

Abstract
The alcohol treatment literature has established in-session client speech as a mechanism of change that therapist behavior can influence and that can be predictive of drinking outcomes. This study aimed to explore temporal patterns of in-session speech in alcohol behavioral couple therapy (ABCT), including the unique interplay between client and partner speech and the role of speech trajectories in predicting client drinking outcomes. Participants were 165 heterosexual couples receiving ABCT in one of four clinical trials. We coded client speech on an utterance-by-utterance basis using the system for coding couples’ interactions in therapy–alcohol. We focused on individual-level speech codes of change talk and sustain talk and couple-level variables of positive and negative interactions. We segmented the initial and midtreatment sessions into quartiles to conduct path analyses and latent growth curve models. Path analyses suggested that clients and partners may not have been aligned in terms of treatment goals at the start of the therapy. This misalignment within couples was pronounced during the initial session and decreased by the midtreatment session, reflecting progression toward treatment goals. Of the latent growth curve models, only client sustain talk during the midtreatment session predicted greater client drinking at the end of treatment. Results provide insight into the inner workings of ABCT and suggest recommendations for ABCT therapists. This study also supports a growing consensus that sustain talk may be a stronger mechanism of change than change talk in various alcohol treatment interventions.
Keywords: Alcohol use disorder, Couples, Treatment, Change talk, Mechanisms
1. Introduction
1.1. Alcohol behavioral couple therapy
Alcohol use disorder (AUD) and relationship functioning are reciprocally associated— AUD frequently causes relationship distress (with associated increases in communication problems, intimate partner violence, separation, and divorce), which, in turn, exacerbates drinking (Klostermann, Kelley, Mignone, Pusateri, & Wills, 2011; McCrady, 2012). Further, partners of individuals with AUD have unique treatment needs, as they often struggle to cope and are at risk of developing their own psychopathology (McCrady, 2012). Even if relationship distress is absent, it is beneficial for couples to collaborate in AUD treatment to modify relationship dynamics and shared environmental factors that may inadvertently reinforce drinking (McCrady, 2012; McCrady, Wilson, et al., 2016). Trials of couple-based AUD treatment approaches, such as alcohol behavioral couple therapy (ABCT; McCrady & Epstein, 2009), have shown that such approached lead to equal or greater rates of abstinence and superior relationship functioning when compared to individual-based interventions for AUD (Klostermann et al., 2011; McCrady, Wilson, et al., 2016; Powers, Vedel, & Emmelkamp, 2008). ABCT (McCrady & Epstein, 2009) meets the criteria for a “well-established” treatment, the highest level of empirical support that the American Psychological Association recognizes.
The four key active ingredients in ABCT are cognitive behavioral interventions focused on changing drinking, cognitive behavioral interventions to improve partner behaviors related to drinking, relationship enhancement interventions, and therapist use of common therapeutic factors. In combination, these active ingredients are expected to enhance patient and partner motivation, increase patient and partner coping skills related to drinking, and improve the couple’s relationship to enhance mutual motivation to maintain changes in drinking. Treatment interventions to enhance the couple’s relationship focus on increasing positive shared activities that do not involve drinking, reducing conflict about alcohol, enhancing partner support around changes in drinking, and both increasing positive and decreasing negative communication. A central premise of the treatment is that couple communication may facilitate or impede therapeutic change; the therapist closely monitors in-session exchanges of positive (e.g., displays of affection) and negative (e.g., criticism) behaviors between partners to help the couple learn more effective ways to communicate.
McCrady and colleagues (2019) recently analyzed the mechanisms of behavior change (MOBCs) across four clinical trials of ABCT using coded session recordings. They found that during treatment, couples increased positive behaviors, talked less about drinking, and decreased their amount of motivational speech. Surprisingly, therapist behaviors did not predict client or partner behaviors during treatment or client drinking outcomes. The authors used hierarchical regression to test the association between client or partner behaviors and drinking outcomes. For all analyses, they entered covariates in the first block, and they entered the independent variables of interest (i.e., therapist behaviors, patient behaviors, or partner behaviors) in the second block. Client codes entered as a block included global ratings of general support, collaboration, and contemptuousness, along with the specific behavior codes of giving advice, confrontation, change talk, and sustain talk. Partner codes entered as a block included global ratings of alcohol-specific support, general support, collaboration, and contemptuousness, along with the specific behavior codes of giving advice, confrontation, and change talk. In the first session, partner advice predicted poorer drinking outcomes. At the mid-treatment session, client behaviors, as a block, and the specific behaviors of contemptuousness toward the partner and sustain talk, predicted poorer drinking outcomes. The authors suggested that future analyses should focus in greater detail on specific aspects of client and partner speech, including proximal relationships between client and partner speech within a session of ABCT.
1.2. Positive and negative couple interactions
The current study focuses on specific aspects of the couple’s relationship that the broader behavioral couple therapy literature has suggested are important. The literature conceptualizes couple distress as multiply determined (Epstein & Baucom, 2003). One key factor contributing to distress is positive versus negative behaviors, including low levels of positive interaction, high levels of negative interaction, and reciprocity of negative exchanges in which the negative behaviors of one partner elicit negative responses from the other. Contemporary models also focus on how partners perceive and interpret each other’s behavior, individual- and couple-level affect and affect regulation, and contextual factors that impact a couple such as economic, occupational, and health resources. Treatment focuses on helping the couple view their difficulties in relational terms (Davis, Lebow, & Sprenkel, 2012), increase positive reciprocity, decrease negative reciprocity, change dysfunctional patterns of interaction, and improve communication skills (Benson, McGinn, & Christensen, 2012). Research on MOBCs in couple therapy suggests the importance of increasing positive behaviors and decreasing negative behaviors, particularly in the first half of couple therapy (Doss, Thum, Sevier, Atkins, & Christensen, 2005). ABCT draws upon this broader couple therapy literature both conceptually and in terms of specific interventions to enhance the couple’s relationship.
1.3. Change talk and sustain talk
Among the most widely studied MOBCs in AUD treatment are client change talk and sustain talk, originally defined in motivational interviewing (MI; Miller & Rollnick, 2013). Change talk encompasses preparatory speech (expressing desire, ability, reasons, or need to change) and mobilizing speech (expressing commitment, activation, and taking steps to change). Sustain talk (or counter-change talk) includes speech expressing hesitation, doubt, or resistance to change and support for the status quo. Client change talk and sustain talk appear to be malleable to the therapist’s influence. Therapist behaviors that are MI-consistent (MICO) and conducive to change talk include affirming client strengths and autonomy, seeking permission before giving advice, and differentially reflecting change talk in proportion to sustain talk. Conversely, therapist behaviors that are MI-inconsistent (MIIN) and conducive to sustain talk include warning about consequences, directly disagreeing with the client, and raising concerns without permission of the client. Temporal analyses have highlighted the dynamic nature of in-session exchanges (e.g., Amrhein, Miller, Yahne, Palmer, & Fulcher, 2003; Houck et al., 2015). For example, Moyers et al. (2007) found that client change talk was significantly more likely to immediately follow therapist MICO behaviors, which in turn were more likely to immediately follow client change talk. Likewise, client sustain talk was significantly more likely to follow therapist MIIN behaviors and less likely to follow MICO behaviors.
MI experts believe that therapist MICO behaviors subtly encourage ambivalent clients to “talk themselves into change,” with evidence suggesting that clients undergo neurocognitive shifts (perhaps to resolve cognitive dissonance) in response to vocalizing change talk in session (Feldstein Ewing, Filbey, Sabbineni, Chandler, & Hutchison, 2011; Houck, Moyers, & Tesche, 2013). Change talk, in turn, appears to predict AUD outcomes above and beyond the influence of self-reported motivation or readiness to change (Apodaca & Longabaugh, 2009; Moyers et al., 2007; Moyers, Martin, Houck, Christopher, & Tonigan, 2009). Recent meta-analyses have largely supported the hypothesized active ingredients and MOBCs in MI including change talk and sustain talk; however, they have raised questions about the predictive value of change talk as a standalone construct, finding that sustain talk and the ratio of change talk to sustain talk are better predictors of outcomes (Magill et al., 2014; Magill et al., 2018).
Researchers also have found evidence that change talk and sustain talk are MOBCs in non-MI interventions such as cognitive behavioral therapy for AUD or generalized anxiety (Lombardi, Button, & Westra, 2014; Moyers et al., 2007; Sijercic, Button, Westra, & Hara, 2016). However, the vast majority of research on in-session client speech has come from individual-based interventions. It remains unclear if partner speech functions similarly to therapist speech in couple-based AUD interventions such as ABCT. It is reasonable to expect that partners could facilitate change talk by offering encouragement or solutions and, conversely, promote sustain talk by expressing skepticism or blame, disagreeing with the client, or focusing on negative consequences of drinking. Studies that have examined the impact of significant others (SOs) on client speech relied on therapy sessions in which a family member, partner, or friend functioned as an occasional adjunct to individual AUD treatment and a general source of feedback and support (Apodaca, Magill, Longabaugh, Jackson, & Monti, 2013; Bourke, Magill, & Apodaca, 2016; Manuel, Houck, & Moyers, 2012).
Manuel and colleagues (2012) found several significant correlations among SO behaviors, client change talk, and drinking outcomes, but they were limited by a small sample size of a subset of sessions from Project MATCH. Notably, when SOs offered more encouragement and advice, and spoke less about themselves, clients were more likely to vocalize change talk. Greater SO sustain talk, on the other hand, predicted more client drinks per drinking day 4–9 months later. Using another subset of Project MATCH sessions, Bourke and colleagues (2016) replicated Manuel et al.’s findings using lag-sequential analyses, which examine speech at the utterance-to-utterance level and determine the probability that a behavior of interest would occur given that another behavior of interest had occurred immediately prior (Auld & White, 1959). Also using lag-sequential analyses, Apodaca and colleagues (2013) found that SO encouragement, advice, and change talk positively predicted subsequent client change talk and negatively predicted client sustain talk; they did not examine drinking outcomes. Interestingly, therapist MICO and MIIN behaviors failed to significantly predict client speech, with therapist change talk accounting for just 3%, and SO change talk accounting for 27%, of the variance in client change talk (Apodaca et al., 2013).
1.4. The study
The purpose of the current study was to build on the findings of McCrady et al. (2019) and add to our understanding of MOBCs in ABCT by examining within-session trajectories of client and partner speech and the relationship of these trajectories to drinking outcomes. ABCT is grounded in the theory that couples are mutually interdependent, and that the behavior of each partner influences the other (McCrady & Epstein, 2009). ABCT is focused on improving the reciprocal association between AUD and romantic relationship dynamics (McCrady, 2012) rather than simply including a general SO (family member, friend, etc.) as an adjunct to individual therapy; thus, our study builds on the results of analyses of Project MATCH (Apodaca et al., 2013; Bourke et al., 2016; Manuel, et al., 2012) with a stronger dyadic focus. We focused on two different types of client and partner speech: change talk and sustain talk (Miller & Rollnick, 2013) as applied specifically to drinking, and positive and negative behaviors as indicators of overall relationship functioning (Doss et al., 2005). Although our aims were somewhat exploratory, we generally anticipated that the speech of each partner would influence the other as the session progressed, and that increases in desirable behavior over the course of the session (i.e., increases in change talk and positive behaviors, decreases in sustain talk and negative behaviors) would be related to better drinking outcomes. Thus, the study aims were to: (a) describe the pattern of within-session speech and interrelationships between client and partner speech over the course of the initial and mid-treatment sessions and (b) examine the trajectory of within-session speech as related to proximal and distal drinking outcomes. To our knowledge, this is the first study of a couple therapy intervention to examine within-session interactions on an utterance-by-utterance level, and the first study to explore temporal trajectories of change talk and sustain talk in relation to AUD outcomes within a couple-based intervention.
2. Material and methods
2.1. Participants
Participants were heterosexual couples from four similar randomized controlled trials of ABCT conducted in the northeastern United States between 1979 and 2009 (McCrady, Epstein, Cook, Jensen, & Hildebrandt, 2009; McCrady, Epstein, Hallgren, Cook, & Jensen, 2016; McCrady, Epstein, & Hirsch, 1999; McCrady et al., 1986). A total of 188 couples from the community engaged in ABCT, for which 169 and 115 audio recordings of the initial and midtreatment sessions, respectively, were available for analysis. Missing recordings were due to participant withdrawal by mid-treatment (n = 65), sessions not having been recorded (n = 60), inaudible or poor audio quality that prevented coding (n = 22), or other reasons (n = 5). Eligibility criteria across all the trials included DSM-III (APA, 1980) or DSM-IV (APA, 1994) diagnosis of AUD in one partner, alcohol use within the past 30–60 days, and willingness of both partners to engage in treatment. Exclusion criteria included diagnosis in either partner of drug dependence, psychotic disorder, or serious cognitive impairment. Half of the trials excluded couples that reported intimate partner violence and/or AUD among both individuals. Additional information about participant selection is available in the original citations and main outcomes paper (McCrady et al., 2019).
Of the final sample of 169 couples, more than half (57.4%) of the presenting clients/identified patients (IPs) were women (n = 97), and the average age of IPs was 44.6 (SD = 10.2) years. IPs on average drank on 66.7% of the 90 days preceding baseline and reported an average duration of AUD of 14.0 (SD = 10.2) years. Most (85.8%) couples were married, while 8.3% were cohabiting, 3.6% were committed but living apart, and 1.2% were separated. Partners of clients/significant others (SOs) averaged 45.0 (SD = 11.3) years old. The sample was predominantly white (91.1% of IPs and 79.3% of SOs), with 4.1% of IPs and 3.6% of SOs identifying as Black; 1.8% of IPs and 3.0% of SOs identifying as American Indian/Alaska Native; and less than 1.0% of the sample identifying as Hispanic/Latino or Asian. IPs and SOs reported an average of 14.3 (SD = 2.8) and 14.6 (SD = 2.4) years of education, respectively.
2.2. Measures
2.2.1. Alcohol consumption.
We used the timeline follow-back (TLFB; Sobell & Sobell, 1992) interview to assess drinks per day over the 90 days preceding the last drinking day before the baseline interview, and the 12 months following treatment. The TLFB has shown very good reliability and validity across cultures (Sobell et al., 2001). Corresponding self-monitoring cards recorded daily drinking during the treatment period, the focus of this investigation. IPs recorded each alcoholic beverage they consumed, including the quantity and percent alcohol. We reconstructed incomplete records with the therapist during the treatment session. If self-monitoring data were missing, we analyzed TLFB data collected post-treatment that covered the within-treatment window. We aggregated within-treatment drinking data as IP percent days abstinent (PDA) per week from session 1 until the end of treatment (week 26).
2.2.2. In-session interactions.
We used the system for coding couples’ interactions in therapy–alcohol (SCCIT-A; Owens, McCrady, Borders, Brovko, & Pearson, 2014) to classify in-session speech. Adapted from the motivational interviewing with significant others (MISO 3.0) coding system (Apodaca, Manuel, Moyers, & Amrhein, 2007), the SCCIT-A is an alternative to using two separate coding schemes for IPs and SOs. Owens and colleagues (2014) reported on the development and promising psychometric properties of the SCCIT-A. The entire coding manual is available to the public online.i The SCCIT-A includes 11 behavior codes for IPs and 11 behavior codes for SOs. We assigned behavior codes to each IP and SO utterance. We defined an utterance as a complete thought, beginning when a new idea was introduced in an existing or new sentence. See Owens et al. (2014) and McCrady et al. (2019) for a list of all codes including descriptive and reliability data.
The behavior codes that we analyzed in the current study were IP change talk (IP CT; e.g., “I’ll lose my job if I don’t stop drinking”), IP sustain talk (IP ST; e.g., “I’m more relaxed and easier to get along with after a few drinks”), and SO change talk (SO CT; e.g., “I think he can do it if he puts his mind to it”). We excluded SO sustain talk (SO ST) due to poor inter-rater reliability (Owens et al., 2014). Factor analytic work with the SCCIT-A has demonstrated that two independent latent variables capture a couple’s positive and negative behaviors (Owens et al., 2014). In this study, therefore, we computed IP and SO positive behavior counts (POS) by summing across categories of encourage/support-general (e.g., “She’s a really good person”), encourage/support-drinking (e.g., “I would go to AA with him if it would help”), and giving advice (e.g., “You could ask your friends not to bring alcohol over to our house”). We computed IP and SO negative behavior counts (NEG) by summing across the categories of direct (e.g., “You should respect yourself more”) and confront (e.g., “I can’t tell you how many times I’ve heard this line”). This approach can be conceptualized as means of examining the couple as a whole, complementing the individual-level speech variables.
2.3. Procedure
2.3.1. Treatment.
The Institutional Review Board where the research was conducted approved all studies. Participants completed up to 12–20 (depending on the study) 90-minute sessions of manual-guided ABCT. The treatment had three major aims: (a) to improve the IP’s ability to maintain abstinence through cognitive behavioral skills training, (b) to improve the SO’s ability to assist with and reinforce the IP’s abstinence through SO skills training, and (c) to attenuate relationship distress and enhance relationship satisfaction and communication (McCrady & Epstein, 2009). Therapists across trials (n = 32, 71% women) were master’s- or doctoral-level clinicians or advanced graduate students who received regular supervision.
We selected audio recordings from the initial treatment session (session 1) and midtreatment session (session 8 or 9 depending on the study; see McCrady et al., 2019 for a description of the selection of treatment sessions) for coding and analysis. In session 1, treatment manual instructions guided therapists to introduce the rationale for treating AUD within a couple therapy framework, encourage both partners to be actively involved in treatment, teach the couple to keep daily recordings of relationship satisfaction and IP drinking, and discuss homework. In session 8/9, manual instructions guided therapists to address the couple’s relationship satisfaction via reciprocity enhancement and to address drinking by teaching skills on assertiveness and/or drink refusal in social situations (McCrady & Epstein, 2009).
2.3.2. Coding.
Trained professionals transcribed all the sessions into Word files. Seven doctoral students in psychology coded the initial and midtreatment sessions. Staff trained coders for 5 months until the group reached fidelity, and they met weekly for the duration of the study to ensure ongoing inter-rater reliability. Coders listened to randomly assigned sessions and referred to the SCCIT-A (Owens et al., 2014) classification system. One coder parsed all transcribed IP and SO speech into discrete utterances that could be assigned a single SCCIT-A code. A second coder assigned behavior codes to each IP and SO utterance. We did not parse therapist speech and coded on an utterance-by-utterance level. More detailed information about the coding procedure is provided in Owens et al. (2014) and McCrady et al. (2019).
2.4. Data analysis plan
2.4.1. Path analyses.
As in prior work (Houck et al., 2015), we split coded data from session 1 and session 8/9 into segments, and we extracted summary scores (sums of IP CT, IP ST, SO CT, POS, and NEG) for each segment. We segmented both sessions into quartiles. To test the effects of within-subjects (or within-couples) speech, we conducted a series of cross-lagged panel analyses (i.e., path analyses) in Mplus (Muthén & Muthén, 2017), using each segment as a wave in the model. We selected this approach because it can provide estimates for the effects of IP speech on SO speech, the effects of SO speech on IP speech, the effects of IP and SO speech on couple-level (POS and NEG) behaviors, and vice versa. We conducted panel analyses using full maximum likelihood estimation. Within each session and quartile, we examined each variable of interest as a predictor three times (four times for SO CT); therefore, we used the Bonferroni correction to adjust for multiple comparisons, resulting in a conservative significance threshold of p ≤ .0166, and for SO CT, p ≤ .0125.
2.4.2. Latent growth curve models.
To test the effects of speech trajectories on drinking outcomes between subjects (or between couples), we entered the quartile data for session 1 and session 8/9 into latent growth curve models (LGCMs) predicting IP percent days abstinent (PDA). We fit PDA to a negative binomial distribution, appropriate for count variables with a high frequency of zeros. We tested PDA at mid-treatment as a dependent variable of speech from session 1, and at the end of treatment (26 weeks) as a dependent variable of speech from session 8/9. LGCMs estimated the trajectories of IP CT, IP ST, SO CT, POS, and NEG using full maximum likelihood estimation in Mplus (Muthén & Muthén, 2017), except in cases where we used maximum likelihood with standard errors approximated by first-order derivatives to achieve convergence. Based on the work of Amrhein and colleagues (2003), we centered each trajectory on the final quartile so that we could interpret the intercept term as the effects of late-session speech on PDA. All LGCMs controlled for IP sex (male/female), baseline PDA, and baseline days since the last reported drink.
3. Results
3.1. Descriptives
Figure 1 displays the mean frequency counts of IP CT, IP ST, SO CT, POS, and NEG per quartile in session 1 and session 8/9. As an initial step of the LGCMs predicting drinking outcomes (described below), we examined the linear slopes of each variable for significance. Across quartiles in session 1, two of the five variables had significant slopes: SO CT significantly decreased [B (SE) = −0.009 (0.002), β = −.985, p < .001] and POS significantly increased [B (SE) = 0.010 (0.003), β = .350, p = .005]. Across quartiles in session 8/9, three of the five variables had significant slopes: IP ST significantly decreased [B (SE) = 0.003 (0.001), β = −.380, p = .005], POS significantly increased [B (SE) = 0.009 (0.004), β = .520, p = .025], and NEG significantly increased [B (SE) = 0.008 (0.003), β = .274, p = .005].
Figure 1.
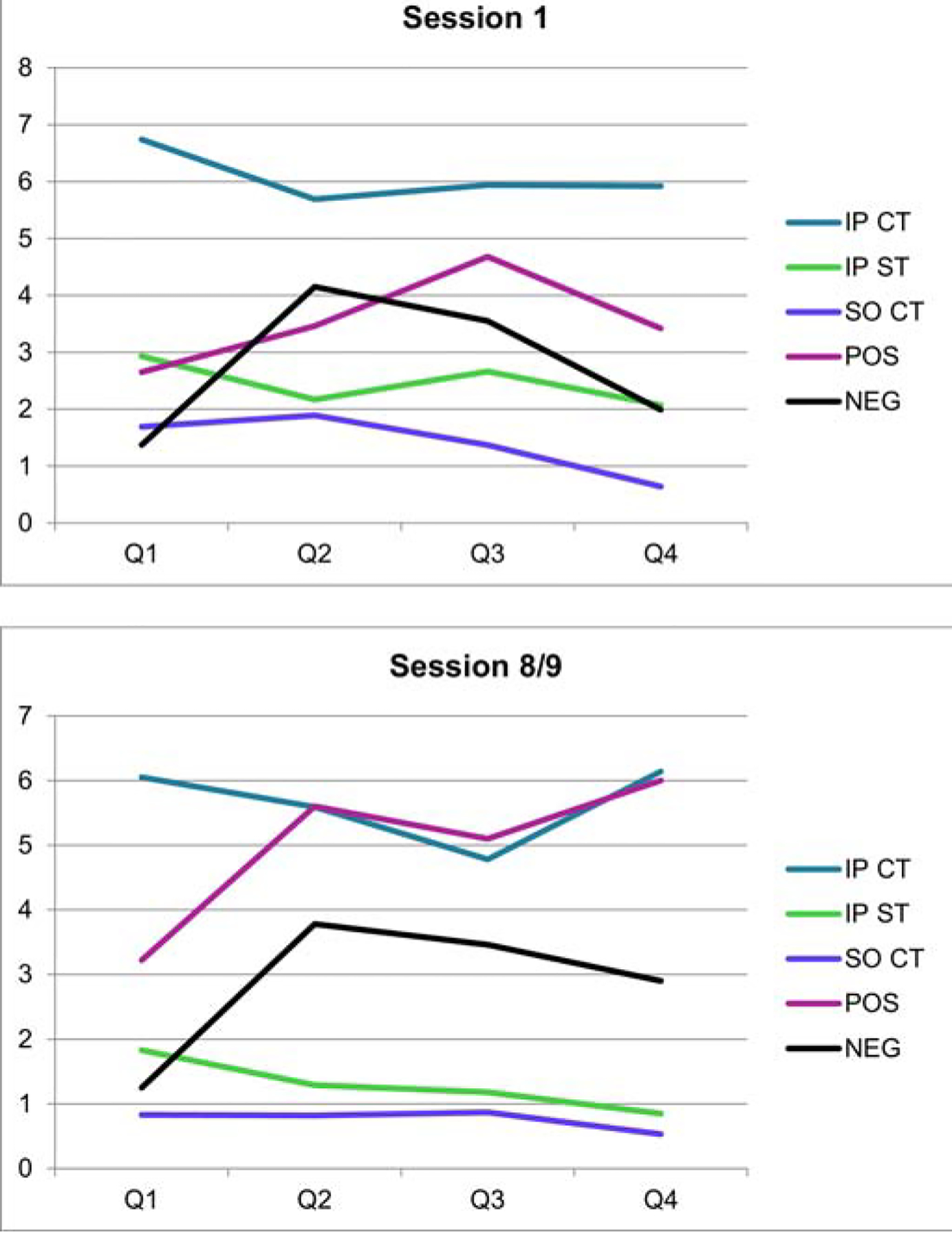
(Color). Mean utterances of speech variables by session quartile (Q). IP = identified patient, SO = significant other, CT = change talk, ST = sustain talk, POS = positive behaviors, NEG = negative behaviors.
3.2. Within couples
Figure 2 depicts results of the path analyses of within-couples speech patterns across quartiles in the initial and midtreatment sessions. We detected significant associations between IP ST and SO CT between quartiles (Qs) 2–3 and 3–4 in both sessions. In session 1, SO CT at Q2 positively predicted IP ST at Q3 [B (SE) = 0.139 (0.049), β = .221, p = .005], and IP ST at Q3 positively predicted SO CT at Q4 [B (SE) = 0.156 (0.059), β = .198, p = .008]. In session 8/9, SO CT at Q2 negatively predicted IP ST at Q3 [B (SE) = −0.287 (0.110), β = −0.214, p = .009], and SO CT at Q3 negatively predicted IP ST at Q4 [B (SE) = −0.205 (0.061), β = −0.229, p = .001]. The association between IP CT and SO CT was significant only at the beginning of the midtreatment session (Session 8/9), where SO CT in Q1 positively predicted IP CT in Q2 [B (SE) = 0.639 (0.178), β = .323, p < .001]. All significant associations remained significant after correction for multiple comparisons.
Figure 2.
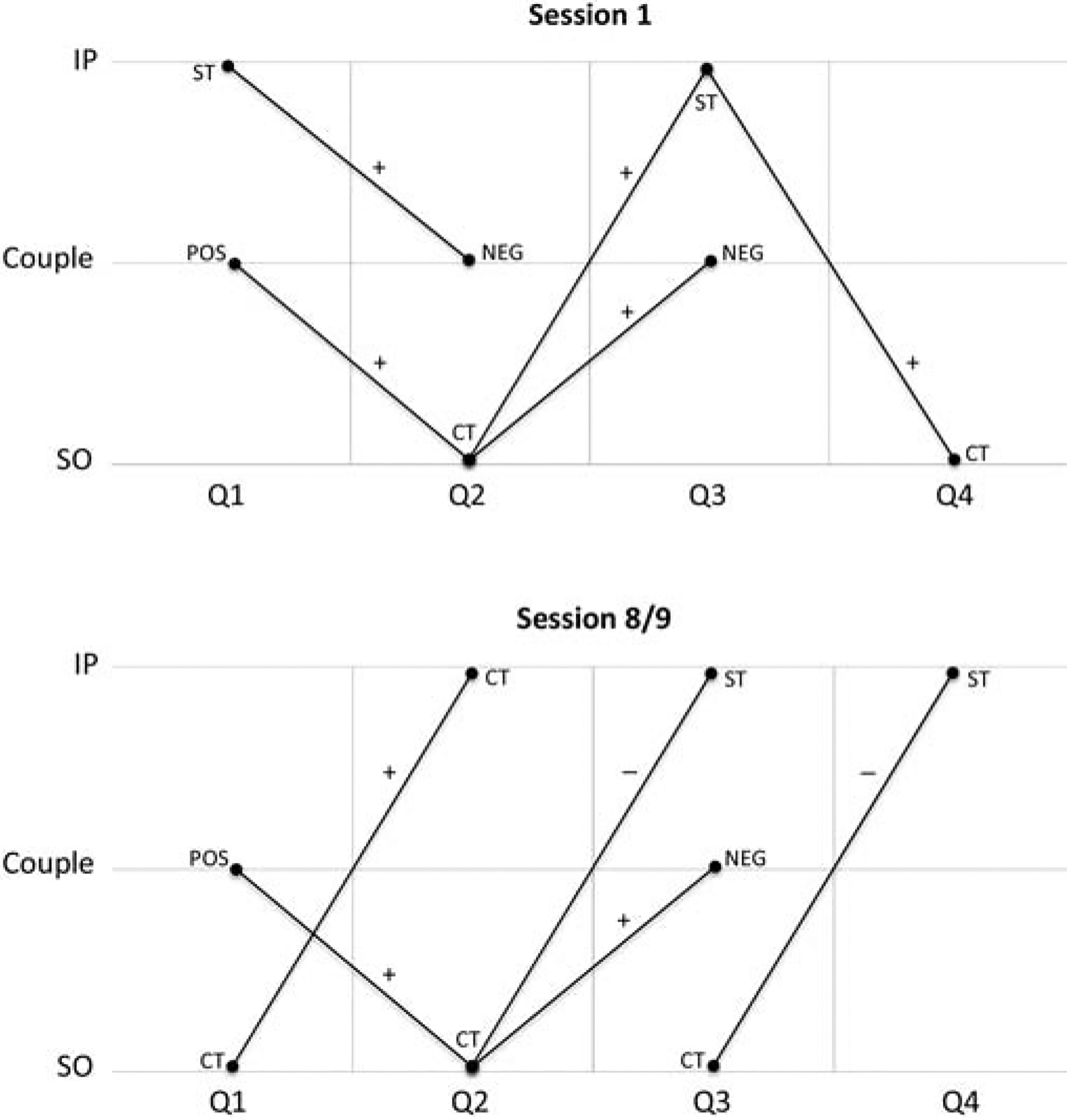
Within-couples speech patterns by session quartile (Q). Only significant or trending paths (p ≤ .05) are presented. Plus and minus signs denote a positive or negative association. IP = identified patient, SO = significant other, CT = change talk, ST = sustain talk, POS = positive behaviors, NEG = negative behaviors.
Additional path analyses revealed significant associations between IP and SO speech and couple-level (POS and NEG) behaviors between Qs 1–2 and 2–3 in both sessions. In session 1, IP ST at Q1 positively predicted NEG at Q2 [B (SE) = 0.538 (0.203), β = .152, p = .008], POS at Q1 positively predicted SO CT at Q2 [B (SE) = 0.140 (0.066), β = .160, p = .034], and SO CT at Q2 positively predicted NEG at Q3 [B (SE) = 0.562 (0.206), β = .204, p = .006]. In session 8/9, POS at Q1 positively predicted SO CT at Q2 trending toward significance [B(SE) = 0.042 (0.021), β = .176, p = .050], and SO CT at Q2 positively predicted NEG at Q3 [B(SE) = 0.884 (0.290), β = .219, p = .002]. No other within-couples path analyses in either session had statistically significant or trending results (p ≤ .05). With the exception of the association between POS at Q1 and SO CT at Q2, all significant associations remained significant after correction for multiple comparisons.
3.3. Between couples
Results of the LGCMs are presented in Table 1. There were no significant associations between speech variable trajectories in session 1 and mid-treatment PDA. Results of the LGCMs predicting end-of-treatment PDA from the speech trajectories of session 8/9 indicated that the trajectory of IP ST was significantly related to PDA. The negative slope of IP ST in session 8/9 predicted higher PDA at the end of treatment: B (SE) = 7.706 (3.857), β = .896, p = .046. None of the other LGCMs from session 8/9 had statistically significant findings.
Table 1.
(Updated) Latent Growth Curve Models Predicting Drinking from Speech Trajectories
| Speech Predictor Variable | Session 1 → Mid-Treatment IP Percent Days Abstinent (PDA) (n = 165) | Session 8/9 → End-of-Treatment IP Percent Days Abstinent (PDA) (n = 114) | ||||||
|---|---|---|---|---|---|---|---|---|
| B (SE) | β | p | B (SE) | β | p | |||
| Intercept | (2.139) | .205 | .601 | (1.234) | −.829 | .368 | ||
| Intercept | (0.615) | .060 | .990 | (0.766) | −.495 | .161 | ||
| Intercept | (2.690) | .231 | .570 | (0.364) | .005 | .997 | ||
| Intercept | (0.833) | .684 | .227 | (0.018) | −.278 | .788 | ||
| Intercept | (0.016) | −.252 | .825 | (0.486) | −.896 | .347 | ||
Note: Significant results (p < .05) are in bold.
Fixed path, probability undefined.
IP = identified patient, SO = significant other, CT = change talk, ST = sustain talk, POS = positive behaviors, NEG = negative behaviors. All models controlled for IP sex (male/female), baseline PDA, and baseline days since the last reported drink.
4. Discussion
The overall aims of the current study were to build on McCrady et al.’s (2019) study of MOBCs in ABCT by exploring patterns of speech within the couple therapy sessions. Specifically, we focused on the interrelationships between client and partner speech over the course of the initial and midtreatment sessions, and on relationships between the trajectory of within-session speech and proximal and distal drinking outcomes. We focused on one mechanism studied across different treatments for AUD, change/sustain talk (Miller & Rollnick, 2013), and one mechanism studied in the general behavioral couple therapy literature, positive/negative interactions (e.g., Doss et al., 2005). The findings, although not consistent across analyses, suggested a few patterns that help to clarify what happens in ABCT treatment sessions, and highlight changes in the sessions as treatment progresses.
The interplay between IP and SO CT and ST, and the changes in this interplay from the first session to midtreatment, is notable. In both sessions, it appears that SO use of CT has a powerful influence on the IP, as reflected in previous studies of select conjoint treatment sessions from Project MATCH (Apodaca et al., 2013; Bourke et al., 2016; Manuel et al., 2012). However, our study shows that the nature of that influence changes over the course of treatment. In session 1, the IP and SO may be less aligned in their goals around the IP’s drinking. Specifically, over the course of the session, higher levels of SO CT predicted more IP ST, which then elicited more SO CT. This pattern may depict an SO trying hard to convince their partner of the value of changing, and the IP reacting negatively to being “pushed” by their partner. This pattern changed significantly by the middle of treatment (session 8/9). By this time, when the SO expressed CT, the IP responded with more CT and less ST, suggesting a greater alignment of their goals around the IP’s drinking and perhaps a greater openness on the IP’s part to input from the SO. This shift may reflect the cumulative effects of the ABCT treatment in promoting a stronger dyadic alliance (McCrady, 2012).
Overall, positive couple interactions increased over the course of both sessions, although negative interactions also increased during the mid-treatment session. The increase in positive interactions is consistent with a couple therapy model, in which the therapist typically is coaching the couple and helping them to use more constructive communication skills during the treatment session. The increase in negative behaviors at the beginning of the midtreatment session is more puzzling, but may reflect the couple’s increasing comfort with discussing conflictual issues in the therapy session. Given that in the midtreatment session SO CT did not elicit IP ST, it may be that the IP’s commitment to change has been solidified by this point in the treatment because of success in changing his/her drinking. It also possible that the couple’s ability to tolerate negative interactions has been strengthened by interventions earlier in the therapy designed to increase positive interactions outside the therapy sessions, such as noticing positive behaviors from the partner and sharing positive leisure activities (McCrady & Epstein, 2009).ii The broader couple therapy literature has observed similar changes in the importance of positive and negative couple interactions to relationship satisfaction over the course of treatment (e.g., Doss et al., 2005).
The interplay between positive and negative couple interactions and their discussions of drinking also reflects the integral connections between a couple’s overall relationship and how they discuss drinking. In the first session, when the SO expressed CT or the IP expressed ST, the couple’s interactions became more negative, again suggesting tension around the discussion of drinking. In contrast, when their interactions were more positive, the SO expressed more CT. By midtreatment, however, these patterns had not changed notably—SO expressions of CT still led to more negative interactions, and positive interactions still led to more SO CT.
Although these nuanced analyses provided a clearer window into the interplay between the IP and SO and their relationship during ABCT sessions, the progression of speech variables within the treatment sessions had little predictive power related to drinking outcomes; only decreases in IP ST in the mid-treatment session predicted better drinking outcomes by the end of treatment. These findings parallel McCrady et al.’s (2019) findings that higher levels of IP ST during midtreatment, and the increases in ST during that session observed in the current study, bode poorly for IP drinking outcomes. The results also support growing findings in MI research that ST may be a stronger mechanism of change than CT (Magill et al., 2014; Magill et al., 2018). However, in contrast to findings in the MI literature that suggest the importance of understanding the progression within treatment sessions in predicting treatment response (Amrhein et al., 2003), the progression of the couple’s interactions across ABCT treatment sessions appears less important to drinking outcomes. Although ABCT does not target motivational language directly, the content of ABCT sessions addresses motivation by providing feedback about the patient’s drinking and consequences (session 1), conducting a functional analysis of drinking that looks at negative consequences of drinking, completing a decisional matrix, and including partner input as part of each intervention (McCrady & Epstein, 2009). The net effect of these interventions would be expected to manifest in an increase in CT and a decrease in ST over the course of the session.
The analysis of within-treatment behavior in ABCT does not provide information about the couple’s behavior outside the treatment sessions. During an ABCT session, the therapist actively guides and coaches the IP and SO in developing drinking-related coping strategies and positive communication skills. Although couples are given homework to practice behaviors between sessions and the data across the original trials suggest fairly high compliance with completing these assignments, we have no data to assess how effectively the couples were using the treatment skills in their everyday life. The lack of information about this key link between behavior within and outside of the session may help us to understand the limited findings on the relationship between within-session behaviors, the progression of those behaviors during a session, and the associations between in-session behaviors and drinking outcomes.
Several limitations of the current study should be noted, many of which presented analytic challenges. First, in both sessions, much of the IP and SO speech was neutral in tone, basically conveying information (McCrady et al., 2019), so that the behaviors of interest occurred infrequently and were not conducive to moment-by-moment analyses. The low rates of these behaviors might speak to advantages of Amrhein’s (2003) suggested preference for measuring the strength rather than frequency of speech categories. Second, we coded therapist behavior globally rather than at an utterance-by-utterance level, so we were unable to examine the role of the therapist in interactional sequences. This inability to consider the therapist in the interactional sequences might have diluted our ability to detect the impact of client and partner utterances on each other. In addition, we were unable to assess one key variable of interest, SO ST, because, despite significant efforts during the validation of the SCCIT-A, the coders did not achieve acceptable inter-rater reliability with the code (Owens et al., 2014). We can only speculate that SO ST might have influenced IP speech and drinking behavior given previous findings from Project MATCH (Manuel et al., 2012). Finally, the sample from the original ABCT clinical trials lacked diversity, in that all couples were heterosexual, predominately white, college educated, from the northeastern United States, and had no comorbid drug dependence.
5. Conclusion
The results suggest several within-treatment behaviors in ABCT that may help therapists to anticipate the course of the treatment sessions. First, the tension between IP and SO in discussing drinking appears to be characteristic of the start of treatment, and therapists might focus on the process that occurs between the partners if the IP begins to react negatively as the SO talks more about the importance of the IP changing their drinking. Similarly, if the therapist does not see an increasing alignment in the couple in discussing drinking over the course of the sessions, it might be important to address this continuing “misalignment” directly. In addition, if the therapist observes the IP and SO expressing high levels of negative behaviors toward each other in the session, the therapist might want to assess the extent to which this negative behavior relates specifically to a misalignment around goals related to the IP’s drinking rather than to other areas of relationship conflict. Finally, by midtreatment the therapist should be attending specifically to IP ST, both in terms of the frequency of ST, and whether ST is increasing or decreasing as the session progresses. The current study did not examine therapist behavior, but therapists can draw upon the MI literature to respond effectively to ST. Future research to understand MOBCs in ABCT could study therapist-IP-SO interactions in more detail, including moment-by-moment analyses, and also study relationships between within-session behavior and behavior outside the therapy room.
Highlights.
Acknowledgments
Research reported in this publication was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under award numbers R01AA081376, T32AA018108, and K01AA021431. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Financial Disclosure Dr. McCrady is the author of a therapist manual and client workbook on Alcohol Behavioral Couple Therapy. She receives royalties from the sale of these publications. The authors have no other conflicts of interest to report.
The authors thank one of the anonymous reviewers for this interpretation.
CT = change talk
ST = sustain talk
References
- American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.). Washington, DC: American Psychiatric Association.. [Google Scholar]
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: American Psychiatric Association.. [Google Scholar]
- Amrhein PC, Miller WR, Yahne CE, Palmer M, & Fulcher L (2003). Client commitment language during motivational interviewing predicts drug use outcomes. Journal of Consulting and Clinical Psychology, 71, 862–878. 10.1037/0022-006X.71.5.862 [DOI] [PubMed] [Google Scholar]
- Apodaca TR, & Longabaugh R (2009). Mechanisms of change in motivational interviewing: A review and preliminary evaluation of the evidence. Addiction, 104, 705–715. 10.1111/j.1360-0443.2009.02527.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Apodaca TR, Magill M, Longabaugh R, Jackson KM, & Monti PM (2013). Effect of a significant other on client change talk in motivational interviewing. Journal of Consulting and Clinical Psychology, 81, 35–46. 10.1037/a0030881 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Apodaca TR, Manuel J, Moyers T, & Amrhein P (2007). Motivational Interviewing with Significant Others (MISO) coding manual. Retrieved from http://casaa.unm.edu/download/miso.pdf
- Auld F Jr., & White AM (1959). Sequential dependencies in psychotherapy. The Journal of Abnormal and Social Psychology, 58(1), 100–104. 10.1037/h0043325 [DOI] [PubMed] [Google Scholar]
- Benson LA, McGinn MM, & Christensen A (2012). Common principles of couple therapy. Behavior Therapy, 43, 25–35. 10.1016/j.beth.2010.12.009 [DOI] [PubMed] [Google Scholar]
- Bourke E, Magill M, & Apodaca TR (2016). The in-session and long-term role of a significant other in motivational enhancement therapy for alcohol use disorders. Journal of Substance Abuse Treatment, 35, 35–43. 10.1016/j.jsat.2016.01.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis SD, Lebow JL, & Sprenkle DH (2012). Common factors of change in couple therapy. Behavior Therapy, 43, 36–48. 10.1016/j.beth.2011.01.009 [DOI] [PubMed] [Google Scholar]
- Doss BD, Thum YM, Sevier M, Atkins DC, & Christensen A (2005). Improving relationships: Mechanisms of change in couple therapy. Journal of Consulting and Clinical Psychology, 73, 624–633. 10.1037/0022-006X.73.4.624 [DOI] [PubMed] [Google Scholar]
- Epstein NB, & Baucom DH (2003). Enhanced cognitive-behavioral therapy for couples A contextual approach. Washington, DC: American Psychological Association. [Google Scholar]
- Feldstein Ewing SW, Filbey FM, Sabbineni A, Chandler LD, & Hutchison KE (2011). How psychosocial alcohol interventions work: A preliminary look at what fMRI can tell us. Alcoholism: Clinical and Experimental Research, 35, 643–651. 10.1111/j.1530-0277.2010.01382.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Houck JM, Hunter SB, Benson JG, Cochrum LL, Rowell LN, & D’Amico EJ (2015). Temporal variation in facilitator and client behavior during group motivational interviewing sessions. Psychology of Addictive Behaviors, 29, 941–949. 10.1037/adb0000107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Houck JM, Moyers TB, & Tesche CD (2013). Through a glass darkly: Some insights on change talk via magnetoencephalography. Psychology of Addictive Behaviors, 27, 489–500. 10.1037/a0029896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klostermann K, Kelley ML, Mignone T, Pusateri L, & Wills K (2011). Behavioral couples therapy for substance abusers: Where do we go from here? Substance Use and Misuse, 46, 1502–1509. 10.3109/10826084.2011.57644 [DOI] [PubMed] [Google Scholar]
- Lombardi DR, Button M, & Westra HA (2014). Measuring motivation: Change talk and counter-change talk in cognitive behavioral therapy for generalized anxiety. Cognitive Behaviour Therapy, 43, 12–21. 10.1080/16506073.2013.846400 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Magill M, Apodaca TR, Borsari B, Gaume J, Hoadley A, Gordon REF, & … Moyers T (2018). A meta-analysis of motivational interviewing process: Technical, relational, and conditional process models of change. Journal of Consulting and Clinical Psychology, 86, 140–157. 10.1037/ccp0000250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Magill M, Gaume J, Apodaca TR, Walthers J, Mastroleo NR, Borsari B, & Longabaugh R (2014). The technical hypothesis of motivational interviewing: A meta-analysis of MI’s key causal model. Journal of Consulting and Clinical Psychology, 82, 973–983. 10.1037/a0036833 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manuel JK, Houck JM, & Moyers TB (2012). The impact of significant others on motivational enhancement therapy: Findings from Project MATCH. Behavioural and Cognitive Psychotherapy, 40, 297–312. 10.1017/S1352465811000592 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrady BS (2012). Treating alcohol problems with couple therapy. Journal of Clinical Psychology: In Session, 68, 514–525. 10.1002/jclp.21854 [DOI] [PubMed] [Google Scholar]
- McCrady BS, & Epstein EE (2009). Overcoming alcohol problems: A couples-focused program. New York, NY: Oxford University Press. [Google Scholar]
- McCrady BS, Epstein EE, Cook S, Jensen N, & Hildebrandt T (2009). A randomized trial of individual and couple behavioral alcohol treatment for women. Journal of Consulting and Clinical Psychology, 77, 243–256. 10.1037/a0014686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrady BS, Epstein EE, Hallgren KA, Cook S, & Jensen NK (2016). Women with alcohol dependence: A randomized trial of couple versus individual plus couple therapy. Psychology of Addictive Behaviors, 30, 287–299. 10.1037/adb0000158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrady BS, Epstein EE, Hirsch LS (1999). Maintaining change after conjoint behavioral alcohol treatment for men: Outcomes at six months. Addiction, 94, 1381–1396. 10.1046/j.1360-0443.1999.949138110.x [DOI] [PubMed] [Google Scholar]
- McCrady BS, Noel NE, Abrams DB, Stout RL, Nelson HF, & Hay WM (1986). Comparative effectiveness of three types of spouse involvement in outpatient behavioral alcoholism treatment. Journal of Studies on Alcohol, 47, 459–467. 10.15288/jsa.1986.47.459 [DOI] [PubMed] [Google Scholar]
- McCrady BS, Tonigan JS, Ladd BO, Hallgren KA, Pearson MR, Owens MD, & Epstein EE (2019). Alcohol Behavioral Couple Therapy: In-session behavior, active ingredients and mechanisms of behavior change. Journal of Substance Abuse Treatment, 99, 139–148. 10.1016/j.jsat.2019.01.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrady BS, Wilson AD, Muñoz RE, Fink BC, Fokas K, & Borders A (2016). Alcohol-focused behavioral couple therapy. Family Process, 55, 443–459. 10.1111/famp.12231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller WR, & Rollnick S (2013). Motivational interviewing: Helping people change (3rd ed.). New York, NY: Guilford Press. [Google Scholar]
- Moyers TB, Martin T, Christopher PJ, Houck JM, Tonigan JS, & Amrhein PC (2007). Client language as a mediator of motivational interviewing efficacy: Where is the evidence? Alcoholism: Clinical and Experimental Research, 31, 40S–47S. 10.1111/j.1530-0277.2007.00492.x [DOI] [PubMed] [Google Scholar]
- Moyers TB, Martin T, Houck JM, Christopher PJ, & Tonigan JS (2009). From in-session behaviors to drinking outcomes: A causal chain for motivational interviewing. Journal of Consulting and Clinical Psychology, 77, 1113–1124. 10.1037/a0017189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2017). Mplus user’s guide (8th ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Owens MD, McCrady BS, Borders AZ, Brovko JM, & Pearson MR (2014). Psychometric properties of the System for Coding Couples’ Interactions in Therapy–Alcohol. Psychology of Addictive Behaviors, 28, 1077–1088. 10.1037/a0038332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Powers MB, Vedel E, & Emmelkamp PM (2008). Behavioral couples therapy (BCT) for alcohol and drug use disorders: A meta-analysis. Clinical Psychology Review, 28, 952–962. 10.1016/j.cpr.2008.02.002 [DOI] [PubMed] [Google Scholar]
- Sijercic I, Button ML, Westra HA, & Hara KM (2016). The interpersonal context of client motivational language in cognitive–behavioral therapy. Psychotherapy, 53, 13–21. 10.1037/pst0000017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sobell LC, Agrawal S, Annis H, Ayala-Velazquez H, Echeverria L, Leo GI, & … Ziólkowski M (2001). Cross-cultural evaluation of two drinking assessment instruments: Alcohol Timeline Followback and Inventory of Drinking Situations. Substance Use and Misuse, 36, 313–331. 10.1081/JA-100102628 [DOI] [PubMed] [Google Scholar]
- Sobell LC, & Sobell MB (1992). Timeline Follow-Back: A technique for assessing self-reported ethanol consumption In Allen J & Litten RZ (Eds.), Measuring alcohol consumption: Psychosocial and biological methods (pp. 41–72). Totowa, NJ: Humana Press. [Google Scholar]