

To the editor:
We read with great interest the article by Abdullah et al. where they described an interesting cytological variant of chronic myeloid leukemia successfully treated with dasatinib (1). We wish to complement the article with our experience to further enhance the imparted knowledge by highlighting a rather rare complication of treatment with dasatinib, which was not emphasized in the above mentioned article for the benefit of the readers. A 61-year-old female with a past medical history of hyperlipidemia was diagnosed to have CML 4 years ago. She had been on dasatinib with complete hematologic and cytogenetic remission. She presented to ER with insidious onset, persistent, worsening shortness of breath and mild, nonproductive cough of 1 week duration. She denied any history of fever, chills, chest pain, and loss of appetite or weight. At presentation, her vitals were stable and she was saturating 98% in 2 L oxygen. Respiratory examination revealed stony dull note on percussion and absent breath sound over the right axillary, interscapular and infrascapular area. CXR confirmed a right-sided pleural effusion (Figure 1A). CT showed large, right pleural effusion with an adjacent collapse of the right lower lobe, consistent with atelectasis. It also showed pericardial effusion with thickening (Figure 1B and 1C). A diagnostic thoracentesis revealed an exudative effusion with low adenosine deaminase and negative cytology. Multiple blood, sputum, and pleural fluid culture were negative. Dasatinib induced pleuro-pericardial effusion was diagnosed and dasatinib was stopped. Following clinical improvement, she was discharged in a stable condition, with the plan of initiating an alternate tyrosine kinase inhibitor Nilotinib.
Figure 1.
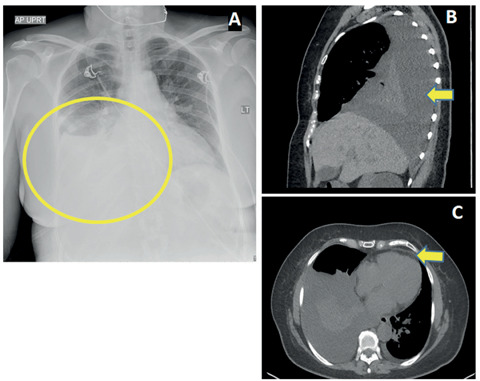
A: Chest radiograph showing right sided pleural effusion and enlargement of cardiac silhouette. B: Coronal view of computed tomography chest showing pleural effusion. C: Transverse view of CT chest showing both pleural and pericardial effusion
Dasatinib is a tyrosine kinase inhibitor used in chronic myeloid leukemia (CML). All tyrosine kinase inhibitors (TKI) can lead to serosal inflammation/serositis hence cause complication of pleural effusion. When used in the treatment of CML, Dasatinib can cause pleural effusion in 10 to 35% of patients (2). Off-target actions of TKIs are postulated to be the mechanism. Effusion can occur any time during treatment and commonly characterized as exudative, lymphocyte predominant effusion, of mild to moderate in severity (3). Concurrent pericardial effusion is seen in 29% of cases. Risk factors are hypertension, hyperlipidemia, previous cardiac disease and rash in response to TKI therapy (2, 3). Other cardiac complications are pulmonary artery hypertension, congestive heart failure, pericardial effusion, QTc prolongation, and sudden cardiac death (3). Management of Dasatinib-induced pleural effusion includes dose interruptions, reductions, or permanent discontinuation. Steroids, diuretics, and therapeutic paracentesis have also been tried (3).
In conclusion among the TKIs pleuro-pericardial effusion is most commonly seen with Dasatinib. Before attributing the serositis to TKIs, infections and underlying malignancy should be ruled out (2, 4-7).
Conflict of interest:
Each author declares that he or she has no commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangement etc.) that might pose a conflict of interest in connection with the submitted article
References
- 1.Abdullah MA, Amer A, Nawaz Z, et al. An uncommon case of chronic myeloid leukemia with variant cytogenetic. Acta Biomed. 2018;89(3-s):28–32. doi: 10.23750/abm.v89i3-S.7217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cortes JE, Jimenez CA, Mauro MJ, Geyer A, Pinilla-Ibarz J, Smith BD. Pleural Effusion in Dasatinib-Treated Patients With Chronic Myeloid Leukemia in Chronic Phase: Identification and Management. Clin Lymphoma Myeloma Leuk. 2017;17(2):78–82. doi: 10.1016/j.clml.2016.09.012. [DOI] [PubMed] [Google Scholar]
- 3.Moslehi JJ, Deininger M. Tyrosine Kinase Inhibitor-Associated Cardiovascular Toxicity in Chronic Myeloid Leukemia. J Clin Oncol. 2015;33(35):4210–8. doi: 10.1200/JCO.2015.62.4718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lal A, Al Hammadi A, Rapose A. Latent Tuberculosis Infection, Treatment initiation and completion rates in Persons seeking immigration and healthcare workers. Am J Med. 2019;132(11):1353–1355. doi: 10.1016/j.amjmed.2019.04.036. [DOI] [PubMed] [Google Scholar]
- 5.Mishra AK, Mani S, George AA, Sudarsanam TD. Recurrent pericardial effusion and tamponade in a patient with Erdheim-Chester disease (ECD) BMJ Case Rep. 2015;2015 doi: 10.1136/bcr-2015-212483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lal A, et al. Rare Cause of Respiratory Failure: A Twist in the Tale. Ann Am Thorac Soc. 2018;15(7):880–883. doi: 10.1513/AnnalsATS.201802-122CC. [DOI] [PubMed] [Google Scholar]
- 7.Lal A, et al. Recurrent Pulmonary Embolism and Hypersensitivity Pneumonitis Secondary to Aspergillus, in a Compost Plant Worker: Case Report and Review of Literature. Lung. 2018;196(5):553–560. doi: 10.1007/s00408-018-0142-6. [DOI] [PubMed] [Google Scholar]