

1. Introduction
Current diagnostic systems such as the Diagnostic and Statistical Manual (DSM) and International Classification of Diseases (ICD) are based on polythetic diagnostic categories, meaning that each psychiatric disorder is defined by multiple symptoms, not all of which need to be present in order for a diagnosis to be made (Olbert et al., 2014). While the current systems have improved upon previous systems, and have been useful for both clinical and research purposes, there are a number of concerns with this type of diagnostic system. First, it allows for vast heterogeneity within any given psychiatric diagnosis. In fact, it is possible for two individuals with only a couple or no overlapping symptoms to both meet criteria for the same psychiatric disorder (Krueger & Bezdjian, 2009). In addition to this, there is also significant symptom overlap across many psychiatric diagnoses, meaning it is possible for two individuals who share several symptoms in common to be diagnosed with two separate psychiatric disorders (Gros et al., 2012). This contributes to significant comorbidity between psychiatric disorders, such that many individuals meet criteria for multiple diagnoses at once (Maj, 2005). Finally, the categorical nature of the current diagnostic systems means that arbitrary cutoffs have been created for the number of symptoms required to meet diagnosis of disorders, and the potential impact of sub-syndromal levels of symptoms have been problematically deemphasized (Krueger & Bezdjian, 2009). Additionally, despite the growing body of literature examining the genetic and neurobiological correlates of psychiatrically relevant phenomena, current diagnostic systems have not incorporated this literature, which could improve the identification of biologically distinct forms of psychopathology or provide a source of objective diagnostic criteria.
The NIMH Research Domain Criteria (RDoC) initiative addresses these issues by providing a dimensional framework to bridge the gap between genetics and neurobiology on one hand and behavior and psychopathology on the other. RDoC seeks to promote research that examines neurobiological and behavioral dimensions that cut across the current diagnostic categories, looking at the full range of functioning within these dimensions to understand both typical and pathological functioning, in order to improve diagnosis and treatment (Cuthbert, 2014). RDoC identifies (thus far) five domains of functioning for which there are known neurobiological correlates, and which are thought to be relevant to different forms of psychopathology: Positive Valence Systems, Negative Valence Systems, Cognitive Systems, Systems for Social Processes, and Arousal/Modulatory Systems (NIMH, 2013).
The RDoC Positive Valence Systems was initially made up of 5 constructs related to reward processes, one of which was Initial Responsiveness to Reward Attainment (IRRA) – the focus of the present study. While the present study was designed based on the original structure of the PVS, this domain has since been revised to be more straightforward, and to better reflect recent research findings. The revised structure consists of three constructs – reward responsiveness, reward learning, and reward valuation – each of which contains three subconstructs. Within this new structure, IRRA is a subconstruct under reward responsiveness. Reward responsiveness refers to processes governing hedonic response to reward. IRRA refers specifically to the processes involved in response to the initial presentation of a positive reinforcer (as opposed to processes involved response to anticipated reward, or repeated receipt of reward, which are captured by the other two subconstructs of reward responsiveness). The RDoC work group suggested several methods for measuring IRRA, including self-report questionnaires such as the Positive and Negative Affect Schedule (PANAS) or the Temporal Experience of Pleasure Scale’s (TEPS) Consummatory subscale, and behavioral paradigms such as the Monetary Incentive Delay (MID) task, gambling tasks, or taste reactivity measures (NIMH, 2013).
Previous research on IRRA has found relationships between IRRA and several different areas of psychopathology. For example, one study using fMRI to examine reward responsiveness in boys with Attention-Deficit/Hyperactivity Disorder (ADHD) and Autism Spectrum Disorder (ASD) found hyperactivation in response to social reward among the participants with ADHD and hypoactivation among participants with ASD, revealing that IRRA may be a relevant construct for understanding ADHD and ASD (Kohl et al., 2014). Several studies have examined the relationship between IRRA and depression, finding that depression is related to reduced responsiveness to reward (Henriques & Davidson, 2000; Bogdan & Pizzagalli, 2006; McFarland & Klein, 2008; Pizzagalli et al., 2008; Bress et al., 2013). Specifically, reduced IRRA is associated with anhedonia, a primary symptom of depression (Pizzagalli et al., 2008). In a longitudinal study, IRRA significantly predicted the future onset of depression (Bress et al., 2013). Additionally, one study found that acute stress predicted impaired reward responsiveness, which in turn predicted depressive symptoms (Bogdan & Pizzagalli, 2006). Reduced responsiveness to reward is also seen in smokers when abstaining from smoking (Al-Adawi & Powell, 1997; Powell et al., 2002) and among patients with chronic pain (Elvemo et al., 2015) and fatigue (Boksem et al., 2006; Pardini et al., 2012). In contrast, hypersensitivity to reward has been associated with overeating in both children and adults and predicts obesity among children (Van den Berg et al., 2011) and binge eating disorder among adults (Schag et al., 2013). The present study aims to expand upon this previous research by examining IRRA in relation to a wide range of different areas of psychopathology, all within the same study.
Previous research has reported sex differences in IRRA, although this issue has not been comprehensively addressed. Females have been found to score higher on reward responsiveness measures than males (Carver & White, 1994; Gard et al., 2006; Hamilton et al., 2015). A few studies suggest that males and females experience different changes in reward responsiveness in response to stress, with females displaying decreased responsiveness and males displaying increased responsiveness to reward under stress (Ossewaarde et al., 2011; Lighthall et al., 2011). These differences might result in different clinical presentations for males and females. The present study aims to further expand upon the previous research on sex differences in relation to IRRA, by examining how sex might moderate the relationship between IRRA and different forms of psychopathology.
There is limited research related to the impact of race and ethnicity on IRRA. However, research examining other areas of reward functioning (e.g. delaying reward) suggests there may be differences in reward processes based on race (Andrade & Petry, 2014). Thus, exploring how ancestry might moderate the relationship between IRRA and different forms of psychopathology is also important to understanding how IRRA relates to psychopathology overall.
In summary, the current study aimed to (1) clarify the associations of IRRA with a broad range of psychopathology and impairment in both children and adults, and (2) examine the potential effects of sex and ancestry on the association between IRRA and psychopathology. This study takes a novel approach by examining the relationship between IRRA and the full range of psychopathology within one study, utilizing similar analyses for adults and children. It is also the first study to our knowledge to examine sex and ancestry as moderators of the relationship between IRRA and psychopathology. Finally, it is the first study to our knowledge to examine familial relationships in IRRA. It is hypothesized that IRRA will be associated with ADHD, depressive, and somatic symptomology, as well as substance use – as previous studies have found relationships between IRRA and these specific areas of psychopathology. Given age of onset differences across different areas of psychopathology, relationships between IRRA and some areas of psychopathology may be apparent in adults, but not in children. Given previous findings that males and females show different patterns of IRRA under stress, it is hypothesized that sex may impact the relationship between IRRA and psychopathology (e.g. IRRA might be associated with elevations in different areas of psychopathology for males versus females). Given the limited previous research examining ancestry and IRRA, no specific hypotheses are made regarding the impact of ancestry on the relationship between IRRA and psychopathology.
2. Methods
2.1. Participants
A total of 1127 children (356 siblings) and 1018 parents participated in this study. All children were between the ages of 6 and 12 (mean age = 8.8 years, SD = 2.1), and their parents were between the ages of 22 and 59 (mean age = 37.7, SD = 6.9). While there were relatively equivalent numbers of female and male children (47% vs. 53%), significantly more of the participating parents were female than male (69% vs. 31%). Participants were diverse in their ancestral backgrounds, with 68% of parents identifying as white, 22% black, and 10% other or multiple races, and 59% of children identifying as white, 22% black, and 19% other or multiple races. Additionally, 7% of parents and 12% of children were Hispanic. Parents reported both for themselves and for their children whether they had ever sought mental health care for emotional or behavioral problems or had received a diagnosis of such, with 41% of children and 45% of parents reporting such psychiatric history. See Table 1 for more demographic information about the participants in this study.
Table 1.
Participant Demographics
| Demographics | Percentage |
|---|---|
| Parents (N = 1018) | |
| Age (mean(SD)) | 37.7 (6.9) |
| Sex (% female) | 69% |
| Race (% white) | 68% |
| (% black) | 22% |
| (% two or more races) | 3% |
| (% other) | 7% |
| Ethnicity (% Hispanic) | 7% |
| Psychiatric (% psychiatric history) | 45% |
| Shipley IQ (mean(SD)) | 94 (18) |
| Education (% less than HS) | 10% |
| (% HS diploma) | 22% |
| (% some college/post secondary non-degree) | 20% |
| (% associates degree) | 13% |
| (% bachelors degree) | 18% |
| (% masters/doctoral/professional degree) | 17% |
| Employment (% unemployed) | 19% |
| (% employed part time) | 15% |
| (% employed full time) | 52% |
| (% homemaker full time) | 8% |
| (% retired/disability/other) | 6% |
| Marital Status (% married) | 55% |
| (% never married) | 27% |
| (% not married, living together) | 3% |
| (% divorced/separated/widowed) | 15% |
| Income (% < 10,000) | 6% |
| (% 10,001 – 20,000) | 11% |
| (% 20,001 – 30,000) | 10% |
| (% 30,001 – 40,000) | 7% |
| (% 40,001 – 50,000) | 6% |
| (% 50,001 – 75,000) | 11% |
| (% 75,001 – 100,000) | 11% |
| (% > 100,000) | 13% |
| (% would rather not say) | 25% |
| IRRA – TEPS-C | 36.12 (7.27) |
| Children (N = 1127) | |
| Age (mean(SD)) | 8.8 (2.1) |
| Sex (% female) | 47% |
| Race (% white) | 59% |
| (% black) | 22% |
| (% two or more races) | 13% |
| (% other) | 6% |
| Ethnicity (% Hispanic) | 12% |
| Psychiatric (% psychiatric history) | 41% |
| Shipley IQ mean(SD) | 100 (17) |
| IRRA - EPSC | 2.35 (.37) |
2.2. Procedure
Participants were recruited from a variety of sources within the greater Syracuse community, including the Child and Adolescent Psychiatry Clinic (CAPC) at SUNY Upstate Medical University and child psychiatrists and mental health clinicians working in private practice in the community, as well as from community events (local fairs, festivals, etc.). We excluded adopted children, and children with any of the following: sensorimotor disabilities, a diagnosed neurological condition, a history of head injury with documented loss of consciousness lasting more than 10 minutes, an uncontrolled medical condition, an IQ below 80 as reported by parents, or an inability to understand the English language. Exclusion criteria were the same for parents, with the exception of the adoption criterion and two additional criteria: 1) parents who did not have the ability to independently complete study tasks; and 2) women who were pregnant or gave birth within six months of the study visit. Informed consent was obtained from all parents and assent was given by all children after the nature of the procedures had been fully explained upon arrival for their study visit. Study visits were approximately three hours in length, and involved the completion of a variety of computerized inventories and behavioral paradigms. The study was carried out in accordance with the Declaration of Helsinki, and the study design was approved by the Institutional Review Board at SUNY Upstate Medical University.
2.3. Measures
2.3.1. Temporal experience of pleasure scale.
The Temporal Experience of Pleasure Scale (TEPS) was developed by Gard and colleagues to measure anticipatory and consummatory experiences of pleasure (Gard et al., 2006). The full scale contains 18 items, and has been found to have strong internal consistency (Cronbach’s alpha = .81). The consummatory subscale, which is made up of eight items, was used in this study as a measure of initial responsiveness to reward attainment (IRRA) in adult participants. Participants were asked to respond to each item on a six-point scale from very false to very true. The consummatory subscale was sum-scored, with possible scores ranging from 8 to 48, and with higher scores indicating greater consummatory pleasure and greater initial responsiveness to reward attainment. The Cronbach’s alpha for the TEPS consummatory subscale was also calculated for the present study, and was found to be acceptable (Cronbach’s alpha = .72).
2.3.2. Experienced pleasure scale.
The Experienced Pleasure Scale for Children (EPSC) was used to measure initial responsiveness to reward attainment in child participants. This 39-item scale was modified from the Pleasure Scale for Children (PSC) developed by Kazdin (1989), for the purposes of this study. The original scale asked participants to respond to hypothetical scenarios about how happy each item would make them on a three-point scale, (1) wouldn’t matter (2) happy (3) very happy, and has been found to have strong internal consistency (Cronbach’s alpha = .92). In order to measure actual rather than hypothetical responses to these scenarios, the EPSC asks participants to respond to a Yes/No item asking if they have personally experienced each scenario, and then asks about their response only to those items they reported experiencing. Participants endorsed experiencing an average of 19 out of 39 items (SD = 8.2). A mean score for each participant was created using only the items that the participant endorsed experiencing. Correlations between each item of the EPSC and the overall EPSC mean score were all greater than .30. Additionally, number of endorsed items was positively correlated with mean EPSC scores (r = .17, p < .001). There were no statistically significant differences in mean EPSC scores based on gender, race, or ethnicity.
2.3.3. Adult self report.
The Adult Self Report (ASR) was used to measure psychopathology and adaptive functioning in adult participants. This 126-item self-report measure is well-validated and widely used in clinical practice to assess symptoms of psychopathology and adaptive functioning in individuals ages 18 to 59 years (Achenbach & Rescorla, 2003). Participants were asked to respond to each item on a three-point scale from not true to very true/often true. The ASR provides T-scores for 7 syndrome scales (anxious/depressed, withdrawn, somatic complaints, thought problems, attention problems, aggressive behavior, rule-breaking behavior), 6 scales specific to symptoms of DSM diagnoses (affective disorders, anxiety disorders, somatic problems, avoidant personality features, attention/deficit hyperactivity problems, antisocial personality features), 3 composite scores (internalizing composite, externalizing composite, total problems composite) and 4 scales assessing substance use (tobacco, alcohol, recreational drugs, substance use composite). An adaptability composite is also provided along with subscale scores for friendships, spouse, family, and employment.
2.3.4. Child behavior checklist.
The Child Behavior Checklist (CBCL) was used to measure psychopathology in children. This 113-item parent-report measure is well-validated and widely used in clinical practice to assess emotional and behavioral functioning in children ages 6 to 18 years (Achenbach, 1991). Parents were asked to respond to each item on a three-point scale from not true to very true/often true, indicating how true the item is for their child. The CBCL provides T-scores for 8 syndrome scales (anxious/depressed, withdrawn/depressed, somatic complaints, social problems, thought problems, attention problems, rule-breaking behavior, aggressive behavior), 9 DSM-oriented scales (Affective problems, anxiety problems, somatic problems, attention deficit/hyperactivity problems, oppositional defiant problems, conduct problems, sluggish cognitive tempo, obsessive compulsive problems, post-traumatic stress problems), and 3 composite scores (internalizing composite, externalizing composite, total problems composite). Higher scores indicate greater pathology.
2.3.5. Social adjustment inventory for children and adolescents.
The Social Adjustment Inventory for Children and Adolescents (SAICA) was used to measure children’s functioning across several domains. This 78-item semi-structured interview was designed to assess social functioning in children ages 6 to 18 years (John et al., 1987). Responses were recorded on a four-point scale, with higher scores indicating greater impairment. Mean scores were created for four domains of functioning: current school functioning, spare time activities, peer functioning, and current home behavior. An overall adaptive functioning score was calculated by taking the mean of these subscale scores. Higher scores indicate greater impairment in functioning.
2.3.6. Shipley-2.
The Shipley-2 is a widely used measure of general intellectual functioning (Shipley, Gruber, Martin, & Klein, 2009). The Shipley-2 was administered to both children and adults in the present study. The present study utilized a single summary score estimating overall IQ, calculated from performance on a vocabulary task and an abstraction task.
2.4. Statistical analyses
Statistical analyses were conducted using SPSS version 23. Preliminary analyses were conducted to examine the relationship between various demographic variables and IRRA in both adults and children. A series of negative binomial regression models were conducted to examine the relationship between IRRA and psychopathology in adults and children. We used negative binomial regression because our dependent variables were count variables truncated at zero leading to markedly non-normal distributions. Main effects of IRRA, sex, race, and ethnicity were tested, as well as interaction effects of IRRA and sex, IRRA and race, and IRRA and ethnicity. All adult models covaried for demographic variables including age, IQ, education, employment, income, and marital status. All child models covaried for parent income and education. Additional GLM models were conducted to examine the relationship between IRRA and adaptive functioning in both children and adults. Robust standard errors were used across all models, in order to account for non-independence in the data (i.e., familial relationships). All continuous model variables were mean-centered, and all categorical variables were dummy coded. When interpreting findings, specific components of interactions were only interpreted if the overall interaction effect was significant.
Multiple imputation was utilized to handle missing data on adult income, as a large number of participants (25%) chose not to report their household income. Ten imputations were conducted. Several demographic variables including education, employment, marital status, age, IQ, ancestry, and sex, were used to predict income in the imputation procedure. When modeled together, these variables explained a large proportion of the variance in income (r2 = .698). Multiple imputation was not used for any other variable, as missing data was not an issue for any other variables included in these analyses.
The Benjamini Hochberg False Discovery Rate method (Benjamini & Hochberg, 1995) was utilized to correct for multiple testing. This procedure is a recommended alternative to Bonferroni-type corrections, which are often criticized for increasing the likelihood of type-II errors, particularly when a large number of tests are conducted (Perneger, 1998). Adult and child findings were corrected separately. A tiered approach was utilized, by which main effects were corrected based on the total number of main effects tests (20 for adults and 22 for children), following which interaction effects were corrected based upon the total number of main effects tests plus the total number of interaction effects tests (60 for adults and 66 for children). A 5% false discovery rate was utilized for determining the significance of findings across both groups. P-values reported throughout the text are unadjusted p-values that have survived the BH FDR correction.
Finally, correlational analyses were conducted to analyze cross-generational relationships in IRRA. Correlation analyses were conducted for mother-child pairs and father-child pairs separately. For families with multiple children, the child utilized for these analyses was randomly assigned.
3. Results
3.1. Preliminary analyses
T-tests revealed significant differences in adult IRRA based on gender, with females displaying greater IRRA than males (t(1016) = 2.70, p = .007). ANOVA revealed significant differences in adult IRRA based on race, employment status, education, income, and marital status, with white participants displaying greater IRRA than black participants and participants of other races (F(2, 1015) = 32.99, p < .001), employed participants displaying greater IRRA than unemployed participants (F(4, 999) = 4.67, p = .001), participants with education beyond high school displaying greater IRRA than participants with a high school education or less (F(5, 1009) = 8.21, p < .001), participants with incomes greater than $50,000/year displaying greater IRRA than participants with incomes less than $20,000/year (F(7, 750) = 3.75, p = .001) married participants displaying greater IRRA than participants who were never married (F(3, 1011) = 10.71, p < .001). IQ was significantly positively correlated with IRRA for both adults and children (r = .267, p < .001 and r = .076, p = .02, respectively). Parent income and education were not significantly associated with child IRRA.
3.2. Adult adaptive functioning and psychopathology
We found significant associations between IRRA and both mean adaptive functioning and alcohol use problems in adults. There was a significant main effect of IRRA on mean adaptive functioning (β = 0.178, p < 0.001), such that greater IRRA was associated with better adaptive functioning in adults (Table 2). In other words, each standardized unit increase in IRRA was associated with a 0.18 standardized unit increase in adaptive functioning. Neither sex nor ancestry, nor their interactions with IRRA, were significantly associated with mean adaptive functioning. Neither IRRA, nor the interactions between IRRA and sex or ancestry, were found to be significantly associated with any area of psychopathology in adults.
3.3. Child adaptive functioning and psychopathology
IRRA was related to overall adaptive functioning in children and also to school, spare time, home, and peer functioning. The model predicting overall functioning found a significant main effect of IRRA (β = −.114, p < .001) (Table 4); greater IRRA was associated with less impaired overall functioning. In other words, each standardized unit increase in IRRA was associated with a 0.11 standardized unit decrease in functional impairment. The model predicting school functioning found significant main effects of both IRRA (β = −0.104, p = 0.001) and sex (β = .076, p = 0.001); greater IRRA was associated with less impaired school functioning, meaning each standardized unit increase in IRRA was associated with a 0.10 standardized unit decrease in school impairment, and male sex was associated with more impaired school functioning (Table 5). The model predicting spare time functioning found a significant main effect of IRRA (β = −0.122, p < .001) (Table 6); greater IRRA was associated with less impaired spare time functioning. In other words, each standardized unit increase in IRRA is associated with a 0.12 standardized unit decrease in spare-time functional impairment. The model predicting home functioning found a significant main effect of IRRA (β = −0.142, p < 0.001); greater IRRA was associated with less impaired home functioning (Table 7). In other words, each standardized unit increase in IRRA is associated with a 0.14 standardized unit decrease in home impairment. Finally, in the model predicting peer functioning, there was a significant main effect of IRRA (β = −0.08, p < .011); greater IRRA was associated with less impaired peer functioning (Table 8). In other words, each standardized unit increase in IRRA is associated with a 0.08 standardized unit decrease in social impairment.
3.4. Correlations between IRRA and Outcomes
To summarize the above analyses, IRRA was significantly associated with adaptive functioning in both adults and children, however there were no main effects of IRRA on psychopathology. See Figure 1 for a summary of the associations between IRRA and all areas of psychopathology and functioning examined in adults, and Figure 2 for a summary of the associations between IRRA and all areas of psychopathology and functioning examined in children.
Figure 1.
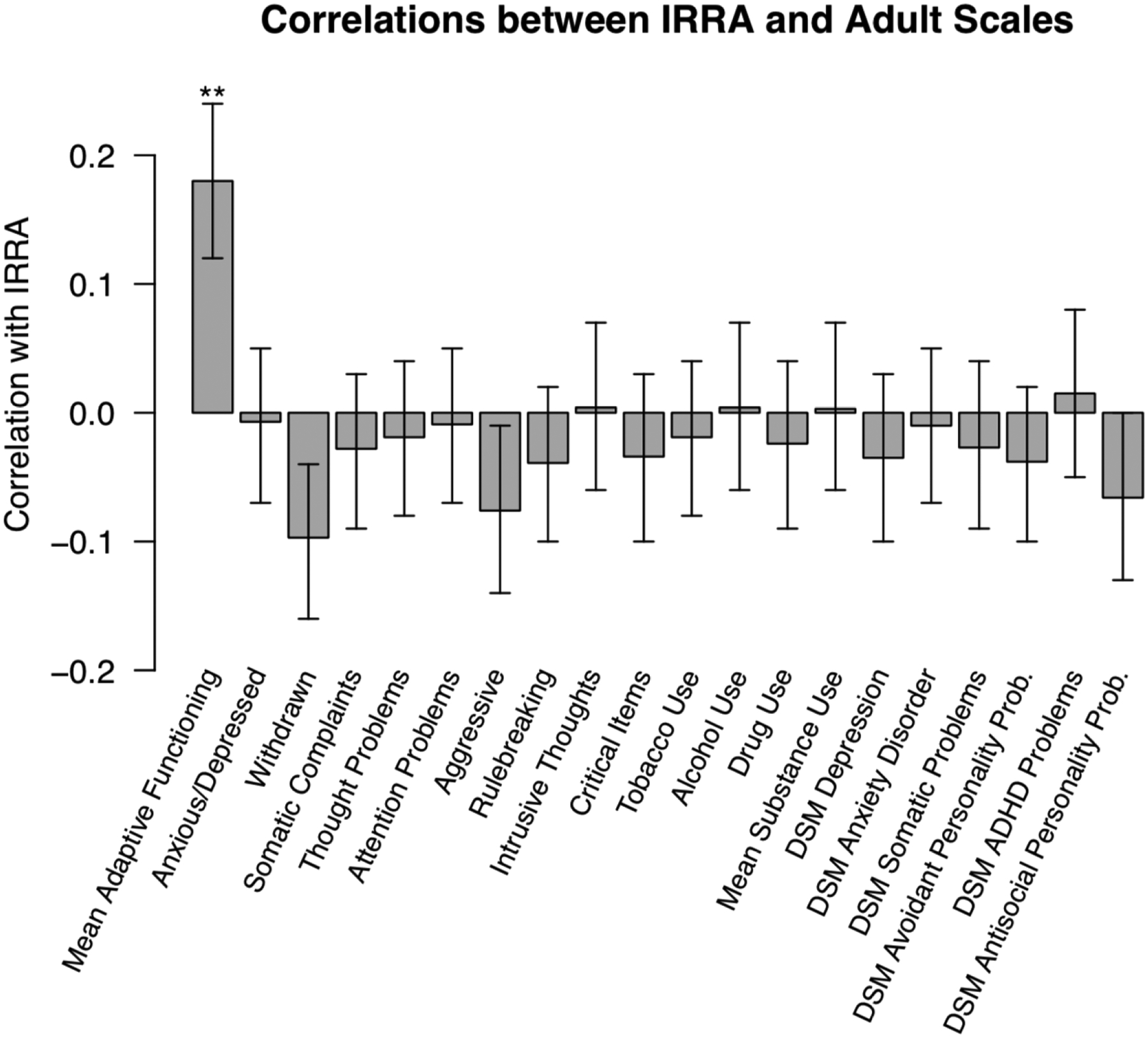
Pearson Correlations between IRRA as measured by the TEPS-C and all Adult Outcomes.
IRRA = Initial Responsiveness to Reward Attainment; TEP-C = Temporal Experience of Pleasure Scale – Consummatory. ** p < .01.
Figure 2.
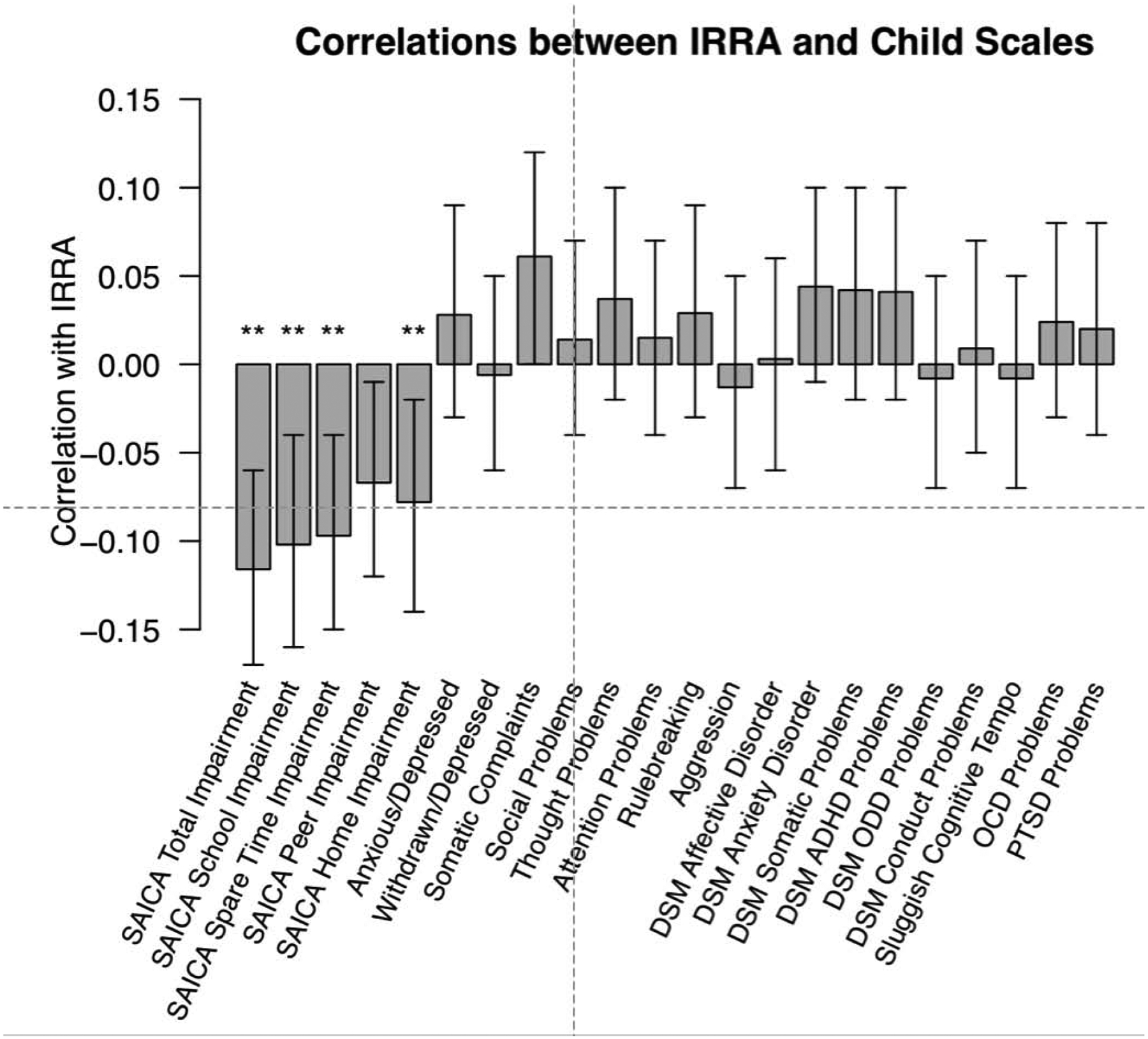
Pearson Correlations between IRRA as measured by the EPSC and all Child Outcomes.
IRRA = Initial Responsiveness to Reward Attainment; EPSC = Experienced Pleasure Scale; SAICA = Social Adjustment Inventory for Children and Adolescents. ** p < .01.
3.5. Familial relationships in IRRA
Correlational analyses examining cross-generational relationships in IRRA revealed nonsignificant correlations between both mother and child IRRA scores (r = .047, p = .230; N mother-child pairs = 665) and father and child IRRA scores (r = .092, p = .123; N father-child pairs = 284).
4. Discussion
The present study sought to examine the relationship between IRRA and psychopathology and functioning in adults and children, and to clarify the impact of ancestry and sex on these relationships. While we found significant relationships between IRRA and adaptive functioning in both adults and children, all of our tests of association with different areas of psychopathology were nonsignificant, and correlations between IRRA and outcomes were generally low. Given our large sample, we cannot attribute these nonsignificant findings to low statistical power. This suggests that IRRA does not have a large impact on a wide range of psychopathology in adults and children.
Our most consistent finding was the positive relationship between IRRA and adaptive functioning for both adults and children. For children, IRRA was related to positive school functioning, spare-time functioning, home functioning, and peer functioning. Although we did not assess mechanisms mediating the link between IRRA and adaptive functioning, several can be hypothesized. For example, someone who is not responsive to social reward may be withdrawn, and may struggle to develop and maintain interpersonal relationships, resulting in lower peer and overall functioning. In the same vein, someone who is not appropriately responsive to academic rewards may be less motivated to learn or perform well on tests, resulting in lower school functioning. The measure of IRRA used for children in the present study (the EPSC) included a wide variety of pleasurable or rewarding items, some social (e.g. related to spending time with friends or family), some performance-based (e.g. getting good grades or winning a contest), some related simply to gaining something desirable (e.g. receiving a gift) or other simple pleasures (e.g. eating your favorite food), and asked children how happy they would feel. The measure for adults (the TEPS-C) includes more simple pleasures. It makes sense that those who report experiencing more positive feelings from such things would generally be functioning well, as positive emotions enhance general well-being (Fredrickson & Joiner, 2002).
Although IRRA had limited associations with psychopathology in our study, other work has associated it with depression, substance use, and somatic problems in adults (Al-Adawi & Powell, 1997; Henriques & Davidson, 2000; Powell et al., 2002; Bogdan & Pizzagalli, 2006; Boksem et al., 2006; McFarland & Klein 2008; Pizzagalli et al., 2008; Pardini et al., 2012; Bress et al., 2013; Elvemo et al., 2015) and with ADHD in children (Kohl et al., 2014). The weaker relationship with psychopathology found in our study may be due to our use of self-report scales assessing psychopathology occurring in the past six months, rather than clinical interviews assessing lifetime and current symptoms.
While past studies have found a relationship between IRRA and substance use, specifically tobacco smoking (Al-Adawi & Powell, 1997; Powell et al., 2002), we did not find a significant relationship between IRRA and substance use of any kind. This may be explained by our method of measuring substance use, or our method of measuring IRRA, which differ from previous studies. Past studies have utilized behavioral paradigms to measure IRRA, while the present study utilizes self-report. Additionally, past studies have differentiated between smokers who have and have not recently abstained, and found important differences between these groups, which the present study was not able to capture using a self-report questionnaire about past 6-month substance use.
While past studies have found a relationship between reduced IRRA and depression (Henriques & Davidson, 2000; Bogdan & Pizzagalli, 2006; McFarland & Klein 2008; Pizzagalli et al., 2008; Bress et al., 2013), we did not find a significant relationship between IRRA and depressive symptoms in adults or children. This may be because the present study measured depressive symptoms over the past six months, while most past studies have measured depression in terms of having a current diagnosis of major depressive disorder. Additionally, given that depression is rare in children, and typically does not onset until adolescence or adulthood (Lewinsohn, Clarke, Seeley, & Rhode, 1994; Kessler et al., 2005), the lack of relationship between IRRA and depression is less surprising within our child sample and more surprising within the adult sample. Previous work suggests that reduced IRRA at one point in time may predict later depression (Bress et al., 2013); thus, future studies should utilize a longitudinal design to examine this relationship. We also found no relationship between IRRA and ADHD. Again, this could be because of the way IRRA was measured in this study compared to previous studies (self-report vs. behavioral paradigm or brain scan) or the way ADHD was measured (symptoms over last 6 months vs. current DSM diagnosis).
While past studies have found somatic complaints such as fatigue and chronic pain to be related to reduced IRRA (Boksem et al., 2006; Pardini et al., 2012; Elvemo et al., 2015), we did not find a significant relationship between IRRA and somatic symptoms in adults or children. This may be because the present study examined somatic complaints broadly, rather than specifically fatigue or chronic pain, as previous research has examined.
Surprisingly, although past studies have found that men and women experience different changes in IRRA under stress, with women experiencing reductions in IRRA and men experiencing increases in IRRA in response to stress (Ossewaarde et al., 2011; Lighthall et al., 2011), we found no significant interactions between IRRA and sex in predicting psychopathology under basal, non-stress conditions. Also surprisingly, there were no significant cross-generational relationships in IRRA, suggesting there may not be a familial link in reward responsiveness, or possibly that the measures used for children and adults were capturing different constructs. However, the consistent findings across children and adults in terms of relationship between IRRA and functional outcomes might provide evidence for construct consistency.
4.1. Limitations
The present study has several limitations. One limitation is the use of self-reported race and ethnicity, rather than genetic data, to understand ancestry. Race and ethnicity are complex concepts with both social and biological components. Thus, an individual’s self-reported racial or ethnic identity may not fully align with what their genetic data might say about their ancestral background. Additionally, while in research, race and ethnicity are thought of as distinct concepts, this might not be how participants understand their ancestral background. For example, Hispanic participants might not identify with any racial category, but only identify with their Hispanic ethnicity. Future research should examine the impact of self-identified ancestry compared to genetic ancestry to see if these discrete ways of defining one’s heritage differentially relate to IRRA and to associated outcomes.
In the present study the number of individuals who identified with racial backgrounds aside from White/Caucasian and Black/African American was very small. Thus, we were unable to examine the impact of these racial identities separately. In addition to this under-representation of some racial minorities, our adult sample was disproportionately female. Future studies should seek to recruit a more balanced sample. There were also few participants with elevated symptoms for some of the psychological problems examined in this study. It is possible that by collecting data from more individuals who experience particular psychological problems, new or clearer patterns might emerge between IRRA and specific forms of psychopathology. An additional limitation is that parent-report was used to measure both adult and child psychopathology. Parent report may not be the most valid way to measure some forms of psychopathology for children (Moretti, Fine, Haley, and Marriage, 1985), and this method invariance may lead to more similar findings across adults and children. Relatedly, the use of self/parent report scales to measure psychopathology, rather than following complete diagnostic procedures for the different forms of psychopathology examined in the present study limits the specificity of our results to specific populations of individuals with psychiatric disorders.
Finally, the present study examined IRRA using a self-reported measure. The inclusion of a behavioral measure of IRRA to examine the relationships between IRRA and psychopathology may have provided additional support for the findings of the present study, or may have produced different results that may align better with the previous literature that has found significant relationships between IRRA and specific areas of psychopathology.
4.2. Future Directions
Future research should supplement the findings of the present study, which are based primarily on self-report measures, with findings utilizing other measurement modalities, such as behavioral paradigms to measure IRRA. Future research might also examine participant stress, or current stressors in the environment, in relation to IRRA and psychopathology, given previous findings suggesting stressful conditions may impact IRRA (Ossewaarde et al., 2011; Lighthall et al., 2011). Additionally, future studies should examine the relationship between other Positive Valence constructs and psychopathology in a similar manner, and determine if these constructs differentially associate with various forms of psychopathology and functioning. This research group has begun this process in a related manuscript examining the impact of effort valuation on the same psychopathology and functioning outcomes (see Nguyen et al., 2019), and intends to examine additional PVS constructs in this manner as well. Finally, longitudinal work will also be important for examining the stability of IRRA over time, and understanding how IRRA at one point in time might predict to future psychopathology and functioning.
4.3. Conclusions
The present study establishes IRRA as a relevant psychological construct for understanding adaptive functioning in adults and children. However, findings suggest that IRRA may be less relevant for understanding specific psychopathology. This study expands upon the extant literature by revealing the importance of considering sex and ancestry when examining how IRRA relates to psychopathology and functioning, and by relating IRRA to areas of psychopathology and functioning to which it has not previously been related.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Achenbach TM (1991). Integrative guide for the 1991 CBCL/4–18, YSR, and TRF Profiles. Burlington, VT: University of Vermont, Department of Psychiatry. [Google Scholar]
- Achenbach TM, Rescorla LA (2003). Manual for the ASEBA Adult Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families. [Google Scholar]
- Andrade LF, Petry NM (2014). White problem gamblers discount delayed rewards less steeply than their African American and Hispanic counterparts. Psychology of Addictive Behaviors, 28(2), 599–606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Al-Adawi S, Powell J (1997). The influence of smoking on reward responsiveness and cognitive functions: a natural experiment. Addiction, 92(12), 1773–1782. 10.1111/j.1360-0443.1997.tb02897.x. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. [Google Scholar]
- Benjamini Y, Hochberg Y. (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: Series B, 57(1), 289–300. http://links.jstor.org/sici?sici=0035-9246%281995%2957%3A1%3C289%3ACTFDRA%3E2.0.CO%3B2-E. [Google Scholar]
- Bogdan R, Pizzagalli DA (2006). Acute stress reduces reward responsiveness: implications for depression. Biological Psychiatry, 60(10), 1147–1154. 10.1016/j.biopsych.2006.03.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bogdan R, Pizzagalli DA (2009). The heritability of hedonic capacity and perceived stress: a twin study evaluation of candidate depressive phenotypes. Psychological Medicine, 39(02), 211–218. 10.1017/S0033291708003619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boksem MA, Meijman TF, Lorist MM (2006). Mental fatigue, motivation and action monitoring. Biological Psychology, 72(2), 123–132. 10.1016/j.biopsycho.2005.08.007. [DOI] [PubMed] [Google Scholar]
- Bress JN, Foti D, Kotov R, Klein DN, Hajcak G (2013). Blunted neural response to rewards prospectively predicts depression in adolescent girls. Psychophysiology, 50(1), 74–81. 10.1111/j.1469-8986.2012.01485.x. [DOI] [PubMed] [Google Scholar]
- Carver CS, White TL (1994). Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: The BIS/BAS Scales. Journal of personality and social psychology, 67(2), 319 10.1037/0022-3514.67.2.319. [DOI] [Google Scholar]
- Cooper ML (1994). Motivations for alcohol use among adolescents: Development and validation of a four-factor model. Psychological Assessment, 6(2), 117–128. 10.1037/1040-3590.6.2.117 [DOI] [Google Scholar]
- Cuthbert BN (2014). The RDoC framework: facilitating transition from ICD/DSM to dimensional approaches that integrate neuroscience and psychopathology. World Psychiatry, 13(1), 28–35. 10.1002/wps.20087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elvemo NA, Landrø NI, Borchgrevink PC, Håberg AK (2015). Reward responsiveness in patients with chronic pain. European Journal of Pain, 19(10), 1537–1543. 10.1002/ejp.687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fredrickson BL, & Joiner T (2002). Positive emotions trigger upward spirals toward emotional well-being. Psychological Science, 13(2), 172–175. [DOI] [PubMed] [Google Scholar]
- Gard DE, Gard MG, Kring AM, John OP (2006). Anticipatory and consummatory components of the experience of pleasure: a scale development study. Journal of research in personality, 40(6), 1086–1102. 10.1016/j.jrp.2005.11.001. [DOI] [Google Scholar]
- Gros DF, Price M, Magruder KM, Frueh BC (2012). Symptom overlap in posttraumatic stress disorder and major depression. Psychiatry Research, 196(2), 267–270. 10.1016/j.psychres.2011.10.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton KR, Sinha R, Potenza MN (2012). Hazardous drinking and dimensions of impulsivity, behavioral approach, and inhibition in adult men and women. Alcoholism: Clinical and Experimental Research, 36(6), 958–966. 10.1111/j.1530-0277.2011.01708.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henriques JB, Davidson RJ (2000). Decreased responsiveness to reward in depression. Cognition & Emotion, 14(5), 711–724. 10.1080/02699930050117684. [DOI] [Google Scholar]
- John K, Gammon DG, Prusoff BA, Warner V (1987). The Social Adjustment Inventory for Children and Adolescents (SAICA): testing of a new semistructured interview. Journal of the American Academy of Child & Adolescent Psychiatry, 26(6), 898–911. 10.1097/00004583-198726060-00015. [DOI] [PubMed] [Google Scholar]
- Kazdin AE (1989). Evaluation of the Pleasure Scale in the assessment of anhedonia in children. Journal of the American Academy of Child & Adolescent Psychiatry, 28(3), 364–372. 10.1097/00004583-198905000-00010. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry, 62(6), 593–602. [DOI] [PubMed] [Google Scholar]
- Kohls G, Thönessen H, Bartley GK, Grossheinrich N, Fink GR, Herpertz-Dahlmann B, Konrad K (2014). Differentiating neural reward responsiveness in autism versus ADHD. Developmental Cognitive Neuroscience, 10, 104–116. 10.1016/j.dcn.2014.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kozak MJ, Cuthbert BN (2016). The NIMH research domain criteria initiative: Background, issues, and pragmatics. Psychophysiology, 53(3), 286–297. 10.1111/psyp.12518. [DOI] [PubMed] [Google Scholar]
- Krueger RF, Bezdjian S (2009). Enhancing research and treatment of mental disorders with dimensional concepts: toward DSM-V and ICD-11. World Psychiatry, 8(1), 3–6. 10.1002/j.2051-5545.2009.tb00197.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewinsohn PM, Clarke GN, Seeley JR, & Rhode P (1994). Major depression in community adolescents: Age at onset, episode duration, and time to recurrence. Journal of the American Academy of Child and Adolescent Psychiatry, 33(6), 809–818. [DOI] [PubMed] [Google Scholar]
- Lighthall NR, Sakaki M, Vasunilashorn S, Nga L, Somayajula S, Chen EY, Samii N, Mather M (2011). Gender differences in reward-related decision processing under stress. Social Cognitive and Affective Neuroscience, 7(4), 476–484. 10.1093/scan/nsr026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maj M (2005). ‘Psychiatric comorbidity’: an artifact of current diagnostic systems?. The British Journal of Psychiatry, 186(3), 182–184. 10.1192/bjp.186.3.182. [DOI] [PubMed] [Google Scholar]
- McFarland BR, Klein DN (2009). Emotional reactivity in depression: diminished responsiveness to anticipated reward but not to anticipated punishment or to nonreward or avoidance. Depression and Anxiety, 26(2), 117–122. 10.1002/da.20513. [DOI] [PubMed] [Google Scholar]
- Moretti MM, Fine S, Haley G, & Marriage K (1985). Childhood and adolescent depression: Child-report versus parent-report information. Journal of the American Academy of Child Psychiatry, 24(3), 298–302. 10.1016/S0002-7138(09)61090-6 [DOI] [PubMed] [Google Scholar]
- National Institute of Mental Health. (2013). Research Domain Criteria (RDoC). http://www.nimh.nih.gov/research-priorities/rdoc/constructs/initial-responsiveness-to-reward-attainment.shtml.
- Nguyen N, Albert AB, Van Orman S, Forken P, Blatt SD, Fremont WP, Glatt SJ, & Faraone SV (2019). Effort valuation and psychopathology in adults and children. Psychological Medicine, 14, 1–7. [DOI] [PubMed] [Google Scholar]
- Olbert CM, Gala GJ, Tupler LA (2014). Quantifying heterogeneity attributable to polythetic diagnostic criteria: theoretical framework and empirical application. Journal of Abnormal Psychology, 123(2), 452 10.1037/a0036068. [DOI] [PubMed] [Google Scholar]
- Ossewaarde L, Qin S, Van Marle HJ, van Wingen GA, Fernández G, Hermans EJ (2011). Stress-induced reduction in reward-related prefrontal cortex function. Neuroimage, 55(1), 345–352. 10.1016/j.neuroimage.2010.11.068. [DOI] [PubMed] [Google Scholar]
- Pardini M, Capello E, Krueger F, Mancardi G, Uccelli A (2012). Reward responsiveness and fatigue in multiple sclerosis. Multiple Sclerosis Journal, 19(2), 233–240. 10.1177/1352458512451509. [DOI] [PubMed] [Google Scholar]
- Perneger TV (1998). What’s wrong with Bonferroni adjustments. British Medical Journal, 316(7139), 1236–1238. 10.1136/bmj.316.7139.1236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pizzagalli DA, Iosifescu D, Hallett LA, Ratner KG, Fava M (2008). Reduced hedonic capacity in major depressive disorder: evidence from a probabilistic reward task. Journal of Psychiatric Research, 43(1), 76–87. 10.1016/j.jpsychires.2008.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Potts R, Martinez IG, Dedmon A, Schwarz L, DiLillo D, Swisher L (1997). Brief Report: Cross-Validtion of the Injury Behavior Checklist in a School-Age Sample. Journal of Pediatric Psychology, 22(4), 533–540. 10.1093/jpepsy/22.4.533. [DOI] [PubMed] [Google Scholar]
- Powell J, Dawkins L, Davis RE (2002). Smoking, reward responsiveness, and response inhibition: tests of an incentive motivational model. Biological Psychiatry, 51(2), 151–163. 10.1016/S0006-3223(01)01208-2. [DOI] [PubMed] [Google Scholar]
- Schag K, Teufel M, Junne F, Preissl H, Hautzinger M, Zipfel S, Giel KE (2013). Impulsivity in binge eating disorder: food cues elicit increased reward responses and disinhibition. PLoS One, 8(10), 477–495. 10.1111/obr.12017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shipley WC, Gruber CP, Martin TA, & Klein AM (2009). Shipley-2 manual. Los Angeles, CA: Western Psychological Services. [Google Scholar]
- Van den Berg L, Pieterse K, Malik JA, Luman M, Van Dijk KW, Oosterlaan J, Delemarre-van de Waal HA (2011). Association between impulsivity, reward responsiveness and body mass index in children. International Journal of Obesity, 35(10), 1301–1307. 10.1038/ijo.2011.116. [DOI] [PubMed] [Google Scholar]