

Abstract
Background
Phone calls as part of multimodal fecal immunochemical test (FIT) outreach are effective but resource-intensive. Previous studies of advanced notification calls before FIT mailing have not differentiated patients’ prior screening status.
Objective
To determine the effectiveness of a phone call preceding mailing of a FIT kit on test completion rate for patients who have completed a prior FIT.
Design
Randomized controlled trial nested within a larger study. All patients were assigned to receive organized mailed FIT outreach in the larger study.
Participants
Patients in a safety-net health setting ages 50–75 years old with a previously negative FIT.
Interventions
Patients were assigned to either receive an advanced notification phone call or no phone call preceding a mailed FIT kit. Both groups received an informational postcard prior to the mailed FIT.
Main Measures
The primary outcome was FIT completion rate at 1 year. The secondary outcomes were FIT completion rates at 60, 90, and 180 days, rates stratified by demographic subgroups, and rates according to outcome of the phone call.
Key Results
A total of 1645 patients were assigned to advanced notification calls and 1595 were assigned to no call preceding the FIT mailing. Although FIT completion rate was higher at day 60 (55.5% vs. 50.8%, p < 0.01), an advanced notification call did not significantly improve FIT completion at 1 year (70.9% vs. 69.9%, p = 0.52). Of the patients assigned to receive an advanced notification call, 90.5% were spoken with or left a voicemail; patients who were spoken with were more likely to complete a FIT at 1 year compared with patients who were only left a voicemail or could not be left a voicemail (79.9% vs. 69.2% vs. 49.6%, p < 0.01).
Conclusions
Advanced notification phone calls prior to FIT mailing did not improve rates at 1 year for patients with a previously negative FIT.
Electronic supplementary material
The online version of this article (10.1007/s11606-020-06009-4) contains supplementary material, which is available to authorized users.
KEY WORDS: colon cancer, screening outreach, introductory call, pre-FIT reminder
INTRODUCTION
Fecal immunochemical testing (FIT) is commonly adopted in resource-limited settings and has been increasingly used to improve colorectal cancer (CRC) population-level screening rates.1–3 Evidence suggests combining effective outreach strategies in a multicomponent intervention increases uptake of screening more than individual strategies alone, and is specifically recommended by the Community Preventive Services Task Force to improve CRC screening in underserved populations.4–6 Direct mailing of FIT kits is a form of organized outreach associated with significant increases in screening rates, but its effectiveness may be enhanced in part by additional components before and after mailing the FIT kit.7
Given that FIT outreach is effective, exploring opportunities to improve the efficiency of this service is warranted. Phone calls may serve as a valuable prompt and can verify a patient’s address and empanelment status in health systems, particularly in underserved communities; however, calls can be a resource-intensive intervention.8–10 While advanced notification calls before FIT outreach are effective,7, 11–13 they may not be necessary for all patients, especially for those more likely to complete a FIT.14–16 Though patients most likely to complete a FIT are those with prior FIT completion,17, 18 studies investigating the effectiveness of pre-FIT advanced notifications did not focus on this subgroup.11, 19, 20 Advanced notification outreach has been examined and shown to be modestly effective in previously unscreened populations,21 whereas the benefits in populations with prior FIT completion are not known. Therefore, our aim was to determine the effectiveness of an advanced notification phone call preceding mailing of a FIT kit in patients who had previously completed a FIT. We hypothesized that those familiar with completing a FIT will require less intervention and thus will not find additional benefit from an advanced notification phone call in a multicomponent outreach program at 1 year.
METHODS
Study Setting and Population
This study was conducted as a randomized substudy of a larger randomized controlled trial22 of mailed FIT kits in the San Francisco Health Network (SFHN), a publicly funded safety-net health system serving low-income populations. In the larger trial (NCT02613260), patients aged 50–75 years who were not up-to-date with CRC screening were assigned to receive multicomponent screening interventions that included mailing of a FIT kit and were compared to usual care. Providers and staff were blinded to which patients were assigned to the outreach intervention. Patients were enrolled between December 2015 and June 2017. The intervention was started at time of enrollment, and outcome assessment continued until 1 year after intervention delivery. The outreach activities were conducted in eight primary care clinic sites. As previously described, patients were excluded from outreach if they were homeless, were no longer empaneled in the health system, had an abnormal FIT but no colonoscopy, colectomy, late-stage cancer, or advanced comorbidities with limited life expectancy.22 This trial was approved by the University of California San Francisco Institutional Review Board (IRB, 14-14861).
Study Intervention
The multicomponent intervention for the larger randomized trial included an informational postcard, followed by a mailed FIT kit packet, and up to two reminder phone calls if the FIT kit was not returned after 2 weeks. In this study, patients in the intervention arm of the larger trial who had any previous negative FIT were randomly allocated to receive an advanced notification phone call (“Advanced Call” group) or no advanced notification phone call (“No Advanced Call” group) after being mailed a postcard and before being mailed a FIT kit. Patients were allocated using randomly permuted blocks of size four, within strata jointly defined by clinic, sex, race, language, and history of FIT completion (Fig. 1). After randomization into the “Advanced Call” group, patients that met the following criteria did not receive an advanced notification call: already received a FIT kit, became up-to-date, no longer received care at one of the eight clinics, screening was deferred or not indicated. A statistician generated the random allocation sequence, and the study team enrolled and conducted outreach to participants. The study team attempted up to two advanced notification phone calls to contact patients before FIT kit mailing and tried to leave a voicemail if the call was not successful. Phone calls were performed during work hours with interpreter services available for all languages. Patients in the “No Advanced Call” group were only called prior to FIT kit mailing if the postcard was returned to sender in an attempt to verify address before FIT mailing. Patients in both the “Advanced Call” and “No Advanced Call” groups were eligible for reminder calls after being mailed a FIT kit if not returned after 2 weeks.
Fig. 1.

CONSORT (Consolidated Standards of Reporting Trials) flow diagram. The outreach protocol included mailing a postcard and FIT kit to patients in both arms. In the “Advanced Call” group, there were 236 (14.3%) patients who were not called because they fulfilled one or more of the following criteria: already received a FIT kit, became up-to-date, no longer received care at one of the eight clinics, screening was deferred or not indicated.
Statistical Analysis
Patient demographic characteristics were summarized by intervention group using proportions and compared using chi-square tests.
The primary outcome was completion of FIT screening, which was defined as the proportion of patients in the “No Advanced Call” and “Advanced Call” groups who had completed a FIT within 1 year after study enrollment. We also examined short-term outcomes of FIT completion at 60, 90, and 180 days. The effect of the intervention was assessed with an unadjusted logistic regression model using an intention-to-treat analysis. We also assessed the effect of the intervention by excluding patients in both arms who were not mailed a FIT. Reasons for not receiving a kit included deferred screening, an unreliable address (returned postcard), no longer in the health network, or death. Participants who were lost to follow-up and were not known to have completed a FIT were assumed to have not completed FIT screening. This logistic regression model was also used to assess the outreach effect on FIT completion over time, and a cumulative incidence plot was used to estimate the proportions up-to-date over time (Fig. 2). The between-group difference in proportions was calculated along with confidence intervals.
Fig. 2.
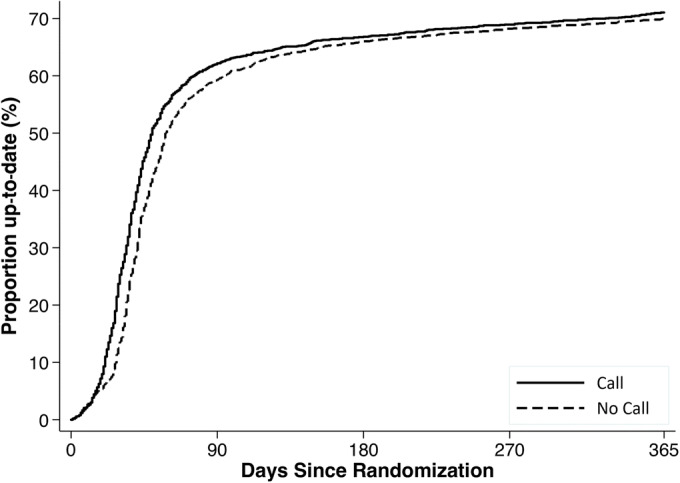
Cumulative incidence curve of the proportion of patients up-to-date on CRC screening in the “Advanced Call” group compared with “No Advanced Call” group up to 1 year from randomization. At 60 days, FIT completion rate was 55.5% in the “Advanced Call” group vs. 50.8% in the “No Advanced Call” group (p < 0.01); at 1 year, the completion rate was 70.9% for the “Advanced Call” group and 69.9% for “No Advanced Call” group (p = 0.52).
Evidence for effect modification of the advanced notification phone call by gender, age, race/ethnicity, insurance coverage, language, marital status, and clinic was examined using logistic regression models with interaction terms. Between-group differences in FIT completion proportions, stratified by levels of each effect modifier, were calculated.
FIT completion rates were examined according to the outcome of the advanced notification call in the “Advanced Call” group. The call outcomes were defined as “spoken with” (patient spoken with), “voicemail only” (patient unable to be spoken with and was left a voicemail), or “no voicemail” (patient unable to be spoken with and unable to be left a voicemail). Call outcomes for patients in the “No Advanced Call” group were summarized using proportions.
The study was powered for the parent clinical trial, which randomized patients to usual care versus organized outreach with FIT mailing.22 Of the 5386 individuals who were assigned to outreach in the intervention arm of the parent study, there were 3240 individuals who had previously completed a FIT; these individuals were eligible for this substudy. Based on the 3240 individuals, this provided 80% power in 2-sided 5% tests to detect between-group differences in 30-day and 1-year completion rates of 3.4 and 5.1 percentage points, respectively. We used Stata (version 15.1; StataCorp LP, College Station, TX) and SAS (version 9.4; SAS Institute Inc., Cary, NC) for all statistical analyses. Results were considered significant if p < 0.05.
RESULTS
Patient Characteristics
The study population was largely insured by Medicaid (48.1%) and Medicare (19.2%) and the two largest racial/ethnic groups were Hispanic (25.2%) and Asian (23.5%). A total of 1595 patients were randomized to the “No Advanced Call” group and 1645 were randomized to the “Advanced Call” group prior to FIT mailing. There were no significant demographic differences between the two groups (Table 1).
Table 1.
Baseline Demographic Characteristics of Patients Assigned to Either “No Advanced Call” or “Advanced Call”
| No Advanced Call (n = 1595) | Advanced Call (n = 1645) | p value | |
|---|---|---|---|
| Gender (%) | 0.80 | ||
| Female | 809 (50.7) | 827 (50.3) | |
| Male | 786 (49.3) | 818 (49.7) | |
| Age (%) | 0.34 | ||
| 50–54 | 285 (17.9) | 302 (18.4) | |
| 55–59 | 459 (28.8) | 432 (26.3) | |
| 60–64 | 408 (25.6) | 455 (27.7) | |
| 65–69 | 303 (19.0) | 296 (18.0) | |
| 70–75 | 140 (8.8) | 160 (9.7) | |
| Race/ethnicity (%) | 0.94 | ||
| Hispanic | 409 (25.6) | 408 (24.8) | |
| Non-Hispanic Black | 306 (19.2) | 311 (18.9) | |
| Non-Hispanic White | 304 (19.1) | 310 (18.8) | |
| Asian | 370 (23.2) | 390 (23.7) | |
| Other/unknown | 206 (12.9) | 226 (13.7) | |
| Insurance (%) | 0.29 | ||
| Medicaid | 757 (47.5) | 800 (48.7) | |
| Medicare | 293 (18.4) | 330 (20.1) | |
| County-sponsored | 166 (10.4) | 132 (8.0) | |
| Healthy worker* | 276 (17.3) | 267 (16.3) | |
| Uninsured | 73 (4.6) | 83 (5.1) | |
| Other/unknown | 29 (1.8) | 31 (1.9) | |
| Primary language (%) | 0.66 | ||
| English | 937 (58.7) | 940 (57.1) | |
| Spanish | 355 (22.3) | 364 (22.1) | |
| Chinese | 143 (9.0) | 161 (9.8) | |
| Other/unknown | 160 (10.0) | 180 (10.9) | |
| Marital status (%) | 0.62 | ||
| Single | 775 (48.6) | 803 (48.8) | |
| Married | 447 (28.0) | 429 (26.1) | |
| Divorced | 151 (9.5) | 152 (9.2) | |
| Separated | 78 (4.9) | 93 (5.7) | |
| Widowed | 77 (4.8) | 85 (5.2) | |
| Unknown | 67 (4.2) | 83 (5.0) | |
| Clinic (%) | 0.88 | ||
| 1 | 433 (27.1) | 440 (26.7) | |
| 2 | 194 (12.2) | 194 (11.8) | |
| 3 | 64 (4.0) | 77 (4.7) | |
| 4 | 141 (8.8) | 157 (9.5) | |
| 5 | 305 (19.1) | 307 (18.7) | |
| 6 | 187 (11.7) | 205 (12.5) | |
| 7 | 158 (9.9) | 144 (8.8) | |
| 8 | 113 (7.1) | 121 (7.4) |
FIT fecal immunochemical test
*Insurance type for in-home support service providers and temporary insurance for county employees
Effect of Organized Outreach to Increase FIT Participation
FIT completion rate at 1 year was 70.9% for the “Advanced Call” group and 69.9% for the “No Advanced Call” group, with no significant difference between the two groups (p = 0.52; Table 2). Though there was a significant difference in completion at 60 days (55.5% Advanced Call vs. 50.8% No Advanced Call, p < 0.01), the difference diminished and was no longer statistically significant after 90 days (62.2% Advanced Call vs. 59.3% No Advanced Call, p = 0.09) (Fig. 2). Completion at 180 days was 66.8% in the “Advanced Call” group and 66.0% in the “No Advanced Call” group (p = 0.63). An analysis excluding patients who did not receive a mailed FIT kit also found no significant difference in FIT completion between the two arms at 1 year (78.8% No Advanced Call vs. 81.0% Advanced Call, p = 0.14).
Table 2.
FIT Completion Rate at 1 Year in Patients Assigned to “No Advanced Call” and “Advanced Call”
| No. complete (%) | |||||
|---|---|---|---|---|---|
| No Advanced Call | Advanced Call | OR (95% CI) | p value | Subgroup interaction with phone call | |
| Overall | 1115 (69.9) | 1167 (70.9) | 1.05 (0.90, 1.22) | 0.52 | |
| Gender | 0.61 | ||||
| Female | 577 (71.3) | 605 (73.2) | 1.10 (0.88, 1.36) | 0.41 | |
| Male | 538 (68.4) | 562 (68.7) | 1.01 (0.82, 1.25) | 0.91 | |
| Age | 0.45 | ||||
| 50–54 | 202 (70.9) | 215 (71.2) | 1.02 (0.71, 1.45) | 0.93 | |
| 55–59 | 314 (68.4) | 301 (69.7) | 1.06 (0.80, 1.41) | 0.68 | |
| 60–64 | 282 (69.1) | 327 (71.9) | 1.14 (0.85, 1.53) | 0.38 | |
| 65–69 | 213 (70.3) | 218 (73.6) | 1.18 (0.83, 1.69) | 0.36 | |
| 70–75 | 104 (74.3) | 106 (66.2) | 0.68 (0.41, 1.12) | 0.13 | |
| Race/ethnicity | 0.81 | ||||
| Hispanic | 307 (75.1) | 306 (75.0) | 1.00 (0.73, 1.37) | 0.98 | |
| Non-Hispanic Black | 194 (63.4) | 204 (65.6) | 1.10 (0.79, 1.53) | 0.57 | |
| Non-Hispanic White | 196 (64.5) | 213 (68.7) | 1.21 (0.86, 1.69) | 0.27 | |
| Asian | 289 (78.1) | 298 (76.4) | 0.91 (0.65, 1.28) | 0.58 | |
| Other/unknown | 129 (62.6) | 146 (64.6) | 1.09 (0.74, 1.61) | 0.67 | |
| Insurance | 0.33 | ||||
| Medicaid | 505 (66.7) | 553 (69.1) | 1.12 (0.90, 1.38) | 0.31 | |
| Medicare | 209 (71.3) | 246 (74.5) | 1.18 (0.83, 1.68) | 0.37 | |
| County-sponsored | 115 (69.3) | 94 (71.2) | 1.10 (0.66, 1.81) | 0.72 | |
| Healthy worker* | 217 (78.6) | 212 (79.4) | 1.05 (0.69, 1.58) | 0.82 | |
| Uninsured | 49 (67.1) | 49 (59.0) | 0.71 (0.37, 1.36) | 0.30 | |
| Other/unknown | 16 (56.2) | 9 (29.4) | 0.32 (0.08, 1.36) | 0.12 | |
| Primary language | 0.94 | ||||
| English | 619 (66.1) | 623 (66.3) | 1.01 (0.83, 1.22) | 0.92 | |
| Spanish | 264 (74.4) | 277 (76.1) | 1.10 (0.78, 1.54) | 0.59 | |
| Chinese | 119 (83.2) | 138 (85.7) | 1.21 (0.65, 2.25) | 0.55 | |
| Other/unknown | 113 (70.6) | 129 (71.7) | 1.05 (0.66, 1.68) | 0.83 | |
| Marital status | 0.14 | ||||
| Single | 546 (70.5) | 575 (71.6) | 1.06 (0.85, 1.31) | 0.61 | |
| Married | 329 (73.6) | 312 (72.7) | 0.96 (0.71, 1.29) | 0.77 | |
| Divorced | 101 (66.9) | 108 (71.1) | 1.22 (0.75, 1.98) | 0.43 | |
| Separated | 46 (59.0) | 72 (77.4) | 2.39 (1.23, 4.63) | 0.01 | |
| Widowed | 50 (64.9) | 54 (63.5) | 0.94 (0.49, 1.79) | 0.85 | |
| Other/unknown | 43 (64.2) | 46 (55.4) | 0.69 (0.36, 1.34) | 0.28 | |
| Clinic | 0.26 | ||||
| 1 | 329 (76.0) | 333 (75.7) | 0.98 (0.72, 1.34) | 0.92 | |
| 2 | 122 (62.9) | 134 (69.1) | 1.32 (0.86, 2.01) | 0.20 | |
| 3 | 49 (76.6) | 60 (77.9) | 1.08 (0.49, 2.38) | 0.85 | |
| 4 | 114 (80.9) | 119 (75.8) | 0.74 (0.43, 1.29) | 0.29 | |
| 5 | 212 (69.5) | 214 (69.7) | 1.01 (0.72, 1.42) | 0.96 | |
| 6 | 133 (71.1) | 134 (65.4) | 0.77 (0.50, 1.18) | 0.22 | |
| 7 | 92 (58.2) | 88 (61.1) | 1.13 (0.71, 1.79) | 0.61 | |
| 8 | 64 (56.6) | 85 (70.2) | 1.81 (1.05, 3.10) | 0.03 | |
FIT fecal immunochemical test
*Insurance type for in-home support service providers and temporary insurance for county employees
Although we found evidence in post hoc analysis that the advanced call was effective within two patient subgroups (specifically patients from Clinic 8 and those separated from their marital partners), none of the tests for modification of the effect of the phone call by patient subgroup or clinic were statistically significant (Table 2).
Advanced Notification Call Outcomes
Of the 1645 patients randomized to the “Advanced Call” group, 236 patients (14.3%) did not receive an advanced notification phone call (Fig. 1). Of the 1409 patients who were called, 767 (54.4%) were spoken with, 509 (36.1%) received a voicemail only, and 133 (9.4%) were called but no voicemail could be left. There were no significant demographic differences between patients with different call outcomes (Supplemental Table 1). Overall, 90.5% were spoken with or left a voicemail; patients who were spoken with were more likely to complete a FIT at 1 year compared with patients who were only left a voicemail or could not be left a voicemail (79.9% vs. 69.2% vs. 49.6%, p < 0.01; Table 3).
Table 3.
FIT Completion Rate at 1 Year in the “Advanced Call” Group According to Call Outcome
| Call outcome | n (%) | FIT completion (%) | OR (95% CI) | p value |
|---|---|---|---|---|
| Spoken with | 767 (54.4) | 79.9 | Ref. | < 0.01 |
| Voicemail | 509 (36.1) | 69.2 | 0.56 (0.44, 0.73) | |
| No voicemail | 133 (9.4) | 49.6 | 0.25 (0.17, 0.36) |
FIT fecal immunochemical test
Of the patients randomized to the “No Advanced Call” group, 114 patients (7.1%) were called prior to FIT mailing because postcard and/or FIT kit was returned to sender. Of these patients, 62 (54.4%) were spoken with, 40 (35.1%) received a voicemail only, and 12 (10.5%) were called but no voicemail could be left.
DISCUSSION
This study compared the effects of an advanced notification phone call for patients with a previously negative FIT and showed this phone call may lead to earlier FIT completion. However, the difference in FIT completion was no longer evident at 1 year. For patients who we intended to provide advanced notification, patients who could not be reached by phone or left a voicemail were less likely to complete the FIT.
Our findings support that advanced notification phone calls as part of a multicomponent intervention in a population with previous FIT may provide only short-term benefits. There was a modest difference in FIT completion favoring advanced notification phone calls at day 60, but the effect did not persist at 1 year. Studies have shown outreach using letters and phone calls in conjunction with FIT mailing increases screening rates,19–21 especially in a population with inconsistent access to healthcare.11, 23 However, our findings suggest that the addition of phone calls to postcards and FIT mailing may not increase screening rates in the subset of this population who have had previous experience with FIT. While there is evidence that multiple combined modalities are important for increasing FIT completion,4, 5 our findings support that patients with previous FIT completion may need less intervention to achieve the same level of screening. Our findings allow for more efficient resource utilization by identifying appropriate and specific outreach in CRC screening.
There are difficulties inherent in a safety-net system including language barriers, health literacy, financial instability, housing insecurity, and difficulties maintaining phone access that may prevent successful outreach.24–26 The level of patient contact was associated with increased FIT completion, and patients who were unable to be reached by phone may require other interventions to improve completion. Despite the limitations in contacting the “Advanced Call” group patients, this study simulates the reality of organized outreach and highlights the need for alternative solutions to address these barriers. One possibility may be short message service (SMS) outreach which has been shown to increase CRC screening participation and may reach people who could not be easily reached via phone call.27
This study has several limitations. For example, some patients were unable to be reached (e.g., could not be called, did not receive mailed FIT) or had difficulties in FIT return. Patients unable to be reached may have underestimated true FIT completion in both arms of the trial. Another limitation of our study is the fact that the “No Voicemail” group likely encapsulates a heterogenous group of patients with different reasons they were unable to be reached; future analyses could characterize patients who were not able to be spoken with or left a voicemail to better target interventions. For this study, we did not have the capacity to scale up the number of calls to directly compare advanced notification postcards to calls. In the future, comparison of individual components of outreach interventions can be pursued, including automated calls, SMS, or other electronic forms of communication. Lastly, this study may be limited by the fact that it was performed in a single safety-net health system with a diverse population, and may not be representative of other settings. In conclusion, our findings suggest that, for patients who have previously completed a FIT, the addition of advanced notification phone calls to multicomponent FIT kit outreach did not increase screening rates. We identified at-risk populations (such as the “No Voicemail” subgroup) who were less likely to complete screening and who may benefit from more targeted interventions. Going forward, further work in determining the effectiveness of individual outreach components can fine-tune staff activities and time. Alternatively, outreach may leverage technology-supported communication and reminders to improve screening rates.
Electronic Supplementary Material
(DOCX 14 kb)
Acknowledgments
This study would not have been possible without the partnership of leaders in the San Francisco Health Network of the San Francisco Department of Public Health.
Funding Information
This work was supported in part by the Centers for Disease Control and Prevention U48DP004998 (SIP 14-012), the UCSF Academic Research Systems, and the National Center for Advancing Translational Sciences, National Institutes of Health, through UCSF-CTSI Grant Number UL1 TR991872, and the SF Cancer Initiative.
Compliance with Ethical Standards
This trial was approved by the University of California San Francisco Institutional Review Board (IRB, 14-14861).
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or NIH.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Singal AG, Gupta S, Tiro JA, et al. Outreach Invitations for FIT and Colonoscopy Improve Colorectal Cancer Screening Rates: A Randomized Controlled Trial in a Safety-Net Health System. Cancer. 2016;122(3):456–463. doi: 10.1002/cncr.29770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chiu H-M, Chen SL-S, Yen AM-F, et al. Effectiveness of Fecal Immunochemical Testing in Reducing Colorectal Cancer Mortality from the One Million Taiwanese Screening Program. Cancer. 2015;121(18):3221–3229. doi: 10.1002/cncr.29462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Levin TR, Corley DA, Jensen CD, et al. Effects of Organized Colorectal Cancer Screening on Cancer Incidence and Mortality in a Large Community-Based Population. Gastroenterology. 2018;155(5):1383–1391.e5. doi: 10.1053/j.gastro.2018.07.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lara CL, Means KL, Morwood KD, et al. Colorectal Cancer Screening Interventions in 2 Health Care Systems Serving Disadvantaged Populations: Screening Uptake and Cost-effectiveness. Cancer. 2018;124(21):4130–4136. doi: 10.1002/cncr.31691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dougherty MK, Brenner AT, Crockett SD, et al. Evaluation of Interventions Intended to Increase Colorectal Cancer Screening Rates in the United States: A Systematic Review and Meta-analysis. JAMA Intern Med. 2018;178(12):1645–1658. doi: 10.1001/jamainternmed.2018.4637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cancer Screening: Multicomponent Interventions—Colorectal Cancer. The Guide to Community Preventive Services (The Community Guide). https://www.thecommunityguide.org/findings/cancer-screening-multicomponent-interventions-colorectal-cancer. Published February 9, 2017.
- 7.Issaka RB, Avila P, Whitaker E, Bent S, Somsouk M. Population Health Interventions to Improve Colorectal Cancer Screening by Fecal Immunochemical Tests: A Systematic Review. Prev Med. 2019;118:113–121. doi: 10.1016/j.ypmed.2018.10.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lofters AK, Vahabi M, Prakash V, et al. Lay Health Educators Within Primary Care Practices to Improve Cancer Screening Uptake for South Asian Patients: Challenges in Quality Improvement. Patient Prefer Adherence. 2017;11:495–503. doi: 10.2147/PPA.S127147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nielson CM, Rivelli JS, Fuoco MJ, et al. Effectiveness of Automated and Live Phone Reminders after Mailed-FIT Outreach in a Pilot Randomized Trial. Prev Med Rep. 2018;12:210–213. doi: 10.1016/j.pmedr.2018.10.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kiran T, Davie S, Moineddin R, Lofters A. Mailed Letter Versus Phone Call to Increase Uptake of Cancer Screening: A Pragmatic, Randomized Trial. J Am Board Fam Med JABFM. 2018;31(6):857–868. doi: 10.3122/jabfm.2018.06.170369. [DOI] [PubMed] [Google Scholar]
- 11.Kempe KL, Shetterly SM, France EK, Levin TR. Automated phone and mail population outreach to promote colorectal cancer screening. Am J Manag Care. 2012;18(7):370–378. [PubMed] [Google Scholar]
- 12.Mosen DM, Feldstein AC, Perrin N, et al. Automated Telephone Calls Improved Completion of Fecal Occult Blood Testing. Med Care. 2010;48(7):604–610. doi: 10.1097/MLR.0b013e3181dbdce7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Basch CE, Wolf RL, Brouse CH, et al. Telephone Outreach to Increase Colorectal Cancer Screening in an Urban Minority Population. Am J Public Health. 2006;96(12):2246–2253. doi: 10.2105/AJPH.2005.067223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Levy BT, Xu Y, Daly JM, Ely JW. A Randomized Controlled Trial to Improve Colon Cancer Screening in Rural Family Medicine: an Iowa Research Network (IRENE) Study. J Am Board Fam Med JABFM. 2013;26(5):486–497. doi: 10.3122/jabfm.2013.05.130041. [DOI] [PubMed] [Google Scholar]
- 15.Baker DW, Brown T, Buchanan DR, et al. Comparative Effectiveness of a Multifaceted Intervention to Improve Adherence to Annual Colorectal Cancer Screening in Community Health Centers: a Randomized Clinical Trial. JAMA Intern Med. 2014;174(8):1235–1241. doi: 10.1001/jamainternmed.2014.2352. [DOI] [PubMed] [Google Scholar]
- 16.Myers RE, Sifri R, Hyslop T, et al. A Randomized Controlled Trial of the Impact of Targeted and Tailored Interventions on Colorectal Cancer Screening. Cancer. 2007;110(9):2083–2091. doi: 10.1002/cncr.23022. [DOI] [PubMed] [Google Scholar]
- 17.Goldman SN, Liss DT, Brown T, et al. Comparative Effectiveness of Multifaceted Outreach to Initiate Colorectal Cancer Screening in Community Health Centers: a Randomized Controlled Trial. J Gen Intern Med. 2015;30(8):1178–1184. doi: 10.1007/s11606-015-3234-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rossi PG, Grazzini G, Anti M, et al. Direct Mailing of Faecal Occult Blood Tests for Colorectal Cancer Screening: a Randomized Population Study from Central Italy. J Med Screen. 2011;18(3):121–127. doi: 10.1258/jms.2011.011009. [DOI] [PubMed] [Google Scholar]
- 19.Cole SR, Smith A, Wilson C, Turnbull D, Esterman A, Young GP. An Advance Notification Letter Increases Participation in Colorectal Cancer Screening. J Med Screen. 2007;14(2):73–75. doi: 10.1258/096914107781261927. [DOI] [PubMed] [Google Scholar]
- 20.van Roon AHC, Hol L, Wilschut JA, et al. Advance Notification Letters Increase Adherence in Colorectal Cancer Screening: a Population-Based Randomized Trial. Prev Med. 2011;52(6):448–451. doi: 10.1016/j.ypmed.2011.01.032. [DOI] [PubMed] [Google Scholar]
- 21.Senore C, Ederle A, DePretis G, et al. Invitation Strategies for Colorectal Cancer Screening Programmes: The Impact of an Advance Notification Letter. Prev Med. 2015;73:106–111. doi: 10.1016/j.ypmed.2015.01.005. [DOI] [PubMed] [Google Scholar]
- 22.Somsouk M, Rachocki C, Mannalithara A, et al. Effectiveness and Cost of Organized Outreach for Colorectal Cancer Screening: a Randomized Controlled Trial. J Natl Cancer Inst. June 2019. doi:10.1093/jnci/djz110 [DOI] [PMC free article] [PubMed]
- 23.Fedewa SA, Corley DA, Jensen CD, et al. Colorectal Cancer Screening Initiation After Age 50 Years in an Organized Program. Am J Prev Med. 2017;53(3):335–344. doi: 10.1016/j.amepre.2017.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Liss DT, Baker DW. Understanding Current Racial/Ethnic Disparities in Colorectal Cancer Screening in the United States: the Contribution of Socioeconomic Status and Access to Care. Am J Prev Med. 2014;46(3):228–236. doi: 10.1016/j.amepre.2013.10.023. [DOI] [PubMed] [Google Scholar]
- 25.Morris NS, Field TS, Wagner JL, et al. The Association Between Health Literacy and Cancer-Related Attitudes, Behaviors, and Knowledge. J Health Commun. 2013;18(Suppl 1):223–241. doi: 10.1080/10810730.2013.825667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lopez-Class M, Luta G, Noone A-M, et al. Patient and Provider Factors Associated with Colorectal Cancer Screening in Safety Net Clinics Serving Low-Income, Urban Immigrant Latinos. J Health Care Poor Underserved. 2012;23(3):1011–1019. doi: 10.1353/hpu.2012.0109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wu Y, Liang Y, Zhou Q, et al. Effectiveness of a Short Message Service Intervention to Motivate People with Positive Results in Preliminary Colorectal Cancer Screening to Undergo Colonoscopy: a Randomized Controlled Trial. Cancer. March 2019. doi:10.1002/cncr.32043 [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX 14 kb)