

Abstract
Background:
Omega-3 fatty acids (FAs) can produce several beneficial effects and are commonly used for the treatment of migraine symptoms. Although current therapeutic measures for migraine included pharmacological therapies, dietary supplements, and herbal ingredients, dietary patterns, acupuncture, relaxation techniques, biofeedback, and psychotherapy, omega-3 FAs therapeutic role seems to be obtained through the inhibition or reduction of the release of inflammatory cytokines. The present review aims to provide updated information about the effects of omega-3 FAs in migraine treatment, investigating their clinical effects alone or in combination with other substances.
Methods:
Bibliographic research was conducted by examining scientific literature from January 2000 until January 31, 2020. Ten clinical studies were included in the review. Quality assessment of randomized controlled trials was performed by using the JADAD scale.
Results:
Clinical studies methodology is not always of good quality and results show moderate evidence concerning the therapeutic role of omega-3 FAs in migraine.
Conclusion:
Further clinical trials are necessary to implement the knowledge concerning the use of omega-3 fatty acids in the treatment of migraine.
Keywords: docosapentaenoic acid, docosahexaenoic acid, eicosapentaenoic acid, headache, migraine, omega-3 fatty acids, pain, polyunsaturated fatty acids
1. Introduction
Omega-3 (or ω-3) is the name for long-chain polyunsaturated fatty acids (PUFAs).[1] Among PUFAs properties, the most relevant are represented by antioxidant,[2] anti-inflammatory,[3] and neuroprotective effects.[4] FAs are key components of nutrition, play a primary role in the lipid composition of cell membranes,[5] and their metabolites are crucial as cell signaling molecules.[6] The main FAs present in the brain and nervous system are long-chain PUFAs.[7,8] The physiological functions of Omega-3 FAs in the nervous system include the maintenance of membrane fluidity and synapse integrity[9] and endogenous derivatives of Omega-3 FAs, act as anti-inflammatory mediators.[10]
Eicosapentaenoic acid (EPA), docosapentaenoic acid (DPA), and docosahexaenoic acid (DHA) are the most important long-chain omega-3 FAs, however, their endogenous formation can be not sufficient for physiological necessities.[11] They are structurally and functionally distinct from omega-6 PUFAs, and inflammatory cells contain high proportions of the omega-6 PUFAs and low proportions of omega-3 PUFAs.[1,12,13] In general, lipids derived from omega-6 FAs show pro-nociceptive properties, while mediators derived from omega-3 FAs have anti-nociceptive properties, with some exceptions.[14] Moreover, omega-3 interferes with the conversion of omega-6 to eicosanoids, thus reducing the production of prostaglandins and leukotrienes.[12,15]
Omega-3 and omega-6 FAs modulate inflammation, and pain-related biochemical pathways,[16] in particular, omega-3 FAs intake have been associated with decreased concentration of C-reactive protein (CRP), pro-inflammatory eicosanoids, cytokines, chemokines, and other inflammatory biomarkers.[17]
In recent years, PUFAs were recommended to treat systemic pathological conditions,[18] and administration of omega-3 PUFAs has been proposed for the treatment neurological diseases such as hyperactive disorder, attention deficit,[19] Alzheimer,[20] depression,[21] neurodegenerative diseases,[22] and spinal cord injury.[23] These FAs mediate numerous physiological functions and have therapeutic potential for neuro-traumatic conditions[24] and omega-3 FAs intake provide relief from neuropathic pain caused by diabetic neuropathy.[25] In addition, patients affected by cervical radiculopathy and thoracic outlet syndrome reported long term significant pain attenuation with high oral doses of omega-3 FAs.[26] More recently, analgesia with omega-3 FAs in chronic headache has also been observed.[27]
1.1. Migraine
Migraine is a common chronic neurological disease, characterized by frequent attacks of disrupting pain, commonly associated with depression, anxiety, hypertension, stroke, and cardiovascular diseases.[28] Even in its episodic form migraine can evolve in a chronic condition.[29] Factors that could contribute to its pathogenesis are menstrual cycle, pregnancy, lifestyle, diet, and chronic stress.[30]
Etiology of migraine is still not completely known, even if genetics and environmental factors could play a central role[31] and current opinion states that neurogenic inflammation contributes to migraine pathogenesis.[32] It is well known that in a neuro-inflammatory condition, increased neuronal activity leads to the release of inflammatory mediators such as the cytokine tumor necrosis factor (TNF)-α.[33] Phases of attack migraine are also frequently associated with higher serum levels of glutamate, magnesium deficiency, monoaminergic pathway and mitochondrial disorders, calcitonin gene related peptide (CGRP) release.[34,35] Cytokines, by increasing membrane permeability and through cell-to-cell interactions, have a significant role in the inflammatory process of the central nervous system (CNS) and generation of pain.[36]
In migraine patients, vascular dysfunction is generated by increased production of adhesion molecules and, during attacks, is sustained by increased concentrations of pro-inflammatory cytokines.[34] Expression of pro-inflammatory cytokines, adhesion molecules, and activation of microglia, contribute to generate and sustain inflammation and neuropathic pain.[37,38] Human and experimental pre-clinical research also highlighted the role of cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS), confirming that they contribute to sustaining inflammation and neurogenic pain in migraine.[39]
Migraine is a neurovascular disorder[40] affecting approximately 11% of the population worldwide[41] and classified among the 10 most prevalent incapacitating diseases.[42] It is a common disorder even at early ages with the prevalence of 10.6% in children 5 to 15 years old.[43] The mean age of onset of migraine symptoms is about 7 years in boys and approximately 10.9 years in girls.[44] Migraine attacks may have a negatively impact the quality of life of children,[45] moreover, recurrent headaches can worsen daily activities even during adolescence.[46]
1.2. The role of fatty acids in neuroinflammation
Neurogenic inflammation plays a crucial role in the pathogenesis and progression of migraine,[47] and also leads to the sensitization and activation of perivascular meningeal afferent nerves.[48] Moreover, the activated glia is responsible for producing pro-inflammatory cytokines and mediators capable of damaging the blood–brain barrier. FAs modulation of membrane proteins related to ion channels including the transient receptor potential family, could be responsible for omega-3 analgesic properties. Changes in lipid composition in the microenvironment influence the physiological function of membrane proteins related to cellular signaling processes,[49] especially those involving G-proteins.[50] On this basis, membrane-lipid supplementation can also be employed in the prevention or the treatment of many health problems as it is for vascular diseases and cancer pathologies.[51,52]
PUFAs produce self-mediated (i.e., acting as peroxisome proliferator-activated receptor alpha ligands) biological effects and effects mediated by their bioactive metabolites.[53,54] These bioactive compounds are specialized mediators such as epoxides, electrophilic oxo-derivatives, ethanolamines, acylglycerols, acrylamides of amino acids or neurotransmitters, and fatty acyl esters of hydroxyl fatty acids (FAHFAs),[7,55–58] exerting mostly anti-inflammatory effects.[59]
The production of pro-inflammatory proteins, such as tumor necrosis factor (TNF)-α, interleukin (IL)-1, IL-6, and IL-8 in various cell types, including endothelial cells, monocytes, macrophages, and dendritic cells is inhibited by PUFAs.[17] Moreover, PUFAs regulate the severity of inflammatory diseases and reduce neurogenic pain.[60,61] In the light of the concepts expressed above, the authors collected clinical studies carried out with omega-3 FAs, alone or in association, with the aim to evaluate the state of the art of their use in migraine therapy.
2. Materials and methods
The authors collected clinical findings carried out investigating the effects of omega-3 FAs use, alone or in combination with other substances, in the treatment of migraine. The analysis included all articles published in peer-reviewed scientific journals describing clinical trials omega-3 fatty acids (FAs) in the treatment of migraine. Articles were excluded if they did not meet the following inclusion criteria: articles written only in English language, articles published in peer-reviewed scientific journals.
2.1. Search strategy
Bibliographic research was carried out, by examining scientific literature from January 2000 until January 31, 2020, independently by 2 researchers (blinded to the authors and initially on results) in the major scientific databases and search engines of peer-reviewed literature on life sciences and biomedical topics (PubMed, Scopus, Embase, Web of Science, Google Scholar).
The investigators used the following keywords or combination of keywords: “Omega-3 fatty acids,” “eicosapentaenoic acid (EPA),” “docosapentaenoic acid (DPA),” “docosahexaenoic acid (DHA),” and “migraine.” All articles published in peer-reviewed scientific journals describing clinical trials and applications of omega-3 FAs in migraine were collected and discussed. Case series, case reports, and human studies were excluded.
2.2. Study selection
The selection review of clinical studies written in English and regarding omega-3 FAs were performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement[62] (Fig. 1). Only clinical trials were included in the review if they were conducted in subjects of all ages, and, investigated the impact of omega-3 supplement, omega-3 in association with other drugs, or omega-3-enriched diet, on patients suffering for migraine according to the criteria of the International Headache Society.
Figure 1.
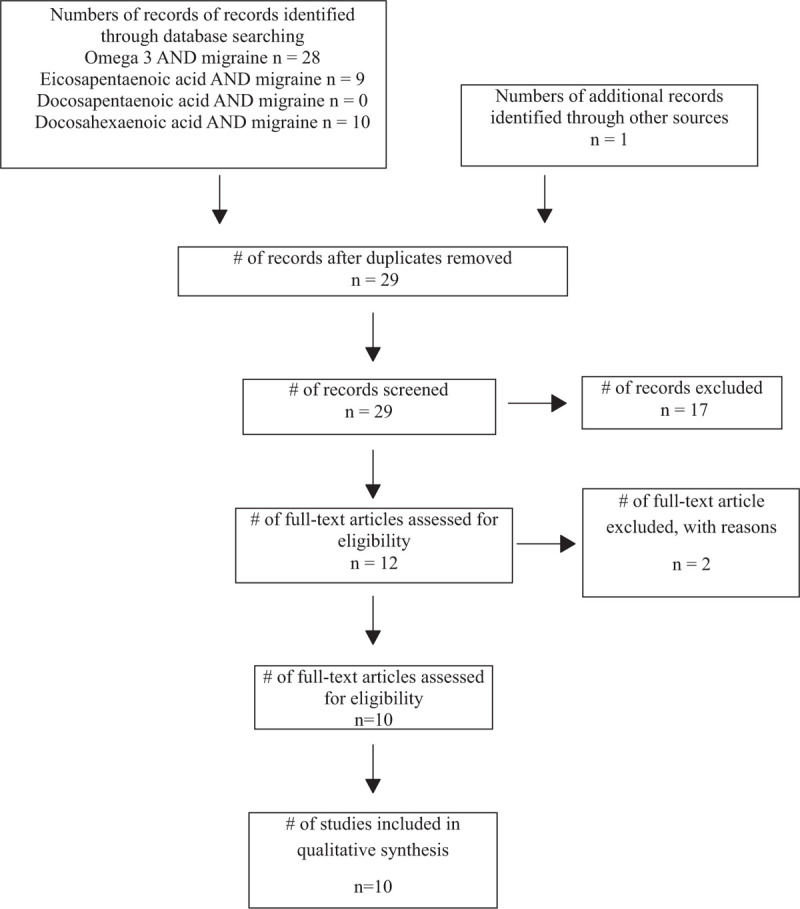
PRISMA flow chart diagram showing the process of literature search and studies selection. PRISMA = preferred reporting items for systematic reviews and meta-analyses.
From the eligible articles, 2 other investigators independently extracted data by using a standard data extraction form. There was not any disagreement between investigators about data extraction. Variables for which data were sought are the therapeutic indication, design of the study, number, sex, and age of subjects included in the studies, endpoints, adverse effects, and outcome.
The JADAD scale was used to assess the risk of bias analysis, evaluating the reported method of randomization, blinding, and loss to follow-up in a clinical trial and assigns a score from 0 to 5, with higher scores (3–5), indicating higher methodological quality and lower scores (0–2) indicating the lower methodological quality of the trial.
This systematic review does not need ethical approval, because it does not utilize the individual patient data.
3. Results
A collection of 29 scientific articles, describing the effects of omega-3 FAs treatment for migraine corresponding to the inclusion criteria were selected from our bibliography research. Seventeen articles were excluded for title and abstract (Fig. 1).
Study selection and characteristics, according to PRISMA guidelines were reported in the relative flow diagram. (Fig. 1).
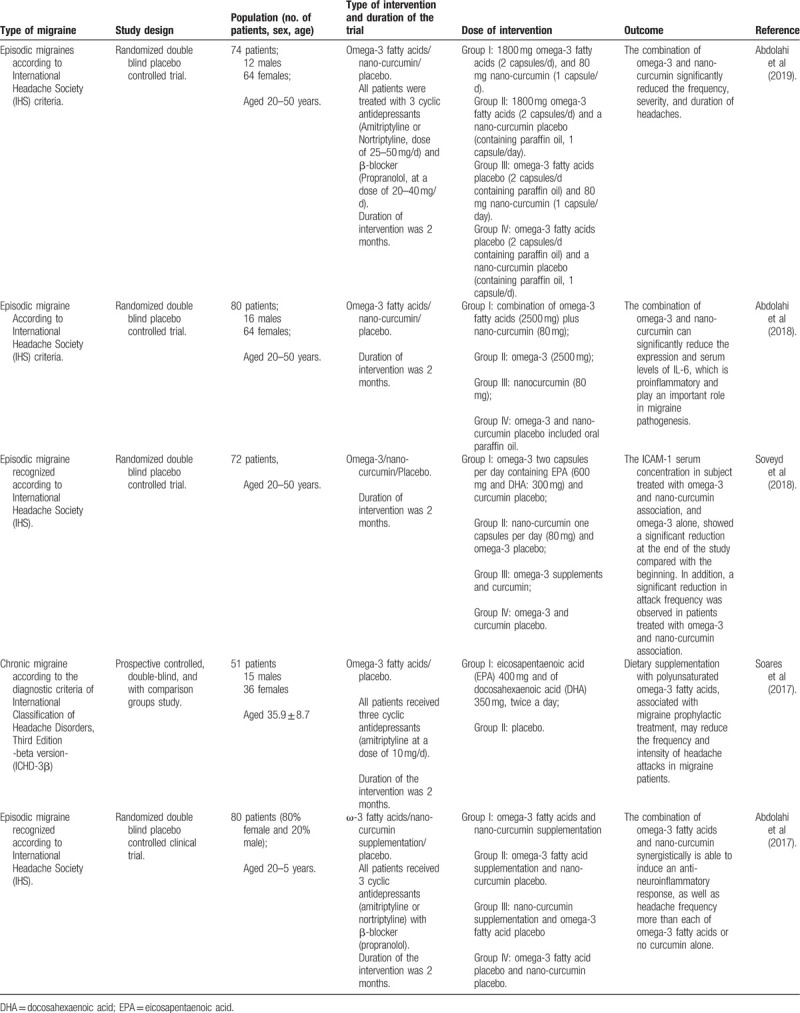
Ten clinical studies were included in the review. Five studies conducted on the effects of omega-3 FAs alone (Table 1) and 5 clinical trials, carried out to study the antimigraine effects of omega-3 FAs in combination with other substances (Table 2), were included in this review. Type of migraine, study design, population, type and duration of intervention, dose of intervention, and outcomes of the trials, were reported.
Table 1.
Clinical studies investigating effects of omega-3 FAs in migraine patients.
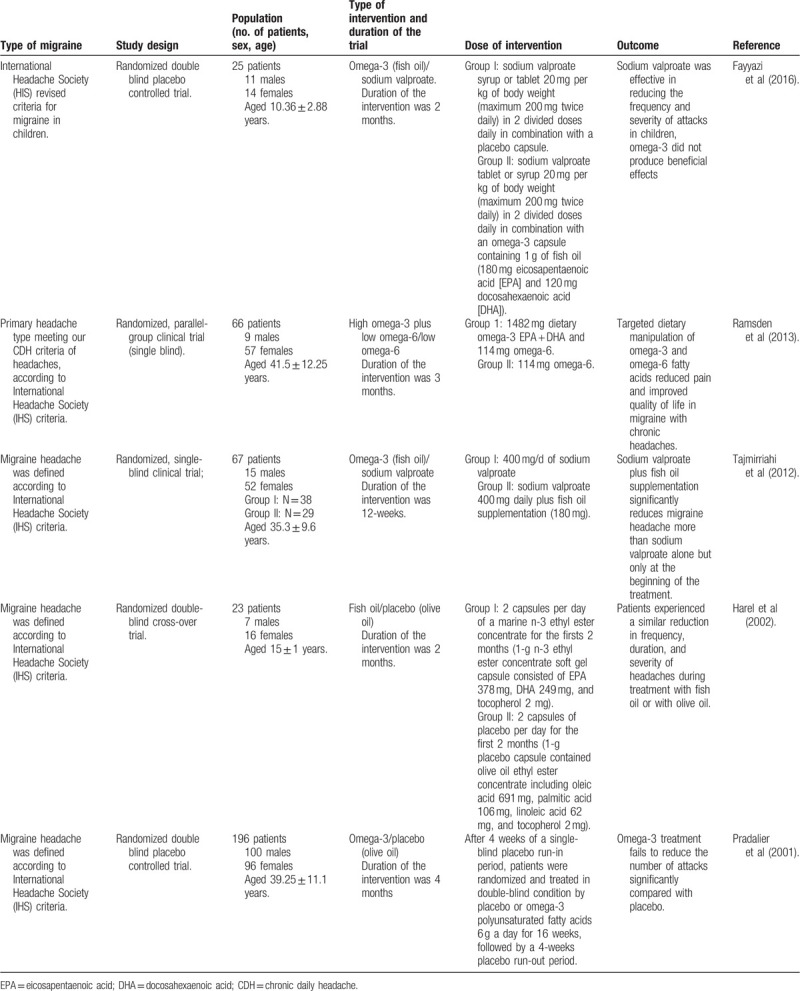
Table 2.
Clinical studies investigating effects of omega-3 FAs in association with other drugs in migraine patients.
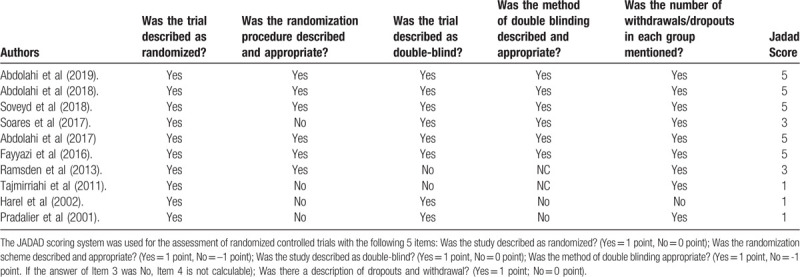
Quality assessment of randomized controlled trials was reported according to the JADAD scale (Table 3). All the studies were described as randomized trials, however, only in 60% of them, the randomization procedure was described and appropriate. A double blinding procedure was adopted in 8 of the 10 studies commented. In 4 of the studies adopting double-blinding, this procedure was not appropriately described. According to the JADAD scale evaluation only 70% (6 clinical trials) of the studies were well designed and conducted following high methodological quality standard and the remaining 30% (4 studies) were poor from the methodological point of view.
Table 3.
Quality assessment of clinical trials according to Jadad score.
4. Discussion
Current therapeutic measures for migraine included pharmacological therapies, moreover, other therapeutic strategies are represented by dietary supplements, and herbal ingredients, dietary patterns, acupuncture, relaxation techniques, biofeedback, and psychotherapy.[63,64]
Therapeutic strategies for the treatment of migraine largely include non-steroidal anti-inflammatory drugs (NSAIDs), COX-2 inhibitors, and triptans.[34]
In an early study, Pradalier et al[65] did not find any difference in mean intensity, mean duration of the attacks, and rescue medication use, between the group treated with omega-3 FAs 6 g/d supplementation for 16 weeks in comparison with placebo.
Similar results were also observed in a cross-over study carried out on adolescent patients suffering from frequent migraines for at least 1 year treated for 2 months with fish oil and 2 months of olive oil (used as placebo). Results showed no difference in frequency, duration, and severity of headaches during treatment with fish oil and olive oil. Authors of the study suggested that, despite the absence of a significant difference between treatments, the marked improvement from baseline experienced by the patients should not be dismissed as simply a placebo effect.[15] However, in this study omega-3 FAs were not compared with a real placebo, and this can be considered a limiting factor to the possibility of evaluating antimigraine effects.
In patients suffering from chronic migraine who supplemented the diet by incrementing omega-3 FAs intake, a reduction of the number of headaches per month has been observed. The authors affirm that this beneficial effect of omega-3 FAs could be due to the decrease in the production of prostaglandins and leukotrienes or to a change in the synthesis and release of serotonin by platelets.[66]
Valproate antimigraine mechanism is based on the increase of brain gamma-aminobutyric acid (GABA) levels and the inhibition of inflammatory cytokine's mRNA expression (TNF-α, IL-1β, IL-6, and IL-17), and, the inhibition of macrophages and B, T cells aggregation leading to the suppression of neuro-inflammatory states.[67] Conventional medications for migraine in children include drugs such as sodium valproate, topiramate, propranolol, amitriptyline, naproxen, and flunarizine.[68] The treatment of migraine in teenagers consists chiefly of prophylactic medications and behavioral therapy.[69,70] However, often, unreliable results have been obtained, raising the necessity for the development of new therapeutic strategies to prevent and to treat migraine attacks in adolescents.
Effects of dietary supplementation with fish oil were investigated in migraine prevention in a 12-week, randomized, single-blind clinical trial conducted on 67 patients (52 women, 15 men) with migraine headache allocated to 2 groups. In the first group, 38 patients received 400 mg/d sodium valproate. In the second group, 29 patients received sodium valproate 400 mg daily plus fish oil supplementation (180 mg). A significant decrease in duration, monthly frequency, and severity of headache after month 1, 2, and 3 in comparison with month 0 occurred in both groups. A reduction occurred in headache severity (P = .046) and frequency (P = .044) in the group with fish oil supplementation after month 1 in comparison with sodium valproate alone. However, there was no significant difference between the 2 treatment groups in the duration of headache attacks after the first month. Mean intensity, mean duration, and mean frequency of the attacks after the second and third months also did not show a significant difference between the 2 treatments.[1]
The effects of omega-3 FAs in combination with valproate were also investigated in the prevention of migraine attacks in children aged 5–15 years. Results of a group treated with sodium valproate and 1 g of omega-3 were compared with a control group treated only with sodium valproate and a placebo for 2 months (12 cases and 13 controls were enrolled). While sodium valproate was effective in reducing the frequency and severity of attacks in children, omega-3 FAs did not produce beneficial effects.[71]
Data from these studies show contradictory results about the use of omega-3 FAs in association with sodium valproate in migraine.
Clinical and biochemical effects of targeted alteration in dietary omega-3 and omega-6 FAs for the treatment of chronic headaches were evaluated in a 4-weeks randomized, single-blinded, parallel-group clinical trial. The analysis of the results indicated that the combination of increasing dietary omega-3 FAs with a concurrent reduction in omega-6 produced statistically significant and clinically relevant improvements in number headache hours per day, severity of headache per days, and headache-related quality of life compared with baseline and compared with the omega-6-lowering group intervention.[14]
In a recent pre-clinical study, it has been observed that the intake of omega-3 FAs (both of EPA and DHA) in association with curcumin, active principle extracted by the plant Curcuma longa, synergistically decrease COX-2 activity and iNOS gene expression as well as nitric oxide (NO) production in macrophage cells, thus increasing antioxidant effects of heme oxygenase-1.[72]
Positive effects have also been shown with the association of omega-3 FAs and curcumin which together seem to potentiate the NSAID's anti-inflammatory effects.[73] A further possible advantage is that potential synergetic effects of the combination of omega-3/curcumin could allow a reduction of the dosage of both substances.[72] These compounds, in addition to their anti-inflammatory and cardio-protective properties, both show neuroprotective capabilities, suggesting wider clinical employment. Moreover, the use of this combination can induce anti-neuroinflammatory adaptation through the downregulation of TNF-α gene expression and gene production. This could cause a major reduction of migraine attacks concerning omega-3 FAs or curcumin when administered alone.[61]
High levels of (IL)-6 and (CRP) can lead to disruption of the integrity of the blood–brain barrier and can contribute to generating and maintaining neurogenic inflammation, and, consequently, to the progression of the disease. A recent study confirms that both omega-3 FAs and nano-curcumin down-regulate IL-6 mRNA and, if used in combination, significantly decrease the serum concentration of both IL-6 and CRP, confirming the possible synergetic relation.[74]
Adhesion of leukocytes to the walls of the cerebral blood vessels constitutes an important stage in the inflammatory process. Curcumin and omega-3 FAs, affecting transcription factors, can regulate the gene expression and serum levels of the endothelial factor ICAM-1, playing an important role in leukocyte trafficking, immunological synapse formation, and numerous cellular immune responses.[75] In a recent study,[76] the authors aimed to evaluate the synergistic effects of omega-3 FAs and nano-curcumin on ICAM-1 gene expression and serum levels in migraine patients, suggesting that the supplementation with these 2 nutrients can lead to an improvement in the function of metabolic pathways, and can also be employed in the treatment or prevention of migraine complications. Other authors agree with this conclusion[30] affirming that omega-3 FAs and nano-curcumin associations can be useful to spare drug consumption in migraine patients or even be a safer substitute for drugs.
A clinical trial involving 74 episodic migraine patients who received omega-3 FAs, nano-curcumin, a combination of them, or a placebo, for a period of over 2 months, evaluated the expression of COX-2/iNOS (in peripheral mononuclear blood cells isolated from patients) and COX-2/iNOS serum levels, measured using real-time polymerase chain reaction and enzyme-linked immunosorbent assay, respectively. Results showed that omega-3 FAs and nano-curcumin could reinforce each other's effects in the downregulation of COX-2/iNOS mRNA, as well as to cause a reduction of their serum levels. These experiments also confirmed that the combination of omega-3/nano-curcumin significantly reduced the frequency, severity, and duration of headache attacks.[39]
5. Conclusions
The rationale for the usage of omega-3 FAs is based on a mechanism showing partial similarity to the COX-2 inhibitor drugs, with the advantage that both EPA and DHA administrations are associated with a lower profile of effects. On the other hand, omega-3 FAs reduce inflammatory and neurogenic pain by decreasing the pain receptor's expression and activity. Comprehensively, data from literature show that they possess neuroprotective properties that result in the prevention of inflammatory, neurologic, and vascular diseases.
Moreover, albeit the exact role of omega-3 FAs in inflammatory processes has not been completely clarified, it was suggested that a therapeutic role is achieved through the inhibition or reduction of the release of inflammatory cytokines (including TNF-α, IL-1β, IL-6) reduced expression of endothelial dysfunction markers (ICAM and VCAM). In this view, the inhibitory effects of omega-3 FAs on cyclooxygenase-2 enzymes and nitrous oxide could be seen as an effective contribution to healing and/or preventing disease progression of migraine.
The limits of this review must be underlined and reported, mainly related to the relative inhomogeneity of the trials, and this is due to the few studies reported in the literature, although from the analysis of the results, the outcomes seem to converge.
In conclusion, from the analysis of the studies included in this narrative review, it is evident that part of the studies are not characterized by good quality methodology and they do not show established evidence of the therapeutic role of Omega-3 FAs in migraine. Further clinical trials of good quality are necessary to implement the knowledge concerning the use of omega-3 fatty acids in the treatment of migraine.
Author contributions
Conceptualization: Luigi Cardia, Domenico Quattrone, Gioacchino Calapai.
Data curation: Luigi Cardia, Fabrizio Calapai, Cristina Mondello, Emanuela Elisa Sorbara, Carmen Mannucci.
Formal analysis: Luigi Cardia, Fabrizio Calapai, Emanuela Elisa Sorbara, Epifanio Mondello.
Investigation: Fabrizio Calapai, Cristina Mondello, Domenico Quattrone, Carmen Mannucci.
Methodology: Luigi Cardia, Fabrizio Calapai, Cristina Mondello, Domenico Quattrone, Carmen Mannucci, Gioacchino Calapai.
Resources: Cristina Mondello.
Supervision: Gioacchino Calapai, Epifanio Mondello.
Validation: Epifanio Mondello.
Visualization: Luigi Cardia, Domenico Quattrone, Emanuela Elisa Sorbara.
Writing – original draft: Luigi Cardia, Carmen Mannucci.
Writing – review & editing: Luigi Cardia, Gioacchino Calapai, Epifanio Mondello.
Footnotes
Abbreviations: CGRP = calcitonin gene related peptide, COX-2 = cyclooxygenase-2, CRP = C-reactive protein, DHA = docosahexaenoic acid, DPA = docosapentaenoic acid, EPA = Eicosapentaenoic acid, FAHFAs = fatty acyl esters of hydroxyl fatty acids, FAs = fatty acids, GABA = gamma-Aminobutyric acid, ICAMs = intercellular adhesion molecules, IL = interleukin, iNOS = inducible nitric oxide synthase, NSAIDs = non-steroidal anti-inflammatory drugs, PUFAs = polyunsaturated fatty acids, TNF = tumor necrosis factor, VCAMs = vascular cell adhesion molecules, ω-3 = Omega-3.
How to cite this article: Cardia L, Calapai F, Mondello C, Quattrone D, Elisa Sorbara E, Mannucci C, Calapai G, Mondello E. Clinical use of omega-3 fatty acids in migraine: A narrative review. Medicine. 2020;99:42(e22253).
The authors wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
References
- [1].Tajmirriahi M, Sohelipour M, Basiri K, et al. The effects of sodium valproate with fish oil supplementation or alone in migraine prevention: a randomized single-blind clinical trial. Iran J Neurol 2012;11:21–4. [PMC free article] [PubMed] [Google Scholar]
- [2].Saravanan P, Davidson NC. The role of omega-3 fatty acids in primary prevention of coronary artery disease and in atrial fibrillation is controversial. J Am Coll Cardiol 2010;55:410–1. (author reply 411–2). [DOI] [PubMed] [Google Scholar]
- [3].Wall R, Ross RP, Fitzgerald L GF, et al. Fatty acids from fish: the anti-inflammatory potential of long-chain omega-3 fatty acids. Nutr Rev 2010;68:280–9. [DOI] [PubMed] [Google Scholar]
- [4].Lauritzen I, Blondeau N, Heurteaux C, et al. Polyunsaturated fatty acids are potent neuroprotectors. EMBO J 2000;19:1784–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Alemany R, Perona JS, Sánchez-Dominguez JM, et al. G protein-coupled receptor systems and their lipid environment in health disorders during aging. Biochim Biophys Acta 2007;1768:964–75. [DOI] [PubMed] [Google Scholar]
- [6].Bazan NG. Omega-3 fatty acids, pro-inflammatory signaling and neuroprotection. Curr Opin Clin Nutr Metab Care 2007;10:136–41. [DOI] [PubMed] [Google Scholar]
- [7].Kuda O, Brezinova M, Rombaldova M, et al. Docosahexaenoic acid-derived fatty acid esters of hydroxy fatty acids (FAHFAs) with anti-inflammatory properties. Diabetes 2016;65:2580–90. [DOI] [PubMed] [Google Scholar]
- [8].Forman MS, Lal D, Zhang B, et al. Transgenic mouse model of tau pathology in astrocytes leading to nervous system degeneration. J Neurosci 2005;25:3539–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Hasadsri L, Wang BH, Lee JV, et al. Omega-3 fatty acids as a putative treatment for traumatic brain injury. J Neurotrauma 2013;30:897–906. [DOI] [PubMed] [Google Scholar]
- [10].Abdelmoaty S, Wigerblad G, Bas DB, et al. Spinal actions of lipoxin A4 and 17(R)-resolvin D1 attenuate inflammation-induced mechanical hypersensitivity and spinal TNF release. PLoS One 2014;8:e75543.doi: 10.1371/journal.pone.0075543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Brenna JT, Carlson SE. Docosahexaenoic acid and human brain development: evidence that a dietary supply is needed for optimal development. J Hum Evol 2014;77:99–106. [DOI] [PubMed] [Google Scholar]
- [12].Simopoulos AP. Omega-3 fatty acids in inflammation and autoimmune diseases. J Am Coll Nutr 2002;21:495–505. [DOI] [PubMed] [Google Scholar]
- [13].Calder PC. Dietary modification of inflammation with lipids. Proc Nutr Soc 2002;61:345–55. [DOI] [PubMed] [Google Scholar]
- [14].Ramsden CE, Faurot KR, Zamora D, et al. Targeted alteration of dietary n-3 and n-6 fatty acids for the treatment of chronic headaches: a randomized trial. Pain 2013;154:2441–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Harel Z, Gascon G, Riggs S, et al. Supplementation with omega-3 polyunsaturated fatty acids in the management of recurrent migraines in adolescents. J Adolesc Health 2002;31:154–61. [DOI] [PubMed] [Google Scholar]
- [16].Sastry PS. Lipids of nervous tissue: composition and metabolism. Prog Lipid Res 1985;24:69–176. [DOI] [PubMed] [Google Scholar]
- [17].Soveyd N, Abdolahi M, Bitarafan S, et al. Molecular mechanisms of omega-3 fatty acids in the migraine headache. Iran J Neurol 2017;16:210–7. [PMC free article] [PubMed] [Google Scholar]
- [18].Sekiya M, Yahagi N, Matsuzaka T, et al. Polyunsaturated fatty acids ameliorate hepatic steatosis in obese mice by SREBP-1 suppression. Hepatology 2003;38:1529–39. [DOI] [PubMed] [Google Scholar]
- [19].Richardson AJ, Puri BK. A randomized double-blind, placebo-controlled study of the effects of supplementation with highly unsaturated fatty acids on ADHD-related symptoms in children with specific learning difficulties, Prog. Prog Neuropsychopharmacol Biol Psychiatry 2002;26:233–9. [DOI] [PubMed] [Google Scholar]
- [20].Jicha GA, Markesbery WR. Omega-3 fatty acids: potential role in the management of early Alzheimer's disease. Clin Interv Aging 2010;5:45–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Logan AC. Neurobehavioral aspects of omega-3 fatty acids: possible mechanisms and therapeutic value inmajor depression. Altern Med Rev 2003;8:410–25. [PubMed] [Google Scholar]
- [22].Palacios-Pelaez R, Lukiw WJ, Bazan NG. Omega-3 essential fatty acids modulate initiation and progression of neurodegenerative disease. Mol Neurobiol 2010;41:367–74. [DOI] [PubMed] [Google Scholar]
- [23].Norouzi Javidan A, Sabour H, Latifi S, et al. Does consumption of polyunsaturated fatty acids influence on neurorehabilitation in traumatic spinal cord-injured individuals? A double-blinded clinical trial. Spinal Cord 2014;52:378–82. [DOI] [PubMed] [Google Scholar]
- [24].Michael-Titus AT. Omega-3 fatty acids: their neuroprotective and regenerative potential in traumatic neurological injury. Clin Lipidology 2009;4:343–53. [Google Scholar]
- [25].Ziegler D, Ametov A, Barinov A, et al. Oral treatment with alpha-lipoic acid improves symptomatic diabetic polyneuropathy: the SYDNEY 2 trial. Diabetes Care 2006;29:2365–70. [DOI] [PubMed] [Google Scholar]
- [26].Ko GD, Nowacki NB, Arseneau L, et al. Omega-3 fatty acids for neuropathic pain: case series. Clin J Pain 2010;26:168–72. [DOI] [PubMed] [Google Scholar]
- [27].Ramsden CE, Faurot KR, Zamora D, et al. Targeted alterations in dietary n-3 and n-6 fatty acids improve life functioning and reduce psychological distress among patients with chronic headache: a secondary analysis of a randomized trial. Pain 2015;156:587–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Tietjen GE. Migraine as a systemic vasculopathy. Cephalalgia 2009;29:987–96. [DOI] [PubMed] [Google Scholar]
- [29].Andreou AP, Edvinsson L. Mechanisms of migraine as a chronic evolutive condition. J Headache Pain 2019;20:117.doi:10.1186/s10194-019-1066-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Abdolahi M, Mohammadzadeh Honarvar N, Tafakhori A, et al. The combined effects of omega3 fatty acids and nanocurcumin supplementation on gene expression and serum levels of some inflammatory and endothelial factors in migraine patients: study protocol for a randomized controlled trial. Int J Pharm Sci Invent 2016;5:42–6. [Google Scholar]
- [31].Mulder EJ, Van Baal C, Gaist D, et al. Genetic and environmental influences on migraine: a twin study across six countries. Twin Res 2003;6:422–31. [DOI] [PubMed] [Google Scholar]
- [32].Malhotra R. Understanding migraine: potential role of neurogenic inflammation. Ann Indian Acad Neurol 2016;19:175–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Fidan I, Yüksel S, Ýmir T, et al. The importance of cytokines, chemokines and nitric oxide in pathophysiology of migraine. J Neuroimmunol 2006;171:184–8. [DOI] [PubMed] [Google Scholar]
- [34].Longoni M, Ferrarese C. Inflammation and excitotoxicity: role in migraine pathogenesis. Neurol Sci 2006;27: suppl: S107–10. [DOI] [PubMed] [Google Scholar]
- [35].D’Andrea G, Leon A. Pathogenesis of migraine: from neurotransmitters to neuromodulators and beyond. Neurol Sci 2010;31: suppl: S1–7. [DOI] [PubMed] [Google Scholar]
- [36].Hamed SA. The vascular risk associations with migraine: relation to migraine susceptibility and progression. Atherosclerosis 2009;205:15–22. [DOI] [PubMed] [Google Scholar]
- [37].DosSantos MF, Holanda-Afonso RC, Lima RL, et al. The role of the blood-brain barrier in the development and treatment of migraine and other pain disorders. Front Cell Neurosci 2014;8:302.doi:10.3389/fncel.2014.00302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Saegusa H, Tanabe T. N-typevoltage-dependentCa2+ channel in non excitable microglial cells in mice is involved in the pathophysiology of neuropathic pain. Biochem Biophys Res Commun 2014;450:142–7. [DOI] [PubMed] [Google Scholar]
- [39].Abdolahi M, Jafarieh A, Sarraf P, et al. The neuromodulatory effects of ω-3 fatty acids and nano-curcumin on the COX-2/iNOS network in migraines: A Clinical Trial Study from Gene Expression to Clinical Symptoms. Endocr Metab Immune Disord Drug Targets 2019;19:874–84. [DOI] [PubMed] [Google Scholar]
- [40].Haut SR, Bigal ME, Lipton RB. Chronic disorders with episodic manifestations: focus on epilepsy and migraine. Lancet Neurol 2006;5:148–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Stovner Lj, Hagen K, Jensen R, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia 2007;27:193–210. [DOI] [PubMed] [Google Scholar]
- [42].Ayatollahi Seyyed Mohammad T, Sahebi L, BorhaniHaghighi A. Epidemiologic and clinical characteristics of migraine and tension-type headaches among hospitals staffs of Shiraz (Iran). ActaMedicaIranica 2009;47:115–20. [Google Scholar]
- [43].Lewis D, Winner P, Saper J, et al. Randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of topiramate for migraine prevention in pediatric subjects 12 to 17 years of age. Pediatrics 2009;123:924–34. [DOI] [PubMed] [Google Scholar]
- [44].Lewis DW, Winner P. The pharmacological treatment options for pediatric migraine: an evidence-based appraisal. NeuroRx 2006;3:181–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Pothmann R, Danesch U. Migraine prevention in children and adolescents: results of an open study with a special butterbur root extract. Headache 2005;45:196–203. [DOI] [PubMed] [Google Scholar]
- [46].Larsson B. The role of psychosocial, health behavioral and medical factors in adolescent headache. Dev Med Child Neurol 1988;30:616–25. [DOI] [PubMed] [Google Scholar]
- [47].Gerring ZF, Powell JE, Montgomery GW, et al. Genome-wide analysis of blood gene expression in migraine implicates immune-inflammatory pathways. Cephalalgia 2018;38:292–303. [DOI] [PubMed] [Google Scholar]
- [48].Levy D. Migraine pain and nociceptor activation – where do we stand? Headache 2010;50:909–16. [DOI] [PubMed] [Google Scholar]
- [49].Vigh L, Escribá PV, Sonnleitner A, et al. The significance of lipid composition for membrane activity: new concepts and ways of assessing function. Prog Lipid Res 2005;44:303–44. [DOI] [PubMed] [Google Scholar]
- [50].Casas J, Ibarguren M, Álvarez R, et al. G protein-membrane interactions II: Effect of G protein-linked lipids on membrane structure and G protein-membrane interactions. Biochim Biophys Acta Biomembr 2017;1859:1526–35. [DOI] [PubMed] [Google Scholar]
- [51].Escribá PV, Wedegaertner PB, Goñi FM, et al. Lipid-protein interactions in GPCR-associated signaling. Biochim Biophys Acta 2007;1768:836–52. [DOI] [PubMed] [Google Scholar]
- [52].Stender S, Dyerberg J. Influence of trans fatty acids on health. Ann Nutr Metab 2004;48:61–6. [DOI] [PubMed] [Google Scholar]
- [53].Diep QN, Touyz RM, Schiffrin EL. Docosahexaenoic acid, a peroxisome proliferator-activated receptor-alpha ligand, induces apoptosis in vascular smooth muscle cells by stimulation of p38 mitogen-activated protein kinase. Hypertension 2000;36:851–5. [DOI] [PubMed] [Google Scholar]
- [54].Zúñiga J, Cancino M, Medina F, et al. N-3 PUFA supplementation triggers PPAR-α activation and PPAR-α/NF-κB interaction: anti-inflammatory implications in liver ischemia-reperfusion injury. PLoS One 2011;6:e28502.doi:10.1371/journal.pone.0028502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Chiang N, Serhan CN. Structural elucidation and physiologic functions of specialized pro-resolving mediators and their receptors. Mol Aspects Med 2017;58:114–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [56].Clària J, Nguyen BT, Madenci AL, et al. Diversity of lipid mediators in human adipose tissue depots. Am J Physiol Cell Physiol 2013;304:C1141–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [57].Galano JM, Lee JC, Gladine C, et al. Non-enzymatic cyclic oxygenated metabolites of adrenic, docosahexaenoic, eicosapentaenoic and α-linolenic acids; bioactivities and potential use as biomarkers. Biochim Biophys Acta 2015;1851:446–55. [DOI] [PubMed] [Google Scholar]
- [58].Kuda O. Bioactive metabolites of docosahexaenoic acid. Biochimie 2017;136:12–20. [DOI] [PubMed] [Google Scholar]
- [59].Calder PC. Long chain fatty acids and gene expression in inflammation and immunity. Curr Opin Clin Nutr Metab Care 2013;16:425–33. [DOI] [PubMed] [Google Scholar]
- [60].Calder PC. n-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases. Am J Clin Nutr 2006;83: 6 suppl: 1505S–19S. [DOI] [PubMed] [Google Scholar]
- [61].Abdolahi M, Tafakhori A, Togha M, et al. The synergistic effects of omega-3 fatty acids and nano-curcumin supplementation on tumor necrosis factor (TNF)-alpha gene expression and serum level in migraine patients. Immunogenetics 2017;69:371–8. [DOI] [PubMed] [Google Scholar]
- [62].Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009;339:b2700.doi: 10.1136/bmj.b2700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [63].Sun-Edelstein C, Mauskop A. Foods and supplements in the management of migraine headaches. Clin J Pain 2009;25:446–52. [DOI] [PubMed] [Google Scholar]
- [64].Damen L, Bruijn JK, Verhagen AP, et al. Symptomatic treatment of migraine in children: a systematic review of medication trials. Pediatrics 2005;116:e295–302. [DOI] [PubMed] [Google Scholar]
- [65].Pradalier A, Bakouche P, Baudesson G, et al. Failure of omega-3 polyunsaturated fatty acids in prevention of migraine: a double-blind study versus placebo. Cephalalgia 2001;21:818–22. [DOI] [PubMed] [Google Scholar]
- [66].Soares AA, Louçana PMC, Nasi EP, et al. A double- blind, randomized, and placebo-controlled clinical trial with omega-3 polyunsaturated fatty acids (OPFA ω-3) for the prevention of migraine in chronic migraine patients using amitriptyline. Nutr Neurosci 2018;21:219–23. [DOI] [PubMed] [Google Scholar]
- [67].Brietzke E, Mansur RB, Grassi-Oliveira R, et al. Inflammatory cytokines as an underlying mechanism of the comorbidity between bipolar disorder and migraine. Med Hypotheses 2012;78:601–5. [DOI] [PubMed] [Google Scholar]
- [68].Tonekaboni SH, Ghazavi A, Fayyazi A, et al. Prophylaxis of childhood migraine: topiramate versus propranolol. Iran J Child Neurol 2013;7:9–14. winter. [PMC free article] [PubMed] [Google Scholar]
- [69].Olness K, MacDonald JT, Uden DL. Comparison of self-hypnosis and propranolol in the treatment of juvenile classic migraine. Pediatrics 1987;79:593–7. [PubMed] [Google Scholar]
- [70].Ziegler DK, Hurwitz A, Preskorn S, et al. Propranolol and amitriptyline in prophylaxis of migraine. Pharmacokinetic and therapeutic effects. Arch Neurol 1993;50:825–30. [DOI] [PubMed] [Google Scholar]
- [71].Fayyazi A, Khajeh A, Ghazavi A, et al. Omega 3 in childhood migraines: a double blind randomized clinical trial. Iran J Child Neurol 2016;10:9–13. Winter. [PMC free article] [PubMed] [Google Scholar]
- [72].Saw CLL, Huang Y, Kong A-N. Synergistic anti-inflammatory effects of low doses of curcumin in combination with polyunsaturated fatty acids: docosahexaenoic acid or eicosapentaenoic acid. Biochem Pharmacol 2010;79:421–30. [DOI] [PubMed] [Google Scholar]
- [73].Mittal N, Joshi R, Hota D, et al. Evaluation of antihyperalgesic effect of curcumin on formalin-induced orofacial pain in rat. Phytother Res 2009;23:507–12. [DOI] [PubMed] [Google Scholar]
- [74].Abdolahi M, Sarraf P, Javanbakht MH, et al. A Novel Combination of ω-3 fatty acids and nano-curcumin modulates interleukin-6 gene expression and high sensitivity c-reactive protein serum levels in patients with migraine: a randomized Clinical Trial Study. CNS Neurol Disord Drug Targets 2018;17:430–8. [DOI] [PubMed] [Google Scholar]
- [75].Ramos TN, Bullard DC, Barnum SR. ICAM-1: isoforms and phenotypes. J Immunol 2014;192:4469–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [76].Soveyd N, Abdolahi M, Djalali M, et al. The combined effects of ω -3 fatty acids and nano-curcumin supplementation on intercellular adhesion molecule-1 (ICAM-1) gene expression and serum levels in migraine patients. CNS Neurol Disord Drug Targets 2018;16:1120–6. [DOI] [PubMed] [Google Scholar]