

Abstract
Objective
This study aimed to appraise the efficacy and safety of the tonifying-Shen (kidney) principle (TS (TK) principle) for primary osteoporosis (POP).
Methods
Randomized controlled clinical trials (RCTs) using the TS (TK) principle for POP were searched from eight electronic databases to search for relevant literature that was published from the initiation to September 2019. Two reviewers performed study selection, data extraction, data synthesis, and quality assessment independently. Review Manager 5.3 software was used to assess the risk of bias and conduct the data synthesis. We assessed the quality of evidence for outcomes by using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system.
Results
Thirty-six studies with 3617 participants were included. Meta-analysis showed a consistently superior effect of the TS (TK) principle combined with conventional Western medicine (CWM) in terms of total effectiveness rates (RR = 1.28; 95% CI (1.23, 1.33); P < 0.00001), BMD of the lumbar spine (SMD = 0.71; 95% CI (0.47, 0.95); P < 0.00001) and proximal femur (SMD = 0.94; 95% CI (0.49, 1.38); P < 0.00001), TCM symptom integral (SMD = −1.23; 95% CI (−1.43, −1.02); P < 0.00001), and VAS scores (SMD = −3.88; 95% CI (−5.29, −2.46); P < 0.00001), when compared to using CWM alone and with significant differences. Besides, in respect of adverse effects, it showed no significant statistical difference between the experimental and control groups, RR = 0.99 and 95% CI (0.65, 1.51), P=0.97.
Conclusion
Our meta-analysis provides promising evidence to suggest that using the TS (TK) principle combined with CWM for POP is more effective than using CWM alone. Also, both of them are safe and reliable for POP.
1. Introduction
Primary osteoporosis (POP), also called “a silent disease,” is one of the pandemic public health issues that seriously threaten people's health all over the world [1]. Theoretically, POP and secondary osteoporosis belong to the field of osteoporosis (OP). POP includes two major types: postmenopausal osteoporosis (PMOP) and age-related or senile osteoporosis [2]. POP is characterized by decreased bone mass and degenerated bone microstructure, which contributes to a high risk of bone fragility and fracture [3, 4]. It is estimated that the number of individuals aged 50 years or over at high risk of osteoporotic fracture worldwide was at 158 million in 2010 and is set to double by 2040 [5]. In China, because of the largest population and the increasing proportion of elderly people, osteoporosis has become a severe challenge to the Chinese family, society, and government [6, 7]. Therefore, an effective prevention and treatment method is urgently needed for POP. Management of POP includes nonpharmacologic treatment and pharmacologic treatment. Conventional Western medicines (CWM) including antiresorptive or anabolic are widely used in the treatment of POP [8–10]. However, due to adverse effects and risk of cancer, the use of CWM as long-term treatment is limited [11].
It is well documented that traditional Chinese medicine (TCM) is commonly combined with pharmacotherapy for POP in China [12–14]. In the theory of TCM, there is no particular disease named POP. According to the clinical symptoms, POP belongs to the TCM category of “Guwei (flaccidity of bones),” “Guku (dryness of bones),” “Guji (disease of bones),” “Gukong (depletion of bones), and Gubi (impediment of bones)” [15]. “Shen (kidney) dominating the bone” is the most fundamental theory in TCM. Shen essence (kidney essence) is closely related to bone physiology and pathology. The sufficient Shen essence can keep the bone healthy and strong. On the contrary, the deficiency of Shen essence will lead to a series of bone-related symptoms. Besides, “liver controlling tendon,” is involved in bone health. Also, the spleen and stomach are considered as the postnatal foundations of organisms and are the material sources of bone growth. Therefore, the tonifying-Shen (kidney) principle (TS (TK) principle) mainly includes bushen huoxue, bushen zhuanggu, bushen jianpi, and buyi ganshen, which are widely used in combination with other TCM therapies or CWM for the treatment of POP. And, this significant principle has its essential meaning in curing POP [16].
In recent years, numerous meta-analyses were carried out to investigate the efficacy of acupuncture or Chinese herbal medicine for POP [17]. However, there was still no sufficient evidence to draw definitive conclusions as most studies were not comparative analysis aiming at the effect of the TS (TK) principle for POP. Besides, most of the meta-analyses did not explore the safety of particular interventions. Therefore, the purpose of this study was to systematically identify available randomized clinical trials (RCTs) using the TS (TK) principle combined with CWM for POP to appraise its efficacy and safety.
2. Materials and Methods
2.1. Study Registration
The study has been registered in PROSPERO (registration number: CRD42020151768). The review reporting was conducted in compliance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement guidelines.
2.2. Study Design
2.2.1. Inclusion Criteria
(1) Types of Participants and Interventions. All RCTs that were reporting the application of the TS (TK) principle combined with CWM for POP were included. The interventions of these studies must include the TS (TK) principle in the experimental group. Studies must be published in English or Chinese language. TS (TK) principle mainly includes bushen huoxue, bushen zhuanggu, bushen jianpi, and buyi ganshen. Specific treatment methods include traditional Chinese herbal medicine, acupuncture and moxibustion combined with traditional Chinese herbal medicine, acupoint catgut embedding, and acupoint injection. POP patients were included. There is no restriction on gender, race, ethnicity, or nation. Patients in the treatment group were given the TS (TK) principle combined with CWM, while patients in the control group were given CWM alone. The dosages and courses were not limited in our studies.
(2) Types of Outcome Measures. The primary outcomes included effectiveness rate and bone mineral density (BMD) of the lumbar spine and proximal femur (femoral neck or total hip). The secondary outcomes consisted of VAS scores and TCM symptom integral. Besides, adverse events were also assessed as a safety measurement.
2.2.2. Exclusion Criteria
Studies with the following characteristics were excluded: irrelevant to TS (TK) principle studies; studies without consistent diagnostic criteria or relevant outcome indicators; non-English or Chinese-language articles; duplicate reports or the data cannot be extracted; case reports, animal experiences, qualitative studies, comments, or review articles.
2.3. Literature Search Strategy
We searched four international electronic databases (PubMed, Cochrane Library, EMBASE, and Web of Science) and four Chinese electronic databases (CNKI, VIP, Wanfang, and CBM) from their initiation to September 2019 to collect for relevant literature. The literature search was constructed around search terms for TS (TK) principle, POP, and randomized controlled trials and adapted for each database as necessary. The references of the included studies were also screened for further material for inclusion. The detailed search strategy for PubMed is in Table 1. Search strategies were also used for other electronic databases.
Table 1.
The search strategy used in the PubMed database.
| Serial number | Search items |
|---|---|
| #1 | Bushen |
| #2 | Tonifying Shen |
| #3 | Bu Shen |
| #4 | Yishen |
| #5 | Nourishing the kidney |
| #6 | Tonifying the kidney |
| #7 | Yi Shen |
| #8 | Tonifying kidney |
| #9 | Nourishing kidney |
| #10 | Nourishing Shen |
| #11 | Reinforcing the kidney |
| #12 | Reinforcing kidney |
| #13 | Reinforcing Shen |
| #14 | Invigorating the kidney |
| #15 | Invigorating kidney |
| #16 | Invigorating Shen |
| #17 | Kidney-reinforcing |
| #18 | Kidney reinforcing |
| #19 | Shen reinforcing |
| #20 | Shen-reinforcing |
| #21 | Kidney-invigorating |
| #22 | Kidney invigorating |
| #23 | Shen-invigorating |
| #24 | Kidney-tonifying |
| #25 | Shen-tonifying |
| #26 | Kidney tonifying |
| #27 | Shen tonifying |
| #28 | Shen invigorating |
| #29 | Invigorating Shen |
| #30 | #1 or #2—#29 |
| #31 | Primary osteoporosis |
| #32 | Osteoporosis |
| #33 | Age-related osteoporosis |
| #34 | Age-related osteoporosis |
| #35 | Osteoporosis, senile |
| #36 | Osteoporosis, involutional |
| #37 | Senile osteoporosis |
| #38 | Osteoporosis, age-related |
| #39 | Osteoporosis, age-related |
| #40 | Bone loss, age-related |
| #41 | Age-related bone loss |
| #42 | Age-related bone losses |
| #43 | Bone loss, age-related |
| #44 | Bone losses, age-related |
| #45 | #31 or #32—#44 |
| #46 | Randomized controlled trials |
| #47 | Randomized |
| #48 | Randomly |
| #49 | Random |
| #50 | RCTs |
| #51 | #46 or #47—#50 |
| #52 | #30 and #45 and #51 |
2.4. Study Selection and Data Extraction
As a first step in the data handling process, titles and abstracts of all studies retrieved by the search strategies were screened for relevance, and all those that were clearly irrelevant have been discarded.
As a second step, two review team members (Junquan Liang and Fengyi Wang) independently assessed the eligibility of the studies by using the predefined inclusion and exclusion criteria. Besides, for the studies that meet the inclusion criteria, the whole article was read by reviewers to ensure that the entire study met the criteria and was prepared to extract relevant information. The disagreements on whether including a specific study or not were resolved by discussion between the reviewers. The lacking information was requested by contacting the writer of the original article.
The information extracted by the two independent review team members included the following: study setting, population study, participant demographics and baseline characteristics, details of the intervention and control conditions, study methodology, outcomes and treatment periods, information for the assessment of the risk of bias. The discrepancies were identified and resolved through discussion (with a third author where necessary). Missing data were requested from the study authors.
2.5. Risk of Bias Assessment
There were two reviewers involved in the quality assessment process, and any major disagreements were resolved by discussion to define the final set of included studies.
Two independent reviewers assessed the risk of bias by considering the following characteristics: randomization sequence generation, treatment allocation concealment, blinding method, completeness of outcome data, selective outcome reporting, and other sources of bias. Besides, the Cochrane Collaboration's risk of bias assessment tool was used to assess the quality of the individual included studies.
2.6. Data Synthesis
Review Manager 5.3 software was used to carry out the quantitative synthesis. Mean difference (MD) or standardized mean difference (SMD) was used for continuous data. Risk ratio (RR) was used for the analysis of dichotomous data. Both were given a 95% confidence interval (CI). In the case of homogeneous data (I2 ≤ 50%, P > 0.10), the fixed-effect model was adopted for the meta-analysis. Otherwise, the sources of heterogeneity were further analyzed. After excluding the influence of marked clinical heterogeneity, a random-effect model was adopted to perform the meta-analysis. Sensitivity and bias risk analyses were also performed.
2.6.1. Analysis of Subgroups
We performed some planned subgroup analysis: different specific therapies (bushen huoxue, bushen zhuanggu, bushen jianpi, and buyi ganshen) included in the TS (TK) principle, different kinds of treatment methods (traditional Chinese herbal medicine, acupuncture and moxibustion combined with traditional Chinese herbal medicine, acupoint catgut embedding, and acupoint injection), different parts of BMD examination (lumbar spine and proximal femur (femoral neck or total hip)), and different treatment periods of the TS (TK) principle (≤3 months, 3–6 months, and >6 months).
2.6.2. Sensitivity Analysis and Reporting Bias Analysis
Sensitivity analysis was carried out to identify the robustness and stability of pooled outcome results by removing the low-quality studies. We have performed a funnel plot of the primary outcome (effectiveness rates of different treatment methods included in the tonifying-Shen (kidney) principle) to evaluate the reporting bias.
2.7. Quality of Evidence
We assessed the quality of evidence for outcomes by using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system [18].
3. Results
3.1. Study Description and Participants
We obtained 390 relevant studies through preliminary searches. After multiple filtering steps, 36 RCTs with a total of 3617 participants were ultimately included in this systematic review. The flowchart of all study selection procedures is shown in Figure 1.
Figure 1.
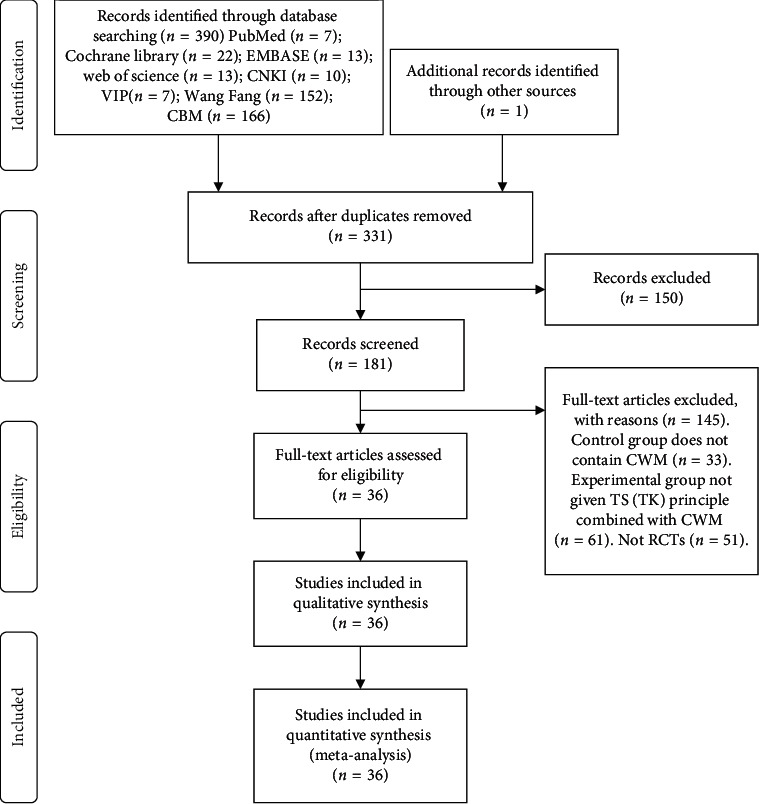
The flowchart of the selection procedure.
The 36 included studies involved 3617 participants. Among these studies, apart from combined with CWM, 23 studies reported using TCM herbal medicine [19–41], 5 studies reported using acupuncture and moxibustion combined with traditional Chinese herbal medicine [42–46], 9 studies reported using acupoint catgut embedding [25, 26, 40, 47–52], and 2 studies reported using acupoint injection [53, 54]. Besides, 3 studies divided their experimental group into two groups, respectively (acupoint catgut embedding group and TCM herbal medicine group) [25, 26, 40]. The detailed characteristics of the included studies are shown in Table 2.
Table 2.
Characteristics of the included studies.
| No. | Included studies (author, year) | Age (years) | Participants (experimental group/control group) | Intervention | Outcomes | Adverse effects (experimental group/control) | Treatment periods (months) | Follow-up (months) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Control group | Experimental group | Control group | Experimental group | Secondary outcomes | Primary outcomes | ||||||
| 1 | Zheng et al. [19], 2019 | 63.9 ± 2.81 | 63.91 ± 2.86 | 70/70 | Placebo capsules ± calcium carbonate | Bushen Yijing Fang ± calcium carbonate | — | BMD of femoral neck; adverse effects | 9/8 | 36 | 120 |
| 2 | Liu and Wang [42], 2016 | 56.15 ± 6.77 | 55.86 ± 6.92 | 62/62 | Alendronate sodium tablets ± calcium carbonate D3 tablets | Erxian Bushen decoction ± acupuncture and moxibustion ± alendronate sodium tablets ± calcium carbonate D3 tablets | — | Effectiveness rate; BMD of femoral neck and lumbar spine | — | 6 | — |
| 3 | Xu et al. [43], 2018 | 63.90 ± 7.59 | 65.16 ± 6.82 | 32/31 | Calcium carbonate D3 | Thunder-fire moxibustion ± calcium carbonate D3 | VAS scores | — | — | 1 | 1 |
| 4 | Zhu et al. [20], 2012 | 64.9 ± 6.0 | 65.4 ± 6.3 | 61/61 | Calcium carbonate ± vitamin D | Xian Ling Gu Bao capsules ± calcium carbonate ± vitamin D | — | BMD of femoral neck and lumbar spine; adverse effects | 11/11 | 12 | 12 |
| 5 | Zhao and Yan [21], 2018 | 61.3 ± 4.1 | 62.1 ± 4.1 | 50/50 | Caltrate ± alpha D3 calciferol | Traditional Chinese medicine prescription ± caltrate ± alpha D3 calciferol | VAS scores | Effectiveness rate; BMD of lumbar spine (L2–4); adverse effects | 9/6 | 6 | 6 |
| 6 | Yuan et al. [22], 2014 | — | — | 40/40 | Alendronate ± calcium carbonate D3 | Chinese herbal medicine ± alendronate ± calcium carbonate D3 | — | Effectiveness rate | — | 6 | — |
| 7 | Huang [23], 2015 | 65.5 ± 1.6 | 65.7 ± 1.5 | 70/70 | Calcium carbonate D3 ± alfacalcidol soft capsules | Bushenhuoxuetang ± calcium carbonate D3 ± alfacalcidol soft capsules | VAS scores | Effectiveness rate | — | 2 | — |
| 8 | Wu et al. [24], 2005 | 56.4 ± 4.6 | 55.6 ± 4.3 | 34/34 | Caltrate D600 | Xian Ling Gu Bao capsules ± caltrate D600 | — | BMD of femoral neck and lumbar spine | — | 12 | — |
| 9 | Liu et al. [25], 2011 (3) | 62.8 ± 5.9 | Liu 2011 (3)∗: 63.7 ± 3.8; Liu 2011 (3): 61.8 ± 8.3 | A: 35/35; B: 35 | Calcichew D3 tablets | Liu 2011 (3)∗: acupoint catgut embedding ± calcichew D3 tablets; Liu 2011 (3): Xianling Gubao capsules ± calcichew D3 tablets | VAS scores | Effectiveness rate; BMD of lumbar spine | — | 6 | — |
| 10 | Lu [47], 2014 | 62.14 ± 6.34 | 60.84 ± 6.95 | 25/22 | Calcium carbonate D3 | Acupoint catgut embedding ± calcium carbonate D3 | — | Effectiveness rate | — | 6 | — |
| 11 | Han et al. [44], 2011 | 67.39 ± 4. 05 | 67.42 ± 3. 89 | 30/30 | Caltrate | Shuganwenshentanyushuangjietang ± acupuncture and moxibustion ± caltrate | — | Effectiveness rate | — | 6 | — |
| 12 | Liu et al. [26], 2011 (1) | 62.8 ± 5.9 | Liu 2011 (1)∗: 63.7 ± 3.8; Liu 2011 (1): 61.8 ± 8.3 | A: 35/35 B: 35 | Calcichew D3 tablets | Liu 2011 (1)∗: acupoint catgut embedding ± calcichew D3 tablets; Liu 2011 (1): Xian Ling Gu Bao capsules ± calcichew D3 tablets | TCM symptom integral | — | 0/0/4 | 6 | — |
| 13 | Peng et al. [48], 2017 | — | — | 35/35 | Calcichew D3 tablets ± alendronate sodium tablets | Acupoint catgut embedding ± calcichew D3 tablets ± alendronate sodium tablets | VAS scores | Effectiveness rate; BMD of lumbar spine | — | 3 | — |
| 14 | Peng et al. [49], 2018 | — | — | 45/45 | Calcichew D3 tablets ± alendronate sodium tablets | Acupoint catgut embedding ± calcichew D3 tablets ± alendronate sodium tablets | VAS scores | Effectiveness rate; BMD of lumbar spine | — | 3 | 3 |
| 15 | Zhong et al. [50], 2018 | — | — | 45/45 | Calcichew D3 tablets ± alendronate sodium tablets | Acupoint catgut embedding ± calcichew D3 tablets ± alendronate sodium tablets | VAS scores | Effectiveness rate; BMD of lumbar spine | — | 3 | — |
| 16 | Zou et al. [53], 2018 | 66.73 ± 3.71 | 66.27 ± 3.18 | 60/60 | Caltrate D tablets ± alendronate sodium tablets ± calcitriol soft capsules | Acupoint injection ± caltrate D tablets ± alendronate sodium tablets ± calcitriol soft capsules | — | Effectiveness rate; BMD of femoral neck and lumbar spine; adverse effects | 0/0 | 6 | — |
| 17 | Ma and Fan [45], 2018 | 68.43 ± 3.68 | 68.56 ± 3.79 | 42/42 | Calcium carbonate ± vitamin D tablets | Bushenzhuanggutang ± acupuncture and moxibustion ± calcium carbonate ± vitamin D tablets | — | Effectiveness rate | — | 3 | 12 |
| 18 | Lin [51], 2006 (1) | — | — | 24/22 | Osteoform capsules | Acupoint catgut embedding ± osteoform capsules | — | BMD of femoral neck | — | 6 | — |
| 19 | Lin [52], 2006 (2) | — | — | 20/18 | Osteoform capsules | Acupoint catgut embedding ± osteoform capsules | — | BMD of femoral neck | — | 6 | — |
| 20 | Qi [27], 2016 | 75.42 ± 6.83 | 76.5 ± 7.28 | 100/100 | Caltrate D | Bushenqianggufang ± caltrate D | — | Effectiveness rate; BMD of femoral neck and lumbar spine | — | 3 | 3 |
| 21 | Li et al. [28], 2017 | 75.4 ± 4.9 | 72.6 ± 5.5 | 30/30 | Calcitriol soft capsules ± caltrate D600 | Bushenjianpitang ± calcitriol soft capsules ± caltrate D600 | — | Effectiveness rate | — | 3 | — |
| 22 | Hu and Li [29], 2012 | — | — | 155/145 | Caltrate D ± miacalcic | Shangkeyishenjianguwan ± caltrate D ± miacalcic | — | BMD of lumbar spine | — | 3 | 6 |
| 23 | Liu and Gong [30], 2018 | 59.88 ± 7.46 | 60.49 ± 7.25 | 38/38 | Calcitriol soft capsules ± calcium carbonate D3 ± alendronate sodium tablets | Bushenjianpihuoxuefang ± calcitriol soft capsules ± calcium carbonate D3 ± alendronate sodium tablets | — | Effectiveness rate; BMD of femoral neck and lumbar spine; adverse effects | 6/4 | 6 | — |
| 24 | Chen et al. [31], 2017 | 66.22 ± 11.3 | 65.12 ± 12.41 | 32/28 | Salmon calcitonin | Bushenjiangufang ± salmon calcitonin | VAS scores | Effectiveness rate | — | 6 | — |
| 25 | Zou [32], 2016 | — | — | 31/31 | Alendronate sodium tablets ± calcichew D3 tablets | Bushenjiangutang ± alendronate sodium tablets ± calcichew D3 tablets | — | BMD of femoral neck and lumbar spine | — | 6 | — |
| 26 | Han [33], 2013 | 55.32 ± 1.53 | 54.08 ± 3.26 | 28/28 | Alfacalcidol soft capsules ± caltrate | Bushenzhuanggutang ± alfacalcidol soft capsules ± caltrate | — | Effectiveness rate; adverse effects | 0/0 | 2 | — |
| 27 | Huang et al. [34], 2018 | — | — | 88/88 | Alendronate sodium tablets | Bushentang ± alendronate sodium tablets | VAS scores | Effectiveness rate; BMD of femoral neck and lumbar spine; adverse effects | 0/0 | 6 | — |
| 28 | Huang et al. [35], 2017 | /— | — | 46/46 | Salmon calcitonin | Bushenhuoxuefang ± salmon calcitonin | — | BMD of femoral neck and lumbar spine | — | 6 | — |
| 29 | Song et al. [36], 2015 | 76.1 ± 3.78 | 76.4 ± 3.56 | 90/90 | Salmon calcitonin | Bushenhuoxuefang ± salmon calcitonin | — | Effectiveness rate; adverse effects | 0/0 | 12 | — |
| 30 | Pan and Ding [37], 2014 | 57. 2 ± 11. 2 | 56. 9 ± 11. 0 | 43/43 | Oyster shell calcium capsules | Bushenhuoxuefang ± oyster shell calcium capsules | — | Effectiveness rate; BMD of femoral neck and lumbar spine; adverse effects | 0/4 | 3 | — |
| 31 | Wang [38], 2018 | 62.25 ± 5.01 | 62.18 ± 4.58 | 100/100 | Calcium carbonate and vitamin D3 tablets | Bushenhuoxuetang ± calcium carbonate and vitamin D3 tablets | — | Effectiveness rate; BMD of lumbar spine | — | 3 | — |
| 32 | Gui et al. [39], 2017 | 66.28 ± 8.17 | 66.19 ± 8.34 | 30/30 | Alendronate sodium tablets ± caltrate D | Bushenyiqihuayutang ± alendronate sodium tablets ± caltrate D | — | Effectiveness rate; BMD of total hip and lumbar spine; adverse effects | 4 Feb | 6 | — |
| 33 | Liu et al. [40], 2011 (2) | 59.8 ± 8.6 | Liu 2011 (2)∗: 62.5 ± 9.7; Liu 2011 (2): 60.3 ± 10.2 | A: 45/45 B: 45 | Calcichew D3 tables | Liu 2011 (2)∗: acupoint catgut embedding ± calcichew D3 tables; Liu 2011 (2): Xian Ling Gu Bao capsules ± calcichew D3 tables | TCM symptom integral; VAS scores | Effectiveness rate; BMD of lumbar spine | — | 6 | — |
| 34 | Ouyang et al. [46], 2011 | 65.6 ± 6.6 | 64.4 ± 5.3 | 25/30 | Alendronate | Acupuncture and moxibustion ± alendronate | TCM symptom integral | BMD of lumbar spine and proximal femur | — | 6 | — |
| 35 | Zhou et al. [54], 2016 | 55 ± 4 | 56 ± 4 | 30/30 | Salmon calcitonin | Acupoint injection | TCM symptom integral | BMD of lumbar spine | — | 2 | — |
| 36 | Xie et al. [41], 2018 | 61.00 ± 3.12 | 59.40 ± 4.12 | 30/31 | Vitamin D chewable tablets ± calcitriol soft capsules | Gushenfang ± vitamin D chewable tablets ± calcitriol soft capsules | — | Effectiveness rate; adverse effects | 0/0 | 3 | — |
Notes: the experimental group of Liu 2011 (1) was divided into 2 groups, respectively: Liu 2011 (1) and Liu 2011 (1)∗; the experimental group of Liu 2011 (2) was divided into 2 groups, respectively: Liu 2011 (2) and Liu 2011 (2)∗; the experimental group of Liu 2011 (3) was divided into 2 groups, respectively: Liu 2011 (3) and Liu 2011 (3)∗. A: experimental group; B: control group.
3.2. Risk of Bias Assessment
We used the Cochrane Collaboration's risk of bias assessment tool to assess the quality of the included studies. Firstly, all studies reported the method of randomization, and 30 studies described the method of generating a randomization number table [19–30, 32, 34, 35, 37–42, 44, 46, 48–54]. The remaining methods to achieve the sequence generation process include the following: drawing opaque envelope randomly [43], using Doll's clinical case random table [47], drawing of lots, [36, 45], and tossing coins [31, 33]. Secondly, there were only 3 studies which achieved allocation concealment [19, 20, 43]. Thirdly, 3 studies were assessed as appropriate double-blinding of participants and provided detailed information for double-blinding during treatment as well as an outcome assessment [19, 20, 43]. None of the studies reported any incomplete outcome data (Table 3 and Figure 2).
Table 3.
Brief table of risk assessment.
| Risk of bias assessment (yes/no/unclear) | |||||||
|---|---|---|---|---|---|---|---|
| No. | Included studies (first author, year) | Random sequence generation | Allocation concealment | Blinding of participants, personnel, and outcome assessors | Incomplete outcome data | Selective outcome reporting | Other sources of bias |
| 1 | Zheng et al. [19], 2019 | Randomization number table | Yes | Yes | Yes | No | No |
| 2 | Liu and Wang [42], 2016 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 3 | Xu et al. [43], 2018 | Draw opaque envelope randomly | Yes | Yes | Yes | No | No |
| 4 | Zhu et al. [20], 2012 | Using a computer random number generator | Yes | Yes | Yes | No | No |
| 5 | Zhao et al. [21], 2018 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 6 | Yuan et al. [22], 2014 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 7 | Huang [23], 2015 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 8 | Wu et al. [24], 2005 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 9 | Liu et al. [25], 2011 (3) | Randomization number table | Unclear | Unclear | Yes | No | No |
| 10 | Lu [47], 2014 | Doll's clinical case random table | Unclear | Unclear | Yes | No | No |
| 11 | Han et al. [44], 2011 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 12 | Liu et al. [26], 2011 (1) | Randomization number table | Unclear | Unclear | Yes | No | No |
| 13 | Peng et al. [48], 2017 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 14 | Peng et al. [49], 2018 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 15 | Zhong et al. [50], 2018 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 16 | Zou et al. [53], 2018 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 17 | Ma et al. [45], 2018 | Drawing of lots | Unclear | Unclear | Yes | No | No |
| 18 | Lin [51], 2006 (1) | Randomization number table | Unclear | Unclear | Yes | No | No |
| 19 | Lin [52], 2006 (2) | Randomization number table | Unclear | Unclear | Yes | No | No |
| 20 | Qi [27], 2016 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 21 | Li et al. [28], 2017 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 22 | Hu and Li [29], 2012 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 23 | Liu and Gong [30], 2018 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 24 | Chen et al. [31], 2017 | Coin tossing | Unclear | Unclear | Yes | No | No |
| 25 | Zou [32], 2016 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 26 | Han [33], 2013 | Coin tossing | Unclear | Unclear | Yes | No | No |
| 27 | Huang et al. [34], 2018 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 28 | Huang et al. [35], 2017 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 29 | Song et al. [36], 2015 | Draw lots randomly | Unclear | Unclear | Yes | No | No |
| 30 | Pan and Ding [37], 2014 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 31 | Wang [38], 2018 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 32 | Gui et al. [39], 2017 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 33 | Liu et al. [40], 2011 (2) | Randomization number table | Unclear | Unclear | Yes | No | No |
| 34 | Ouyang et al. [46], 2011 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 35 | Zhou et al. [54], 2016 | Randomization number table | Unclear | Unclear | Yes | No | No |
| 36 | Xie et al. [41], 2018 | Randomization number table | Unclear | Unclear | Yes | No | No |
Figure 2.
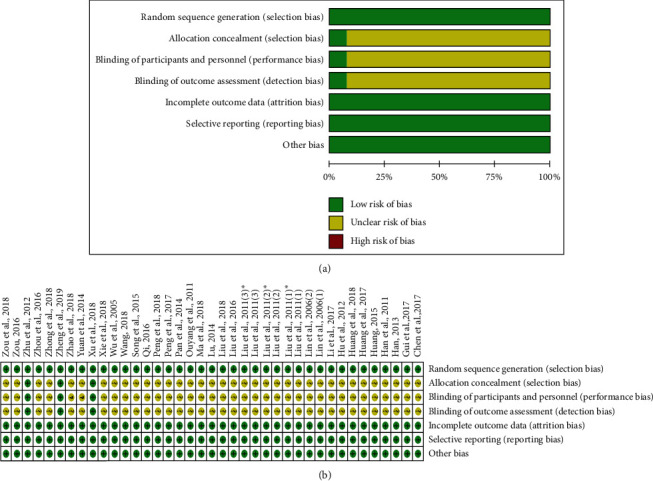
Risk of bias assessment. Notes: the experimental group of Liu 2011 (1) was divided into 2 groups, respectively: Liu 2011 (1) and Liu 2011 (1)∗; the experimental group of Liu 2011 (2) was divided into 2 groups, respectively: Liu 2011 (2) and Liu 2011 (2)∗; the experimental group of Liu 2011 (3) was divided into 2 groups, respectively: Liu 2011 (3) and Liu 2011 (3)∗.
3.3. Meta-Analysis
3.3.1. Effectiveness Rates of Different Treatment Methods Included in TS (TK) Principle
Twenty-five RCTs reported effectiveness rates of different treatment methods included in the TS (TK) principle [21–23, 25, 27, 28, 30, 31, 33, 34, 36–42, 44–50, 53]. Sixteen RCTs reported effectiveness rates of TCM herbal medicine [21–23, 25, 27, 28, 30, 31, 33, 34, 36–41], and there was low statistical heterogeneity among studies (chi2 = 19.09, P=0.21; I2 = 21%). Therefore, the fixed-effect model was applied to calculate the combined RR and 95% CI as 1.24 (1.19, 1.30), P < 0.00001, indicating a statistically significant difference between TCM herbal medicine combined with CWM and CWM alone. This result suggests that TCM herbal medicine combined with CWM in the treatment of POP can significantly improve clinical efficacy when compared with using CWM alone. Three studies reported effectiveness rates of acupuncture and moxibustion combined with TCM herbal medicine [42, 44, 45]. The result showed that there was no statistical heterogeneity among studies (chi2 = 3.94, P=0.14; I2 = 49%), so we adopted a fixed-effect model to calculate the combined RR and 95% CI as 1.34 (1.19, 1.51), P < 0.00001, indicating a statistically significant difference between the experimental group and the control group. This result suggests that, in respect of effectiveness rates, using acupuncture and moxibustion combined with TCM herbal medicine plus CWM for POP was better than using CWM alone. There are 6 studies which reported effectiveness rates of acupoint catgut embedding [25, 40, 47–50]. The heterogeneity was not detected among studies (chi2 = 4.53, P=0.48; I2 = 0%), so a fixed-effect model was used to calculate the combined RR and 95% CI as 1.42 (1.27, 1.58), P < 0.00001, indicating a statistically significant difference between acupoint catgut embedding combined with the CWM group and the CWM alone group. This result shows that the effectiveness rates of catgut embedding combined with CWM for POP were better than using CWM alone. There is only 1 study which reported effectiveness rates of acupoint injection [53]. The combined RR and 95% CI was 1.25 (1.05, 1.48), P < 0.00001, indicating the difference between acupoint injection combined with the CWM group and the CWM alone group. Owing to the small sample size, this result would show that the effectiveness rates of acupoint injection combined with CWM for POP were better than using CWM alone. All in all, the pooled data showed that different treatment methods included in the TS (TK) principle combined with CWM were more effective than using CWM alone in improving effectiveness rates, with significant differences (RR = 1.28; 95% CI (1.23, 1.33); P < 0.00001) (Figure 3(a)).
Figure 3.
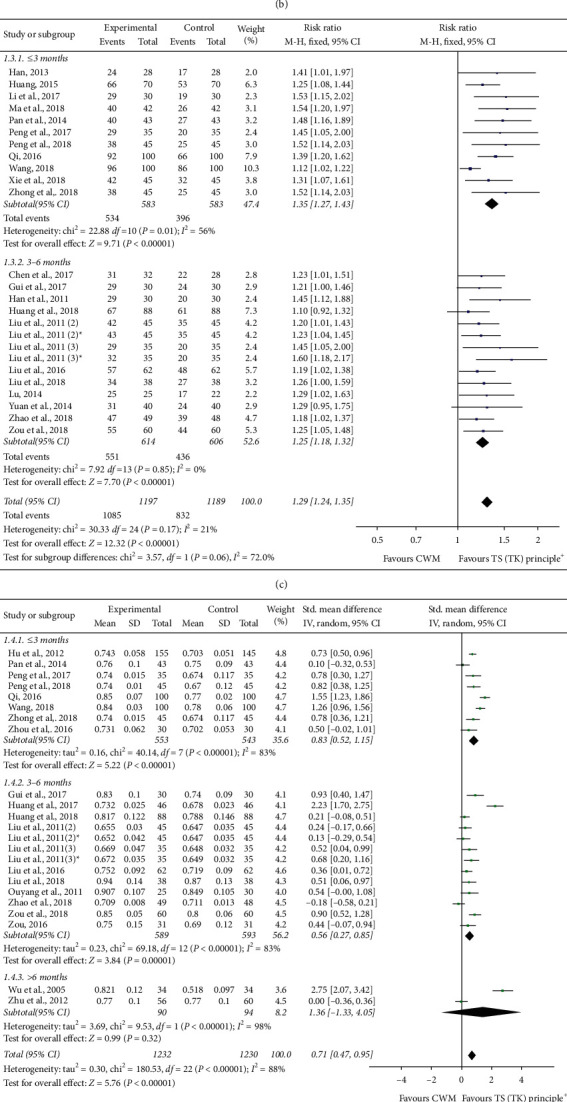
(a) Effectiveness rates of different treatment methods included in the TS (TK) principle. (b) Effectiveness rates of different specific therapies included in TCM herbal medicine. (c) Effectiveness rates of different treatment periods. (d) BMD (lumbar spine) of different treatment periods. (e) BMD (proximal femur (femoral neck or total hip)) of different treatment periods. (f) Adverse effects. (g) TCM symptom integral. (h) VAS scores. Notes: the experimental group of Liu 2011 (2) was divided into 2 groups, respectively: Liu 2011 (2) and Liu 2011 (2)∗; the experimental group of Liu 2011 (3) was divided into 2 groups, respectively: Liu 2011 (3) and Liu 2011 (3)∗.
3.3.2. Effectiveness Rates of Different Specific Therapies Included in TCM Herbal Medicine
There were 16 studies which reported effectiveness rates of different specific therapies included in TCM herbal medicine [21–23, 25, 27, 28, 30, 31, 33, 34, 36–41]. Five studies reported the effectiveness rates of bushen huoxue therapy [23, 36–39], three studies reported the effectiveness rates of bushen zhuanggu therapy [27, 31, 33], three studies reported the effectiveness rates of bushen jianpi therapy [22, 28, 30], and five studies reported the effectiveness rates of buyi ganshen therapy [21, 25, 34, 40, 41]. The heterogeneity among these studies was chi2 = 3.07, P=0.55; I2 = 0%, chi2 = 1.05, P=0.59; I2 = 0%, chi2 = 1.16, P=0.56; I2 = 0%, and chi2 = 3.02, P=0.55; I2 = 0%, respectively. Therefore, the fixed-effect model was applied to calculate the combined RR and 95% CI. After calculating, the combined RR and 95% CI was 1.18 (1.11, 1.24); P < 0.00001, 1.36 (1.21, 1.53); P < 0.00001, 1.34 (1.15, 1.57); P=0.0002, and 1.21 (1.11, 1.32); P < 0.00001, respectively, indicating a statistically significant difference between the experimental group and the control group. This result suggests that bushen huoxue, bushen zhuanggu, bushen jianpi, and buyi ganshen TCM herbal medicine combined with CWM in the treatment of POP can significantly improve clinical efficacy when compared with using CWM alone. The combined data showed that different specific therapies included in TCM herbal medicine combined with CWM were more effective than using CWM alone in improving effectiveness rates, with significant differences (RR = 1.23; 95% CI (1.18, 1.29); P < 0.00001) (Figure 3(b)).
3.3.3. Effectiveness Rates of Different Treatment Periods
Twenty-three literature studies reported effectiveness rates of different treatment periods [21–23, 26–28, 30, 31, 33, 34, 37–42, 44, 45, 47–50, 53]. Eleven literature studies reported treatment periods of less than 3 months [23, 27, 28, 37, 38, 41, 44, 45, 48–50]. However, there was high statistical heterogeneity among studies (chi2 = 22.88, P=0.01; I2 = 56%). A sensitivity analysis was performed to identify the source of heterogeneity. By removing one trial [38], no heterogeneity was detected (chi2 = 4.88, P=0.84; I2 = 0%). We confirmed the accuracy of the data without publication bias after contacting the author. So, we adopted a random-effect model to calculate the combined RR and 95% CI as 1.35 (1.27, 1.43), P < 0.00001, indicating a statistically significant difference between the TS (TK) principle combined with the CWM group and the CWM alone group. It is suggested that using the TS (TK) principle combined with CWM for POP was better than using CWM alone in improving effectiveness rates when the treatment periods were less than 3 months. Twelve literature studies reported treatment periods of three to six months [21, 22, 25, 30, 31, 34, 39, 40, 42, 44, 47, 53]. There was no statistical heterogeneity among studies (chi2 = 7.92, P=0.85; I2 = 0%). Therefore, the fixed-effect model was applied to calculate the combined RR and 95% CI as 1.25 (1.18, 1.32), P < 0.00001, indicating a statistically significant difference between the TS (TK) principle combined with the CWM group and the CWM alone group. It is suggested that using the TS (TK) principle combined with CWM for POP was better than using CWM alone in improving effectiveness rates when the treatment periods were three to six months. The pooled data showed that different treatment periods combined with CWM were more effective than using CWM alone in improving effectiveness rates, with significant differences (RR = 1.29; 95% CI (1.24, 1.35); P < 0.00001) (Figure 3(c)).
3.3.4. BMD (Lumbar Spine) of Different Treatment Periods
Twenty-one studies reported BMD (lumbar spine) of different treatment periods [20, 21, 24, 25, 27, 29, 30, 32, 34, 35, 37–40, 42, 46, 48–50, 53, 54]. There were 8 studies which reported BMD (lumbar spine) of less than 3 months [27, 29, 37, 38, 48–50, 54], and 11 studies reported BMD (lumbar spine) of three to six months [21, 25, 30, 32, 34, 35, 39, 40, 42, 46, 53]. However, we detected high statistical heterogeneity among studies, chi2 = 40.14, P < 0.00001; I2 = 83% and chi2 = 69.18, P < 0.00001; I2 = 83%. The source of heterogeneity may be related to different treatment methods. Therefore, we adopted the random-effect model, and meta-analysis showed that there was a significant difference between the experimental and control groups (SMD = 0.83; 95% CI (0.52, 1.15); P < 0.00001 and SMD = 0.56; 95% CI (0.27, 0.85); P < 0.00001). It is suggested that using the TS (TK) principle combined with CWM less than three months or three to six months can both improve the BMD of the lumbar spine and is better than using CWM alone. Two studies reported BMD (lumbar spine) of more than six months [20, 24], and there was high statistical heterogeneity among studies (chi2 = 49.53, P < 0.00001; I2 = 98%). We adopted the random-effect model, and meta-analysis showed that there was no significant difference between the experimental and control groups (SMD = 1.36; 95% CI (−1.33, 4.0); P=0.32). In general, the meta-analysis showed that different treatment periods combined with CWM were more effective than using CWM alone in improving the BMD of the lumbar spine, with significant differences (SMD = 0.71; 95% CI (0.47, 0.95); P < 0.00001) (Figure 3(d)).
3.3.5. BMD (Proximal Femur (Femoral Neck or Total Hip)) of Different Treatment Periods
There were 15 studies which reported BMD (proximal femur (femoral neck or total hip)) of different treatment periods [19, 20, 24, 27, 30, 32, 34, 35, 37, 39, 42, 46, 51–53]. Two studies reported BMD (proximal femur (femoral neck or total hip)) of less than 3 months [27, 37]. High statistical heterogeneity among studies was detected (chi2 = 10.41, P=0.001; I2 = 90%); therefore, we adopted the random-effect model, and meta-analysis showed that there was no significant difference between the experimental and control groups (SMD = 0.53; 95% CI (−0.30, 1.36); P=0.21). Ten studies reported BMD (proximal femur (femoral neck or total hip)) of three to six months [30, 32, 34, 35, 39, 42, 46, 51–53]. There was high statistical heterogeneity among studies (chi2 = 52.61, P < 0.00001; I2 = 83%). We performed sensitivity analysis by removing one trial [35], and low heterogeneity was detected (chi2 = 11.68, P=0.17; I2 = 32%). The source of heterogeneity may be related to different treatment methods. So, a random-effect model was adopted. The results showed that using the TS (TK) principle combined with CWM three to six months can improve the BMD of the proximal femur (femoral neck or total hip) and was better than using CWM alone (SMD = 0.69; 95% CI (0.34, 1.04); P < 0.00001). Three studies reported BMD of more than six months, and these showed that there was high heterogeneity (chi2 = 135.92, P < 0.00001; I2 = 99%) [19, 20, 24]. By removing one study [20], no heterogeneity was detected. The high heterogeneity may result from different treatment methods adopted by these studies. Thus, a random-effect model was adopted, and the results showed that there was no significant difference between the experimental and control groups (SMD = 2.06; 95% CI (0.36, 4.49); P=0.10). The combined data showed that different treatment periods combined with CWM were more effective than using CWM alone in improving the BMD of the proximal femur (femoral neck or total hip), with significant differences (SMD = 0.94; 95% CI (0.49, 1.38); P < 0.00001) (Figure 3(e)).
3.3.6. Adverse Effects
Eleven studies reported adverse effects [19–21, 30, 33, 34, 36, 37, 39, 41, 53], and there was no statistical heterogeneity among studies (chi2 = 4.07, P=0.54; I2 = 0%). Hence, the fixed-effect model was applied to calculate the combined RR and 95% CI as 0.99 (0.65, 1.51), P=0.97, indicating no statistically significant difference between the experimental group and the control group. This result suggests that the TS (TK) principle combined with CWM or using CWM alone in the treatment of POP are both safe. Besides, the common adverse effects in the experimental group were gastrointestinal complaints, liver enzyme abnormal, hypertension, joint pain, stomach discomfort, nausea, vomiting, headache, musculoskeletal pain, etc. The adverse effects in the control group included gastrointestinal complaints, liver enzyme abnormal, hypertension, nausea, and vomiting (Figure 3(f)).
3.3.7. TCM Symptom Integral
The TCM symptom integral was established according to the Clinical Research Guidance of New Chinese Herbal Medicine [55]. Four studies reported TCM symptom integral [26, 40, 46, 54], and there was low statistical heterogeneity among studies (chi2 = 7.49, P=0.19; I2 = 33%). Therefore, the fixed-effect model was applied. The meta-analysis showed that there was a statistically significant difference between the experimental group and the control group (SMD = −1.23; 95% CI (−1.43, −1.02); P < 0.00001). This result suggests that the TS (TK) principle combined with CWM in the treatment of POP can significantly improve TCM symptom integral when compared with using CWM alone (Figure 3(g)).
3.3.8. VAS Scores
There were 10 studies which reported VAS scores [21, 23, 25, 31, 34, 40, 43, 48–50]. The result showed that there was high statistical heterogeneity among studies (chi2 = 733.80, P < 0.00001; I2 = 99%), so we adopted a random-effect model. The combined data showed that there was a statistically significant difference between the experimental group and the control group (SMD = −3.88; 95% CI (−5.29, −2.46); P < 0.00001). This result suggests that the TS (TK) principle combined with CWM in the treatment of POP was more effective than using CWM alone in improving VAS scores (Figure 3(h)).
3.3.9. Publication Bias
The funnel plots were generated for studies with data on the effectiveness rates of different treatment methods included in the TS (TK) principle. The results showed that most of the points in the funnel plots were symmetrical. However, two points were outside the 95% CIs, which indicates that there may have been publication bias in our studies and that might influence the results of our analysis, as can be seen in Figure 4.
Figure 4.
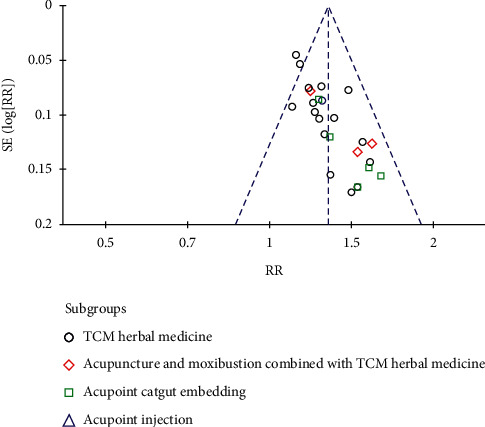
Funnel plot of effectiveness rates of different treatment methods included in the TS (TK) principle.
3.3.10. Quality of Evidence
There were 8 results for levels of evidence in our study. The detailed GRADE evidence profile of results is shown in Figure 5.
Figure 5.
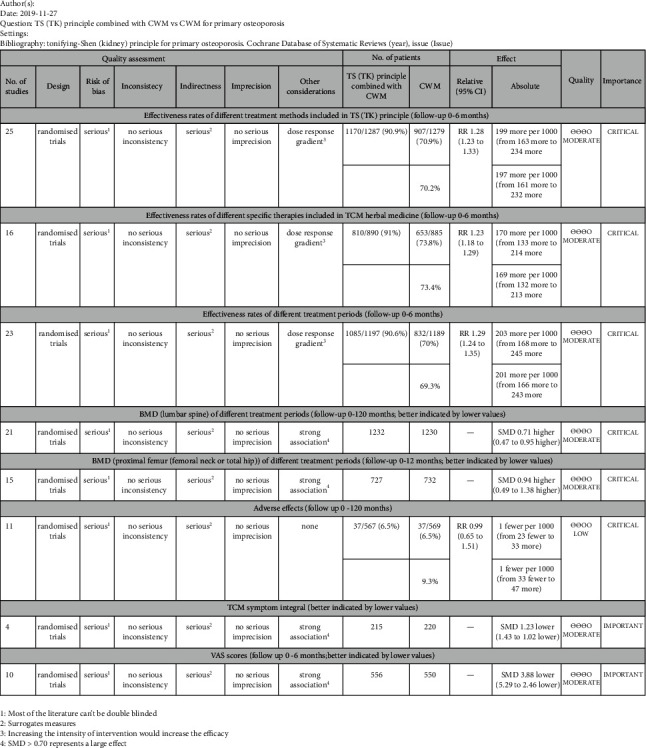
GRADE evidence profile.
4. Discussion
4.1. Summary of Main Results
There were 36 included RCTs with 3617 participants in our research. Even though most of the trials had small sample sizes and poor methodological quality, our meta-analysis reached the following results: (1) analysis of the pooled data showed a consistently superior effect of the TS (TK) principle combined with CWM in terms of total effectiveness rates, BMD of the lumbar spine and proximal femur (femoral neck or total hip), TCM symptom integral, and VAS scores when compared to using CWM alone; (2) in terms of adverse effects, the same safety was obtained for the TS (TK) principle combined with CWM or using CWM alone for POP; (3) different treatment methods included in the TS (TK) principle combined with CWM were more effective than using CWM alone in improving effectiveness rates. It should be noted that since the sample size of acupoint injection effectiveness rates was small, the combined RR and 95% CI was reported from the original study, not from the meta-analysis results; (4) in respect of TCM herbal medicine, different specific therapies combined with CWM for POP were more effective than using CWM alone; (5) compared with using CWM alone, the TS (TK) principle combined with CWM was more effective for POP in the aspect of different treatment periods; (6) in the three-to six-month treatment period, the TS (TK) principle combined with CWM for POP in terms of BMD of the lumbar spine and proximal femur (femoral neck or total hip) was better than using CWM alone; (7) according to the guideline of GRADE, the effectiveness rates of different treatment methods included in the TS (TK) principle, effectiveness rates of different specific therapies included in TCM herbal medicine, effectiveness rates of different treatment periods, BMD (lumbar spine) of different treatment periods, BMD (proximal femur (femoral neck or total hip)) of different treatment periods, TCM symptom integral, and VAS scores were moderate level of evidence. The adverse effects were low of evidence.
4.2. Analysis of TS (TK) Principle
TCM has been used in a range of medical management and health interventions in China and any other Asian countries for over 2500 years. POP patients are usually seeking TCM treatment, when the therapeutic effect of CWM is unsatisfactory. According to TCM theory, the establishment of a therapeutic principle is based on TCM syndromes, not symptoms. The clinical diagnosis of the TCM syndrome relies on the gathering of clinical information through inspection, auscultation and olfaction, inquiry, and palpation [56]. For POP, the fundamental physiopathological changes of the bone depend on whether Shen (kidney) essence is sufficient or not. Therefore, the TS (TK) principle is the key point to prevent and treat Shen (kidney)-deficiency syndrome of POP [57–60]. On the one hand, the effective mechanisms of pharmaceutical treatment included in the TS (TK) principle on POP have been demonstrated in the voluminous literature. Icariin (ICA), similar to estrogen, has a definite antiosteoporotic effect [61, 62]. Besides, oleanolic acid (OA) and psoralen have been reported to prevent bone loss by inhibiting osteoclast formation [63–65]. On the other hand, in respect of nonpharmaceutical treatment included in the TS (TK) principle, experiments have demonstrated that acupuncture could alleviate osteoporosis by regulating the expression of members in OPG/RANKL, Wnt/β-catenin, and MAPK pathways [66]. Acupoint catgut embedding could regulate the hypothalamic-pituitary-ovarian axis to raise the serum E2 level which would be significant in preventing osteoporosis [67]. Even experiments have shown that acupoint catgut embedding ameliorated the ovariectomization- (OVX-) caused metabonomic changes more effectively than hormone replacement therapy (HRT) with nilestriol [68]. Also, nonpharmaceutical treatment could alleviate related symptoms of osteoporosis and improve the quality of life [43]. Therefore, the TS (TK) principle would be a promising approach for POP, and it can not only improve physiological and biochemical indicators but also alleviate the TCM syndromes [16].
4.3. Limitations of Research
However, some limitations in our meta-analysis should be mentioned. (1) Although all of our included studies were RCTs, the methodological quality of them was generally improvable. Most of them failed to describe the blinding methods in detail, allocation, and concealment methods. (2) Among 36 studies, only 8 studies reported follow-up. The longest follow-up period was 120 months, and no further follow-up data were collected. The long-term effect of the TS (TK) principle for POP should be further studied. (3) For POP, fracture incidence should be the most patient-important outcomes. However, no fracture incidence data were collected in our studies. It is necessary to focus on fracture incidence as a patient-important outcome in further studies. (4) The studies included in this analysis were insufficient, especially in terms of subgroup analysis. Thus, potential publication bias probably exists. (5) The high heterogeneity among studies may be related to the different treatment methods, treatment periods, and even the skill level of the practitioners. It is a common problem in the research of TCM therapy. (6) The study for different specific therapies of TCM herbal medicine was insufficient, and further data mining should be carried out.
5. Conclusion
In summary, our meta-analysis suggests that using the TS (TK) principle combined with CWM for POP is effective and safe. However, the limitation in the quality and quantity of the included RCTs might weaken the overall reliability of this conclusion. Therefore, large-volume, well-designed RCTs with extensive follow-up are awaited to confirm and update the findings of this analysis.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant no. 81574064, Yunxiang Xu; 81473755, Guizhen Chen); the Shenzhen Science and Technology Planning Project (grant no. JCYJ20170306152650625); the Shenzhen Bao'an District TCM Hospital Research Program (no. BAZYY20200609).
Abbreviations
- POP:
Primary osteoporosis
- OP:
Osteoporosis
- PMOP:
Postmenopausal osteoporosis
- CWM:
Conventional Western medicines
- TCM:
Traditional Chinese Medicine
- TS (TK) principle:
Tonifying-Shen (kidney) principle
- RCTs:
Randomized clinical controlled trials
- BMD:
Bone mineral density
- VAS:
Visual analogue scale
- PRISMA:
Preferred reporting item for systematic review and meta-analysis
- CNKI:
China National Knowledge Infrastructure
- VIP:
Chinese Scientific Journal Database
- CBM:
China Biology Medicine
- MD:
Mean difference
- SMD:
Standardized mean difference
- RR:
Risk ratio
- 95% CI:
95% confidence interval
- GRADE:
Grading of Recommendations Assessment, Development, and Evaluation
- ICA:
Icariin
- OA:
Oleanolic acid
- OVX:
Ovariectomization
- HRT:
Hormone replacement therapy.
Contributor Information
Yunxiang Xu, Email: xuyx1968@163.com.
Guizhen Chen, Email: cgzhen2000@163.com.
Data Availability
The data used to support the findings of this study have been deposited in the following repository: PubMed: https://www.ncbi.nlm.nih.gov/pubmed/; Cochrane Library: https://www.cochranelibrary.com/; EMBASE: https://www.embase.com/; Web of Science: http://webofscience.com/; CNKI: https://www.cnki.net/; VIP: http://www.cqvip.com/; Wanfang: http://www.wanfangdata.com.cn/; CBM: http://www.sinomed.ac.cn/.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
Authors' Contributions
Junquan Liang, Guizhen Chen, and Yunxiang Xu conceptualized the study and were responsible for writing–review and editing. Yunxiang Xu and Junquan Liang curated the data. Junquan Liang and Fengyi Wang performed formal analysis and were responsible for methodology, resources, software, visualization, and writing–original draft. Guizhen Chen and Yunxiang Xu were responsible for project administration.
References
- 1.Wylie C. D. Setting a standard for a “silent” disease: defining osteoporosis in the 1980s and 1990s. Studies in History and Philosophy of Science Part C: Studies in History and Philosophy of Biological and Biomedical Sciences. 2010;41(4):376–385. doi: 10.1016/j.shpsc.2010.10.015. [DOI] [PubMed] [Google Scholar]
- 2.Orimo H., Sugioka Y., Fukunaga M., et al. Diagnostic criteria of primary osteoporosis. Journal of Bone and Mineral Metabolism. 1998;16(3):139–150. doi: 10.1007/s007740050038. [DOI] [Google Scholar]
- 3.Muto E. S., Adler R., Bilezikian J., et al. The clinical diagnosis of osteoporosis: a position statement from the national bone health alliance working group. Osteoporosis International. 2014;25(5):1439–1443. doi: 10.1007/s00198-014-2655-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bolognese F., Xia W. The epidemiology of osteoporosis, associated fragility fractures, and management gap in China. Arch Osteoporos. 2019;14(1):p. 32. doi: 10.1007/s11657-018-0549-y. [DOI] [PubMed] [Google Scholar]
- 5.Odén A., McCloskey E. V., Kanis J. A., Harvey N. C., Johansson H. Burden of high fracture probability worldwide: secular increases 2010–2040. Osteoporosis International. 2015;26(9):2243–2248. doi: 10.1007/s00198-015-3154-6. [DOI] [PubMed] [Google Scholar]
- 6.Yuan L.-Q., Lin X., Xiong D., et al. Epidemiology and management of osteoporosis in the People’s Republic of China: current perspectives. Clinical Interventions in Aging. 2015;10:1017–1033. doi: 10.2147/cia.s54613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wang Y., Tao Y., Hyman M. E., Li J., Chen Y. Osteoporosis in China. Osteoporosis International. 2009;20(10):1651–1662. doi: 10.1007/s00198-009-0925-y. [DOI] [PubMed] [Google Scholar]
- 8.Chandran T., Venkatachalam I. Efficacy and safety of denosumab compared to bisphosphonates in improving bone strength in postmenopausal osteoporosis: a systematic review. Singapore Medical Journal. 2019;60(7):364–378. doi: 10.11622/smedj.2019028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Berry S. D., Shi S., Kiel D. P. Considering the risks and benefits of osteoporosis treatment in older adults. JAMA Internal Medicine. 2019;179(8):1103–1104. doi: 10.1001/jamainternmed.2019.0688. [DOI] [PubMed] [Google Scholar]
- 10.Black D. M., Rosen C. J. Postmenopausal osteoporosis. New England Journal of Medicine. 2016;374(3):254–262. doi: 10.1056/nejmcp1513724. [DOI] [PubMed] [Google Scholar]
- 11.Skjødt M. K., Frost M., Abrahamsen B. Side effects of drugs for osteoporosis and metastatic bone disease. British Journal of Clinical Pharmacology. 2019;85(6):1063–1071. doi: 10.1111/bcp.13759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zeng Q., Li N., Wang Q., et al. The prevalence of osteoporosis in china, a nationwide, multicenter DXA survey. Journal of Bone and Mineral Research. 2019;34(10):1789–1797. doi: 10.1002/jbmr.3757. [DOI] [PubMed] [Google Scholar]
- 13.Leung P.-C., Siu W.-S. Herbal treatment for osteoporosis: a current review. Journal of Traditional and Complementary Medicine. 2013;3(2):82–87. doi: 10.4103/2225-4110.110407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Xie Y.-M., Yuwen Y., Dong F.-H., et al. Clinical practice guideline of traditional medicine for primary osteoporosis. Chinese Journal of Integrative Medicine. 2011;17(1):52–63. doi: 10.1007/s11655-011-0613-6. [DOI] [PubMed] [Google Scholar]
- 15.Sun J.-B., Chen M.-H., Lin D.-K. New insights into the tonifying kidney-yin herbs and formulas for the treatment of osteoporosis. Archives of Osteoporosis. 2017;12(1):p. 14. doi: 10.1007/s11657-016-0301-4. [DOI] [PubMed] [Google Scholar]
- 16.Shu B., Shi Q., Wang Y.-J. Shen (kidney)-tonifying principle for primary osteoporosis: to treat both the disease and the Chinese medicine syndrome. Chinese Journal of Integrative Medicine. 2015;21(9):656–661. doi: 10.1007/s11655-015-2306-z. [DOI] [PubMed] [Google Scholar]
- 17.Lin H., Wang X., Mo Y., et al. Acupuncture for primary osteoporosis: evidence, potential treatment prescriptions, and mechanisms. Evidence-Based Complementary and Alternative Medicine. 2019;2019:15. doi: 10.1155/2019/2705263.2705263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Atkins D., Best D., Briss P. A., et al. Grading quality of evidence and strength of recommendations. BMJ (Clinical Research Ed) 2004;328(7454):p. 1490. doi: 10.1136/bmj.328.7454.1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zheng Y. X., Wang X. Z., Zhang Z. K. Bushen Yijing Fang reduces fall risk in late postmenopausal women with osteopenia: a randomized double-blind and placebo-controlled trial. Scientific Reports. 2019;9:p. 2089. doi: 10.1038/s41598-018-38335-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zhu H. M., Qin L., Garnero P., et al. The first multicenter and randomized clinical trial of herbal Fufang for treatment of postmenopausal osteoporosis. Osteoporosis International. 2012;23(4):1317–1327. doi: 10.1007/s00198-011-1577-2. [DOI] [PubMed] [Google Scholar]
- 21.Zhao Z. Q., Yan X. X. A study on the improvement of clinical symptoms of primary osteoporosis with tonifying kidney method by traditional Chinese medicine. Chinese Journal of Osteoporosis. 2018;24(3):371–375. [Google Scholar]
- 22.Yuan Y., Tang T., Shi S. Q., Wang W. D. Clinical application effect of therapy combined traditional Chinese and western medicine for senile osteoporosis. Chinese Archives of Traditional Chinese Medicine. 2014;32(8):2014–2017. [Google Scholar]
- 23.Huang P. Observation on the curative effect of Chinese and Western medicine in the treatment of primary osteoporosis. Journal of Practical Traditional Chinese Medicine. 2015;31(4):298–299.2015530819 [Google Scholar]
- 24.Wu W., Li D. F., Zhi X., Meiqing H. Preventive and therapeutic effects of xianling gubao capsules for postmenopausal osteoporosis. Journal of Guangzhou University of Traditional Chinese Medicine. 2005;22(3):191–193.2005276556 [Google Scholar]
- 25.Liu B. X., Wang L. P., Xu M., et al. Postmenopausal osteoporosis of liver and kidney deficiency type treated with acupoint catgut embedding by stages. Chinese Acupuncture & Moxibustion. 2011;31(4):315–319. [PubMed] [Google Scholar]
- 26.Liu B. X., Wang L. P., Xu M., Huang C. J., Tang F. Y. Effect of embedding thread at acupoints on TCM syndrome integral and quality of life scale of the patients with postmenopausal osteoporosis of liver and kidney deficiency type. Chinese Archives of Traditional Chinese Medicine. 2011;29(3):550–552. [Google Scholar]
- 27.Qi Y. J. Clinical effect of bushen qianggu decoction on senile osteoporosis. Modern Journal of Integrated Traditional Chinese and Western Medicine. 2016;25(22):2461–2463.2016515893 [Google Scholar]
- 28.Li Y. D., Fan Z. Q., Lu C. Y. The effect of Bushen Jianpi Decoction assisted with western medicine on senile osteoporosis and its effect on bone mineral density. Nei Mongol Journal of Traditional Chinese Medicine. 2017;36(21):105–106. [Google Scholar]
- 29.Hu J., Li C. Observation on the therapeutic effect of Tonifying the kidney and strengthening the spleen on primary osteoporosis. Hubei Journal of Traditional Chinese Medicine. 2012;34(4):11–12.2012349754 [Google Scholar]
- 30.Liu W. X., Gong Y. Y. Study on the therapeutic effect of Bushen Jianpi Huoxue decoction combined with alendronate sodium tablets on osteoporosis. Shaanxi Journal of Traditional Chinese Medicine. 2018;39(10):1426–1428. [Google Scholar]
- 31.Chen S., Xie L., Tao Y., Xu G., Ma Y. M. Observation on the therapeutic effect of Bushen Jiangu formula combined with salmon calcitonin on senile osteoporosis. Chinese Journal of Traditional Medical Science and Technology. 2017;24(3):320–321. [Google Scholar]
- 32.Zou Z. Clinical effect of bushen jiangu decoction on postmenopausal osteoporosis. Journal of Modern Medicine & Health. 2016;32(11):1725–1726. [Google Scholar]
- 33.Han J. Primary osteoporosis randomized parallel group study bushenzhuanggutang combined western medicine. Journal of Practical Traditional Chinese Internal Medicine. 2013;12:32–34. [Google Scholar]
- 34.Huang Y. Q., Shao M., Xu S. J., Jiang T. Clinical observation on bushen tang combined with alendronate sodium tablets for primary osteoporosis with kidney deficiency type. Journal of New Chinese Medicine. 2018;50(9):102–105. [Google Scholar]
- 35.Huang S., Chen J. Y., Gao H. The effect of bushen huoxue recipe on bone density and the biochemical index of bone metabolism in senile osteoporosis. Journal of Clinical Orthopaedics. 2017;20(5):629–632. [Google Scholar]
- 36.Song S., Liu C., Jiang D. L. Random parallel control shudy of bushen huoxue recipe combine with miacalcic on senile osteoporosis. Journal of Practical Traditional Chinese Internal Medicine. 2015;29(5):88–90. [Google Scholar]
- 37.Pan J., Ding W. T. Study on the clinical effect of Bushen Huoxue decoction combined with oyster calcium carbonate in the treatment of primary osteoporosis of middle-aged and old people in rural areas. Chinese Journal of Clinical Rational Drug Use. 2014;33:133–134. [Google Scholar]
- 38.Wang X. W. Clinical observation on 100 cases of postmenopausal primary osteoporosis treated with Bushen Huoxue Decoction and calcium Erqi. Chinese Journal of Ethnomedicine and Ethnopharmacy. 2018;27(24):127–129. [Google Scholar]
- 39.Gui X., Gong G. X., Huang F. M. Clinical observation of 60 cases of primary osteoporosis treated with bushen yiqi huayu decoction. Drugs and Clinic. 2017;14(17):18–20.2017703424 [Google Scholar]
- 40.Liu B. X., Huang C. J., Liang D. B., Tang H. W. Clinical control study on postmenopausal osteoporosis treated with embedding thread according to syndrome differentiation and medication. Chinese Journal of Integrated Traditional and Western Medicine. 2011;31(10):1349–1354. [PubMed] [Google Scholar]
- 41.Xie X. Y., Zhang W. J., Yu W. W., Yang X. H. Effect of gushen recipe on bone turnover in osteoporosis patients. Journal of Guangzhou University of Traditional Chinese Medicine. 2018;35(5):805–809. [Google Scholar]
- 42.Liu Y., Wang C. W. Clinical effect of Erxian Bushen decoction combined with warm acupuncture in treating post-menopause osteoporosis with syndrome of kidney-Yang deficiency. Chinese Journal of Experimental Traditional Medical Formulae [zhongguo Shi Yan Fang Ji Xue Za Zhi] 2016;22(9):162–166. [Google Scholar]
- 43.Xu D.-M., Xu H., Liu J., et al. of thunder-fire moxibustion on pain, quality of life, and tension of multifidus in patients with primary osteoporosis: a randomized controlled trial. Medical Science Monitor. 2018;24:2937–2945. doi: 10.12659/msm.909725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Han X. L., Lou Z. J., Lin H. W. Treatment of senile osteoporosis with shugan wenshen tanyu shuangjie decoction and acupuncture. Gansu Journal of Traditional Chinese Medicine. 2011;24(2):32–34. [Google Scholar]
- 45.Ma D. N., Fan Y. J. Study on the effect of combination of traditional Chinese medicine and acupuncture in the treatment of osteoporosis. Contemporary Medical Symposium. 2018;16(7):58–59. [Google Scholar]
- 46.Ouyang G. O., Wang D.-Y., Xu X.-M. Clinical observation on acupuncture for male osteoporosis. World Journal of Acupuncture-Moxibustion. 2011;31(1):23–25. [PubMed] [Google Scholar]
- 47.Lu S. J. Effective observation on treating postmenopausal osteoporosis by catgut embedding therapy combined with medicine. Clinical Journal of Chinese Medicine. 2014;6(11):48–49. [Google Scholar]
- 48.Peng N. J., Zhong P. C., Zhao X. H. Clinical observation on 35 cases of primary osteoporosis treated by Acupoint Catgut Embedding. Hunan Journal of Traditional Chinese Medicine. 2017;33(10):101–102. [Google Scholar]
- 49.Peng N. J., Zhong P. C., Zhao X. H. Clinical study of acupoint catgut-embedding on primary osteoporosis. Guiding Journal of Traditional Chinese Medicine and Pharmacy. 2018;24(12):72–74. [Google Scholar]
- 50.Zhong P. C., Peng N. J., Zhao X. H. Observation of the curative effect of acupoint catgut embedding combined with western medicine on osteoporosis. Modern Journal of Integrated Traditional Chinese and Western Medicine. 2018;27(16):1714–1716. [Google Scholar]
- 51.Lin Z. W. The effect of Shenshu acupoint catgut embedding on bone mineral density of primary osteoporosis. Chinese Journal of Osteoporosis. 2006;12(4):381–383. [Google Scholar]
- 52.Lin Z. W. Clinical study on Shenshu acupoint catgut embedding therapy for postmenopausal osteoporosis. Journal of Clinical Acupuncture and Moxibustion. 2006;22(4):1–3. [Google Scholar]
- 53.Zou X. J., Hao Y. Y., Hou J., Pan S. L. Curative effect observation on point injection of saline combined with routine western medicine for primary senile osteoporosis. Journal of New Chinese Medicine. 2018;50(11):183–185. [Google Scholar]
- 54.Zhou Z. H., Wang N. Q., Ting C. E., Zhou X. G., Zhou J. W. Postmenopausal osteoporosis treated with acupoint injection of salmon calcitonin:a randomized contro. Chinese Acupuncture & Moxibustion. 2016;36(7):705–708. doi: 10.13703/j.0255-2930.2016.07.008. [DOI] [PubMed] [Google Scholar]
- 55.Zheng X. Y. Clinical Research Guidance of New Chinese Herbal Medicine (China) Beijing, China: China Medical Science and Technology Press; 2002. p. 356–360. [Google Scholar]
- 56.Su S.-B., Jia W., Lu A., Li S. Evidence-based ZHENG: a traditional Chinese medicine syndrome. Evidence-based Complementary and Alternative Medicine: ECAM. 2014;2014:2. doi: 10.1155/2014/484201.484201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Gao Z., Lu Y., Halmurat·Upur U., Jing J., Xu D. Study of osteoporosis treatment principles used historically by ancient physicians in Chinese medicine. Chinese Journal of Integrative Medicine. 2013;19(11):862–868. doi: 10.1007/s11655-013-1328-z. [DOI] [PubMed] [Google Scholar]
- 58.Liu Y., Liu J. P., Xia Y. Chinese herbal medicines for treating osteoporosis. Cochrane Database of Systematic Reviews. 2014;3 doi: 10.1002/14651858.CD005467.pub2.CD005467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Deng W.-M., Zhang P., Huang H., et al. Five-year follow-up study of a kidney-tonifying herbal Fufang for prevention of postmenopausal osteoporosis and fragility fractures. Journal of Bone and Mineral Metabolism. 2012;30(5):517–524. doi: 10.1007/s00774-012-0351-7. [DOI] [PubMed] [Google Scholar]
- 60.Shen Y., Liu X., Li H., Liu H., Pan Z., Chen G. Brain neural effects of the ‘tonifying kidney and benefiting marrow’ method in the treatment of osteoporosis. Journal of Traditional Chinese Medicine. 2019;39(6):902–909. [PubMed] [Google Scholar]
- 61.Bian Q., Huang J. H., Liu S. F., et al. Different molecular targets of Icariin on bMSCs in CORT and OVX -rats. Frontiers in Bioscience (Elite Edition) 2012;4:1224–1236. doi: 10.2741/453. [DOI] [PubMed] [Google Scholar]
- 62.Wang H., Ma M.-H., Nian S.-S., Xu L.-L. Antiosteoporotic activity of icariin in ovariectomized rats. Phytomedicine. 2009;16(4):320–326. doi: 10.1016/j.phymed.2008.12.006. [DOI] [PubMed] [Google Scholar]
- 63.Li J.-F., Zhao Y., Cai M.-M., Li X.-F., Li J.-X. Synthesis and evaluation of a novel series of heterocyclic oleanolic acid derivatives with anti-osteoclast formation activity. European Journal of Medicinal Chemistry. 2009;44(7):2796–2806. doi: 10.1016/j.ejmech.2008.12.024. [DOI] [PubMed] [Google Scholar]
- 64.Yang Z., Huang J. H., Liu S. F. The osteoprotective effect of psoralen in ovariectomy-induced osteoporotic rats via stimulating the osteoblastic differentiation from bone mesenchymal stem cells. Menopause. 2012;19(10):1156–1164. doi: 10.1097/gme.0b013e3182507e18. [DOI] [PubMed] [Google Scholar]
- 65.Zhao Y., Huai Y., Jin J., Geng M., Li J.-X. Quinoxaline derivative of oleanolic acid inhibits osteoclastic bone resorption and prevents ovariectomy-induced bone loss. Menopause. 2011;18(6):690–697. doi: 10.1097/gme.0b013e3181fd7f4b. [DOI] [PubMed] [Google Scholar]
- 66.Zheng X., Wu G., Nie Y., Lin Y. Electroacupuncture at the governor vessel and bladder meridian acupoints improves postmenopausal osteoporosis through osteoprotegerin/RANKL/RANK and Wnt/β-catenin signaling pathways. Experimental and Therapeutic Medicine. 2015;10(2):541–548. doi: 10.3892/etm.2015.2553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Chen G.-Z., Xu Y.-X., Zhang J.-W., Liu S.-H., Guo Z.-Y. Effect of acupoint catgut-embedding on the quality of life, reproductive endocrine and bone metabolism of postmenopausal women. Chinese Journal of Integrative Medicine. 2010;16(6):498–503. doi: 10.1007/s11655-010-0574-1. [DOI] [PubMed] [Google Scholar]
- 68.Zhang L., Wang Y., Xu Y., et al. Metabonomic analysis reveals efficient ameliorating effects of acupoint stimulations on the menopause-caused alterations in mammalian metabolism. Scientific Reports. 2014;4:p. 3641. doi: 10.1038/srep03641. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used to support the findings of this study have been deposited in the following repository: PubMed: https://www.ncbi.nlm.nih.gov/pubmed/; Cochrane Library: https://www.cochranelibrary.com/; EMBASE: https://www.embase.com/; Web of Science: http://webofscience.com/; CNKI: https://www.cnki.net/; VIP: http://www.cqvip.com/; Wanfang: http://www.wanfangdata.com.cn/; CBM: http://www.sinomed.ac.cn/.