

Abstract
Background Although patients who work and have related health issues are usually first seen in primary care, providers in these settings do not routinely ask questions about work. Guidelines to help manage such patients are rarely used in primary care. Electronic health record (EHR) systems with worker health clinical decision support (CDS) tools have potential for assisting these practices.
Objective This study aimed to identify the need for, and barriers and facilitators related to, implementation of CDS tools for the clinical management of working patients in a variety of primary care settings.
Methods We used a qualitative design that included analysis of interview transcripts and observational field notes from 10 clinics in five organizations.
Results We interviewed 83 providers, staff members, managers, informatics and information technology experts, and leaders and spent 35 hours observing. We identified eight themes in four categories related to CDS for worker health (operational issues, usefulness of proposed CDS, effort and time-related issues, and topic-specific issues). These categories were classified as facilitators or barriers to the use of the CDS tools. Facilitators related to operational issues include current technical feasibility and new work patterns associated with the coordinated care model. Facilitators concerning usefulness include users' need for awareness and evidence-based tools, appropriateness of the proposed CDS for their patients, and the benefits of population health data. Barriers that are effort-related include additional time this proposed CDS might take, and other pressing organizational priorities. Barriers that are topic-specific include sensitive issues related to health and work and the complexities of information about work.
Conclusion We discovered several themes not previously described that can guide future CDS development: technical feasibility of the proposed CDS within commercial EHRs, the sensitive nature of some CDS content, and the need to assist the entire health care team in managing worker health.
Keywords: attitude to computers, hospital information systems, physician order entry, clinical decision support, occupational health
Background and Significance
Although patients with medical issues, such as symptoms of asthma that may be caused by the work environment, are usually first seen by primary care providers (PCPs), these patients are not regularly asked about their work situations. 1 2 3 4 5 While occupational health specialists have developed evidence-based guidelines to manage such patients, PCPs are rarely aware of the existence of these guidelines. 6 Computerized clinical decision support (CDS) tools could be used to increase awareness and provide guidance, but they must be developed and implemented with care in conjunction with the users who would benefit from the CDS. 7
The aims of the parent project, funded by the National Institute for Occupational Safety and Health (NIOSH) of the Centers for Disease Control and Prevention (CDC), were to design, develop, and pilot CDS for improving the health of working patients in primary care settings. The parent study design phase included prior development of three knowledge resources (KRs) containing evidence-based information, decision logic, scenarios, and examples of use as step one. Step two was fieldwork to assess need and provide feedback, which is the focus of this paper.
In step one, the KR topics were carefully selected based on need expressed in an Institute of Medicine report. 8 The KRs were related to (1) work environment factors that impact the management of diabetes, (2) guidance for managing recommendations for returning to work after a low back pain diagnosis not related to work, and (3) the diagnosis and management of work-related asthma. These three topics were selected because they are related to the health of patients who work and are considered especially pertinent to primary care. 8 Please see Table 1 for summaries of the KRs.
Table 1. Summaries of the Knowledge Resources.
| Refractory diabetes |
|---|
| A diabetic patient's working conditions, such as working more or different hours or working in hot environments, can contribute to hyper- or hypoglycemic episodes. Also, for some “safety-sensitive” jobs, a worker with impairment of cognition due to low blood sugar could be at risk for injury to himself or to others. Triggered by an A1C level greater than 8 or a hypoglycemia diagnosis, the clinical decision support (CDS) would prompt providers to ask specific work-related questions and would generate educational information for the provider and patient based on the responses. |
| Return to work activity prescriptions for low–back pain |
| Some patients with low back pain (CDS trigger) and functional limitations may request their provider write a letter to their employer describing their limitations. The provider, based on both the patients’ reported function limitations (e.g., in a questionnaire) and the clinical assessment, chooses from four levels of recommended activity (sedentary, light, light-medium, medium). The system would guide the provider through generating a letter that specifies permitted activities based on which activity level was chosen and provides a date for elimination of activity restrictions. |
| Work-related asthma |
| Many cases of work-related asthma first present in a primary care setting and recognizing this connection is important to the success of the patient's management. The proposed CDS system would be triggered for adult patients with new onset or worsening asthma symptoms of less than 2 years of duration. The system would suggest the provider ask three questions about the relationship of the asthma symptoms to the patient's work. If the patient responds positively to any of these screening questions and the diagnosis of asthma is supported by spirometry results, the system would provide both clinician and patient information about work-related asthma. This information would help identify specific potential high-risk work exposures and referral resources. It would also prompt scheduling an extended visit to obtain work and exposure history and documentation in the EHR of the discussion. |
The KRs follow the Guideline Elements Model (GEM) 9 for translating specific guidelines into a computable format that an information system designer could adapt into their local information system. Each KR was prepared by a subject matter expert (SME) group guided by an informatician (R.N.S.) with expertise in GEM. Each consists of computable decision rules, along with evidence-based supporting information, scenarios, and examples of use. Creation of computable decision rules was aided by BRIDGE-Wiz 10 software. Details of the development of the KRs and their contents have been described elsewhere. 11 12 13 14 15
The primary care context within which the CDS described in the KRs would be implemented was expected to impact its usefulness and primary care was not represented in the SME groups that developed the KRs. Therefore, we designed a field study in primary care clinics to gain a picture of the environment and to assess the need.
Objectives
The goals of this qualitative study were to (1) evaluate the need for CDS for the clinical management of working patients in a variety of primary care settings, (2) investigate the barriers and facilitators related to implementation and use of the proposed CDS tools, and (3) assess the technical and organizational feasibility of implementing the CDS represented by each KR.
Methods
This study was approved by the NIOSH and Oregon Health & Science University's (OHSU) Institutional Review Boards (IRBs) and each relevant human subjects review panel at the study sites. For sites that did not have IRBs, we received permission from relevant committees designated by the sites.
Study Design
We selected the Rapid Assessment Process (RAP) 16 17 18 19 as our methodological approach, both because it was feasible within the time frame and is rigorous. We followed generally accepted strategies for assuring trustworthiness, including triangulation, member checking, audit tracking, reflexivity, and saturation. 18 Interdisciplinary team members, several of whom had used RAP for numerous other projects, were trained prior to fieldwork. Five organizations were selected as sites based on variability of geography, type of health care organization (providing varied patient demographics), and size. Ten clinics within those organizations served as observation sites because they offered primary care services to socioeconomically diverse groups of patients. Patients were selected based on role for interviewing and availability for observing. We developed and tested semistructured interview guides. To gain a sense of clinic workflow, we also shadowed staff members, as well as clinicians, including providers, nurses, and pharmacists, as they worked.
Setting
The research sites included: two federally qualified health centers (FQHC), both using the NextGen (Irvine, CA) EHR, located in California and Mississippi; two large integrated health systems, one in New York and one in Ohio, using Allscripts (Chicago, IL) and Epic (Verona, WI) EHRs, respectively; and one smaller integrated health system in Massachusetts using Epic. Although we did not deliberately select sites with clinics that had been designated as patient-centered medical homes (PCMHs), it turned out that all five settings included them, though not all of the specific clinics we studied were in that category.
Sample Selection
We asked a local investigator at each site, who also helped with human subjects approval and arrangements, to identify interviewees based on role (providers and other clinicians, medical assistants, information technology personnel, informaticians, managers, and quality improvement staff), and to arrange for observations throughout the clinics. Providers were also selected to represent a broad range of EHR users, from champions to skeptics.
Data Collection
The research team consisted of social scientists, clinicians, an information technology (IT) specialist, informaticians, and NIOSH staff. In part 1 of each interview, subjects were asked several questions (see Table 2 for a summary of topic areas) to elicit general views about CDS. In part 2, they were queried about descriptions of hypothetical CDS tools developed based on the KRs. 20 21 We have previously published a detailed description of the interview process, along with sample interview guides including questions for both parts of the interviews. 20
Table 2. Topics in interview guides.
| 1. Clinical interviewee question areas |
| Background and role of interviewee |
| Your work patterns |
| About CDS |
| About CDS for worker health |
| The three knowledge resources: how useful, who should be involved in asking questions and educating, and where each fits workflow; rank and discuss |
| 2. Informatics and IT question areas |
| Background and role of interviewee |
| Clinician work patterns and clinic workflows |
| About your EHR |
| About training, support, and customization |
| About CDS |
| About CDS for worker health |
| The three knowledge resources: how useful, who should be involved in asking questions and educating, and where each fits workflow; rank and discuss; technical feasibility |
| 3. Management and staff question areas |
| Background and role of interviewee |
| Your work patterns |
| About CDS |
| About worker health CDS |
| The three knowledge resources: how useful, who should be involved in asking questions and educating, and where each fits workflow; rank and discuss; technical feasibility |
Source: Used with permission from Clinical Decision Support for Worker Health Qualitative Study Final Report to NIOSH. Submitted by Ash JS, Baron S, Chase D, Filios M, Luensman G, Marovich S, Murphy E, McCormack J, Shiffman RN, Wiesen J. October, 2016. Produced under contract 200–2015-M-61837 for CDC/NIOSH.
Abbreviations: CDS, clinical decision support; EHR, electronic health record; IT, information technology.
Summaries and flow diagrams of the KRs were shared with interviewees during part 2 when appropriate. For example, IT experts were especially interested in the flow diagrams. Interviews were recorded and later transcribed. All interviewees were formally consented.
We shadowed clinicians and other personnel interacting with the EHR and office management systems during their work. Subjects who agreed to be shadowed were formally consented. Researchers then unobtrusively observed subjects for periods from 30 minutes to 2 hours at various times during clinic hours, depending on the subject's availability. Field notes were subsequently expanded and typed within days.
Data Analysis
Transcripts and field notes were entered into NVivo (QSR International, Doncaster, Victoria, Australia). We used both grounded hermeneutic and template approaches to data analysis. 22 23 Six team members broke into static dyads and each dyad read all documents. The first dyad coded data using a high-level template after each site visit to obtain initial results prior to the next site visit and wrote preliminary reports to the SMEs. The second dyad used an open grounded approach, developing codes directly from the part-1 data and building themes. The third dyad analyzed comments in the part-2 interview data about each KR summary and used both a predefined template and open coding. The team met frequently to discuss and agree on themes.
Results
Data Gathered
We conducted five site visits between July 21 and September 11, 2015. We interviewed 41 clinicians (physicians, nurses, pharmacists, etc.), not deeply involved in informatics, 23 individuals who were primarily informaticians or information technology specialists, 15 managers or staff members in differing roles, and 4 quality improvement specialists, for a total of 83 interviewees ( Tables 3 and 4 ). We spent 35 person-hours observing in 10 locations within the five organizations. Analysis of data pertaining to the three KRs gathered during graphic elicitation interviews 20 yielded valuable content and context-related information which subsequently led to revision of the KRs by the expert groups.
Table 3. Site information and data gathered.
| Organization | A | B | C | D | E | Total |
|---|---|---|---|---|---|---|
| Location | California | Mississippi | Massachusetts | New York | Ohio | |
| Setting | Federally qualified health center | Academic and community outpatient | ||||
| System | NextGen | Epic | Allscripts | Epic | ||
| Date of visit | 7/21–22 | 7/22–23 | 8/18–19 | 8/20–21 | 9/9–11 | |
| Hours observing | 8 | 3 | 6 | 8 | 10 | 35 |
| No. clinic locations observed | 2 | 10 | ||||
| No. interviews and patients | 12 interviews 12 patients |
11 interviews 16 patients |
18 interviews 17 patients |
15 interviews 15 patients |
22 interviews 23 patients |
78 interviews 83 patients |
Table 4. Number and role of subjects at each site.
| Organization | A | B | C | D | E | Total |
|---|---|---|---|---|---|---|
| Clinicians | 7 | 5 | 9 | 7 | 9 | 41 |
| Clinical informatics and Information technology | 3 | 5 | 9 | 23 | ||
| Management and staff | 5 | 3 | 2 | 3 | 4 | 15 |
| Quality improvement | 1 | 0 | 1 | 4 | ||
| Total interview patients | 12 | 16 | 17 | 15 | 23 | 83 |
Facilitators, Barriers, and Themes
We identified eight themes ( Fig. 1 ) during our needs assessment process. The themes explore the need for the CDS described in the KRs, and the feasibility of implementing the CDS as described. They naturally grouped into four major categories of barriers and facilitators. Below we discuss each of the themes, found at all sites, and provide representative, especially succinct, quotes for each. For a list of themes and a more complete list of representative quotes, see Supplementary Appendices A and B (available in the online version).
Fig. 1.
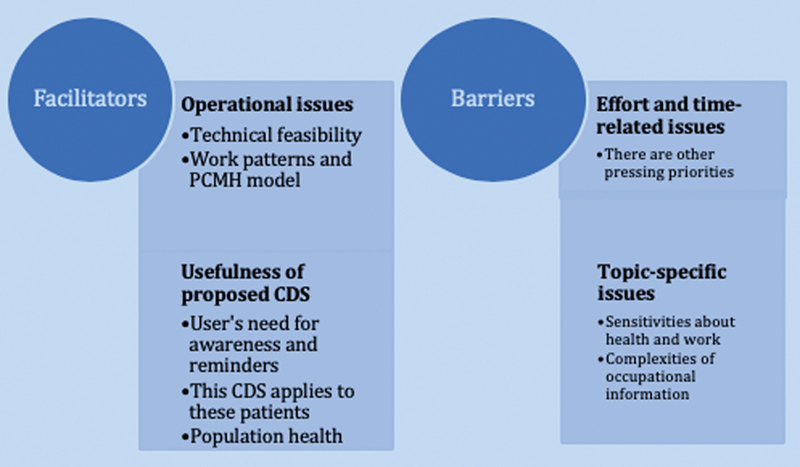
Facilitators and barriers to worker health CDS.
Facilitators
Operational Issues
Technical Feasibility
Although the sites had widely varying levels of experience with CDS, all had the technical expertise to put into machine executable form the three KRs without assistance from their vendors. The ability to build CDS tools in-house is important because, as we were told by an IT staff member, “it's going to cost” to have it built by the vendor unless the vendor decides to provide it for all customers. A CDS analyst is essential, according to interviewees, and all sites had at least a part-time person in this role. Most vendors supply development tools for the use of local analysts. IT staff at all sites felt that, if analysts are given the information in the KR describing the content about asthma, back pain, and diabetes, the CDS could be built on site. In fact, interviewees felt they were underutilizing the CDS development capabilities offered by their EHRs: “they (the vendor) gave us the keys to the kingdom, and if you have the resources, you can set it up to make it bark and rollover and do whatever you want it to.”
Many interviewees suggested that patients themselves should enter the data that would screen for information and trigger the CDS when we asked who should be doing this. They suggested this be done through patient portals, which all sites had available. Implementation of a portal is one of the recommended options for PCMH designation, consistent with the PCMH emphasis on patient involvement. The sites varied considerably in the extent to which patient portals were used and the degree of integration with the EHR. Some sites were just beginning to use a portal, but one site already had patients filling out questionnaires on tablet computers in the waiting room, sometimes aided by staff.
As designed, the logic to trigger each CDS to fire was not based on a patient's job information. Information in EHRs about jobs is not regularly updated, a finding which was confirmed during our site visits, and was an unstructured field in the majority of EHR systems. The diabetes KR uses A1C level as a trigger; the asthma KR uses recent onset; the return to work KR uses a complaint of low back pain. However, even though the CDS modules we described were not triggered by work information interviewees were quick to spontaneously point out that patients could be routinely entering job information themselves, so that it is always up to date ( Fig. 1 ).
Work Patterns, the Patient-Centered Medical Home Model, and Roles Involved
All of these organizations had work patterns into which the decision support could fit at appropriate times without disrupting provider workflow. Interviewees described how the PCMH model is different from traditional models, and we noted these differences while observing. We were told that, because of the team orientation of PCMH activities, the CDS should target the team, not just the provider.
Usefulness of the Proposed Clinical Decision Support
Users' Need for Awareness, Reminders, and Evidence
Some nonprovider interviewees noted that they had never considered asking patients about their jobs. One said the diabetes KR summary appealed to her “because I've worked with diabetics so long, and I never thought about their occupation.”
Even providers who did indicate that they often considered this relationship said they would like to be reminded about it. Guidance about how to question patients would be especially helpful for new or unfamiliar patients. Interestingly, during our many hours of observing, we rarely heard the topics of occupation or jobs discussed by patients and their providers.
Many clinicians expressed the desire for truly evidence-based clinical decision support. Several interviewees involved with quality improvement or management thought that the proposed CDS would be useful for standardizing clinical practice.
The Three Knowledge Resource Topics are Relevant in These Settings
For all of these organizations, diabetes in particular was a common diagnosis in their patient populations. About work and diabetes one provider said: “I have patients doing day shift and then they do a graveyard and then go home and rest for a couple of hours and they do babysitting stuff,” which makes managing diabetes difficult.
Each of the five sites serves diverse populations of patients. We asked each interviewee to give us examples of instances where knowing a patient's job could help in patient care. In California, they described housecleaners and warehouse workers who were exposed to airborne pollutants and heat. The staff in Mississippi told us about casino workers in smoke-filled environments and fishermen and oil-rig workers exposed to flesh-eating bacteria. Interviewees in Massachusetts often described job exposure to lead paint. In Ohio and New York, we heard about a broad mix of blue-collar workers' health risks. The latter sites also served white-collar workers, with carpal tunnel syndrome often mentioned, but interviewees noted that it is the blue-collar workers most at risk. Several interviewees emphasized that their most vulnerable populations would receive the greatest benefit from our proposed CDS.
Population Health and Registries
Interviewees often noted that information about patients' work would be helpful for triggering CDS and also for searching registries, so it would serve two purposes. Because of their emphasis on integrated care, all of our sites used registries for identifying high risk or targeted patients. For example, a diabetes care manager could query a registry to find high-risk patients who needed to be reminded to make an appointment. Some used third-party population analytics software that somewhat integrates with their EHR (some information could go back and forth between systems), one used a third-party product that could be accessed from within the EHR, and one directly used its EHR, which had recently developed a more robust analytics capability. The registries were used for writing reports, to plan individual care, and to meet requirements for quality and funding purposes, in addition to risk identification. Many interviewees spontaneously raised the idea of including information about patient occupations in registries. One interviewee suggested that a registry might be searched to find patients with lung problems to find those who might have recently taken on new jobs that could have exacerbated symptoms. As much as they were looking forward to using population data, however, they also expressed frustrations with the present state: “the quality of the data and the skills of the people who have to get the data out are both problematic.”
Barriers
Effort- and Time-Related Issues
Interviewees consistently noted that our proposed CDS might add to their time burdens or to that of others in their clinics. As is the case with most organizations, some of these sites had received complaints from users about the number of alerts causing alert fatigue. When we asked users what CDS they most appreciated, they said it was reminders and information resources. They were willing to take the time to seek out these resources if they were in the EHR, easily found, up to date, and evidence based. They wanted CDS that would be well worth their time. For example, many interviewees noted that the CDS that would help to generate a letter about returning to work after a low back pain diagnosis might offer them extremely useful guidance, so they reacted positively to it ( Fig. 1 ).
Other Pressing Organizational Priorities
Interviewees told us that their organizations were so burdened by responding to other needs such as PCMH designation at the time of our study that they were just “struggling to get the basics working.” When asked about other priorities, one IT manager said “well, first priority is how it's affecting billing.” Efficiency was offered as another priority: “and then it would be, you know, how can we streamline the process?”
Topic-Specific Issues
Sensitivities about Worker Health and a Sense of Powerlessness
Within all organizations, we heard that asking questions related to worker health is challenging. Such questions could raise issues of workers' compensation. These clinics had difficulty, or no capability for, filing workers' compensation claims that can be administratively challenging and time consuming for clinicians. Several do not have occupational health services to which patients can be referred. Patients might not be working and may not want to discuss work. Others are working two or three jobs in unpleasant circumstances that they do not want to talk about because they perceive that asking for changes at work would lead to retaliation. Raising work-related issues during a patient encounter, we were told, could present a barrier to provider–patient communications. A manager said “there can be sensitivity around asking about the workplace” because these patients have no choice about their jobs and job conditions.
Complexities of Occupational Information
While the three proposed CDS approaches we were describing that do not require the collection of information about work to use as a trigger, many of our more technical and managerial interviewees wanted to talk about capturing job information in a more structured way. Because gathering information about occupation is required or recommended for PCMH designation by different entities, it is collected by all of our sites, usually as free text or through a limited drop-down menu, but not in a fashion that is clinically useful. We asked everyone to describe when in the workflow this type of information is collected, and the question elicited complaints, both about putting the information in and getting it out. Information about a patient's employer is usually in the system because it relates to insurance, but interviewees sometimes questioned the usefulness of information about occupation, industry, or job title for clinical purposes. Some respondents said that knowing high level information like occupation or industry is most useful: “being a fisherman … we really have to watch out for, because we have had patients with significant issues, and especially with the flesh-eating bacteria that can progress really rapidly.” Others said they need to know the tasks done by a patient at work, and often learning the patient's occupation does not offer that level of detail. Regardless, we were told that if the information about work could be entered easily in a structured way, the information could potentially be used for CDS.
On the other hand, there is considerable distrust about structured data about occupations. There was quite a difference in the way providers reacted to our questions about the need for worker health CDS and the way nonproviders reacted. When providers talked about themselves personally, they usually said that they seek information about a patient's work activities when they need it and they prefer asking about it themselves. They indicated that they do not trust the information they might find in structured fields in the EHR, no matter how it got there. We were told repeatedly that patients change jobs often or describe an occupation they no longer have, or have several jobs and only describe one. Providers said that they trust their own notes or those of a team member, such as a care coordinator, but not entries in fields for demographic information.
There were also issues with the input of work information and the retrieval of it. When we asked providers if, when they discovered that the patient had a new job, they would enter that information into a structured field in addition to their note, they said no, that would take too much time. We most often received the same answer from other team members, who noted they keep their notes up to date in this respect but did not have time to update other areas of the EHR. We were also consistently told that even if they wanted to retrieve information on a patient's job, it would be too hard and take too much time. Many interviewees had given up looking for occupational information. One interviewee told us that she had stopped using the drop-down list when she once searched for “nurse” and found nothing.
Discussion
We identified eight themes in four categories related to how to enable CDS in EHRs to use work information about patients in a meaningful way, as well as barriers and challenges. While some themes we found were similar to those described in prior studies, others were new and unexpected and likely they reflect changes precipitated by newer models of care.
Facilitators
Of the facilitators listed in Fig. 1 , technical feasibility is immensely important. We expected to discover that users would express a need for the proposed CDS, especially if it were evidence based. This is consistent with what others have found. 24 25 We also expected there to be interest in population health, since health care is moving toward value-based care creating greater interest in data analytics to improve management of the health of their patient population. 26 We did not expect there would be such interest across all clinic sizes, however. With this selection of sites, the interest in population health is likely tied to their status as PCMHs required to identify high-risk patients and report on numerous measures.
Barriers
On the barrier side, we fully expected to hear that any CDS that might take additional time and cognitive effort on the part of providers would be unpopular. This is consistent with prior work. 27 28 Interviewees thought nonproviders should receive the CDS, but it needs to be noninvasive because of their time burden. We suspected that there would be competing priorities in health care organizations. Conveniently, one of their competing priorities, the “journey,” as several patients called it, toward fully implementing the PCMH model, can actually become a facilitator for implementing the CDS we are proposing because a PCMH must collect extensive data about its patients, so data to trigger CDS then becomes more available.
A barrier that has been described in the occupational health literature, the sensitivities about work and health, has not been discussed in the primary care or informatics literature, yet recognition of it by these disciplines could lead to better provider–patient communications.
Past studies have reported underutilization of workers' compensation insurance by injured workers, 29 fear of divulging PTSD symptoms by police after September 11, 30 patients' fear of retaliation after reporting work-related exacerbation of asthma, 31 and reluctance by coal miners to participate in a program to identify and track the progress of lung disease. 32 Investigating and developing CDS to help manage discussions about this and similar sensitive issues could help guide development of the most effective CDS for this purpose.
Several patients expressed frustration that a useful list of occupations was not available in their EHR systems. NIOSH has since developed occupational data for health (ODH) which includes an information model, vocabularies, data sharing standards, and a functional profile to guide collection and use of information related to work in EHRs. The vocabularies for data elements including occupation and industry are available in the Public Health Information Network Vocabulary Access and Distribution System (PHIN VADS). 33 They can be used to provide accessible choices for patients to identify their jobs. A work and health functional profile provides guidance for EHR vendors on the use of elements in ODH. 34 ODH provides an approach that can be adopted across commercial EHR systems to capture consistent, structured information about work.
Unexpected Results
What we also did not expect to discover was that experts at all of our sites, regardless of the vendor they used, were confident that the three proposed CDS KRs could be transformed into CDS tools by in-house staff members. Prior studies 35 led us to believe this would be difficult, but the provision of new tools by vendors made it possible for the participating sites. Tools from vendors for CDS modification and development must be used by trained on-site analysts, however, thus organizations must be willing to invest in the right people and train them to use the tools. 36
Another surprise facilitator was the uniform recommendation that our proposed CDS should not necessarily be targeting providers. Past literature notes that as the primary decision maker, the provider is usually the target. 27 However, there is recent recognition that with continued development of team medicine, different members of the care team, including the patient, could receive different notifications through the CDS. 37 The patient, as a member of the team, could not only enter data needed to trigger the CDS, but might also be a receiver of a reminder, for example. It appears that the PCMH model needs CDS and also can facilitate the usefulness of CDS by incorporating CDS into a team-based approach rather than one aimed solely at the provider.
Our results imply that commercial EHR vendors are increasingly providing needed tools for both CDS development and population health and that newer models of care such as the PCMH can benefit from a team-based approach to CDS. The results also point to the need for future research about terminologies representing occupations, CDS for sensitive topics, and CDS that might increase rather than decrease efficiency. In addition, further study is needed to determine the standardized data and tools needed to support widespread adoption beyond the types of sites selected in this study.
Based on what we learned in the field, we believe that CDS to improve the health of workers is technically feasible and can be customized within different EHR products using tools already available. The three KRs would provide information participants feel is important and useful, but the CDS should involve other team members in addition to providers to limit the time demands on providers and to achieve more coordinated care.
Limitations
This study had some limitations. As a qualitative study, this investigation produced rich, in-depth knowledge about five sites and three proposed CDS tools. It is possible that these sites are not truly representative. Though we did not seek out PCMH sites, all five fit this category, so our results may apply more specifically to organizations using this model of care. We did purposive sampling, so we approached the clinics and they needed to agree to participate. Given that they knew we were researching work-related CDS, clinics that had an interest and a need in this area were more likely to participate. Though we prefer conducting interviews with one person at a time, so we can discover individual perspectives, at times we had to interview two together because of their schedules. Interviewers may have differed in their interview styles and perspectives, but an assistant interviewer was always present to ask follow-up questions. The topics of the three KRs may be such that findings about them may not be generalizable to other occupational CDS. Three of our five sites used the same EHR product and all implementations differ, so generalizability of our results is limited, as it is with any qualitative study. Finally, data gathering began several years ago, so it is possible the technology has changed somewhat since then. Regardless, there remains a need for this type of CDS in primary care and the topics addressed by the KRs remain relevant.
Conclusion
Our aim was to identify the need for, and barriers and facilitators related to, implementation of CDS tools for the clinical management of working patients in a variety of primary care settings.
We identified themes representing both barriers and facilitators that can be considered as CDS is further developed and implemented. Some of these factors are similar to those discovered in prior CDS research. Others, such as changing work patterns and roles due to the PCMH model, and the sensitivities and complexities of work-related information are novel and deserve further investigation.
Clinical Relevance Statement
Individuals who are designing and implementing CDS might use our descriptions of barriers and facilitators when attempting to optimize successful use of CDS. Our discussion of themes could assist organizational decision makers in primary care settings in understanding issues related to both CDS and worker health.
Multiple Choice Questions
1. The authors of this paper found that commercial EHRs
Already provide useful data about the work of patients.
Are capable of incorporating the proposed CDS.
Do not provide CDS.
Are not useful for diabetes management.
Correct Answer: The correct answer is option b. The commercial EHR vendors provide tools so that trained staff at local sites can develop certain types of CDS for use by that site.
2. CDS for worker health could be useful because:
Primary care providers do not always take into account what patients do for a living and how that might influence their health.
Hazards like flesh eating bacteria cannot be identified without CDS.
Workers are always eager to talk about their jobs.
Providers always ask about work, so the data are available in the system.
Correct Answer: The correct answer is option a. Primary care providers rarely ask patients what they do for a living, yet while they are at work they might be exposed to health risks.
Acknowledgments
We appreciate the help of the following at our sites: Rose H. Goldman, MD, MPH, Laura Brightman, MD; Stacey Curry, MPH, Larry J. Knight, MSA, MSHRM; Deborah Lerner, MD; Michael Rabovsky, MD; Joseph Conigliaro, MD, MPH, and Nicole Donoghue, MPH. This paper is based in part on our final report to NIOSH 21 that included preliminary results. The tables and themes have been revised and are described here with permission.
Funding Statement
Funding This project was supported by CDC/NIOSH Contract 200–2015–61837 as part of NORA project no.: 927ZLDN. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Conflict of Interest None declared.
Protection of Human and Animal Subjects
This study was approved by the Institutional Review Boards (IRBs) at NIOSH, Oregon Health & Science University (OHSU), and two of our study sites. IRB waivers and/or official determinations (if a site did not have an IRB, it had other mechanisms for reviewing our protocol) were also obtained from the other three sites.
Supplementary Material
References
- 1.Goldman R H, Peters J M. The occupational and environmental health history. JAMA. 1981;246(24):2831–2836. [PubMed] [Google Scholar]
- 2.Shofer S, Haus B M, Kuschner W G. Quality of occupational history assessments in working age adults with newly diagnosed asthma. Chest. 2006;130(02):455–462. doi: 10.1378/chest.130.2.455. [DOI] [PubMed] [Google Scholar]
- 3.Politi B J, Arena V C, Schwerha J, Sussman N. Occupational medical history taking: how are today's physicians doing? A cross-sectional investigation of the frequency of occupational history taking by physicians in a major US teaching center. J Occup Environ Med. 2004;46(06):550–555. doi: 10.1097/01.jom.0000128153.79025.e4. [DOI] [PubMed] [Google Scholar]
- 4.Mazurek J M, Storey E. Physician-patient communication regarding asthma and work. Am J Prev Med. 2012;43(01):72–75. doi: 10.1016/j.amepre.2012.03.021. [DOI] [PubMed] [Google Scholar]
- 5.Mazurek J M, White G E, Moorman J E, Storey E. Patient-physician communication about work-related asthma: what we do and do not know. Ann Allergy Asthma Immunol. 2015;114(02):97–102. doi: 10.1016/j.anai.2014.10.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Newman L S. Occupational illness. N Engl J Med. 1995;333(17):1128–1134. doi: 10.1056/NEJM199510263331707. [DOI] [PubMed] [Google Scholar]
- 7.Lomotan E A, Hoeksema L J, Edmonds D E, Ramírez-Garnica G, Shiffman R N, Horwitz L I. Evaluating the use of a computerized clinical decision support system for asthma by pediatric pulmonologists. Int J Med Inform. 2012;81(03):157–165. doi: 10.1016/j.ijmedinf.2011.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wegman D H, Liverman C T, Schultz A M, Strawbridge L M. Institute of Medicine . Washington, DC: the Academic Press; 2011. Incorporating occupational information in electronic health records: Letter report. [Google Scholar]
- 9.Shiffman R N, Michel G, Essaihi A, Thornquist E. Bridging the guideline implementation gap: a systematic, document-centered approach to guideline implementation. J Am Med Inform Assoc. 2004;11(05):418–426. doi: 10.1197/jamia.M1444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Shiffman R N, Michel G, Rosenfeld R M, Davidson C. Building better guidelines with BRIDGE-Wiz: development and evaluation of a software assistant to promote clarity, transparency, and implementability. J Am Med Inform Assoc. 2012;19(01):94–101. doi: 10.1136/amiajnl-2011-000172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Filios M S, Storey E, Baron S, Luensman G B, Shiffman R N. Enhancing worker health through clinical decision support (CDS): An introduction to a compilation. J Occup Environ Med. 2017;59(11):e227–e230. doi: 10.1097/JOM.0000000000001179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Baron S, Filios M S, Marovich S, Chase D, Ash J S. Recognition of the relationship between patients' work and health: A qualitative evaluation of the need for clinical decision support for worker health I five primary care practices. J Occup Environ Med. 2017;59(11):e245–e250. doi: 10.1097/JOM.0000000000001183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Harber P, Redlich C A, Hines S, Filios M S, Storey E. Recommendations for a clinical decision support system for work related asthma in primary care settings. J Occup Environ Med. 2017;59(11):e231–e235. doi: 10.1097/JOM.0000000000001182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Allen A, Welch L, Kirkland K, Trout D, Baron S. Development of a diabetes mellitus knowledge resource for clinical decision support— assisting primary care physicians with work-related issues. J Occup Environ Med. 2017;59(11):e236–e239. doi: 10.1097/JOM.0000000000001181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McLellan R K, Haas N S, Kownacki R P, Pransky G S, Talmage J B, Dreger M. Using electronic health records and clinical decision support to provide return-to-work guidance for primary care practitioners for patients with low back pain. J Occup Environ Med. 2017;59(11):e240–e244. doi: 10.1097/JOM.0000000000001180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ash J S, Sittig D F, McMullen C K. Studying the vendor perspective on clinical decision support. AMIA Annu Symp Proc. 2011;2011:80–87. [PMC free article] [PubMed] [Google Scholar]
- 17.Beebe J. Walnut Creek, CA: Alta Mira Press; 2001. Rapid Assessment Process: An Introduction. [Google Scholar]
- 18.McMullen C K, Ash J S, Sittig D F. Rapid assessment of clinical information systems in the healthcare setting: an efficient method for time-pressed evaluation. Methods Inf Med. 2011;50(04):299–307. doi: 10.3414/ME10-01-0042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ash J S, Sittig D F, McMullen C K, Guappone K, Dykstra R, Carpenter J. A rapid assessment process for clinical informatics interventions. AMIA Annu Symp Proc. 2008;2008:26–30. [PMC free article] [PubMed] [Google Scholar]
- 20.Ash J S, Chase D, Wiesen J F, Murphy E V, Marovich S. Studying readiness for clinical decision support using the rapid assessment process and mixed methods interviews. AMIA Annu Symp Proc. 2017;2016:285–294. [PMC free article] [PubMed] [Google Scholar]
- 21.Ash J S, Baron S, Chase D, Filios M, Luensman G, Marovich S, Murphy E, McCormack J, Shiffman R N, Wiesen J. Clinical Decision Support for Worker Health Qualitative Study Final Report to NIOSH. 2016.
- 22.Crabtree B F, Miller W L. Thousand Oaks, CA: Sage Publications; 1999. Doing Qualitative Research. 2nd ed. [Google Scholar]
- 23.Berg B L, Lune H. Boston, MA: Pearson; 2012. Qualitative Research Methods for the Social Sciences. 8th ed. [Google Scholar]
- 24.Mellis C. Evidence-based medicine: what has happened in the past 50 years? J Paediatr Child Health. 2015;51(01):65–68. doi: 10.1111/jpc.12800. [DOI] [PubMed] [Google Scholar]
- 25.Lulin Z, Yiranbon E, Asante Antwi H. Complementarity of clinician judgement and evidence based models in medical decision making: antecedents, prospects, and challenges. BioMed Res Int. 2016;2016:1.425693E6. doi: 10.1155/2016/1425693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Schaeffer C, Booton L, Halleck J, Studeny J, Coustasse A. Big data management in U.S. hospitals. Health Care Manag (Frederick) 2017;36(01):87–95. doi: 10.1097/HCM.0000000000000139. [DOI] [PubMed] [Google Scholar]
- 27.Kilsdonk E, Peute L WP, Knijnenburg S L, Jaspers M WM. Factors known to influence acceptance of clinical decision support systems. Stud Health Technol Inform. 2011;169:150–154. [PubMed] [Google Scholar]
- 28.Mamykina L, Vawdrey D K, Hripcsak G. How do residents spend their shift time? A time and motion study with a particular focus on the use of computers. Acad Med. 2016;91(06):827–832. doi: 10.1097/ACM.0000000000001148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Azaroff L S, Davis L K, Naparstek R, Hashimoto D, Laing J R, Wegman D H. Barriers to use of workers' compensation for patient care at Massachusetts community health centers. Health Serv Res. 2013;48(04):1375–1392. doi: 10.1111/1475-6773.12045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schwarzer R, Cone J E, Li J, Bowler R M. A PTSD symptoms trajectory mediates between exposure levels and emotional support in police responders to 9/11: a growth curve analysis. BMC Psychiatry. 2016;16:201. doi: 10.1186/s12888-016-0907-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Harris D A, Mainardi A, Iyamu O. Improving the asthma disparity gap with legal advocacy? A qualitative study of patient-identified challenges to improve social and environmental factors that contribute to poorly controlled asthma. J Asthma. 2018;55(08):924–932. doi: 10.1080/02770903.2017.1373393. [DOI] [PubMed] [Google Scholar]
- 32.Laney A S, Blackley D J, Halldin C N. Radiographic disease progression in contemporary US coal miners with progressive massive fibrosis. Occup Environ Med. 2017;74(07):517–520. doi: 10.1136/oemed-2016-104249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Centers for Disease Control and Prevention. Public Health Information Network Vocabulary Access and Distribution System (PHIN VADS) Accessed September 3, 2019 athttps://www.cdc.gov/phin/tools/phinvads/
- 34.HL7 EHRS-FM Release 2 Functional Profile: Work and Health, Release 1, U.S. Realm Accessed September 3, 2019 at:http://www.hl7.org/implement/standards/product_brief.cfm?product_id=498
- 35.Wright A, Sittig D F, Ash J S, Sharma S, Pang J E, Middleton B. Clinical decision support capabilities of commercially-available clinical information systems. J Am Med Inform Assoc. 2009;16(05):637–644. doi: 10.1197/jamia.M3111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wright A, Ash J S, Erickson J L. A qualitative study of the activities performed by people involved in clinical decision support: recommended practices for success. J Am Med Inform Assoc. 2014;21(03):464–472. doi: 10.1136/amiajnl-2013-001771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Revere D, Hills R H, Dixon B E, Gibson P J, Grannis S J. Notifiable condition reporting practices: implications for public health agency participation in a health information exchange. BMC Public Health. 2017;17(01):247. doi: 10.1186/s12889-017-4156-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.