

Abstract
In the United States, the efficacy and safety of convalescent plasma for treating coronavirus disease 2019 (COVID-19) is currently being tested in randomized placebo-controlled clinical trials. Treatment of individual patients with COVID-19 with convalescent plasma outside such trials is also now permitted through U.S. Food and Drug Administration Emergency Use Authorization. Here, members of the National Institutes of Health COVID-19 Treatment Guidelines Panel provide their views regarding use of convalescent plasma for treating COVID-19.
Currently, no Food and Drug Administration (FDA)–approved therapeutics exist for coronavirus disease 2019 (COVID-19). In this context, the pandemic has put considerable pressure on health care providers to prescribe treatments despite limited information about their safety and efficacy. This pressure has exacerbated the tension between the importance of practicing evidence-based medicine and the urgency of providing access to promising therapies before their safety and efficacy are established.
As members of the National Institutes of Health COVID-19 Treatment Guidelines Panel (the Panel) (1), we are charged with providing guidance for U.S. clinicians on the treatment of COVID-19 by reviewing current scientific evidence and providing real-time recommendations based on the strength and quality of the data.
On 23 August 2020, the FDA issued an Emergency Use Authorization (EUA) for convalescent plasma for treating COVID-19 (2). An EUA does not constitute drug approval by the FDA. Rather, an EUA allows the FDA to facilitate the availability and unapproved uses of medical products during a public health emergency (3). The criteria for issuing an EUA for medical products include the following: The public health concern must be serious or life threatening; sufficient evidence must exist that the product “may be effective”; the known and potential benefits of the product, when used to diagnose, prevent, or treat the identified disease or condition, outweigh the known and potential risks of the product; and no adequate, approved alternatives to the product are available (3).
A strong scientific rationale and historical precedents exist for the study of passive immunotherapeutic approaches for viral infections (4). Concentrated, virus-specific immunoglobulin preparations are FDA approved for the postexposure prophylaxis of such viral infections as hepatitis B, varicella, and rabies (5). Recently, a randomized controlled trial (RCT) demonstrated the efficacy of 2 different monoclonal antibody products for treating Ebola virus disease (6).
The situation is less clear regarding the safety and efficacy of convalescent plasma, which has been used to treat viral infections from the 1918 influenza pandemic to the recent epidemics of severe acute respiratory syndrome (SARS), H1N1 influenza, Middle East respiratory syndrome, and Ebola virus disease (7–10). The only RCT demonstrating efficacy of convalescent plasma for an infectious disease was conducted more than 40 years ago, for treating Argentine hemorrhagic fever (11).
Early in the COVID-19 pandemic, convalescent plasma was used in China to treat hospitalized patients with COVID-19 (7). Shortly thereafter, RCTs evaluating convalescent plasma in patients with COVID-19 began in several countries, including the United States (12). In March 2020, the FDA authorized expanded access to convalescent plasma for treating severe or life-threatening COVID-19 under individual-patient emergency Investigational New Drug applications. The Mayo Clinic's Expanded Access Program (EAP) was developed in parallel to provide broader access to convalescent plasma; however, it was not designed to generate definitive data on safety or to evaluate efficacy (13). One of the requirements for an EAP is that it not interfere with pivotal trials (14). Adequately powered RCTs of convalescent plasma in the United States have been slow to enroll patients.
Given the lack of data from properly powered RCTs, and the need to inform regulatory decision making regarding continued access to convalescent plasma, both the FDA and the Mayo Clinic performed retrospective, indirect evaluations of efficacy by using EAP data, hypothesizing that patients who received plasma units with higher titers of neutralizing antibodies would have better clinical outcomes. The results of the analyses were used as supporting evidence for the EUA.
The FDA analysis included 4330 patients, and donor neutralizing antibody titers were measured by the Broad Institute, using a SARS coronavirus 2 (SARS-CoV-2) neutralization assay (15). The analysis revealed no difference in 7-day mortality between the patients who received high-titer and those who received low-titer plasma in the overall population or in the subset of patients who were intubated. However, among nonintubated patients (approximately two thirds of those analyzed), 11% of those who received high-titer plasma died within 7 days of transfusion compared with 14% who received low-titer plasma (P = 0.03) (16). In a post hoc analysis of nonintubated patients who were younger than 80 years and treated within 72 hours of diagnosis, 7-day mortality for those who received high- versus low-titer plasma was 6.3% and 11.3%, respectively (P = 0.0008) (15).
A similar efficacy analysis by the Mayo Clinic included 3082 participants who had received a single unit of plasma among the 35 322 participants who had received plasma through the EAP by 4 July 2020 (17). Antibody titers were measured by using the VITROS anti–SARS-CoV-2 IgG assay (Ortho Clinical Diagnostics), and outcomes were compared among patients receiving low- (lowest 18%), medium-, and high-titer (highest 17%) plasma. After adjusting for baseline characteristics, the 30-day mortality rate was 29.1% in the low-titer group and 24.7% in the high-titer group. This difference did not reach statistical significance. The Mayo Clinic post hoc subgroup analyses also suggested a benefit of high-titer plasma in patients who received plasma within 3 days of COVID-19 diagnosis (17).
The FDA concluded that the totality of data, including additional data from small randomized trials and nonrandomized, observational, and animal studies, met the criteria for EUA issuance.
Despite clearly meeting the “may be effective” criterion for EUA issuance, the analyses of the EAP data are not sufficient to establish the efficacy or safety of convalescent plasma because of the lack of an untreated control group. For example, the possibility that differences in outcomes are attributable to harm from low-titer plasma rather than benefit from high-titer plasma cannot be excluded. In addition, the EAP data may be subject to several confounders, including regional differences and temporal trends in COVID-19 management. There is no widely available and generally agreed-upon best test for measuring neutralizing antibodies, and the antibody titers in convalescent plasma from patients who have recovered from COVID-19 are highly variable. In addition, the analyses focused on early mortality, which may not be clinically meaningful in the context of the prolonged disease course of COVID-19. The efficacy analyses rely on a subset of EAP patients and thus represent only a fraction of patients who received plasma through the EAP (17). In this regard, additional analyses of the EAP cohort and completion of the current RCTs will be of critical importance.
Taking everything into account, the Panel has determined that currently the data are insufficient to recommend for or against convalescent plasma for treating COVID-19 (18). Prospective, well-controlled, and adequately powered RCTs are needed to determine whether convalescent plasma and other passive immunotherapies are effective and safe for COVID-19 treatment. Although providers have access to this therapy, the Panel cannot recommend it as a standard of care for treating COVID-19 at this time. This is consistent with the language of the convalescent plasma EUA Fact Sheet (19).
The COVID-19 pandemic has intensified the tension between providing rapid access to promising therapies and generating the scientific evidence needed to establish whether those therapies are safe and effective. This tension was also noted during the West African Ebola outbreak in 2014 to 2016, when several therapies, including convalescent plasma, were claimed to be of benefit. A National Academies of Sciences, Engineering, and Medicine review of that response noted that RCTs are critical during an outbreak, because they are the quickest way to identify effective therapies (20). Experience with convalescent plasma, hydroxychloroquine, and other interventions has taught us that large observational cohorts, EAPs, and EUAs can have a profound impact on our ability to conduct the properly designed RCTs necessary to provide definitive evidence of safety and efficacy. Conversely, the lack of access to large RCTs at many health care centers during the COVID-19 pandemic may exacerbate issues of equity in access to care. Expanded Access Programs continue to be an important mechanism to provide promising therapies for patients who do not otherwise have access to them (that is, through clinical trials). Balancing this tension is challenging but imperative to maintaining the ability to generate rigorous and convincing evidence during a public health crisis.
Despite the challenges of the COVID-19 pandemic, conducting well-controlled, adequately powered RCTs is possible. Two such trials, ACTT (Adaptive COVID-19 Treatment Trial) and RECOVERY (Randomized Evaluation of COVID-19 Therapy), recently demonstrated the efficacy of remdesivir and dexamethasone, respectively, for treating COVID-19 (21, 22). Collaboration and partnership among governmental agencies, industry, academia, and the public are needed to establish and carry out a robust and coordinated emergency research response, including the rapid development, deployment, and analysis of high-caliber RCTs. This approach is the quickest and most efficient way to generate the answers needed to provide the best evidence-based patient care.
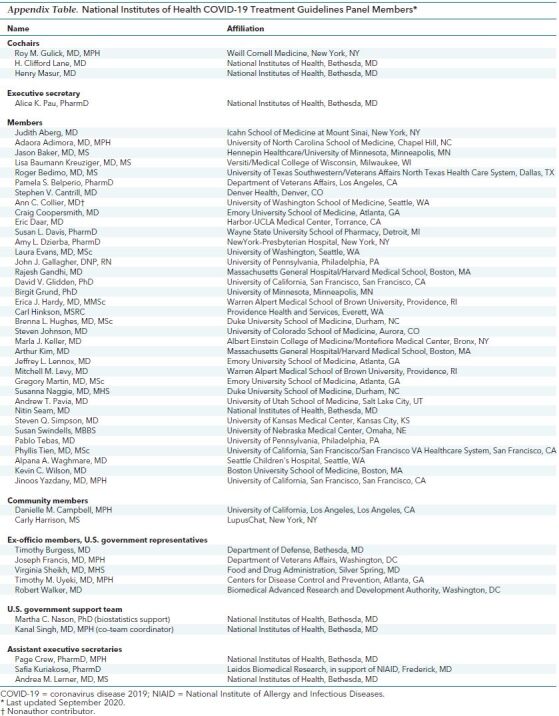
Appendix Table. National Institutes of Health COVID-19 Treatment Guidelines Panel Members*.
Footnotes
This article was published at Annals.org on 25 September 2020
* For members of the National Institutes of Health COVID-19 Treatment Guidelines Panel, see the Appendix Table (available at Annals.org).
References
- 1. National Institutes of Health. COVID-19 Treatment Guidelines. Appendix A, Table 1. COVID-19 Treatment Guidelines Panel Members. Accessed at www.covid19treatmentguidelines.nih.gov/panel-roster on 7 September 2020.
- 2. U.S. Food and Drug Administration. Convalescent plasma letter of authorization. Accessed at www.fda.gov/media/141477/download on 6 September 2020.
- 3. U.S. Food and Drug Administration. Emergency Use Authorization of Medical Products and Related Authorities: Guidance for Industry and Other Stakeholders. Accessed at www.fda.gov/media/97321/download on 31 August 2020.
- 4. Fischer JC, Zänker K, van Griensven M, et al. The role of passive immunization in the age of SARS-CoV-2: an update. Eur J Med Res. 2020;25:16. [PMID: 32404189] doi:10.1186/s40001-020-00414-5 [DOI] [PMC free article] [PubMed]
- 5. Centers for Disease Control and Prevention. ACIP Vaccine Recommendations and Guidelienes. Accessed at www.cdc.gov/vaccines/hcp/acip-recs/index.html on 7 September 2020.
- 6. Mulangu S, Dodd LE, Davey RT Jr, et al; PALM Writing Group. A randomized, controlled trial of Ebola virus disease therapeutics. N Engl J Med. 2019;381:2293-2303. [PMID: 31774950] doi:10.1056/NEJMoa1910993 [DOI] [PMC free article] [PubMed]
- 7. Mair-Jenkins J, Saavedra-Campos M, Baillie JK, et al; Convalescent Plasma Study Group. The effectiveness of convalescent plasma and hyperimmune immunoglobulin for the treatment of severe acute respiratory infections of viral etiology: a systematic review and exploratory meta-analysis. J Infect Dis. 2015;211:80-90. [PMID: 25030060] doi:10.1093/infdis/jiu396 [DOI] [PMC free article] [PubMed]
- 8. Beigel JH, Tebas P, Elie-Turenne MC, et al; IRC002 Study Team. Immune plasma for the treatment of severe influenza: an open-label, multicentre, phase 2 randomised study. Lancet Respir Med. 2017;5:500-511. [PMID: 28522352] doi:10.1016/S2213-2600(17)30174-1 [DOI] [PMC free article] [PubMed]
- 9. Ko JH, Seok H, Cho SY, et al. Challenges of convalescent plasma infusion therapy in Middle East respiratory coronavirus infection: a single centre experience. Antivir Ther. 2018;23:617-622. [PMID: 29923831] doi:10.3851/IMP3243 [DOI] [PubMed]
- 10. van Griensven J, Edwards T, de Lamballerie X, et al; Ebola-Tx Consortium. Evaluation of convalescent plasma for Ebola virus disease in Guinea. N Engl J Med. 2016;374:33-42. [PMID: 26735992] doi:10.1056/NEJMoa1511812 [DOI] [PMC free article] [PubMed]
- 11. Maiztegui JI, Fernandez NJ, de Damilano AJ. Efficacy of immune plasma in treatment of Argentine haemorrhagic fever and association between treatment and a late neurological syndrome. Lancet. 1979;2:1216-7. [PMID: 92624] [DOI] [PubMed]
- 12. National Institutes of Health. List of randomized trials of convalescent plasma. ClinicalTrials.gov. Accessed at www.clinicaltrials.gov/ct2/results?term=convalescent+plasma&cond=Covid19&intr=Randomized on 7 September 2020.
- 13. Mayo Clinic. Expanded Accesss to Convalescent Plasma for the Treatment of Patients With COVID-19 [Protocol]. Version 10.0. Accessed at www.uscovidplasma.org/physicians-protocol on 6 September 2020.
- 14. U.S. Food and Drug Administration. Title 21. Chapter 1. Part 312. Subpart I. Expanded Access to Investigational Drugs for Treatment Use. Section 312.305(a)(3).
- 15. U.S. Food and Drug Administration. EUA 26382: Emergency Use Authorization (EUA) Request. Accessed at www.fda.gov/media/141481/download on 6 September 2020.
- 16. U.S Food and Drug Administration. Decisional memo. Accessed at www.fda.gov/media/141480/download on 6 September 2020.
- 17. Joyner MJ, Senefeld JW, Klassen SA, et al. Effect of convalescent plasma on mortality among hospitalized patients with COVID-19: initial three-month experience. medRxiv. 2020. [PMID: 32817978] doi:10.1101/2020.08.12.20169359
- 18. National Institutes of Health. The COVID-19 Treatment Guidelines Panel's Statement on the Emergency Use Authorization of Convalescent Plasma for the Treatment of COVID-19. Accessed at www.covid19treatmentguidelines.nih.gov/statement-on-convalescent-plasma-eua on 7 September 2020.
- 19. U.S. Food and Drug Administration. Fact Sheet for Health Care Providers. Emergency Use Authorization (EUA) of COVID-19 Convalescent Plasma for Treatment of COVID-19 in Hospitalized Patients. Accessed at www.fda.gov/media/141478/download on 6 September 2020.
- 20. National Academies of Sciences, Engineering, and Medicine. Integrating Clinical Research into Epidemic Response: The Ebola Experience. National Academies Pr; 2017. [PubMed]
- 21. Beigel JH, Tomashek KM, Dodd LE. Remdesivir for the treatment of COVID-19 - preliminary report. Reply [Letter]. N Engl J Med. 2020;383:994. [PMID: 32649078] doi:10.1056/NEJMc2022236 [DOI] [PubMed]
- 22. Horby P, Lim WS, Emberson JR, et al; RECOVERY Collaborative Group. Dexamethasone in hospitalized patients with COVID-19 - preliminary report. N Engl J Med. 2020. [PMID: 32678530] doi:10.1056/NEJMoa2021436 [DOI] [PMC free article] [PubMed]