

TO THE EDITOR:
Since its introduction 3 decades ago, upfront autologous hematopoietic stem cell transplantation (auto-HCT) with melphalan (Mel) 200 mg/m2 remains the standard of care in the treatment of patients with transplant-eligible, newly diagnosed multiple myeloma (MM).1-4 Several drug combinations for an optimal conditioning regimen have been tried without a convincing benefit. The combination of busulfan (Bu) and Mel is synergistic against MM cell lines.5 Previous studies with the combination of oral busulfan and Mel showed longer progression-free survival (PFS), albeit with a higher rate of veno-occlusive disease.6,7 Since then, the introduction of intravenous busulfan with linear pharmacokinetics and more reproducible systemic exposure has largely ameliorated veno-occlusive disease.8 We studied this combination regimen in a phase 3 trial in newly diagnosed MM patients receiving upfront auto-HCT. Our results showed that IV Bu plus Mel (Bu-Mel) was associated with a significantly better PFS than single-agent Mel (hazard ratio, 0.53; 3-year PFS, 72% vs 50%).5
Even with the use of novel drugs in the treatment of MM, the outcome in patients harboring high-risk (HR) cytogenetic abnormalities remains suboptimal.1,3 We hypothesized that myeloma patients with HR cytogenetics may particularly benefit from the intensification of conditioning in the Bu-Mel regimen. In a subset analysis of our trial, where 62 HR patients were evaluated separately, a significantly longer PFS in the Bu-Mel arm (median PFS not reached; P = .0087) vs Mel arm (median 25 months) was observed. Here, we report the updated outcomes of HR patients enrolled in that trial.
Between 2011 and 2017, 205 patients were enrolled in the trial, 105 to the Bu-Mel arm and 100 to the Mel arm. HR myeloma was defined based on the presence of HR cytogenetic profile per International Myeloma Working Group criteria9 and included 17p deletion, t(4;14), t(14;16), t(14;20), and 1q gain detected by fluorescence in situ hybridization and del13q detected by karyotyping. Sixty-two patients had HR MM, 32 in the Bu-Mel arm and 30 in the Mel arm. Patients in the Bu-Mel arm received a test dose of 32 mg/m2 Bu on day −8 if the participant was an outpatient or on day −9 if the participant was an inpatient, followed by pharmacokinetically adjusted doses of Bu on days −7, −6, −5, and −4, with a daily target area under the curve of 5000 mmol/min, and Mel was administered on days −2 and −1 with a total Mel dose 140 mg/m2. Patients in the Mel arm received Mel 200 mg/m2 on day-2. The primary objective was to compare PFS in HR NDMM patients who underwent upfront auto-HCT with Bu-Mel vs Mel conditioning.
Baseline patient characteristics of HR MM arms are provided in Table 1. There was no significant difference in the hematopoietic cell transplantation–specific comorbidity index score, induction therapy, response to induction, number of patients receiving maintenance therapy, or other characteristics between the 2 treatment arms. The median age at auto-HCT was 61 years (range, 31.7-70.6 years) in the Bu-Mel arm and 60 years (range, 38.8-69.5 years) in the Mel arm. Overall, 32 (100%) and 29 (97%) patients received induction therapy with immunomodulatory drugs and/or proteasome inhibitors in the Bu-Mel and Mel arms, respectively (Table 1).
Table 1.
Summary of patient and clinical characteristics
| Variables | Bu-Mel (n = 32) | Mel (n = 30) | P |
|---|---|---|---|
| Age at auto-HCT, y | 32 | 30 | .28 |
| Median (range), y | 61.4 (31.7-70.6) | 59.8 (38.8-69.5) | |
| Sex, n (%) | |||
| Male | 16 (50) | 18 (60) | .46 |
| Female | 16 (50) | 12 (40) | |
| R-ISS, n (%) | |||
| I | 6 (22) | 8 (38) | .39 |
| II | 17 (63) | 9 (43) | |
| III | 4 (15) | 4 (19) | |
| Missing | 5 | 9 | |
| HR features (IMWG), n (%) | |||
| Individual | |||
| del(17p) | 11 (34) | 8 (27) | |
| Gain 1q | 18 (56) | 17 (57) | |
| Copy number 3 | 14 | 8 | |
| Copy number ≥4 | 1 | 3 | |
| Not available | 3 | 6 | |
| t(4;14) | 6 (19) | 4 (13) | |
| del(13q) (karyotype) | 6 (19) | 8 (27) | |
| Combined | .61 | ||
| del(17p)/Gain 1q (copy number ≥ 4)/t(4;14) | 17 (55) | 14 (47) | |
| Other | 14 (45) | 16 (53) | |
| Missing | 1 | 0 | |
| Serum LDH | |||
| Normal | 19 (83) | 19 (86) | 1.00 |
| Abnormal | 4 (17) | 3 (14) | |
| Missing | 9 | 8 | |
| HCT-CI, n (%) | |||
| 0 | 11 (34) | 14 (47) | .23 |
| 1-2 | 8 (25) | 10 (33) | |
| ≥3 | 13 (41) | 6 (20) | |
| Response to induction, n (%) | |||
| sCR/CR | 6 (19) | 4 (13) | .55 |
| nCR | 3 (9) | 1 (3) | |
| VGPR | 9 (28) | 11 (37) | |
| PR | 14 (44) | 12 (40) | |
| SD | 0 | 2 (7) | |
| Maintenance regimen, n (%) | |||
| Lenalidomide | 14 (44) | 8 (27) | .69 |
| Lenalidomide and elotuzumab | 4 (13) | 5 (17) | |
| Lenalidomide and ixazomib | 1 (3) | 3 (10) | |
| Lenalidomide and dexamethasone | 2 (6) | 1 (3) | |
| Bortezomib | 3 (9) | 7 (23) | |
| IRD | 2 (6) | 1 (3) | |
| KRD | 1 (3) | 2 (7) | |
| VRD | 2 (6) | 1 (3) | |
| None | 3 (9) | 2 (7) | |
| Induction regimen, n (%) | |||
| VRD | 19 (59) | 17 (59) | .99 |
| VCD | 6 (19) | 5 (17) | |
| KRD | 4 (13) | 3 (10) | |
| Vd | 3 (9) | 3 (10) | |
| CBAD | 0 | 1 (3) | |
| Missing | 0 | 1 |
CBAD, cyclophosphamide, bortezomib, adriamycin, and dexamethasone; CR, complete response; HCT-CI, hematopoietic cell transplantation–specific comorbidity index; IMWG, International Myeloma Working Group; IRD, ixazomib, lenalidomide, and dexamethasone; KRD, carfilzomib, lenalidomide, and dexamethasone; LDH, lactate dehydrogenase; nCR, near CR; PR, partial response; sCR, stringent complete response; SD, stable disease; VCD, bortezomib, cyclophosphamide, and dexamethasone; Vd, bortezomib and dexamethasone; VGPR, very good partial response; VRD, .
The median time to neutrophil engraftment (absolute neutrophil count ≥0.5 × 109/L) was 11 and 12 days in the Bu-Mel and Mel arms, respectively (P = .002). The median time to platelet engraftment (platelet count ≥20 × 109/L without transfusion support) was 10 and 12.5 days in the Bu-Mel and Mel arms, respectively (P < .001). There was no 100-day treatment-related mortality in either arm. There was an increased incidence of grade II to IV toxicities in the Bu-Mel arm (32/32; 100%) compared with the Mel arm (25/30; 83%) (P < .001). Details of these toxicities are provided in supplemental Table 1. These toxicities were mostly reversible and self-limited and included mucositis, febrile neutropenia, and transaminase elevation. There was no grade IV toxicity in either arm. Grade II to III mucositis was seen in 24 (75%) and 5 (17%) patients in the Bu-Mel and the Mel arms, respectively (P < .001). Grade III neutropenic fever was seen in 22 (69%) and 9 (30%) patients in the Bu-Mel and Mel arms, respectively (P = .005).
The median duration of follow-up from randomization was 42.6 months (range, 18.9-85.7 months) and 36.6 months (range, 3.4-74.9 months) in the Bu-Mel and Mel arms, respectively. The overall response rate, defined as partial response or better, at day 90 after auto-HCT was 100% (32/32) and 93% (28/30) of patients in the Bu-Mel and the Mel arm, respectively (P = .23). The rates of day-90 stringent complete response plus and complete response were 34% (11/32) and 37% (11/30) of patients in the Bu-Mel and Mel arms, respectively (P = 1.00). At day 90, no patients in the Bu-Mel arm and 3 patients in the Mel arm had progressive disease. The rate of best response (≥ very good partial response) achieved was 94% (30/32) and 83% (25/30) of patients in the Bu-Mel and Mel arms, respectively (P = .25). The survival outcomes are provided in supplemental Table 2. The 3-year PFS rates were 69% (95% confidence interval [CI], 50% to 82%) and 41% (95% CI, 22% to 59%) in the Bu-Mel and Mel arms, respectively. Median PFS was 44.7 (95% CI, 31.9 to not reached) months and 25.7 (95% CI, 16.5 to not reached) months in the Bu-Mel and Mel arms, respectively (P = .044; Figure 1A) (hazard ratio [95% CI], 0.48 [0.24-1.00]; P = .049). The 3-year overall survival rates were 90% (95% CI, 73% to 97%) and 87% (95% CI, 65% to 96%) in the Bu-Mel and Mel arms, respectively. The median overall survival was not reached in either arm (P = .50; Figure 1B) (hazard ratio [95% CI], 0.67 [0.20-2.20]; P = .51). In a fitted Bayesian piecewise exponential regression model, treatment with Bu-Mel was associated with superior PFS where the posterior probability of a beneficial effect was 0.90 (Bu-Mel arm vs Mel arm: mean hazard ratio, 0.62 [95% CI, 0.18-1.21]). Additional details are provided in supplemental Table 3.
Figure 1.
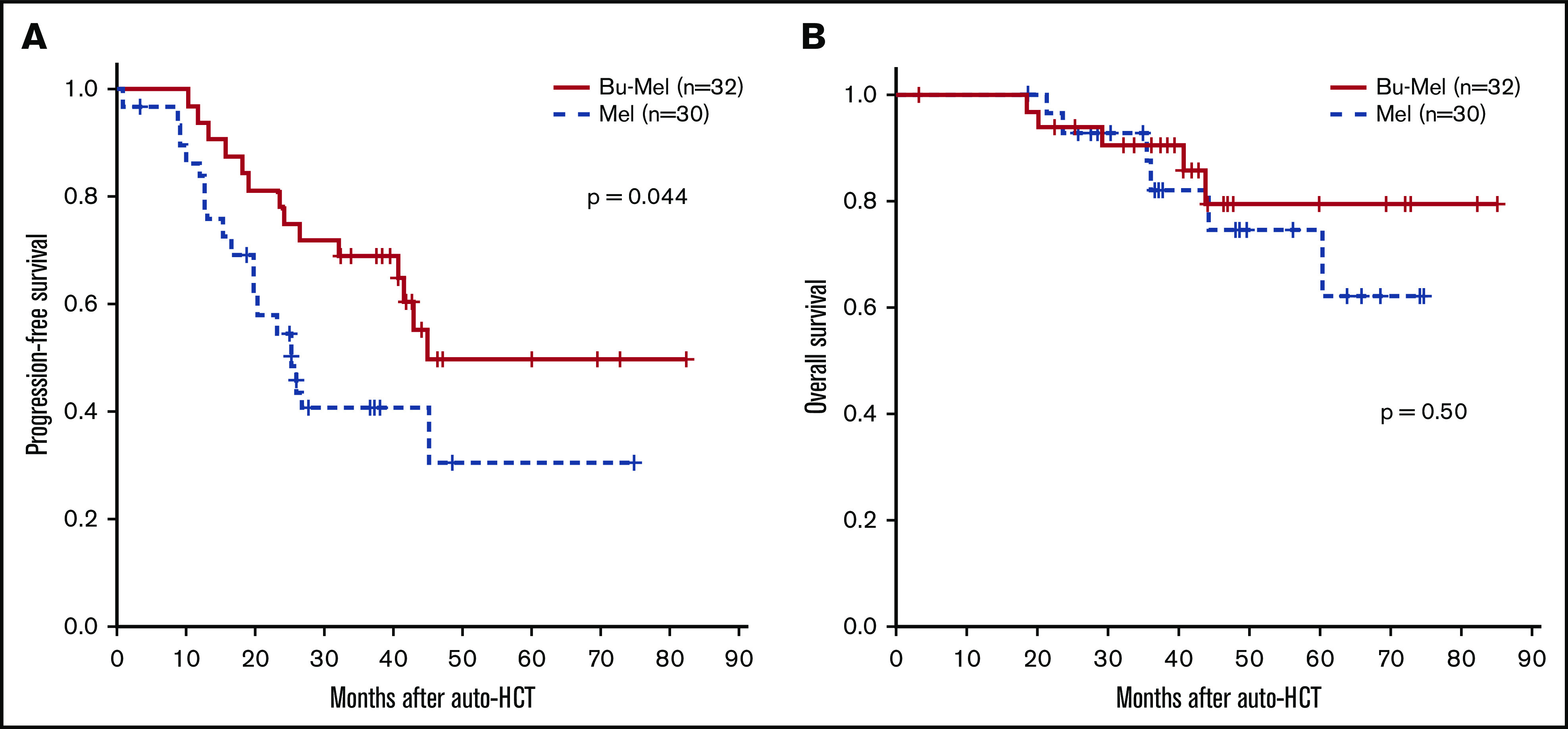
Survival outcomes. (A) PFS by treatment group. (B) Overall survival.
Two patients (7%) in the Mel arm received consolidation therapy after auto-HCT compared with 5 patients (16%) in the Bu-Mel arm (P = .62). Fifty-seven patients received maintenance therapy during the trial (29 in the Bu-Mel arm [median duration, 14.0 months (range, 1.8-53.4 months)] and 28 in the Mel arm [median duration, 9.8 months (range, 0.3-38.8 months)]; P = .19). Of these patients, 12 (41%) in the Bu-Mel arm discontinued maintenance therapy because of disease progression or toxicity after a median duration of 10.3 months (range, 2.2-36.0 months) of maintenance compared with 16 (57%) patients in the Mel arm after a median duration of 9.4 months (range, 2.2-23.8 months) of maintenance (P = .96). More patients had early disease progression in the Mel arm than in the Bu-Mel arm, resulting in early discontinuation of maintenance therapy, which partly explains the shorter median duration of maintenance in the Mel arm. Furthermore, the median follow-up in the Mel arm was shorter compared with the Bu-Mel arm, which might also have contributed to a shorter duration of maintenance in the Mel arm.
This randomized trial showed an improvement in PFS with the Bu-Mel conditioning regimen in patients with newly diagnosed myeloma with HR cytogenetics. In addition, we showed that the combination of Bu-Mel led to a 52% reduction in the risk of disease progression or death compared with Mel alone. These results compare favorably with recent prospective randomized trials conducted in the era of novel therapeutics, which include BMTCTN 070210 and EMN02/HO95.2 The 3-year PFS for HR patients with single auto-HCT was 40% and ∼45% in the BMTCTN0702 and EMN02/HO95 trials, respectively. Although it is always challenging to compare the results of different clinical trials, the PFS reported in these 2 trials was similar to the PFS seen in the Mel arm of our trial but significantly lower than what we reported in the Bu-Mel arm.
Interestingly, in the EMN02/HO95 trial, the 3-year PFS of 63% with tandem transplant in HR MM was comparable to what we reported in the Bu-Mel arm of our study. These data highlight that a risk-adapted approach using a higher intensity conditioning regimen, such as Bu-Mel, has the potential to significantly improve the outcomes in HR MM patients.11 Although the combination of Bu-Mel had caused more adverse events compared with Mel alone, most of the toxicities were reversible and self-limiting. We acknowledge that our trial is a single-center study, and we expect these results to be validated in a multicenter trial. A similar phase 3 randomized trial comparing IV Bu-Mel to Mel alone conditioning regimen has been completed (NCT019162520) by PETHEMA foundation group, and results are currently being awaited. In conclusion, our updated data continue to show that the Bu-Mel conditioning regimen leads to significantly better PFS when compared with Mel alone in HR MM patients.
Supplementary Material
The full-text version of this article contains a data supplement.
Contribution: N.S. interpreted the data and wrote the manuscript; D.R.M. performed the statistical analysis, interpreted the data, and critically reviewed the manuscript; R.D. and G.R. collected the data; Q.B., G.T., U.R.P., C.M.H., Y.N., P.K., A.M.A., R.M., S.S., I.F.K., D.M.W., S.K.T., H.C.L., K.K.P., R.Z.O., and R.E.C. critically reviewed the manuscript; and M.H.Q. designed and supervised the study, interpreted the data, and revised the manuscript.
Conflict-of-interest disclosure: R.Z.O. declares laboratory research funding from BioTheryX and clinical research funding from CARsgen Therapeutics, Celgene, Exelixis, Janssen Biotech, Sanofi-Aventis, and Takeda Pharmaceuticals North America; has served on advisory boards for Amgen, Bristol-Myers Squibb, Celgene, EcoR1 Capital LLC, Forma Therapeutics, Genzyme, GSK Biologicals, Ionis Pharmaceuticals, Janssen Biotech, Juno Therapeutics, Kite Pharma, Legend Biotech USA, Molecular Partners, Regeneron Pharmaceuticals, Sanofi-Aventis, Servier, and Takeda Pharmaceuticals North America; and is a founder of Asylia Therapeutics, with associated patents and an equity interest, though this technology does not bear on the current study. The remaining authors declare no competing financial interests.
Correspondence: Muzaffar H. Qazilbash, Department of Stem Cell Transplantation and Cellular Therapy, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX 77030; e-mail: mqazilba@mdanderson.org.
References
- 1.Attal M, Lauwers-Cances V, Hulin C, et al. ; IFM 2009 Study . Lenalidomide, bortezomib, and dexamethasone with transplantation for myeloma. N Engl J Med. 2017;376(14):1311-1320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cavo M, Gay F, Beksac M, et al. . Autologous haematopoietic stem-cell transplantation versus bortezomib-melphalan-prednisone, with or without bortezomib-lenalidomide-dexamethasone consolidation therapy, and lenalidomide maintenance for newly diagnosed multiple myeloma (EMN02/HO95): a multicentre, randomised, open-label, phase 3 study. Lancet Haematol. 2020;7(6):e456-e468. [DOI] [PubMed] [Google Scholar]
- 3.Gay F, Cerrato C, Petrucci MT, et al. . Efficacy of carfilzomib lenalidomide dexamethasone (KRd) with or without transplantation in newly diagnosed myeloma according to risk status: results from the FORTE trial. J Clin Oncol. 2019;37(15_suppl):8002. [Google Scholar]
- 4.Voorhees PM, Kaufman JL, Laubach J, et al. . Daratumumab, lenalidomide, bortezomib, and dexamethasone for transplant-eligible newly diagnosed multiple myeloma: the GRIFFIN trial. Blood. 2020;136(8):936-945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bashir Q, Thall PF, Milton DR, et al. . Conditioning with busulfan plus melphalan versus melphalan alone before autologous haemopoietic cell transplantation for multiple myeloma: an open-label, randomised, phase 3 trial. Lancet Haematol. 2019;6(5):e266-e275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lahuerta JJ, Mateos MV, Martínez-López J, et al. ; Grupo Español de MM and Programa para el Estudio de la Terapéutica en Hemopatía Maligna Cooperative Study Groups . Busulfan 12 mg/kg plus melphalan 140 mg/m2 versus melphalan 200 mg/m2 as conditioning regimens for autologous transplantation in newly diagnosed multiple myeloma patients included in the PETHEMA/GEM2000 study. Haematologica. 2010;95(11):1913-1920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lahuerta JJ, Grande C, Blade J, et al. ; Spanish Multiple Myeloma Group . Myeloablative treatments for multiple myeloma: update of a comparative study of different regimens used in patients from the Spanish registry for transplantation in multiple myeloma. Leuk Lymphoma. 2002;43(1):67-74. [DOI] [PubMed] [Google Scholar]
- 8.Madden T, de Lima M, Thapar N, et al. . Pharmacokinetics of once-daily IV busulfan as part of pretransplantation preparative regimens: a comparison with an every 6-hour dosing schedule. Biol Blood Marrow Transplant. 2007;13(1):56-64. [DOI] [PubMed] [Google Scholar]
- 9.Sonneveld P, Avet-Loiseau H, Lonial S, et al. . Treatment of multiple myeloma with high-risk cytogenetics: a consensus of the International Myeloma Working Group. Blood. 2016;127(24):2955-2962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stadtmauer EA, Pasquini MC, Blackwell B, et al. . Autologous transplantation, consolidation, and maintenance therapy in multiple myeloma: results of the BMT CTN 0702 trial. J Clin Oncol. 2019;37(7):589-597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Joseph NS, Kaufman JL, Dhodapkar MV, et al. . Long-term follow-up results of lenalidomide, bortezomib, and dexamethasone induction therapy and risk-adapted maintenance approach in newly diagnosed multiple myeloma. J Clin Oncol. 2020;38(17):1928-1937. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.