

Abstract
Corrosive injury is a devastating injury which carries significant morbidity. The upper gastrointestinal tract is predominantly affected with severity ranging from mild inflammation to full thickness necrosis which may result in perforation and death. Among the complications, stricture formation is most common, causing dysphagia and malnutrition. Endoscopy has a pivotal role in the diagnosis and management, with a few shortcomings. Imaging has an important role to play. Besides radiography, there is an increasing role of CT scan in the emergency setting with good accuracy in identifying patients who are likely to benefit from surgery. Further, CT scan has a role in the diagnosis of complications. Oral contrast studies help in assessing the severity and extent of stricture formation and associated fistulous complications in the subacute and chronic phase. The scope of intervention radiology for this condition is increasing. Fluoroscopy-guided balloon dilatation, drainage of collections or mucoceles, endovascular embolization of point bleeders, placement of feeding jejunostomy and image-guided biopsy are among the procedures that are being performed. Through this review we aim to stress the role the radiologist plays in the diagnosis and follow-up of these patients and in performing radiological interventions. Besides this, we have also highlighted few salient points to help understand the pathophysiology and management of such injuries which is paramount to ensure a good long-term outcome.
Introduction
Corrosive injuries of the gastrointestinal tract (GIT), although uncommon, are devastating and, in severe cases, are associated with significant morbidity and mortality.1 The nature and incidence of ingestion is different for developed and developing countries, with the incidence being higher in the lower socio-economic group.2 Accidental ingestion is more common in younger age group whereas in adults, suicidal intent is frequently encountered.2,3
Corrosive ingestion predominantly affects the upper GIT, from the oral cavity to the stomach. In the acute stage, the injury varies from mild inflammation to lethal form, whereas in the chronic stage, stricture formation is common which leads to dysphagia and malnutrition.4,5 Management of these patients requires a multidisciplinary team approach. Imaging plays a critical role in evaluating the affected organs, both in the acute and chronic settings. Another major role of a radiologist is to perform radiological interventions whenever necessary. In this review, we briefly present the pathophysiological and clinical features of corrosive injury of the upper GIT along with detailed illustration of the various imaging findings and brief discussion on the relevant radiological interventions performed in this setting.
Properties of corrosive agents and pathophysiology
A corrosive agent causes destruction of the tissue with which it comes in contact. They are broadly classified into acid and alkali.2 Basic knowledge of the properties of these agents helps in better understanding the pathophysiology of the injury caused by them. Alkali ingestion is common in the Western countries whereas acid ingestion is more common in developing countries, with sulphuric acid being the most common agent (seen in 68.75% cases).4,6,7
Acids have a pungent odour and noxious taste, which accounts for the smaller quantity frequently ingested and the immediate vomiting.6 They are less viscous and cause coagulative necrosis with formation of an eschar. This acts as a barrier for further penetration of the acid, limiting the depth of injury.8 Another property of acids is their potential to cause pylorospasm, resulting in stasis and increased contact time of the ingested agent in the pre-pyloric region and thus, development of an antropyloric stricture.9,10 The common acids which are commercially available are in the form of toilet cleaners (hydrochloric acid), storage battery acids (sulphuric acid), jewellery cleaners (hydrochloric and nitric acid in a 3:1 proportion), and certain metal cleaners (phosphoric acid).
Alkalis, on the other hand, are tasteless and odourless, and thus larger quantities are usually ingested.6 They are more viscous, which leads to longer contact time with the tissue and cause liquefactive necrosis, thus resulting in deeper penetration and increased risk of adjacent organ injury.4 Alkalis have neutralising action on the acid in the stomach and avoid pyloric spasm, making the stomach less prone to injury.10 The common alkalis available are drain cleaners (30% liquid sodium hydroxide) and household cleaners (70% sodium hypochlorite).
Although it was initially thought that acids more commonly affect the stomach and alkalis, the oesophagus’ this belief has been recently questioned.4 Strong acids and alkali (pH <2 and >12, respectively) cause more severe and transmural injury and can also cause systemic side effects such as electrolyte imbalances.11
The nature of injury caused by a corrosive agent depends upon various factors such as the type and property of the ingested agent, its concentration and the intent of ingestion with injury being more severe in suicidal as compared to accidental ingestion.5 When the agent is in solid form or is immediately expelled, the organs which suffer significant injury are the oral cavity, pharynx and upper oesophagus. In cases where the agent is in liquid form or is ingested in larger quantities, the distal oesophagus and the stomach are mostly affected.5 The pathological changes are usually similar with both these agents. Based on the time elapsed after ingestion of the corrosive agent, pathological changes in the upper GIT vary and have been divided into three phases.12
Phase I (within 24 h): Initially, there are mucosal erosions and ulcerations followed by small vessel thrombosis, haemorrhage and inflammation. With increasing severity, there is extensive thrombosis of the submucosal vessels that leads to necrosis of the mucosa and then transmural necrosis, which may result in perforation.
Phase II (1–2 weeks): In the first week following injury, granulation tissue begins to replace the mucosal slough. Fibroblast infiltration starts around the second week and this marks the beginning of tissue repair.
Phase III (third week to months): In this phase, there is increased fibroblastic activity and scarring which results in the formation of a stricture in due course of time. There is completion of re-epithelisation by the sixth week.
Clinical presentation
In the presence of relevant history, the diagnosis is obvious. In the acute phase of the illness, patients present with intense oropharyngeal and chest pain, associated with vomiting, excessive salivation and drooling.12 Haematemesis may also be present in few cases. Upper airway involvement leads to respiratory distress, stridor and hoarseness. Severe chest pain radiating to the back, with episodes of fever and cough may suggest oesophageal perforation.13 Epigastric pain or severe abdominal pain can occur in the presence of gastric injury.
In the chronic phase, scarring and fibrosis lead to oesophageal stricture which present as dysphagia, regurgitation, substernal discomfort or recurrent aspiration.8,14 Gastric strictures present with vomiting, early satiety and weight loss.8 Laryngeal or epiglottic involvement may lead to stridor, hoarseness or recurrent aspirations.15 Recurrent pulmonary infections are noted in cases of oesophago-bronchial or oesophago-pulmonary fistulas. In long-standing cases, years after the episode of ingestion, there may be malignant transformation of the involved segment of the GIT (more common with alkali ingestion) and the patients may present with new onset or progressive dysphagia and neck or chest pain.16
Imaging modalities
Diagnosis is usually based on history and clinical examination. Radiological investigations help in assessing the severity of injury and aiding further management.
Plain radiograph
Chest and abdominal radiographs are usually the initial investigations carried out in the emergency setting. The findings on the chest radiograph include pleural effusion, pneumomediastinum, pneumothorax as well as nodules and consolidation secondary to aspiration pneumonitis (Figure 1).17 Abdominal radiograph may help in the diagnosis of pneumoperitoneum in cases of hollow visceral perforation.18 Radiographs also help in the detection of metallic foreign bodies such as button batteries.18,19
Figure 1.

Plain radiographs. (a) Chest radiograph of a 40-year-old male with suicidal acid ingestion with subsequent oesophageal perforation showing left hydropneumothorax. (b) Chest radiograph of a 35-year-old male 1 week after suicidal acid ingestion shows pneumomediastinum with large left pleural effusion. (c) Abdominal radiograph of a 45-year-old female with acid ingestion showing pneumoperitoneum due to gastric perforation.
Barium or oral contrast studies
In the acute phase, endoscopy is more important in severity assessment and oral contrast studies have a limited role.12 They are usually not indicated as barium can cause inflammatory reaction in the extraluminal tissues in the event of perforation and oral iodinated contrast medium may cause pulmonary oedema, if aspirated.20 Use of iso-osmolar non-ionic or low osmolar contrast medium is preferred due to lower risk of pulmonary oedema.20 Oral contrast studies are usually performed once the patient is able to swallow liquids and are helpful in the patients planned for non-operative management. Findings on the contrast study in the acute or subacute phase include diffuse oesophageal narrowing,(Figure 2A) reduced peristalsis of the oesophagus and stomach with low-amplitude contractions, mucosal ulcerations and, in cases of transmural necrosis and perforation, leak of contrast into the airway, mediastinum, pleural cavity or peritoneal cavity.21
Figure 2.

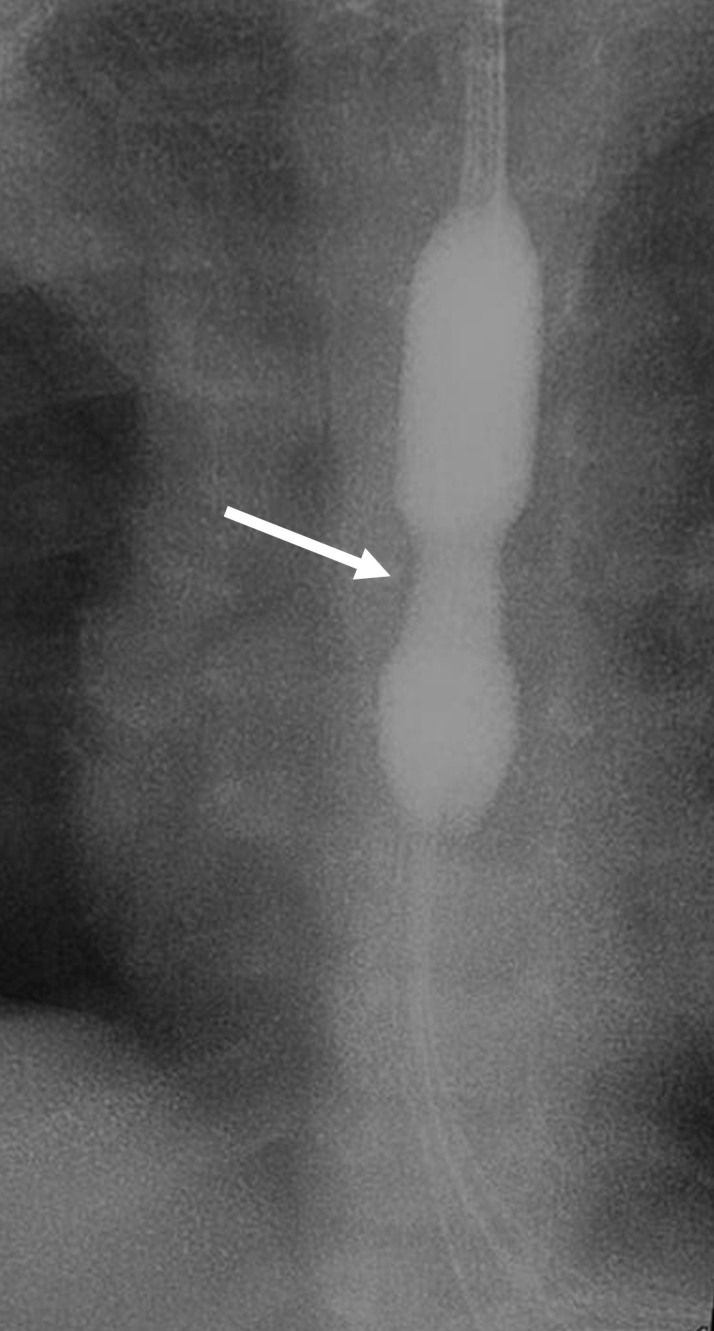
Barium studies. Acute stage. (a) Barium swallow of a 20-year-old female, presenting with dysphagia, one day after corrosive ingestion shows long segment under distensibility of the thoracic oesophagus (arrows) with reduced frequency and strength of primary peristalsis (seen on fluoroscopy). Chronic stage. (b) 18-year-old female with accidental acid ingestion shows deformity of bilateral vallecula and pyriform sinus (arrows) with complete stricture. (c) A 20-year-old female with history of suicidal acid ingestion shows short segment stricture in the hypopharynx and upper cervical oesophagus (arrow). (d) A 19-year-old girl with alkali ingestion shows a long-segment stricture in the oesophagus (white arrow) with multiple diverticula (black arrows). (e) A 32-year-old female with acid ingestion shows long-segment stricture with contained leak of barium into mediastinum (arrow). (f) A 20-year-old male with suicidal acid ingestion shows distal gastric stricture with diverticula in the gastric wall (arrows).
The ideal time to perform barium studies is around the third week, when they can reliably define the characteristics of the various abnormalities, particularly strictures, of the upper GIT.22,23 They help to assess the severity and the extent of the disease prior to endoscopic or surgical treatment.21,23 Furthermore, they may demonstrate the presence of any fistulous communications with adjacent viscera (trachea, bronchi, lungs, pleura, peritoneum), diverticula, abnormal oesophageal motility and gastro-oesophageal reflux (Figure 2).11 Another important role of oral contrast study is in the evaluation of post-operative patients, either for anastomotic site leaks immediately after surgery or for anastomotic strictures during follow-up.
Endoscopy
Endoscopy plays a crucial role in the diagnosis and management of patients with corrosive injury. Endoscopy is usually performed within 24–48 h after ingestion, and initial endoscopy after 96 h of corrosive ingestion is not advised because the injured oesophagus is in the phase of ulceration and granulation tissue formation, when it is fragile and easily perforated.24,25 Endoscopic findings in acute setting help to classify patients based on the severity of mucosal injury and helps in prognostication (Figure 3A and B). The Zargar classification is used for grading the early endoscopic findings and treatment varies based on the severity of grading (Table 1).25 Patients with no evidence of mucosal injury may be discharged timely leading to reduced cost of hospital stay. In patients with grade III injury based on endoscopy, surgery is usually indicated. However, endoscopy is unable to differentiate between superficial and transmural necrosis and based on endoscopy alone unnecessary surgeries may be performed.24,26
Figure 3.

Endoscopy. Acute stage. (a) Endoscopy images of two patients of acute corrosive injury show areas of linear ulcers and necrosis in the oesophagus and (b) bleeding from circumferential esophageal ulcers.Chronic stage. (c) Endoscopy image shows oesophageal stricture after 3 months of corrosive injury. (d) Endoscopy image shows minimal residual stricture in the oesophagus after multiple sessions of dilatation with oesophagus showing pseudotrachealisation. [Image courtesy: Dr Soumya Jagannath and Dr Pramod K Garg, Department of Gastroenterology, All India Institute of Medical Sciences, New Delhi, India].
Table 1.
Zargar endoscopic grading of acute corrosive injury
| Zargar score | Endoscopic findings | Prognosis and treatment |
| I | Oedema and hyperaemia of the mucosa | Stricture formation is very unlikely; patients can start oral feeds and are discharged. |
| IIa | Friability, haemorrhages, erosion, blisters, whitish membranes, exudates and superficial ulcerations | |
| IIb | Grade IIa with deep or circumferential ulceration | Stricture formation likely in 30–70% of patients Follow up with barium swallow at 3 weeks and balloon dilatation, if required. |
| IIIa | Small scattered areas of necrosis | Esophageal strictures form in up to 90%. Risk of perforation |
| IIIb | Extensive necrosis | Emergency surgery is recommended. |
| IV | Perforation |
In the chronic stage, endoscopy plays a role in the diagnosis and treatment of strictures (Figure 3C and D). Endoscopic dilatation of strictures is usually done at 3 weeks, after its diagnosis on barium swallow study.24 In addition to dilatation, procedures such as electrocision, intralesional steroid or mitomycin-C injection and oesophageal stent placement may be performed for refractory strictures.27
Computed Tomography (CT) scan
Emergency CT is increasingly being used in the evaluation of acute corrosive injury.5,28,29 In view of the disadvantages of endoscopy described above, CT becomes a good alternative to assess the degree of injury and triage patients for management.5 The World Society of Emergency Surgery consensus conference in 2015 supported and reinforced the use of emergency CT scan in the management of acute corrosive injury.10
CT is increasingly being used to grade acute corrosive injury. Ryu et al, proposed a classification system for corrosive injury of the upper GIT based on CT findings and showed that it was better than the endoscopic grading in predicting long-term complications.28 The grading system by Ryu et al, defines four grades with good endoscopic correlation (Figure 4).28 Grade I: normal wall (thickness <3 mm); Grade II: wall oedema only (thickness >3 mm); Grade III: wall oedema with surrounding soft tissue stranding, with sharp interface; and Grade IV: wall oedema with surrounding soft tissue stranding and ill-defined interface with or without collection. Following this, Lurie et al, in their study, concluded that early endoscopy is more sensitive and cannot be replaced by CT alone.30 Their grading were similar to that of Ryu et al, except that their highest grade included air bubbles in the organ wall and around it. Although CT had a high sensitivity of 90%, the specificity was only 30–40%. This conclusion was challenged by other studies which found that using CT for Grade 3b injuries improved patient survival and decreased management costs and CT outperformed endoscopy in deciding between operative and non-operative management.26,31 The high interobserver agreement between specialised and general radiologists in assessing the oesophagus for transmural involvement allows this modality to be used outside tertiary-care centres.5 Based on the presence and extent of oesophageal and gastric wall enhancement on CT scan, which determines viability, another classification was defined by Chirica et al.5 Their classification is defined as follows: Grade I: normal appearing organs; Grade II: wall oedema with surrounding soft tissue inflammation and post-contrast wall enhancement; and Grade III: absence of post-contrast wall enhancement, suggesting transmural involvement. Although the classification by Ryu et al, is commonly used at present, the classification by Chirica et al, adds wall enhancement as a criterion making it more suitable for deciding clinical management.
Figure 4.

CT grades of acute corrosive injury (Ryu et al) of upper gastrointestinal tract with schematic diagrams and corresponding CT images. (a–c): Grade I: Normal wall thickness (<3 mm) and enhancement. Oesophagus may be dilated due to motility changes (arrows in b and c). (d–f): Grade II: Wall oedema (>3 mm thick) with hypo-enhancement. Normal serosa or adventitia (arrows in e and f). G–I: Grade III: Wall oedema (>3 mm thick) with surrounding soft tissue stranding (arrows in h and i). Sharp interface maintained with serosa (arrows). (j–l): Grade IV: Wall oedema (>3 mm thick) with surrounding soft tissue stranding (arrow in k) or collection (arrow in l) with loss of sharp interface with serosa.
The standard CT protocol is to perform a scan from the neck to the iliac crest level after administration of intravenous iodinated contrast agent. In cases of additional or predominant abdominal symptoms, extension of the scan to include the pelvis becomes necessary. Chirica et al, have suggested performing a non-contrast scan prior to contrast scans for better definition of the extent of injury.5
Besides oesophageal and gastric evaluation, CT scan also allows assessment of the chest, including the mediastinum and the abdomen for associated findings.30 These include aspiration changes in the lungs, presence of pleural effusion, mediastinal inflammation or collection, abdominal collections, pneumoperitoneum and vascular complications like pseudoaneurysm.
In the chronic setting, CT scan has limited role. However, it can be used as an adjunct to oral contrast studies in the evaluation of pharyngeal, oesophageal and gastric morphology in patients with absolute dysphagia (Figure 5). It is also useful in the assessment of long-term complications like aspiration pneumonitis, oesophageal – airway fistulas, oesophageal or gastric mucocele formation due to post-surgical isolation or closed obstruction due to severe strictures at two sites and more importantly, malignancies developing in the oesophagus post-caustic injury.32 Furthermore, CT scan helps in the evaluation of post-operative complications and can act as a guide for interventions like drainage of collections and mucoceles.33
Figure 5.

A 31-year-old female with suicidal acid ingestion. (a) Barium study shows long-segment stricture of distal stomach (black arrow) with diverticula (white arrows). (b) Coronal CT image shows gross low-density smooth thickening of distal body of the stomach (arrow) consistent with fibrosis.
Complications of corrosive ingestion
Strictures: These are the most common complication of corrosive injury and commonly involve the oesophagus and stomach.5,8 They are typically long segment and usually have a smooth outline (Figures 2 and 5). However, in long-standing cases, there may be irregularity due to asymmetric strictures, diverticula and contained leaks.34 Short segment strictures may also be seen and are often amenable to endoscopic or fluoroscopic balloon dilatation.
Haemorrhage: Bleeding is a rare complication and usually presents in the subacute phase of injury, that is, 3rd −4th week of injury.35 It has high mortality and morbidity.35 It usually presents as sentinel bleed, one or two days before a life-threatening bleeding. The corrosive agent erodes the viscera and causes vascular injury which may result in active leak or formation of a pseudoaneurysm. These cases can be managed either by surgery or by endovascular embolization of the bleeding site (Figure 6). CT angiography is often necessary for the diagnosis of the cause and source of bleeding prior to treatment.
Figure 6.

A 27-year-old female, presenting with haematemesis, 3 weeks after corrosive intake. (a): Coronal CT image shows a small pseudoaneurysm arising from right gastro-epiploic artery (arrow). (b–c): Digital subtraction angiography images of gastroduodenal artery show the pseudoaneurysm (arrow in c), which was successfully embolized using n-butyl cyanoacrylate (arrow in c).
Pulmonary complications: Pulmonary complications include pneumonia secondary to aspiration and opportunistic infections in the lung secondary to reduced immune status and malnutrition (Figure 7).36 Other rare complications are fistulas such as oesophago-bronchial fistula, oesophago-pulmonary fistula or oesophago-pleural fistula or leaks, particularly in the acute stage (Figure 7).37 Occasionally, there may be spontaneous rupture of an oesophageal mucocele into the airway.38
Figure 7.

Pulmonary complications. (a, b) A 32-year-old male with history of corrosive injury presenting with recurrent cough. Barium swallow (a) shows contrast agent in both bronchi (arrows) and axial CT scan (b) shows fistulous communication between the oesophagus and left main bronchus (arrow). (c–d) A 20-year-old male with history of suicidal alkali ingestion and repeated chest infections. Barium swallow (c) shows leak of contrast agent into an area of retrocardiac consolidation (arrow) and axial CT image (d) shows oesophago-pulmonary fistula and left lower lobe consolidation with oral contrast agent in the alveoli. (e–f) A 34-year-old male, with history of gastric pull up for corrosive injury, presenting with cough, fever and weight loss. Axial CT images, mediastinal (e) and lung (f) windows show necrotic mediastinal nodes (arrow), nodules in left lower lobe (circle) and bilateral pleural effusion (asterisks) suggestive of pulmonary tuberculosis.
Perforation and collections: Perforation and development of collections are uncommon complications and typically occur in the acute stage and is associated with full thickness necrosis of the oesophagus or stomach.22 Esophageal perforation may result in pneumomediastinum and mediastinitis which may lead to formation of mediastinal abscess. In cases of full thickness stomach injury, pneumoperitoneum and abdominal collections may develop.17,22 Involvement of contiguous organs such as transverse colon and pancreas may also occur in rare instances.39
Surgical complications: In the post-operative period, these patients may develop anastomotic site leaks and collections (Figure 8), presenting with fever and/or leucocytosis. Oral contrast studies and CT scan help to identify the site of leak and collection and aid in aspiration or drainage. One of the late surgical complications is the development of anastomotic site stricture (Figure 8).40 These patients present with persistent or recurrent dysphagia. Rarely, in the late post-operative period, the surgically isolated oesophagus or stomach with an intact epithelium may distend due to retained secretions resulting in a mucocele (Figure 8).41 However, in most situations, this does not happen as the mucosa is destroyed by chronic inflammation and scarring.42 Larger mucoceles present as chest pain, dysphagia, abdominal pain and, rarely, respiratory distress due to airway compression.41 Definitive management is oesophagectomy or gastrectomy or a gastrojejunostomy. Sometimes, as a bridging or temporary procedure, image-guided drainage of the mucocele can be performed. Chemical ablation of the mucocele has also been reported.43
Figure 8.

Surgical complications. (a–b). A 23-year-old male with presenting with fever after oesophagectomy and colonic interposition. Axial CT scans show collections in the neck (arrow in a) and pleural cavity (arrow in b). (c) A 17-year-old girl with persistent dysphagia post-surgery. Barium swallow shows proximal anastomotic site stricture (arrow). (d–e) A 19-year-old male post-retrosternal gastric pull-up presenting with chest pain and respiratory discomfort. Coronal (d) and axial (e) CT scans show mucocele formation in the isolated native oesophagus (arrow).
Malignancy: Although this complication is rare, a few cases of squamous cell carcinoma have been reported in long-standing caustic injury of the oesophagus. The incidence of developing oesophageal malignancy is low (3–7.2%).16,32 Imaging with CT scan is required in patients presenting with progressive symptoms and weight loss (Figure 9).32 A few case reports have also shown squamous metaplasia and cancer developing in the stomach post-corrosive injury.44
Figure 9.

Malignancy. A 54-year-old male, with history of retrosternal gastric pull-up for corrosive intake, 14 years ago, presenting with increasing upper chest pain. (a) Axial CT scan shows a homogeneous mass (thin arrow) in the region of the native oesophagus encasing aorta. Pulled-up stomach is noted (block arrow). (b) CT-guided biopsy of the mass through extrapleural route showed squamous cell carcinoma.
Management
Management depends on the time of presentation. Initial management includes resuscitation with airway management and haemodynamic stabilisation.11 There is varied consensus on the placement of naso-gastric tube in patients with acute corrosive injury with no uniform recommendations.10 Oesophageal catheterisation with a nasogastric tube may induce vomiting and retching which can increase the exposure of the oesophageal mucosa to the corrosive agent. The procedure also increases the risk of oesophageal perforation. Furthermore, its role in preventing vomiting and stricture formation is controversial and it may cause long-segment strictures, act as a nidus for infection and may worsen reflux.11 However, nasogastric tube placement can help to maintain luminal patency, may be helpful in initiating early enteral feeding and provide alumen for future dilatation.45 This decision, therefore, is based on the institutional protocol and individual case. Most experts prefer to place a nasogastric tube, whenever required, under endoscopic guidance to avoid the risks of blind placement.10
In the acute phase, low-grade injuries are managed conservatively.46 An oral contrast study is usually performed at follow-up. High-grade injuries require radical surgery with resection of the necrosed viscera (oesophagectomy, gastrectomy and oesophago-gastrectomy) along with a feeding jejunostomy. The common indications for surgery in the acute phase are the presence of oesophageal perforation, transmural injury, peritonitis and massive haematemesis.5,29
In the late phase, fibrosis and scarring develops, leading to complications like strictures, bleeding (occurring 3–4 weeks after ingestion), fistulas with adjacent trachea-bronchial tree or aorta and aspiration-related changes in lung.36 In the chronic phase, definitive treatment is mainly done by either endoscopic or surgical approaches. Endoscopic treatment involves staged dilatation for the oesophageal or gastric strictures and stent placement.24 Stents are also used for fistulas.47 Indications for surgery include failure of endoscopic treatment (refractory strictures), long-segment strictures (>10 cm) or presence of multiple strictures.27,48 Oesophageal reconstruction is done using stomach, colon and rarely jejunum.
Radiological interventions
Interventional radiologists play a major role in the management of corrosive injury in both stages. In the acute setting, the main role is in the drainage of inflammatory or perforation-related collections, pleural effusion and ascites under image guidance (Figure 10).
Figure 10.

Drainage. (a) An 18-year-old male with history of acid ingestion. Axial CT image shows an abdominal collection with air-fluid level due to gastric perforation and placement of pigtail catheter. (b) A 30-year-old female with acute corrosive intake and respiratory distress. Frontal chest radiograph shows left pleural collection with pigtail catheter in situ. (c,d) An 18-year-old female with history of corrosive injury 18 months back and surgical feeding jejunostomy presenting with abdominal distension and pain. Axial CT image (c) shows a large gastric mucocele (asterisk) due to pyloric stricture (arrow), which was drained under ultrasound guidance (d) by catheter.
In the chronic stage, the interventional radiologist has more roles to play. These include:
Balloon dilatation or stenting of the oesophageal strictures under fluoroscopy.
Drainage of mucoceles and post-operative collections under image guidance.
Endovascular embolization of vascular complications like pseudoaneurysm or active contrast leak.
Percutaneous feeding jejunostomy.
Image-guided biopsy for malignancy developing in the surgically isolated oesophagus, where endoscopic approach is not possible.
Fluoroscopic balloon dilatation or stenting of strictures: This is usually performed either as a primary procedure or in cases where endoscopy is contraindicated or difficult. Dilatation is performed in a staged manner, using smaller balloons initially followed by larger ones to avoid perforation (Figure 11).49 An oesophageal lumen diameter of 14–15 mm is usually adequate. The dilatation sessions are repeated at 3–4 week intervals as necessary. The recurrence rate of strictures after balloon dilatation is 30–40%, and 10% of the strictures are refractory.50 Stent placement across the oesophageal stricture can also be performed under fluoroscopic guidance.49 However, these indwelling stents are associated with complications like fistula formation, ulceration and tissue hyperplasia.51 Biodegradable stents have fewer complications, and do not need to be retrieved, but are more expensive.51 Covered stents also help in the treatment of long-standing fistulas and leaks.
Figure 11.
Balloon dilatation. A 5-year-old male with history of accidental corrosive intake 4 months back and oesophageal stricture. Fluoroscopic spot shows balloon dilatation of the short-segment oesophageal stricture. Waist is noted at the stricture site (arrow).
Drainage of mucoceles: Mucoceles are seen in the chronic phase and occur after surgical isolation of the oesophagus and stomach.41 Mucoceles become symptomatic when large, presenting with chest pain, respiratory distress, fever and regurgitation of mucoid content. Drainage can be done as a temporary procedure either under fluoroscopic guidance when there is a stricture in the proximal opening of the oesophagus (due to incomplete surgical isolation) or under ultrasound (Figure 10) or CT guidance, when it is completely isolated.
To prevent recurrence, a definitive surgery, either removal of the distended segment or surgical decompression into jejunal loop is required.41 Alternatively, sclerotherapy can be performed successfully under fluoroscopic guidance.43 In this technique, a sclerosant, usually absolute alcohol, is instilled into the mucocele through the same catheter used for drainage. The solution is reaspirated after 15–30 min and the catheter is clamped. The procedure is repeated 2–3 times at an interval of 3–4 weeks for successful destruction of the mucosa and obliteration of the lumen (Figure 12).
Figure 12.

Ablation of mucocele. A 23-year-old female with pre-existing chest wall deformity and retrosternal gastric pull-up for accidental acid ingestion 1-year back, presenting with chest pain and dyspnoea due to mucocele. (a) Fluoroscopic spot image shows the filling of the mucocele with absolute alcohol mixed with iodinated contrast agent (arrow) through a drainage catheter. The procedure was repeated after 1 month. (b) Initial axial CT image shows the oesophageal mucocele (arrow). (c) Follow-up axial balanced turbo field echo MR image after 4 months shows near complete ablation of the oesophagus (arrow).
Endovascular embolization for vascular complications: Bleeding is a rare complication presenting in the 3rd–4th week.35 Endoscopic treatment is possible for superficial bleeders. Endovascular embolization is an effective treatment option with high success rates in patients with delayed bleeding after corrosive injury and especially in those who demonstrate a single site of bleed on endoscopy or CT angiography (Figure 6).52 In cases where endoscopy or embolization fails, surgery is required.52
Percutaneous feeding jejunostomy: Most of the patients with severe corrosive injury are treated with a surgical feeding jejunostomy for maintaining nutrition.53 However, surgical feeding jejunostomy is associated with much higher complication rates and has other disadvantages such as need for general anaesthesia, post-operative ileus and wound infection.54 Therefore, placement of a feeding jejunostomy catheter under image guidance is helpful.54 Under ultrasound guidance, a jejunal loop is identified in the left upper quadrant and punctured. After confirming the jejunal loop by injecting small amount of iodinated contrast medium, two T-anchor sutures are placed (Figure 13). Then, a guidewire is advanced into the jejunum under fluoroscopic guidance, followed by serial dilatation of the tract and 12 – 14F catheter placement.
Figure 13.

Percutaneous feeding jejunostomy. A 34-year-old female, with corrosive oesophageal stricture and failed endoscopic dilatation. (a–c): Fluoroscopic spot images show the steps of percutaneous feeding jejunostomy tube placement. (a) Anchor sutures to fix the jejunum followed by guidewire placement into the jejunum (arrow). (b) serial dilatation of the tract (arrow). (c) final position of 14F foley’s catheter (arrow).
Image-guided biopsy: In patients of corrosive injury who develop malignancy in the surgically isolated oesophagus, sampling through endoscopic approach is not possible. Hence, biopsy under CT guidance is the technique of choice and can be performed safely (Figure 9B).
Conclusion
Corrosive injuries of the upper GIT are rare but incapacitating. The disease can be devastating in both the acute and chronic forms and is potentially lethal. Their chronic sequelae increase morbidity and considerably influence the quality of life. Oral contrast study and CT scan are the investigations of choice and play a major role in the disease evaluation, in both acute and chronic stages. Management requires a multidisciplinary team approach with the radiologist playing an important role in grading the injury in the acute phase, assessing disease extent in the late phase and in performing radiological interventions in both phases.
Contributor Information
Ayushi Agarwal, Email: ayushi.193@gmail.com.
Deep Narayan Srivastava, Email: drdeepsrivastava@rediffmail.com.
Kumble Seetharama Madhusudhan, Email: drmadhuks@gmail.com.
REFERENCES
- 1.Ertekin C, Alimoglu O, Akyildiz H, Guloglu R, Taviloglu K. The results of caustic ingestions. Hepatogastroenterology 2004; 51: 1397–400. [PubMed] [Google Scholar]
- 2.Kamat R, Gupta P, Reddy YR, Kochhar S, Nagi B, Kochhar R. Corrosive injuries of the upper gastrointestinal tract: a pictorial review of the imaging features. Indian J Radiol Imaging 2019; 29: 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Keh SM, Onyekwelu N, McManus K, McGuigan J. Corrosive injury to upper gastrointestinal tract: still a major surgical dilemma. World J Gastroenterol 2006; 12: 5223–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chibishev A, Pereska Z, Chibisheva V, Simonovska N. Corrosive poisonings in adults. Mater Sociomed 2012; 24: 125–30. doi: 10.5455/msm.2012.24.125-130 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chirica M, Bonavina L, Kelly MD, Sarfati E, Cattan P. Caustic ingestion. The Lancet 2017; 389: 2041–52. doi: 10.1016/S0140-6736(16)30313-0 [DOI] [PubMed] [Google Scholar]
- 6.Lakshmi CP, Vijayahari R, Kate V. Ananthakrishnan N. a hospital-based epidemiological study of corrosive alimentary injuries with particular reference to the Indian experience. Natl Med J India 2013; 26: 6. [PubMed] [Google Scholar]
- 7.Swain R, Behera C, Gupta SK. Fatal corrosive ingestion: a study from South and south-east Delhi, India (2005–2014. Med Sci Law 2016; 56: 252–7. doi: 10.1177/0025802416657762 [DOI] [PubMed] [Google Scholar]
- 8.Lusong MAAD, Timbol ABG, Tuazon DJS. Management of esophageal caustic injury. World J Gastrointest Pharmacol Ther 2017; 8: 90–8. doi: 10.4292/wjgpt.v8.i2.90 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ciftci AO, Şenocak ME, Büyükpamukç N, Hiçsönmez A. Gastric outlet obstruction due to corrosive ingestion: incidence and outcome. Pediatr Surg Int 1999; 15: 88–91. doi: 10.1007/s003830050523 [DOI] [PubMed] [Google Scholar]
- 10.Kluger Y, Ishay OB, Sartelli M, Katz A, Ansaloni L, Gomez CA, et al. Caustic ingestion management: world Society of emergency surgery preliminary survey of expert opinion. World J Emerg Surg 2015; 10: 48. doi: 10.1186/s13017-015-0043-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Contini S, Scarpignato C. Caustic injury of the upper gastrointestinal tract: a comprehensive review. WJG 2013; 19: 3918–30. doi: 10.3748/wjg.v19.i25.3918 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lahoti D, Broor SL. Corrosive injury to the upper gastrointestinal tract. Indian J Gastroenterol 1993; 12: 135–41. [PubMed] [Google Scholar]
- 13.Søreide J, Viste A. Esophageal perforation: diagnostic work-up and clinical decision-making in the first 24 hours. Scand J Trauma Resusc Emerg Med 2011; 19: 66. doi: 10.1186/1757-7241-19-66 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gumaste VV, Dave PB. Ingestion of corrosive substances by adults. Am J Gastroenterol 1992; 87: 1–5. [PubMed] [Google Scholar]
- 15.Zangi M, Saghebi SR, Biharas Monfared A, Lajevardi S, Shadmehr MB. Colopharyngoplasty in patients with severe pharyngoesophageal corrosive injury: a complicated but worthwhile procedure to restore Gi tract continuity, a case series. Tanaffos 2017; 16: 68–75. [PMC free article] [PubMed] [Google Scholar]
- 16.Csíkos M, Horváth OP, Petri A, Petri I. Late malignant transformation of chronic corrosive oesophageal strictures. Magy Seb 2005; 58: 357–62. [PubMed] [Google Scholar]
- 17.Elkaramany M. An overview of corrosive injury of the upper gastrointestinal tract: discussion of types, clinical evaluation, and management procedures. Adv Dig Med 2018; 5: 115–20. doi: 10.1002/aid2.13091 [DOI] [Google Scholar]
- 18. Caustic ingestions workup: laboratory studies, imaging studies. Procedures. Accessed April 9, 2020. [Google Scholar]
- 19.Jain M, Waghmare C, Adkar S, Sircar S, Jain AK. Button battery ingestion in children: an emerging hazard. Journal of Digestive Endoscopy 2013; 04: 071–4. doi: 10.4103/0976-5042.129969 [DOI] [Google Scholar]
- 20.Gastrointestinal (GI) contrast media in adults: indications and guidelines ACR manual on contrast media 2020. ACR Committee on drugs and contrast media. ACR Committee on Drugs and Contrast Media 2020;: 57–73. [Google Scholar]
- 21.Muhletaler CA, Gerlock AJ, de Soto L, Halter SA. Acid corrosive esophagitis: radiographic findings. American Journal of Roentgenology 1980; 134: 1137–40. doi: 10.2214/ajr.134.6.1137 [DOI] [PubMed] [Google Scholar]
- 22.Zargar SA, Kochhar R, Nagi B, Mehta S, Mehta SK. Ingestion of strong corrosive alkalis: spectrum of injury to upper gastrointestinal tract and natural history. Am J Gastroenterol 1992; 87: 337–41. [PubMed] [Google Scholar]
- 23.Kikendall JW. Caustic ingestion injuries. Gastroenterol Clin North Am 1991; 20: 847–57. [PubMed] [Google Scholar]
- 24.Methasate A, Lohsiriwat V. Role of endoscopy in caustic injury of the esophagus. World J Gastrointest Endosc 2018; 10: 274–82. doi: 10.4253/wjge.v10.i10.274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ali Zargar S, Kochhar R, Mehta S, Kumar Mehta S, Zargar SA, Mehta SK. The role of fiberoptic endoscopy in the management of corrosive ingestion and modified endoscopic classification of burns. Gastrointest Endosc 1991; 37: 165–9. doi: 10.1016/S0016-5107(91)70678-0 [DOI] [PubMed] [Google Scholar]
- 26.Chirica M, Resche-Rigon M, Pariente B, Fieux F, Sabatier F, Loiseaux F, et al. Computed tomography evaluation of high-grade esophageal necrosis after corrosive ingestion to avoid unnecessary esophagectomy. Surg Endosc 2015; 29: 1452–61. doi: 10.1007/s00464-014-3823-0 [DOI] [PubMed] [Google Scholar]
- 27.Kochman ML, McClave SA, Boyce HW. The refractory and the recurrent esophageal stricture: a definition. Gastrointest Endosc 2005; 62: 474–5. doi: 10.1016/j.gie.2005.04.050 [DOI] [PubMed] [Google Scholar]
- 28.Ryu HH, Jeung KW, Lee BK, Uhm JH, Park YH, Shin MH, et al. Caustic injury: can CT grading system enable prediction of esophageal stricture? Clin Toxicol 2010; 48: 137–42. doi: 10.3109/15563650903585929 [DOI] [PubMed] [Google Scholar]
- 29.Ananthakrishnan N, Parthasarathy G, Kate V. Acute corrosive injuries of the stomach: a single unit experience of thirty years. ISRN Gastroenterol 2011; 2011: 1: 914013–52011. doi: 10.5402/2011/914013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lurie Y, Slotky M, Fischer D, Shreter R, Bentur Y. The role of chest and abdominal computed tomography in assessing the severity of acute corrosive ingestion. Clin Toxicol 2013; 51: 834–7. doi: 10.3109/15563650.2013.837171 [DOI] [PubMed] [Google Scholar]
- 31.Chirica M, Resche-Rigon M, Zagdanski AM, Bruzzi M, Bouda D, Roland E, et al. Computed tomography evaluation of esophagogastric necrosis after caustic ingestion. Ann Surg 2016; 264: 107–13. doi: 10.1097/SLA.0000000000001459 [DOI] [PubMed] [Google Scholar]
- 32.Hopkins RA, Postlethwait RW. Caustic burns and carcinoma of the esophagus. Ann Surg 1981; 194: 146–8. doi: 10.1097/00000658-198108000-00005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Manickam Neethirajan S, S M C, Velayoudam V, Aridhasan Meenakshi L, Harikrishnan S. Giant mucocele of the remnant esophagus: case report of a rare complication following a bipolar esophageal exclusion procedure. Cureus 2019; 11: e6317: e6317. doi: 10.7759/cureus.6317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nagi B, Kochhar R, Thapa BR, Singh K. Radiological spectrum of late sequelae of corrosive injury to upper gastrointestinal tract. A pictorial review. Acta radiol 2004; 45: 7–12. doi: 10.1080/02841850410003329 [DOI] [PubMed] [Google Scholar]
- 35.Tseng Y-L, Wu M-H, Lin M-Y, Lai W-W. Massive upper gastrointestinal bleeding after acid-corrosive injury. World J Surg 2004; 28: 50–4. doi: 10.1007/s00268-003-6831-0 [DOI] [PubMed] [Google Scholar]
- 36.Tseng Y, WU M, LIN M, LAI W. Outcome of acid ingestion related aspiration pneumonia. European Journal of Cardio-Thoracic Surgery 2002; 21: 638–43. doi: 10.1016/S1010-7940(02)00045-3 [DOI] [PubMed] [Google Scholar]
- 37.Chibishev A, Simonovska N, Bozinovska C, Pereska Z, Smokovski I, Glasnovic M. Respiratory complications from acute corrosive poisonings in adults. Mater Sociomed 2014; 26: 80–3. doi: 10.5455/msm.2014.26.80-83 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Manoharan D, Srivastava DN, Madhusudhan KS. Spontaneous rupture of an esophageal mucocele into the airway. ACG Case Reports Journal 2019; 6: e00285: e00285. doi: 10.14309/crj.0000000000000285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Estrera A, Taylor W, Mills LJ, Platt MR. Corrosive burns of the esophagus and stomach: a recommendation for an aggressive surgical approach. Ann Thorac Surg 1986; 41: 276–83. doi: 10.1016/S0003-4975(10)62769-5 [DOI] [PubMed] [Google Scholar]
- 40.Gupta NM, Gupta R. Transhiatal esophageal resection for corrosive injury. Ann Surg 2004; 239: 359–63. doi: 10.1097/01.sla.0000114218.48318.68 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rathinam D, Madhusudhan KS, Srivastava DN, Dash NR, Gupta AK. Esophageal mucocele after surgical isolation of thoracic esophagus presenting with respiratory distress. Trop Gastroenterol 2017; 37: 147–8. [PubMed] [Google Scholar]
- 42.Kamath MV, Ellison RG, Rubin JW, Moore HV, Pai GP. Esophageal mucocele: a complication of blind loop esophagus. Ann Thorac Surg 1987; 43: 263–9. doi: 10.1016/S0003-4975(10)60609-1 [DOI] [PubMed] [Google Scholar]
- 43.Nachira D, Chiappetta M, Congedo MT, Petracca-Ciavarella L, Mastromarino MG, Di Stasi C, et al. Successful three-stage ethanol ablation of esophageal mucocele. Journal of Vascular and Interventional Radiology 2016; 27: 152–4. doi: 10.1016/j.jvir.2015.08.010 [DOI] [PubMed] [Google Scholar]
- 44.Eaton H, Tennekoon GE. Squamous carcinoma of the stomach following corrosive acid burns. Br. J. Surg. 1972; 59: 382–7. doi: 10.1002/bjs.1800590514 [DOI] [PubMed] [Google Scholar]
- 45.Ramasamy K, Gumaste VV. Corrosive ingestion in adults. J Clin Gastroenterol 2003; 37: 119–24. doi: 10.1097/00004836-200308000-00005 [DOI] [PubMed] [Google Scholar]
- 46.Chibishev A, Pereska Z, Simonovska N, Chibisheva V, Glasnovic M, Chitkushev LT. Conservative therapeutic approach to corrosive poisonings in adults. J Gastrointest Surg 2013; 17: 1044–9. doi: 10.1007/s11605-013-2190-9 [DOI] [PubMed] [Google Scholar]
- 47.Blackmon SH, Santora R, Schwarz P, Barroso A, Dunkin BJ. Utility of removable esophageal covered self-expanding metal stents for leak and fistula management. Ann Thorac Surg 2010; 89: 931–7. doi: 10.1016/j.athoracsur.2009.10.061 [DOI] [PubMed] [Google Scholar]
- 48.Chirica M, Veyrie N, Munoz-Bongrand N, et al. Late morbidity after colon interposition for corrosive esophageal injury: risk factors, management, and outcome. A 20-years experience. Ann Surg 2010; 252: 271–80. [DOI] [PubMed] [Google Scholar]
- 49.Therasse E, Oliva VL, Lafontaine E, Perreault P, Giroux M-F, Soulez G. Balloon dilation and stent placement for esophageal lesions: indications, methods, and results. RadioGraphics 2003; 23: 89–105. doi: 10.1148/rg.231025051 [DOI] [PubMed] [Google Scholar]
- 50.Ham YH, Kim GH. Plastic and biodegradable stents for complex and refractory benign esophageal strictures. Clin Endosc 2014; 47: 295–300. doi: 10.5946/ce.2014.47.4.295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hindy P, Hong J, Lam-Tsai Y. Gress f. a comprehensive review of esophageal stents. Gastroenterol Hepatol 2012; 8: 526–34. [PMC free article] [PubMed] [Google Scholar]
- 52.Singh AN, Kilambi R, Madhusudhan KS, Pal S. An alternative approach to life-threatening gastrointestinal bleeding after corrosive ingestion. Indian J Surg 2018; 80: 187–9. doi: 10.1007/s12262-018-1739-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Katzka DA. Caustic injury to the esophagus. Curr Treat Options Gastroenterol 2001; 4: 59–66. doi: 10.1007/s11938-001-0047-x [DOI] [PubMed] [Google Scholar]
- 54.van OH, Schipper J. Percutaneous jejunostomy. Semin Interv Radiol 2004; 21: 199–204. [DOI] [PMC free article] [PubMed] [Google Scholar]