|
|
|
|
|
|
|
|
|
|
Guided | 15 | 958 | 0.41e | 0.21 to 0.61 | 48.01 | 5 to 71 | .47 | 4.39 |
|
|
Self-guided | 9 | 829 | 0.30g | 0.07 to 0.53 | 60.28 | 17 to 81 |
|
5.95 |
| Adherenced |
|
|
|
|
|
|
|
|
|
|
|
Low | 8 | 894 | 0.44e | 0.19 to 0.68 | 38.77 | 0 to 73 | .61 | 4.1 |
|
|
High | 11 | 655 | 0.27g | 0.04 to 0.51 | 55.6 | 13 to 77 |
|
6.58 |
| Recruitment typed |
|
|
|
|
|
|
|
|
|
|
|
Clinical | 3 | 267 | 0.06 | −0.34 to 0.46 | 0 | 0 to 90 | .28 | 29.41 |
|
|
Community | 8 | 620 | 0.43f | 0.17 to 0.68 | 58.97 | 10 to 81 |
|
4.2 |
|
|
University/school | 13 | 900 | 0.40e | 0.20 to 0.61 | 51.22 | 7 to 74 |
|
4.5 |
| Number of modulesd |
|
|
|
|
|
|
|
|
|
|
|
<5 | 5 | 167 | 0.47g | 0.05 to 0.89 | 68.76 | 20 to 88 | .91 | 3.85 |
|
|
5-9 | 12 | 1051 | 0.38f | 0.16 to 0.60 | 63.37 | 32 to 80 |
|
4.72 |
|
|
10-14 | 5 | 492 | 0.29 | −0.04 to 0.61 | 12.58 | 0 to 82 |
|
6.17 |
aNcom: number of comparisons.
bNpar: number of participants.
cNNT: number needed to treat.
dOutlier Sethi (2013) excluded.
eP<.001.
fP<.01.
gP<.05.
Table 6.
Bivariate meta-regression analyses regarding anxiety symptoms in studies comparing computerized cognitive behavior therapy in adolescents and young adults with active treatment and passive controls at posttreatment.
| Variable | Ncoma | b | 95% CI | P | |
| Mean ageb |
|
|
|
|
|
|
|
Intercept | 24 | −0.07 | −0.77 to 0.63 | .84 |
|
|
Mean age | 24 | 0.02 | −0.01 to 0.06 | .21 |
| Adherenceb |
|
|
|
|
|
|
|
Intercept | 19 | 0.42 | 0.10 to 0.74 | .01 |
|
|
Adherence | 19 | 0.00 | −0.01 to 0.00 | .65 |
| Risk of Biasb |
|
|
|
|
|
|
|
Intercept | 24 | 0.13 | −0.38 to 0.65 | .61 |
|
|
Risk of Bias | 24 | 0.04 | −0.05 to 0.13 | .36 |
aNcom: number of comparisons.
bOutlier Sethi (2013) excluded.
Short-Term Follow-Up Effects
Three studies reported short-term follow-up effects (ie, up to 5 months posttreatment) for cCBT on depressive symptoms. The pooled effect size for studies with cCBT aimed specifically at depressive disorders or at both depressive and anxiety disorders compared with active treatment controls was not significant (g=0.12, 95% CI −0.11 to 0.35, P=.29, k=2; Table 7). Compared with passive controls, the pooled effect size showed no significant difference between cCBT and control conditions either (g=0.19, 95% CI −0.08 to 0.46, P=.16, k=2). Although effect sizes were in favor of cCBT, these results indicated that cCBT is not superior to controls at short-term follow-up. However, owing to the small number of comparisons, the statistical power to detect small differences was limited. Heterogeneity was low (I2=0.00%), but the number of studies was too small to enable calculation of 95% CI. No studies reported short-term follow-up effects for cCBT on anxiety symptoms.
Table 7.
Effect sizes regarding depressive and anxiety symptoms in the meta-analysis of studies comparing computerized cognitive behavior therapy in adolescents and young adults with active treatment and passive controls at short-term follow-up (1-5 months) and long-term follow-up (6-12 months).
| Variable | Ncoma | Nparb | Effect size | Heterogeneity | Gradec | NNTd | ||||
| g | 95% CI | I 2 | 95% CI | |||||||
| Depressive symptoms |
|
|
|
|
|
|
|
|
||
|
|
Short-term follow-up |
|
|
|
|
|
|
|
|
|
|
|
|
Active treatment controls | 2 | 288 | 0.12 | −0.11 to 0.35 | 0 | N/Ae | +++ | 14.71 |
|
|
|
Passive controls | 2 | 211 | 0.19 | −0.08 to 0.46 | 0 | N/Ae | ++ | 9.43 |
|
|
Long-term follow-upf |
|
|
|
|
|
|
|
|
|
|
|
|
Passive controls | 3 | 461 | 0.27g | 0.09 to 0.45 | 0 | 0 to 90 | +++ | 6.58 |
| Anxiety symptoms |
|
|
|
|
|
|
|
|
||
|
|
Long-term follow-uph |
|
|
|
|
|
|
|
|
|
|
|
|
Active treatment controls | 2 | 140 | 0.08 | −0.41 to 0.56 | 50.61 | N/Ae | ++ | 21.74 |
aNcom: number of comparisons.
bNpar: number of participants.
c++: low quality; +++: moderate quality.
dNNT: number needed to treat.
eN/A: not applicable; calculation of 95% CI not possible because df=1.
fOnly one study with active treatment controls available.
gP<.01.
hNo studies with passive controls available.
Long-Term Follow-Up Effects
Three studies reported long-term follow-up effects (ie, 6-12 months posttreatment) for cCBT on depressive symptoms. The pooled effect size indicated cCBT aimed at depressive symptoms or both depressive and anxiety symptoms to be effective compared with passive controls at long-term follow-up (g=0.27, 95% CI 0.09-0.45, P=.004, k=3), corresponding with an NNT of 6.58. Heterogeneity was low, although the wide 95% CI indicated uncertainty regarding the exact level of heterogeneity (I2=0.00%, 95% CI 0-90). As only one study [65] reported long-term follow-up effects for cCBT on depressive symptoms compared with active treatment controls, meta-analysis was not possible.
Only two studies reported long-term follow-up effects (ie, 6-12 months posttreatment) for cCBT aimed at anxiety or both anxiety and depression on anxiety symptoms. The pooled effect size showed no significant effect for cCBT compared with active treatment controls (g=0.08, 95% CI −0.41 to 0.56, P=.75, k=2) at long-term follow-up. No study reported long-term follow-up effects for cCBT on anxiety symptoms compared with passive controls.
Discussion
Principal Findings
This study provides an up-to-date meta-analysis examining the effects of cCBT on anxiety and depressive symptoms in adolescents and young adults compared with active treatment and passive controls, differentiating between posttreatment and follow-up. Our results indicate that cCBT is beneficial for reducing anxiety and depressive symptoms at posttreatment in adolescents and young adults compared with passive controls, with small to medium effect sizes. For cCBT aimed at depressive disorders or depressive and anxiety disorders, we found a pooled effect size of g=0.51 regarding depressive symptoms, which corresponds to an NNT of 3.55. For cCBT aimed at anxiety disorders or anxiety and depressive disorders, we found an effect size of g=0.50 regarding anxiety symptoms. After adjustment for missing studies owing to a minor indication of publication bias, the effect size lowered slightly to g=0.44, corresponding to an NNT of 4.10. Compared with active treatment controls, the pooled effect size regarding depressive symptoms was in favor of controls (g=−0.70). However, the effect size was not significant and heterogeneity was very high. For anxiety symptoms, cCBT and active treatment controls showed similar effects (g=0.04). Subgroup analyses did not reveal any differences between groups; however, owing to the small number of studies, the statistical power to detect small differences was limited. Meta-regression analyses showed no associations between age, adherence rate, or risk of bias and effect sizes.
Overall, this study shows robust evidence of the effectiveness of cCBT in reducing anxiety and depressive symptoms in adolescents and young adults compared with passive controls. Our results are largely in line with those of previous studies on cCBT in children and young people aged up to 25 years [36], adolescents and young adults aged 12 to 25 years [37] and 10 to 25 years [43], and children and adolescents aged up to 18 years [44]. However, these studies generally reported somewhat larger effect sizes (range 0.62-0.77) regarding both depressive symptoms and anxiety symptoms [36], anxiety symptoms [37], or depressive and/or anxiety symptoms [44] compared with passive controls [36,37,44]. Similarly, research in adults found larger effect sizes for cCBT regarding depression and anxiety compared with passive controls (g=0.90) [34]. Compared with the effects of traditional face-to-face CBT in children and adolescents with anxiety disorders against waiting list controls (NNT=3.0) [19], we found a somewhat lower NNT for cCBT against passive controls (NNT=4.10) after adjusting for potential publication bias. Effect sizes in our study were similar to those found in a meta-analysis comparing face-to-face CBT for depression (0.60) and anxiety disorders (0.48) to passive controls in college and university students [21].
Our results suggest that the effects of cCBT do not differ from those of active treatment controls (ie, face-to-face CBT or face-to-face TAU) regarding anxiety symptoms, but may be inferior to active treatment controls regarding depressive symptoms, although the effect size was not significant. These findings are in line with those of previous meta-analyses in youth across three early studies that were also included in the current meta-analysis [37,41]. Although our meta-analysis included three additional studies, the number of RCTs comparing cCBT with face-to-face treatment in adolescents and young adults remains small. With regard to depressive symptoms, heterogeneity was very high (I2=90.63), and the pooled effect size should be interpreted with caution. Hence, more research directly comparing both treatments is needed to determine whether cCBT is effective compared with face-to-face treatment controls in adolescents and young adults. Research in adults has shown largely equivalent effects of cCBT on both anxiety and depressive symptoms compared with face-to-face CBT [34,35]. However, the number of studies directly comparing cCBT with face-to-face CBT in adults remains limited as well.
This study also aimed to investigate the effectiveness of cCBT at short-term and long-term follow-ups. However, the number of studies reporting follow-up effects was limited. Regarding long-term effects, cCBT was effective in reducing depressive symptoms compared with passive controls, with a small effect size (g=0.27). Our results indicated no long-term follow-up effect for cCBT on anxiety symptoms compared with active treatment controls. Meta-analyses of short-term follow-up data on depressive symptoms indicated similar effects for cCBT compared with active treatment and passive controls. Only Välimäki et al [43] investigated the follow-up effects of cCBT and other internet-based interventions in adolescents and young adults, reporting mid-term and long-term effects on depressive symptoms and mid-term effects on anxiety symptoms. However, they only reported mean differences, and no standardized effect size or NNT. In addition, they did not separately examine the effects of cCBT. Moreover, their selection of studies was based on interventions aimed at depression and not anxiety. Therefore, their results are not easily comparable to those of the current study.
Importantly, owing to the small number of studies reporting follow-up effects, the power to detect small effect sizes was limited in both this study and the study of Välimäki et al [43]. In contrast, the number of studies reporting follow-up effects of cCBT in adults is substantially larger. A recent meta-analysis found 29 trials that reported short-term follow-up effects and 15 trials that reported long-term follow-up effects [34]. cCBT for depressive disorder or anxiety disorder was found to be effective at short-term follow-up (ie, 3-6 months) and long-term follow-up (ie, 9-18 months) compared with posttreatment effect sizes, with small effect sizes across disorders (ie, g=0.15 and g=0.22, respectively). In contrast with the small effect sizes identified in our study, Andersson et al [82] found very large effect sizes for cCBT regarding depressive or anxiety symptoms in adults (g=1.31 across 10 studies) at long-term follow-up of 2 to 5 years compared with mainly passive controls. However, the authors noted that it was unclear whether randomization remained intact over the follow-up period. In summary, in order to determine the long-term effects of cCBT in adolescents and young adults, it is of great importance that future studies include follow-up assessments. Studies comparing cCBT with active treatment control conditions should aim to maintain randomization during the entire follow-up period.
Furthermore, this study aimed to explore whether respondents’ age, guidance level, and treatment adherence were associated with effect sizes. No moderators of treatment effects could be identified. We found no differences in effect sizes for adolescents and young adults regarding anxiety or depressive symptoms, and no association between respondents’ mean age and effect sizes. Previous studies that examined the moderating role of age in meta-analyses among youth reported mixed results. Pennant et al [37] found a higher effect size in young adults compared with adolescents regarding anxiety symptoms, but not depressive symptoms. However, the authors noted that these groups also differed in terms of symptom level, which may have caused the difference in effect sizes. Ebert et al [36] and Podina et al [42] found a higher effect size in adolescents compared with children [36], whereas others [38,44] did not find evidence for such a moderating role of age. Regarding the absence of an association between guidance level and effect sizes, our results correspond with those of Pennant et al [37] in the same age groups. Studies in children and adolescents found mixed results, with Podina et al [42] reporting higher effect sizes for lower levels of guidance and Grist et al [44] reporting higher effect sizes for higher levels of guidance. The lack of an association between adherence rates and effect sizes in our study contrasts findings in adults with depression and anxiety [33,83]. However, most studies included in this meta-analysis did not report the most common operationalization of treatment adherence, and several did not report any information on treatment completion. Post-hoc subgroup analyses and meta-regression analyses found no association of the diagnostic focus of the intervention, risk of bias, recruitment type, or number of sessions with effect sizes.
This study included a thorough evaluation of the risk of bias and quality of evidence, which indicated an overall high risk of bias in 22 out of 24 studies, and, accordingly, low to moderate overall quality of evidence. The high risk of bias was mainly due to an increased risk of bias in measurement of the outcome caused by self-report or unblinded use of observer-rated measures. However, as self-report measures allow both treatment and outcome measures of studies on computerized interventions to be completed entirely from the participant’s home, they are commonly used in studies on cCBT. As such, using the Cochrane RoB tool 2.0, a high risk of bias in measurement of the outcome is inevitable in many studies on computerized interventions for depression and anxiety. Nevertheless, studies ideally should aim to complement self-report measures with blinded observer-rated outcomes, although measures of anxiety and depressive symptoms will always remain subjective to some extent, even when observer-rated outcomes are used.
Limitations
Several limitations should be considered when interpreting the results. First, the number of studies in the meta-analyses was limited, especially with regard to short-term and long-term follow-up effects. Therefore, the power to detect small effect sizes was limited. Likewise, subgroup analyses consisted of a small number of comparisons, and the lack of relevant differences in most subgroup analyses might be caused by low statistical power. Second, the included studies showed large variations in intervention content, treatment intensity, and outcome measures. Heterogeneity was considerable in the majority of analyses, and pooled effect sizes should be interpreted with caution. Third, most studies had a high risk of bias owing to the use of self-report measures and/or inappropriate handling of missing data. Overall quality was low for most comparisons because of the high risk of bias and, in most cases, considerable heterogeneity. Lastly, almost all studies were conducted in high-income countries, and most studies in young adults were conducted among university students. Hence, generalizability of these results to other populations may be limited.
Future Directions
In the rapidly growing field of computerized mental health treatment in adolescents and young adults, new interventions are developed at a fast pace. Since the publication of the most recent previous meta-analysis in adolescents and young adults [43], six new studies were published, which have been included in our meta-analysis. However, the evidence base in young people remains limited compared with the large body of research in adults, and the quality of RCTs is often low. In addition, most RCTs have compared cCBT to passive control conditions, which appears to lead to an overestimation of effects. It is of utmost importance to compare the effects of cCBT with gold standard face-to-face treatment in order to determine whether cCBT can provide an equally effective alternative. Furthermore, more rigorous high-quality research in accordance with the CONSORT and CONSORT eHealth guidelines for conducting and reporting RCTs [84,85] is needed. In particular, future studies should minimize risk of bias by appropriately handling missing data and, ideally, complementing the use of self-report questionnaires with blinded observer-rated measures. Future research should also include larger sample sizes and longer follow-up periods in which randomization is maintained in case of active control groups [82] and should report adherence rates. Finally, future studies should investigate the effect of cCBT in lower-educated samples, as well as young people from low-income countries, for whom face-to-face mental health treatment is often unavailable [86-88]. When high-quality evidence in adolescents and young adults accumulates, future researchers will be able to draw stronger conclusions on the effectiveness of cCBT compared with both active treatment and passive controls and to determine differences in effect sizes for various subgroups and populations.
Conclusions
This meta-analysis provides robust evidence for the effectiveness of cCBT in the treatment of anxiety and depressive disorders in adolescents and young adults compared with passive controls, with small to medium posttreatment effect sizes. Furthermore, our results indicate that effects of cCBT are similar to those of active treatment controls in reducing anxiety symptoms. Regarding depressive symptoms, however, the results remain unclear, since heterogeneity was high and the number of studies comparing cCBT with active treatment controls was small. No moderators of treatment effects could be identified. cCBT appears to be a promising treatment option for young people, of whom most do not receive face-to-face treatment [23-25]. Importantly, this study also demonstrates the need for more methodologically high-quality research in this population, including active treatment control groups and long-term follow-up assessments.
Acknowledgments
The authors wish to thank Mrs CHM Planting, information specialist, for her advice and assistance regarding the search strategy.
Abbreviations
- CBT
cognitive behavior therapy
- cCBT
computerized cognitive behavior therapy
- CMA
Comprehensive Meta-Analysis software
- GRADE
Grading of Recommendations Assessment, Development and Evaluation
- NNT
number needed to treat
- RCT
randomized controlled trial
- RoB 2
risk-of-bias tool for randomized trials, version 2.0
- SMD
standardized mean difference
- TAU
treatment as usual
Appendix
Search strings.
Selected characteristics of the included studies examining the effects of computerized cognitive behavior therapy for depression and anxiety in adolescents and young adults.
Adherence rates of the included studies examining the effects of computerized cognitive behavior therapy for depression and anxiety in adolescents and young adults.
Risk of bias classification for each study.
{kind=link}
Forest plot with standardized posttreatment effect sizes (Hedges g) regarding depressive symptoms for computerized cognitive behavior therapy compared with active treatment control conditions.
{kind=link}
Forest plot with standardized posttreatment effect sizes (Hedges g) regarding depressive symptoms for computerized cognitive behavior therapy compared with passive control conditions.
{kind=link}
Forest plot with standardized posttreatment effect sizes (Hedges g) regarding anxiety symptoms for computerized cognitive behavior therapy compared with active treatment control conditions.
{kind=link}
Forest plot with standardized posttreatment effect sizes (Hedges g) regarding anxiety symptoms for computerized cognitive behavior therapy compared with passive control conditions.
{kind=link}
Footnotes
Conflicts of Interest: None declared.
References
- 1.Merikangas KR, Nakamura EF, Kessler RC. Epidemiology of mental disorders in children and adolescents. Dialogues Clin Neurosci. 2009;11(1):7–20. doi: 10.31887/DCNS.2009.11.1/krmerikangas. http://europepmc.org/abstract/MED/19432384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Patel V, Flisher AJ, Hetrick S, McGorry P. Mental health of young people: a global public-health challenge. The Lancet. 2007 Apr;369(9569):1302–1313. doi: 10.1016/S0140-6736(07)60368-7. [DOI] [PubMed] [Google Scholar]
- 3.Johnson D, Dupuis G, Piche J, Clayborne Z, Colman I. Adult mental health outcomes of adolescent depression: A systematic review. Depress Anxiety. 2018 Aug;35(8):700–716. doi: 10.1002/da.22777. [DOI] [PubMed] [Google Scholar]
- 4.Fergusson DM, Woodward LJ. Mental health, educational, and social role outcomes of adolescents with depression. Arch Gen Psychiatry. 2002 Mar;59(3):225–31. doi: 10.1001/archpsyc.59.3.225. [DOI] [PubMed] [Google Scholar]
- 5.Fergusson DM, Horwood LJ, Ridder EM, Beautrais AL. Subthreshold depression in adolescence and mental health outcomes in adulthood. Arch Gen Psychiatry. 2005 Jan;62(1):66–72. doi: 10.1001/archpsyc.62.1.66. [DOI] [PubMed] [Google Scholar]
- 6.McLeod GF, Horwood LJ, Fergusson DM. Adolescent depression, adult mental health and psychosocial outcomes at 30 and 35 years. Psychol Med. 2016 May;46(7):1401–12. doi: 10.1017/S0033291715002950. [DOI] [PubMed] [Google Scholar]
- 7.McKenzie M, Jorm AF, Romaniuk H, Olsson CA, Patton GC. Association of adolescent symptoms of depression and anxiety with alcohol use disorders in young adulthood: findings from the Victorian Adolescent Health Cohort Study. Med J Aust. 2011 Aug 01;195(3):S27–30. doi: 10.5694/j.1326-5377.2011.tb03262.x. [DOI] [PubMed] [Google Scholar]
- 8.Wolitzky-Taylor K, Dour H, Zinbarg R, Mineka S, Vrshek-Schallhorn S, Epstein A, Bobova L, Griffith J, Waters A, Nazarian M, Rose R, Craske MG. Experiencing core symptoms of anxiety and unipolar mood disorders in late adolescence predicts disorder onset in early adulthood. Depress Anxiety. 2014 Mar;31(3):207–13. doi: 10.1002/da.22250. [DOI] [PubMed] [Google Scholar]
- 9.Hawton K, Saunders KE, O'Connor RC. Self-harm and suicide in adolescents. Lancet. 2012 Jun 23;379(9834):2373–82. doi: 10.1016/S0140-6736(12)60322-5. [DOI] [PubMed] [Google Scholar]
- 10.Patton GC, Coffey C, Sawyer SM, Viner RM, Haller DM, Bose K, Vos T, Ferguson J, Mathers CD. Global patterns of mortality in young people: a systematic analysis of population health data. The Lancet. 2009 Sep;374(9693):881–892. doi: 10.1016/s0140-6736(09)60741-8. [DOI] [PubMed] [Google Scholar]
- 11.Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. 2015 Mar;56(3):345–65. doi: 10.1111/jcpp.12381. [DOI] [PubMed] [Google Scholar]
- 12.Avenevoli S, Swendsen J, He JP, Burstein M, Merikangas KR. Major depression in the national comorbidity survey-adolescent supplement: prevalence, correlates, and treatment. J Am Acad Child Adolesc Psychiatry. 2015 Jan;54(1):37–44.e2. doi: 10.1016/j.jaac.2014.10.010. http://europepmc.org/abstract/MED/25524788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Costello E, Copeland W, Angold A. Trends in psychopathology across the adolescent years: what changes when children become adolescents, and when adolescents become adults? J Child Psychol Psychiatry. 2011 Oct;52(10):1015–25. doi: 10.1111/j.1469-7610.2011.02446.x. http://europepmc.org/abstract/MED/21815892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ormel J, Raven D, van Oort F, Hartman CA, Reijneveld SA, Veenstra R, Vollebergh WA, Buitelaar J, Verhulst FC, Oldehinkel AJ. Mental health in Dutch adolescents: a TRAILS report on prevalence, severity, age of onset, continuity and co-morbidity of DSM disorders. Psychol Med. 2015 Jan;45(2):345–60. doi: 10.1017/S0033291714001469. [DOI] [PubMed] [Google Scholar]
- 15.Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005 Jun;62(6):593–602. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- 16.Kessler RC, Petukhova M, Sampson NA, Zaslavsky AM, Wittchen H. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res. 2012 Sep;21(3):169–84. doi: 10.1002/mpr.1359. http://europepmc.org/abstract/MED/22865617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Klein DN, Glenn CR, Kosty DB, Seeley JR, Rohde P, Lewinsohn PM. Predictors of first lifetime onset of major depressive disorder in young adulthood. J Abnorm Psychol. 2013 Feb;122(1):1–6. doi: 10.1037/a0029567. http://europepmc.org/abstract/MED/22889243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bennett K, Manassis K, Duda S, Bagnell A, Bernstein GA, Garland EJ, Miller LD, Newton A, Thabane L, Wilansky P. Treating child and adolescent anxiety effectively: Overview of systematic reviews. Clin Psychol Rev. 2016 Dec;50:80–94. doi: 10.1016/j.cpr.2016.09.006. [DOI] [PubMed] [Google Scholar]
- 19.James AC, James G, Cowdrey FA, Soler A, Choke A. Cognitive behavioural therapy for anxiety disorders in children and adolescents. Cochrane Database Syst Rev. 2013 Jun 03;(6):CD004690. doi: 10.1002/14651858.CD004690.pub3. [DOI] [PubMed] [Google Scholar]
- 20.Zhou X, Hetrick SE, Cuijpers P, Qin B, Barth J, Whittington CJ, Cohen D, Del Giovane C, Liu Y, Michael KD, Zhang Y, Weisz JR, Xie P. Comparative efficacy and acceptability of psychotherapies for depression in children and adolescents: A systematic review and network meta-analysis. World Psychiatry. 2015 Jun;14(2):207–22. doi: 10.1002/wps.20217. doi: 10.1002/wps.20217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Huang J, Nigatu YT, Smail-Crevier R, Zhang X, Wang J. Interventions for common mental health problems among university and college students: A systematic review and meta-analysis of randomized controlled trials. J Psychiatr Res. 2018 Dec;107:1–10. doi: 10.1016/j.jpsychires.2018.09.018. [DOI] [PubMed] [Google Scholar]
- 22.Mojtabai R, Olfson M, Han B. National Trends in the Prevalence and Treatment of Depression in Adolescents and Young Adults. Pediatrics. 2016 Dec;138(6):e20161878. doi: 10.1542/peds.2016-1878. http://pediatrics.aappublications.org/cgi/pmidlookup?view=long&pmid=27940701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Auerbach RP, Alonso J, Axinn WG, Cuijpers P, Ebert DD, Green JG, Hwang I, Kessler RC, Liu H, Mortier P, Nock MK, Pinder-Amaker S, Sampson NA, Aguilar-Gaxiola S, Al-Hamzawi A, Andrade LH, Benjet C, Caldas-de-Almeida JM, Demyttenaere K, Florescu S, de Girolamo G, Gureje O, Haro JM, Karam EG, Kiejna A, Kovess-Masfety V, Lee S, McGrath JJ, O'Neill S, Pennell B, Scott K, Ten Have M, Torres Y, Zaslavsky AM, Zarkov Z, Bruffaerts R. Mental disorders among college students in the World Health Organization World Mental Health Surveys. Psychol Med. 2016 Oct;46(14):2955–2970. doi: 10.1017/S0033291716001665. http://europepmc.org/abstract/MED/27484622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cadigan JM, Lee CM, Larimer ME. Young Adult Mental Health: a Prospective Examination of Service Utilization, Perceived Unmet Service Needs, Attitudes, and Barriers to Service Use. Prev Sci. 2019 Apr;20(3):366–376. doi: 10.1007/s11121-018-0875-8. http://europepmc.org/abstract/MED/29411197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Merikangas KR, He J, Burstein M, Swendsen J, Avenevoli S, Case B, Georgiades K, Heaton L, Swanson S, Olfson M. Service utilization for lifetime mental disorders in U.S. adolescents: results of the National Comorbidity Survey-Adolescent Supplement (NCS-A) J Am Acad Child Adolesc Psychiatry. 2011 Jan;50(1):32–45. doi: 10.1016/j.jaac.2010.10.006. http://europepmc.org/abstract/MED/21156268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gulliver A, Griffiths KM, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry. 2010 Dec 30;10:113. doi: 10.1186/1471-244X-10-113. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-10-113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Babajide A, Ortin A, Wei C, Mufson L, Duarte CS. Transition Cliffs for Young Adults with Anxiety and Depression: Is Integrated Mental Health Care a Solution? J Behav Health Serv Res. 2020 Apr;47(2):275–292. doi: 10.1007/s11414-019-09670-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Andersson G, Titov N. Advantages and limitations of Internet-based interventions for common mental disorders. World Psychiatry. 2014 Feb;13(1):4–11. doi: 10.1002/wps.20083. doi: 10.1002/wps.20083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.MacDonell KW, Prinz RJ. A Review of Technology-Based Youth and Family-Focused Interventions. Clin Child Fam Psychol Rev. 2017 Jun;20(2):185–200. doi: 10.1007/s10567-016-0218-x. http://europepmc.org/abstract/MED/27787701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sweeney GM, Donovan CL, March S, Forbes Y. Logging into therapy: Adolescent perceptions of online therapies for mental health problems. Internet Interv. 2019 Mar;15:93–99. doi: 10.1016/j.invent.2016.12.001. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(15)30018-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cuijpers P, Ebert D, Reijnders M, Stikkelbroek Y. Evidence-Based Psychotherapies for Children and Adolescents. New York: The Guildford Press; 2017. Technology-assisted treatments for mental health problems in children and adolescents; pp. 555–576. [Google Scholar]
- 32.Clinical Practice Guideline for the Treatment of Depression Across Three Age Cohorts. American Psychological Association. 2019. [2019-10-24]. https://www.apa.org/depression-guideline.
- 33.Karyotaki E, Riper H, Twisk J, Hoogendoorn A, Kleiboer A, Mira A, Mackinnon A, Meyer B, Botella C, Littlewood E, Andersson G, Christensen H, Klein JP, Schröder J, Bretón-López J, Scheider J, Griffiths K, Farrer L, Huibers MJ, Phillips R, Gilbody S, Moritz S, Berger T, Pop V, Spek V, Cuijpers P. Efficacy of Self-guided Internet-Based Cognitive Behavioral Therapy in the Treatment of Depressive Symptoms: A Meta-analysis of Individual Participant Data. JAMA Psychiatry. 2017 Apr 01;74(4):351–359. doi: 10.1001/jamapsychiatry.2017.0044. [DOI] [PubMed] [Google Scholar]
- 34.Andrews G, Basu A, Cuijpers P, Craske MG, McEvoy P, English CL, Newby JM. Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: An updated meta-analysis. J Anxiety Disord. 2018 Apr;55:70–78. doi: 10.1016/j.janxdis.2018.01.001. https://linkinghub.elsevier.com/retrieve/pii/S0887-6185(17)30447-4. [DOI] [PubMed] [Google Scholar]
- 35.Carlbring P, Andersson G, Cuijpers P, Riper H, Hedman-Lagerlöf E. Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: an updated systematic review and meta-analysis. Cogn Behav Ther. 2018 Jan;47(1):1–18. doi: 10.1080/16506073.2017.1401115. [DOI] [PubMed] [Google Scholar]
- 36.Ebert DD, Zarski A, Christensen H, Stikkelbroek Y, Cuijpers P, Berking M, Riper H. Internet and computer-based cognitive behavioral therapy for anxiety and depression in youth: a meta-analysis of randomized controlled outcome trials. PLoS One. 2015;10(3):e0119895. doi: 10.1371/journal.pone.0119895. https://dx.plos.org/10.1371/journal.pone.0119895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pennant ME, Loucas CE, Whittington C, Creswell C, Fonagy P, Fuggle P, Kelvin R, Naqvi S, Stockton S, Kendall T, Expert Advisory Group Computerised therapies for anxiety and depression in children and young people: a systematic review and meta-analysis. Behav Res Ther. 2015 Apr;67:1–18. doi: 10.1016/j.brat.2015.01.009. [DOI] [PubMed] [Google Scholar]
- 38.Vigerland S, Lenhard F, Bonnert M, Lalouni M, Hedman E, Ahlen J, Olén O, Serlachius E, Ljótsson B. Internet-delivered cognitive behavior therapy for children and adolescents: A systematic review and meta-analysis. Clin Psychol Rev. 2016 Dec;50:1–10. doi: 10.1016/j.cpr.2016.09.005. https://linkinghub.elsevier.com/retrieve/pii/S0272-7358(15)30090-8. [DOI] [PubMed] [Google Scholar]
- 39.Hollis C, Falconer CJ, Martin JL, Whittington C, Stockton S, Glazebrook C, Davies EB. Annual Research Review: Digital health interventions for children and young people with mental health problems - a systematic and meta-review. J Child Psychol Psychiatry. 2017 Apr;58(4):474–503. doi: 10.1111/jcpp.12663. [DOI] [PubMed] [Google Scholar]
- 40.Harrer M, Adam SH, Baumeister H, Cuijpers P, Karyotaki E, Auerbach RP, Kessler RC, Bruffaerts R, Berking M, Ebert DD. Internet interventions for mental health in university students: A systematic review and meta-analysis. Int J Methods Psychiatr Res. 2019 Jun;28(2):e1759. doi: 10.1002/mpr.1759. http://europepmc.org/abstract/MED/30585363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ye X, Bapuji SB, Winters SE, Struthers A, Raynard M, Metge C, Kreindler SA, Charette CJ, Lemaire JA, Synyshyn M, Sutherland K. Effectiveness of internet-based interventions for children, youth, and young adults with anxiety and/or depression: a systematic review and meta-analysis. BMC Health Serv Res. 2014 Jul 18;14:313. doi: 10.1186/1472-6963-14-313. https://bmchealthservres.biomedcentral.com/articles/10.1186/1472-6963-14-313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Podina IR, Mogoase C, David D, Szentagotai A, Dobrean A. A Meta-Analysis on the Efficacy of Technology Mediated CBT for Anxious Children and Adolescents. J Rat-Emo Cognitive-Behav Ther. 2015 Nov 17;34(1):31–50. doi: 10.1007/s10942-015-0228-5. [DOI] [Google Scholar]
- 43.Välimäki M, Anttila K, Anttila M, Lahti M. Web-Based Interventions Supporting Adolescents and Young People With Depressive Symptoms: Systematic Review and Meta-Analysis. JMIR Mhealth Uhealth. 2017 Dec 08;5(12):e180. doi: 10.2196/mhealth.8624. https://mhealth.jmir.org/2017/12/e180/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Grist R, Croker A, Denne M, Stallard P. Technology Delivered Interventions for Depression and Anxiety in Children and Adolescents: A Systematic Review and Meta-analysis. Clin Child Fam Psychol Rev. 2019 Jun;22(2):147–171. doi: 10.1007/s10567-018-0271-8. http://europepmc.org/abstract/MED/30229343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Karyotaki E, Ebert DD, Donkin L, Riper H, Twisk J, Burger S, Rozental A, Lange A, Williams AD, Zarski AC, Geraedts A, van Straten A, Kleiboer A, Meyer B, Ünlü Ince BB, Buntrock C, Lehr D, Snoek FJ, Andrews G, Andersson G, Choi I, Ruwaard J, Klein JP, Newby JM, Schröder J, Laferton JA, Van Bastelaar K, Imamura K, Vernmark K, Boß L, Sheeber LB, Kivi M, Berking M, Titov N, Carlbring P, Johansson R, Kenter R, Perini S, Moritz S, Nobis S, Berger T, Kaldo V, Forsell Y, Lindefors N, Kraepelien M, Björkelund C, Kawakami N, Cuijpers P. Do guided internet-based interventions result in clinically relevant changes for patients with depression? An individual participant data meta-analysis. Clin Psychol Rev. 2018 Jul;63:80–92. doi: 10.1016/j.cpr.2018.06.007. [DOI] [PubMed] [Google Scholar]
- 46.Baumeister H, Reichler L, Munzinger M, Lin J. The impact of guidance on Internet-based mental health interventions — A systematic review. Internet Interventions. 2014 Oct;1(4):205–215. doi: 10.1016/j.invent.2014.08.003. [DOI] [Google Scholar]
- 47.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009 Jul 21;6(7):e1000100. doi: 10.1371/journal.pmed.1000100. https://dx.plos.org/10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M. Cochrane handbook for systematic reviews of interventions. Hoboken: John Wiley & Sons; 2019. [Google Scholar]
- 49.Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng H, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JP. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019 Aug 28;366:l4898. doi: 10.1136/bmj.l4898. [DOI] [PubMed] [Google Scholar]
- 50.Schünemann H, Brozek J, Guyatt G, Oxman A. GRADE handbook for grading quality of evidence and strength of recommendations. The GRADE Working Group. 2013. [2019-10-24]. https://gdt.gradepro.org/app/handbook/handbook.html.
- 51.Cohen J. Statistical power analysis for the behavioral sciences. Cambridge: Academic Press; 2013. [Google Scholar]
- 52.Kraemer HC, Kupfer DJ. Size of treatment effects and their importance to clinical research and practice. Biol Psychiatry. 2006 Jun 01;59(11):990–6. doi: 10.1016/j.biopsych.2005.09.014. [DOI] [PubMed] [Google Scholar]
- 53.Laupacis A, Sackett DL, Roberts RS. An Assessment of Clinically Useful Measures of the Consequences of Treatment. N Engl J Med. 1988 Jun 30;318(26):1728–1733. doi: 10.1056/nejm198806303182605. [DOI] [PubMed] [Google Scholar]
- 54.Ioannidis JP, Patsopoulos NA, Evangelou E. Uncertainty in heterogeneity estimates in meta-analyses. BMJ. 2007 Nov 03;335(7626):914–6. doi: 10.1136/bmj.39343.408449.80. http://europepmc.org/abstract/MED/17974687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.von Hippel PT. The heterogeneity statistic I(2) can be biased in small meta-analyses. BMC Med Res Methodol. 2015 Apr 14;15:35. doi: 10.1186/s12874-015-0024-z. https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/s12874-015-0024-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000 Jun;56(2):455–63. doi: 10.1111/j.0006-341x.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- 57.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997 Sep 13;315(7109):629–34. doi: 10.1136/bmj.315.7109.629. http://europepmc.org/abstract/MED/9310563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Smith P, Scott R, Eshkevari E, Jatta F, Leigh E, Harris V, Robinson A, Abeles P, Proudfoot J, Verduyn C, Yule W. Computerised CBT for depressed adolescents: Randomised controlled trial. Behav Res Ther. 2015 Oct;73:104–10. doi: 10.1016/j.brat.2015.07.009. [DOI] [PubMed] [Google Scholar]
- 59.Botella C, Gallego MJ, Garcia-Palacios A, Guillen V, Baños RM, Quero S, Alcañiz M. An Internet-based self-help treatment for fear of public speaking: a controlled trial. Cyberpsychol Behav Soc Netw. 2010 Aug;13(4):407–21. doi: 10.1089/cyber.2009.0224. [DOI] [PubMed] [Google Scholar]
- 60.Sethi S. Treating Youth Depression and Anxiety: A Randomised Controlled Trial Examining the Efficacy of Computerised versus Face-to-face Cognitive Behaviour Therapy. Australian Psychologist. 2013 Feb 14;48(4):249–257. doi: 10.1111/ap.12006. doi: 10.1111/ap.12006. [DOI] [Google Scholar]
- 61.Ellis L, Campbell A, Sethi S, O'Dea B. Comparative randomized trial of an online cognitive-behavioral therapy program and an online support group for depression and anxiety. Journal of CyberTherapy and Rehabilitation. 2011;4(4):461–467. [Google Scholar]
- 62.Sethi S, Campbell A, Ellis L. The Use of Computerized Self-Help Packages to Treat Adolescent Depression and Anxiety. Journal of Technology in Human Services. 2010 Aug 31;28(3):144–160. doi: 10.1080/15228835.2010.508317. doi: 10.1080/15228835.2010.508317. [DOI] [Google Scholar]
- 63.Spence SH, Donovan CL, March S, Gamble A, Anderson RE, Prosser S, Kenardy J. A randomized controlled trial of online versus clinic-based CBT for adolescent anxiety. J Consult Clin Psychol. 2011 Oct;79(5):629–42. doi: 10.1037/a0024512. [DOI] [PubMed] [Google Scholar]
- 64.Waite P, Marshall T, Creswell C. A randomized controlled trial of internet-delivered cognitive behaviour therapy for adolescent anxiety disorders in a routine clinical care setting with and without parent sessions. Child Adolesc Ment Health. 2019 Sep;24(3):242–250. doi: 10.1111/camh.12311. [DOI] [PubMed] [Google Scholar]
- 65.Poppelaars M, Tak YR, Lichtwarck-Aschoff A, Engels RC, Lobel A, Merry SN, Lucassen MF, Granic I. A randomized controlled trial comparing two cognitive-behavioral programs for adolescent girls with subclinical depression: A school-based program (Op Volle Kracht) and a computerized program (SPARX) Behav Res Ther. 2016 May;80:33–42. doi: 10.1016/j.brat.2016.03.005. [DOI] [PubMed] [Google Scholar]
- 66.Merry SN, Stasiak K, Shepherd M, Frampton C, Fleming T, Lucassen MF. The effectiveness of SPARX, a computerised self help intervention for adolescents seeking help for depression: randomised controlled non-inferiority trial. BMJ. 2012 Apr 18;344:e2598. doi: 10.1136/bmj.e2598. http://www.bmj.com/cgi/pmidlookup?view=long&pmid=22517917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Fleming T, Dixon R, Frampton C, Merry S. A pragmatic randomized controlled trial of computerized CBT (SPARX) for symptoms of depression among adolescents excluded from mainstream education. Behav Cogn Psychother. 2012 Oct;40(5):529–41. doi: 10.1017/S1352465811000695. [DOI] [PubMed] [Google Scholar]
- 68.Fitzpatrick KK, Darcy A, Vierhile M. Delivering Cognitive Behavior Therapy to Young Adults With Symptoms of Depression and Anxiety Using a Fully Automated Conversational Agent (Woebot): A Randomized Controlled Trial. JMIR Ment Health. 2017 Jun 06;4(2):e19. doi: 10.2196/mental.7785. https://mental.jmir.org/2017/2/e19/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Clarke G, Kelleher C, Hornbrook M, Debar L, Dickerson J, Gullion C. Randomized effectiveness trial of an Internet, pure self-help, cognitive behavioral intervention for depressive symptoms in young adults. Cogn Behav Ther. 2009;38(4):222–34. doi: 10.1080/16506070802675353. http://europepmc.org/abstract/MED/19440896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Bowler JO, Mackintosh B, Dunn BD, Mathews A, Dalgleish T, Hoppitt L. A comparison of cognitive bias modification for interpretation and computerized cognitive behavior therapy: effects on anxiety, depression, attentional control, and interpretive bias. J Consult Clin Psychol. 2012 Dec;80(6):1021–33. doi: 10.1037/a0029932. http://europepmc.org/abstract/MED/22963595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Ip P, Chim D, Chan KL, Li TM, Ho FK, Van Voorhees BW, Tiwari A, Tsang A, Chan CW, Ho M, Tso W, Wong WH. Effectiveness of a culturally attuned Internet-based depression prevention program for Chinese adolescents: A randomized controlled trial. Depress Anxiety. 2016 Dec;33(12):1123–1131. doi: 10.1002/da.22554. [DOI] [PubMed] [Google Scholar]
- 72.McCall HC, Richardson CG, Helgadottir FD, Chen FS. Evaluating a Web-Based Social Anxiety Intervention Among University Students: Randomized Controlled Trial. J Med Internet Res. 2018 Mar 21;20(3):e91. doi: 10.2196/jmir.8630. https://www.jmir.org/2018/3/e91/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Day V, McGrath PJ, Wojtowicz M. Internet-based guided self-help for university students with anxiety, depression and stress: a randomized controlled clinical trial. Behav Res Ther. 2013 Jul;51(7):344–51. doi: 10.1016/j.brat.2013.03.003. [DOI] [PubMed] [Google Scholar]
- 74.Lenhard F, Andersson E, Mataix-Cols D, Rück C, Vigerland S, Högström J, Hillborg M, Brander G, Ljungström M, Ljótsson B, Serlachius E. Therapist-Guided, Internet-Delivered Cognitive-Behavioral Therapy for Adolescents With Obsessive-Compulsive Disorder: A Randomized Controlled Trial. J Am Acad Child Adolesc Psychiatry. 2017 Jan;56(1):10–19.e2. doi: 10.1016/j.jaac.2016.09.515. https://linkinghub.elsevier.com/retrieve/pii/S0890-8567(16)31857-3. [DOI] [PubMed] [Google Scholar]
- 75.Richards D, Timulak L, Rashleigh C, McLoughlin O, Colla A, Joyce C, Doherty G, Sharry J, Duffy D, Anderson-Gibbons M. Effectiveness of an internet-delivered intervention for generalized anxiety disorder in routine care: A randomised controlled trial in a student population. Internet Interv. 2016 Nov;6:80–88. doi: 10.1016/j.invent.2016.10.003. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(16)30029-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Stjerneklar S, Hougaard E, McLellan LF, Thastum M. A randomized controlled trial examining the efficacy of an internet-based cognitive behavioral therapy program for adolescents with anxiety disorders. PLoS One. 2019;14(9):e0222485. doi: 10.1371/journal.pone.0222485. https://dx.plos.org/10.1371/journal.pone.0222485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Tillfors M, Andersson G, Ekselius L, Furmark T, Lewenhaupt S, Karlsson A, Carlbring P. A randomized trial of Internet-delivered treatment for social anxiety disorder in high school students. Cogn Behav Ther. 2011;40(2):147–57. doi: 10.1080/16506073.2011.555486. [DOI] [PubMed] [Google Scholar]
- 78.Wuthrich VM, Rapee RM, Cunningham MJ, Lyneham HJ, Hudson JL, Schniering CA. A randomized controlled trial of the Cool Teens CD-ROM computerized program for adolescent anxiety. J Am Acad Child Adolesc Psychiatry. 2012 Mar;51(3):261–70. doi: 10.1016/j.jaac.2011.12.002. [DOI] [PubMed] [Google Scholar]
- 79.Topooco N, Berg M, Johansson S, Liljethörn L, Radvogin E, Vlaescu G, Nordgren LB, Zetterqvist M, Andersson G. Chat- and internet-based cognitive-behavioural therapy in treatment of adolescent depression: randomised controlled trial. BJPsych Open. 2018 Jul;4(4):199–207. doi: 10.1192/bjo.2018.18. https://www.cambridge.org/core/product/identifier/S2056472418000182/type/journal_article. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Stallard P, Richardson T, Velleman S, Attwood M. Computerized CBT (Think, Feel, Do) for depression and anxiety in children and adolescents: outcomes and feedback from a pilot randomized controlled trial. Behav Cogn Psychother. 2011 May;39(3):273–84. doi: 10.1017/S135246581000086X. [DOI] [PubMed] [Google Scholar]
- 81.van der Zanden R, Kramer J, Gerrits R, Cuijpers P. Effectiveness of an online group course for depression in adolescents and young adults: a randomized trial. J Med Internet Res. 2012 Jun 07;14(3):e86. doi: 10.2196/jmir.2033. https://www.jmir.org/2012/3/e86/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Andersson G, Rozental A, Shafran R, Carlbring P. Long-term effects of internet-supported cognitive behaviour therapy. Expert Rev Neurother. 2018 Jan;18(1):21–28. doi: 10.1080/14737175.2018.1400381. [DOI] [PubMed] [Google Scholar]
- 83.Donkin L, Christensen H, Naismith SL, Neal B, Hickie IB, Glozier N. A systematic review of the impact of adherence on the effectiveness of e-therapies. J Med Internet Res. 2011 Aug 05;13(3):e52. doi: 10.2196/jmir.1772. https://www.jmir.org/2011/3/e52/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Schulz KF, Altman DG, Moher D, CONSORT Group CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMC Med. 2010 Mar 24;8:18. doi: 10.1186/1741-7015-8-18. https://bmcmedicine.biomedcentral.com/articles/10.1186/1741-7015-8-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Eysenbach G, CONSORT-EHEALTH Group CONSORT-EHEALTH: improving and standardizing evaluation reports of Web-based and mobile health interventions. J Med Internet Res. 2011 Dec 31;13(4):e126. doi: 10.2196/jmir.1923. https://www.jmir.org/2011/4/e126/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Arjadi R, Nauta MH, Chowdhary N, Bockting CL. A systematic review of online interventions for mental health in low and middle income countries: a neglected field. Glob Ment Health (Camb) 2015;2:e12. doi: 10.1017/gmh.2015.10. http://europepmc.org/abstract/MED/28596860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.World Health Organization . mhGAP: Mental Health Gap Action Programme: scaling up care for mental, neurological and substance use disorders. Geneva: WHO Press; 2008. [PubMed] [Google Scholar]
- 88.World Health Organization . mhGAP Intervention Guide for mental, neurological and substance use disorders in non-specialized health settings. Geneva: WHO Press; 2011. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strings.
Selected characteristics of the included studies examining the effects of computerized cognitive behavior therapy for depression and anxiety in adolescents and young adults.
Adherence rates of the included studies examining the effects of computerized cognitive behavior therapy for depression and anxiety in adolescents and young adults.
Risk of bias classification for each study.
Forest plot with standardized posttreatment effect sizes (Hedges g) regarding depressive symptoms for computerized cognitive behavior therapy compared with active treatment control conditions.
Forest plot with standardized posttreatment effect sizes (Hedges g) regarding depressive symptoms for computerized cognitive behavior therapy compared with passive control conditions.
Forest plot with standardized posttreatment effect sizes (Hedges g) regarding anxiety symptoms for computerized cognitive behavior therapy compared with active treatment control conditions.
Forest plot with standardized posttreatment effect sizes (Hedges g) regarding anxiety symptoms for computerized cognitive behavior therapy compared with passive control conditions.