

Abstract
Mobility among sex workers has been linked not only to improved economic and social opportunities, but also to concerns regarding displacement, criminalization, and violence. In 2014, new “end-demand” legislation criminalized new aspects of sex work in Canada (e.g., third-party advertising, purchasing) while leaving the sale of sex legal. Utilizing data from a longitudinal community-based cohort of women sex workers in Metro Vancouver (An Evaluation of Sex Workers Health Access [AESHA], 2010–2016), we used kernel density mapping to understand and identify geographic patterns of workplace neighborhood mobility (i.e., changing the primary neighborhood in which one worked in the last 6 months); multivariable logistic regression using generalized estimating equations was also used to model contextual (policing, violence, and safety) and individual correlates of workplace mobility among sex workers over the 6-year period, including potential changes in mobility patterns pre- and post-end-demand criminalization. A total of 543 sex workers were included in analyses, contributing 2,199 observations. A total of 402 (74.0%) experienced workplace neighborhood mobility during the study period. Neighborhood mobility was negatively correlated with age (adjusted odds ratio [AOR] = 0.98/year older, 95% confidence interval [CI] = [0.97, 0.99]) and positively correlated with homelessness (AOR = 1.43, 95% CI = [1.12, 1.82]), identifying as a gender/sexual minority (AOR = 1.31, 95% CI = [1.04, 1.70]), and servicing clients primarily outdoors (vs. informal indoor or in-call venues; AOR = 1.48, 95% CI = [1.21, 1.81]); police harassment (AOR = 1.19, 95% CI = [0.96, 1.48], p= .11) and changing one’s neighborhood of work due to safety concerns (AOR = 1.37, 95% CI = [0.94, 2.00], p = .09) were both marginally correlated. Steps to promote safer working conditions for marginalized women in urban environments remain urgently needed, including shifts away from criminalized enforcement toward community-led initiatives and promoting access to safer indoor workspaces.
Keywords: Sex work, mobility, displacement, spatial epidemiology, work environment
Introduction
Mobility within a population is often driven by a desire for improved employment and social opportunities, and often leads to changes in health and wellbeing in the new place of residence. (S. M. Goldenberg et al., 2014; S. M. Goldenberg, Strathdee, Perez-Rosales, & Sued, 2012; Shira Goldenberg, Strathdee, Gallardo, & Patterson, 2010; SM Goldenberg, Silverman, Engstrom, Bojorquez-Chapela, & Strathdee, 2014; Reed, Gupta, Biradavolu, & Blankenship, 2012) However, despite the potential availability of better economic opportunities in their new location, mobile populations also report, in certain contexts, experiences of increased isolation, reduced access to social networks and social support, barriers to health access, precarious and unsafe working conditions, and increased stigma and discrimination. (S. Y. Choi, 2011; Shira Goldenberg et al., 2010; Parrado & Flippen, 2010; Platt et al., 2006; Reed et al., 2012; Sou et al., 2017)
Women who engage in mobility and migration are overrepresented in precarious and informal work, including sex work. (Platt et al., 2012) Existing literature indicates that mobility among sex workers may be driven by ‘pull’ factors such as economic needs, social networks, and a search for improved working conditions and new experiences, as well as ‘push’ factors such as displacement related to criminalization and law enforcement and gender-based violence. (S. Goldenberg et al., 2014; Jie et al., 2012; Lippman et al., 2007; Niranjan Saggurti et al., 2012; Yi et al., 2010) Research on the relationship between mobility and sex workers’ health and safety in urban environments within the global north remains limited, with most work focused on international or internal migration and impacts on sex workers’ working conditions in low and middle-income countries and links with infectious diseases (1,3,10). Less attention has been given to the safety or interactions with law enforcement, yet we know these are crucial concerns for marginalized women, especially in global north contexts. (Ferguson & Morris, 2007; Lyttleton & Amarapibal, 2002; Reed et al., 2012; Richter et al., 2014; Rushing, Watts, & Rushing, 2005; Verma, Saggurti, Singh, & Swain, 2010)
Previous research has demonstrated significant concerns regarding high rates of violence, criminalization, and social inequities faced by sex workers globally(Decker et al., 2015; Shannon et al., 2015), including physical and sexual violence, barriers to consistent condom use and health access, and frequent stigma and discrimination. (S. M. Goldenberg et al., 2014; Ramesh, Ganju, Mahapatra, Mishra, & Saggurti, 2012; Niranjan Saggurti et al., 2012) Although several studies globally have suggested that sex workers who are highly mobile experience more violence and discrimination (N Saggurti et al., 2008; Niranjan Saggurti et al., 2012), little is known about the extent to which geographic mobility patterns amongst sex workers within urban settings relate to experiences of criminalization or displacement by law enforcement. For example, Indian research previously found that sex workers engaging in work-related mobility to attend religious festivals faced twice the rate of violence as those who did not engage in such mobility. (Niranjan Saggurti et al., 2012) A second Indian study highlighted the fact that a greater proportion of those engaging in sex work-related mobility outside their place of residence experienced violence and abuse compared to those who were not mobile. (Ramesh et al., 2012; Richter et al., 2014) Within high-income settings, however, there remains a gap in our understanding of how mobility patterns shape the well being and safety of sex workers.
Prior research from the city of Vancouver, Canada has found that international and internal migration amongst sex workers are linked to both positive and negative health and social outcomes, with short-term internal migration being linked to being younger, lower odds of HIV/STI positivity, higher income, and barriers to health access, and internal migration for sex work was also linked to enhanced work-related violence and increased condom refusal by intimate partners. (S. M. Goldenberg et al., 2014)
Within sex worker migration research only a limited number of studies have used spatial analysis. For example, spatial research conducted in Vancouver has previously shown that sex workers may avoid areas in which health and social services are concentrated due to concerns regarding policing. (Shannon et al., 2008) Amongst sex workers living with HIV, a recent spatial study in Vancouver also found that heightened displacement due to policing was independently correlated with HIV treatment interruptions (S. M. Goldenberg et al., 2017), suggesting that the social geography of sex work criminalization may undermine access to HIV treatment. Despite the demonstrated value of spatial analysis for understanding migration patterns and health access patterns amongst other populations(Collinson, 2010; Wolffers & Fernandez, 1995), particularly within urban environments, spatial analysis has been infrequently utilized to understand sex workers’ migration and mobility patterns and social outcomes.
While sex work was previously criminalized through provisions targeting various aspects of the sale of sex, in 2014 the Canadian government introduced the Protection of Communities and Exploited Persons Act (PCEPA) (Chu, Canadian, & Network, 2014; Perrin, 2014), also know as the ‘end-demand law’, new legislation which aims to reduce or eliminate prostitution by criminalizing the purchase of sex (also known as the ‘Swedish model’), despite a dearth of evidence of beneficial impacts for sex workers. Concerns have been raised that as a result of shifting surveillance and law enforcement efforts, sex workers may face reduced access to safer indoor work environments and potential displacement to more unsafe and less populated places, which has been shown to increase exposure to physical and sexual violence.(S. M. Goldenberg et al., 2014) These concerns are supported by experiences reported within Nordic countries where similar laws were implemented, yet were not demonstrated to improve safety but rather shown to result in unintended negative consequences, including those stemming from avoidance of outdoor public places and lost income. (Chu & Glass, 2013) Furthermore, this legislation has the potential to increase displacement, alter interactions with law enforcement and create a new working environment for sex workers.
Our study was informed by the dearth of longitudinal evidence regarding the social geography of neighbourhood mobility among sex workers within high-income settings, as well as serious concerns regarding the potential for shifting criminalization enforcement, as a result of the end-demand legislation, to impact urban displacement patterns and working conditions amongst sex workers. Our objective was to examine the spatial patterning and longitudinal correlates of workplace neighbourhood mobility (i.e., changing the neighbourhood in which one’s primary work environment is located) and potential changes pre and post implementation of end-demand legislation, amongst a community-based cohort of women sex workers in Metro Vancouver, Canada over a six-year period.
Methods
The data used for this research were derived from ‘An Evaluation of Sex Workers Health Access (AESHA)’, an open community-based prospective cohort of on- and off-street sex workers in Metro Vancouver in the period January 2010 to February 2016. On a semi-annual basis, participants completed interviewer-administered questionnaires which involved questions concerning their work environment, criminalization, health, and safety, and included spatial measures of work environment (e.g. places of servicing and soliciting clients, violence, policing).
Interviews were conducted in English or Mandarin by trained interviewers including experiential (sex workers) and non-experiential staff with extensive community experience. As previously described, the study was overseen by a large Community Advisory Board and was based on close collaboration with local community partners including sex workers women’s support groups and HIV agencies (Anderson et al., 2015; S. M. Goldenberg et al., 2014). The study holds ethical approval from the Research Ethics Boards at Providence Health Care/University of British Columbia and Simon Fraser University.
Cohort inclusion criteria involved self-identifying as women (trans inclusive), being 14 years of age or older, and having exchanged sex for money in the past 30 days. During the informed consent process, study staff thoroughly explained all study procedures, risks and benefits, and all participants provided written informed consent prior to enrolment. Through time-location sampling, sex workers were recruited through regular community-based outreach to public/outdoor settings (e.g., streets, alleys), diverse indoor sex work venues (e.g. massage parlors, micro-brothels, other in-call locations), and online (Shannon et al., 2007). Study participants completed questionnaires at study offices in Metro Vancouver or during outreach visits to their work or home location. Participants received $40 CAD at each visit for their time, expertise, and travel expenses.
Outcome Variable
The outcome variable (workplace neighbourhood mobility) was defined as whether participants reported one or more changes in their primary neighbourhood of servicing/soliciting clients between any two study visits during the study period and was coded as a binary variable (yes vs. no). Place of work included the primary places of solicitation and servicing provided by participants. The study was situated within Metro Vancouver, which consists of the city of Vancouver and its bordering municipalities (e.g., Burnaby, Surrey). The City of Vancouver is geographically divided into 24 neighbourhoods and for the purpose of this analysis, bordering municipalities were considered as individual neighbourhoods for a total of 46 neighbourhoods within our study area.
Independent Variables
Independent variable selection was informed by a priori hypotheses based on previous research highlighting how mobility within the context of sex work is influenced by factors at multiple levels (J. Y. Choi, 2009; S. Goldenberg et al., 2014; Platt et al., 2012; Ragsdale, Anders, & Philippakos, 2007; Ramesh et al., 2012; Swain, Saggurti, Battala, Verma, & Jain, 2011; Yi et al., 2010), including individual-level (e.g. age, Indigenous ancestry) and structural (e.g. policing, violence, access to healthcare) determinants. Time-independent measures considered at baseline included sociodemographic characteristics such as age, gender/sexual orientation, Indigenous, im/migrant status, and level of education. All other variables were considered as time-dependent measures asked at each study visit and referred to occurrences within the previous 6 months.
Individual and sociodemographic variables included age (in years), identifying as a gender/sexual minority (with gay, lesbian, bisexual, two-spirit, asexual, transgender, transsexual, intersex, genderqueer (LGBTQ2S), or other considered as ‘yes’ vs. straight and cisgender, which were coded as ‘no’), identifying as Aboriginal/Indigenous (yes vs. no), being an im/migrant to Canada (born outside of Canada, yes vs. no), level of education (high school graduate vs. less than high school), substance use (including separate measures of use of non-injection and injection drugs, which were coded as yes vs. no), and self-rated health (defined as whether their health was perceived to be better/same compared to six months ago, yes vs. no).
Structural factors considered included average monthly income from non-government sources ($CAD; continuous), physical or sexual violence at work (defined as ‘yes’ to any of ‘Abducted/kidnapped’, ‘Attempted sexual assault’, ‘Raped’, ‘Strangled’, ‘Physically assaulted/beaten’, ‘Locked/trapped in a car’, ‘Thrown out of moving car’, ‘Assaulted with weapon’ yes vs. no), client condom refusal, homelessness (yes vs. no), and access to primary healthcare services when needed (yes vs. no). Primary type of place of servicing clients was coded as outdoor space (i.e., Street/outdoor public space’) vs. informal indoor (i.e., ‘Crack/drug house’, ‘Sauna/steam bath’, ‘Bar/nightclub’, ‘Exotic dance club/strip club/show lounge’, ‘Your place (in-call)’, ‘Client’s place (out-call)’, ‘Friend’s place’, ‘Hotel/hourly rental’), or formal indoor space (ie., ‘Massage/beauty parlor’, ‘Micro-brothel’, ‘Managed indoor space’). Several measures of criminalization and displacement were considered, including experiencing police harassment while working without being arrested (e.g., ‘Told to move on’, ‘Police raid’, ‘Threatened with arrest/detainment/fine’, ‘Searched’, ‘Followed’, ‘Picked up and driven elsewhere to work’, ‘Verbally harassed’, ‘Parked nearby/drove by repeatedly’, ‘Detained’, ‘Physically assaulted’, ‘Drugs/drug use equipment taken’, ‘Condoms taken’, ‘Searched for condoms’, ‘Other property taken’, ‘Propositioned to exchange sex’, ‘Coerced into providing sexual favours’; yes vs. no), rushing negotiations with clients due to police presence (yes vs. no), reporting that police presence affected where you work (yes vs. no), having red zones/legal restrictions affect where you work (yes vs. no), and changing the neighbourhood in which you work because of safety concerns (yes vs. no). Our variable examining exposure to end-demand legislation periods was defined as the period post- implementation of end-demand legislation (April 2015–2016) in comparison with the period prior to implementation (2010–2013); 2014 data were excluded as laws criminalizing sex workers were struck down at end of 2013 and the new laws were not put into place until the end of 2014.
Statistical Analysis
Descriptive statistics were calculated to examine differences in potential independent variables of interest according to whether or not participants had changed the neighbourhood of their primary work environment between study visits. The Mann-Whitney test was used for continuous variables and the Pearson’s chi-squared test (or Fisher’s exact test for small cell counts) were used to assess categorical variables.
Bivariate and multivariable logistic regression with generalized estimating equations (GEE) (Ballinger, 2004; Hanley, Negassa, & Forrester, 2003) was used to model individual and contextual factors correlated with workplace neighbourhood mobility over the six-year study period. GEE was used to account for repeated measurements of the same subjects across multiple study visits, and analyses were performed with a logit link function and an exchangeable correlation structure. Explanatory variables associated with neighbourhood mobility at a significance level of p <0.10 in bivariate analyses were considered for inclusion in the multivariable model. Identification of the best fitting multivariable model was conducted using a manual backward model selection process, as indicated by the lowest quasi-likelihood under the independence model criterion (QIC) value (Pan, 2001). All p-values are two-sided, and all statistical analyses were conducted in SAS 9.4 (© SAS Institute Inc., SAS). (SAS inc, 2015)
Given the concern that changes in criminalization patterns related to the implementation of end-demand legislation might influence patterns of mobility and displacement over time, we also conducted a sensitivity analysis to assess potential changes in neighbourhood mobility between the pre- vs. post-law implementation periods amongst sex workers interviewed during both time periods.
Spatial analysis
Mapping technology using ESRI ArcGIS 10.3 (ESRI, 2012) was employed to explore, visualize and highlight patterns of neighbourhood mobility, including the neighbourhoods between which participants moved most often during the study period.
Spatial variables collected within the AESHA questionnaire include places of service, solicitation and residence, as well as locations of violence, policing, and other structural measures and are collected at baseline and at each follow-up visit based on address or cross street. For this analysis, spatial data on place of service and solicitation was geocoded and assigned to the neighbourhood where it was located. Locations were then updated and mapped for each time period and coded to indicate whether a participant had changed the neighbourhood of their primary work environment. Patterns of in- and out-migration (I.e., net out-migration vs. in-migration amongst sex workers for each catchment area) were calculated and visually examined in order to identify the neighbourhoods that experienced the largest differences in these measures. Within the identified neighbourhoods, a hotspot analysis using kernel density techniques was applied to visually explore and represent locations within neighborhoods with high rates of net in- and out- migration.
Results
A total of 543 sex workers who provided a valid location of solicitation and/or service in at least two separate study visits were included in the analysis, who contributed 2199 observations over a median follow-up period of 24 months (interquartile range (IQR) 6 –40). 402 (74.0%) of the sample had changed the neighbourhood of their primary work environment between study visits at least once over the course of the six-year study.
The participants’ median age was 36 at baseline (IQR 28–43), 33.7% (n=183) self-identified as a gender/sexual minority, and 23.6% were im/migrants to Canada. 35.3% of the sample reported primarily servicing clients in outdoor/public spaces, 41.1% in informal indoor spaces, and 22.1% in formal indoor (in-call) environments at first follow-up (Table 1).
Table 1:
Baseline characteristics of sex workers (N=543) in Metro Vancouver between 2010–2016, stratified by workplace neighbourhood mobility
| Workplace Neighbourhood Mobility | |||
|---|---|---|---|
| Variables | Yes n (%) | No n (%) | p - value |
| n = 264 (48.6%) | n = 279 (51.4%) | ||
| INDIVIDUAL | |||
| Age | |||
| (years) (median, IQR) | 34(28–42) | 37(29–43) | 0.007 |
| Gender/sexual minority | |||
| LGBTQ2S and other | 99(37.5) | 84(30.1) | 0.069 |
| Straight and Cisgender | 165(62.5) | 195(69.9) | |
| Indigenous | |||
| yes | 111(42.1) | 117(41.9) | 0.979 |
| no | 153(58.0) | 162(58.1) | |
| Im/migrant to Canada | |||
| yes | 56(21.2) | 72(25.8) | 0.199 |
| no | 208(78.8) | 206(73.8) | |
| Education (Completed High School) | |||
| High school graduate | 140(53.0) | 139(49.8) | 0.455 |
| less than high school | 124(47.0) | 140(50.2) | |
| Non-injection drug use * | |||
| yes | 189(71.6) | 183(65.6) | 0.116 |
| no | 74(28.0) | 96(34.4) | |
| Injection drug use * | |||
| yes | 127(48.1) | 115(41.2) | 0.107 |
| no | 137(51.9) | 164(58.8) | |
| Self-rated health is better/same compared to six months ago * | |||
| yes | 214(81.1) | 237(85.0) | 0.265 |
| no | 49(18.6) | 42(15.1) | |
| STRUCTURAL | |||
| Income CAD$ * (median, IQR) | 2400(1200–4200) | 2000(1000–4000) | 0.297 |
| Physical/sexual workplace violence* | |||
| yes | 44(16.7) | 45(16.1) | 0.804 |
| no | 216(81.8) | 234(83.9) | |
| Client condom refusal * | |||
| yes | 48(18.2) | 40(14.3) | 0.263 |
| no | 202(76.5) | 219(78.5) | |
| Homeless * | |||
| yes | 79(29.9) | 50(17.9) | 0.001 |
| no | 185(70.1) | 226(81.0) | |
| Have access to health services when needed * | |||
| yes | 239(90.5) | 249(89.3) | 0.427 |
| no | 22(8.3) | 29(10.4) | |
| Primary place of service * | |||
| Outdoor | 105(39.8) | 81(29.0) | |
| Informal indoor | 105(39.8) | 118(42.3) | 0.001 |
| Formal indoor | 46(17.4) | 74(26.5) | 0.007 |
| Police harassment (without arrest)* | |||
| Yes | 76(28.8) | 73(26.2) | 0.476 |
| No | 187(70.8) | 206(73.8) | |
| Rushed client negotiations because of police presence * | |||
| Yes | 96(36.4) | 92(33.0) | 0.371 |
| No | 166(62.9) | 187(67.0) | |
| Police presence affected where you worked * | |||
| Yes | 107(40.5) | 104(37.3) | 0.416 |
| No | 156(59.1) | 175(62.7) | |
| Red zones/ legal restrictions affected where you worked * | |||
| Yes | 11(4.2) | 5(1.8) | 0.110 |
| No | 237(89.8) | 252(90.3) | |
| Moved neighbourhood of work because of safety concerns * | |||
| Yes | 26(9.9) | 15(5.4) | 0.056 |
| No | 225(85.2) | 245(87.8) | |
Refers to 6 months prior to the interview
All measures refer to n (%) unless otherwise noted
LGBTQ2S= gay, lesbian, bisexual, two-spirit, asexual, transgender, transsexual, intersex, genderqueer
Column percentages may not sum to 100% due to missing observations
In bivariate analysis, participants had lower odds of experiencing neighbourhood mobility if they were older (odds ratio (OR) 0.98/year older, 95% CI 0.97–0.99) or were im/migrants to Canada (OR 0.70, 95% CI 0.52–0.94). Participants had higher odds of experiencing neighbourhood mobility if they self-identified as a gender/sexual minority (OR 1.41, 95% CI 1.11–1.81), were homeless (OR 1.62, 95% CI 1.28–2.04), or experienced workplace physical and/or sexual violence (OR 1.30, 95% CI 1.01–1.69). Those who reported rushing negotiations with clients because of police presence also had higher odds of neighbourhood mobility (OR 1.17, 95% CI 0.96–1.42), as did those who reported having been harassed by police (without being arrested) (OR 1.24, 95% CI 1.03–1.51) or those whose work location was affected by police presence (OR 1.29, 95% CI 1.06–1.57), or who moved neighbourhood of work due to safety concerns (OR 1.53, 95% CI 1.08–2.18). Servicing clients primarily in outdoor/public spaces was correlated with higher odds of workplace neighbourhood mobility in comparison to those servicing in informal or formal indoor settings (OR 1.62, 95% CI 1.35–1.96). Finally, there was no difference in neighbourhood mobility rates pre and post-implementation ofs end-demand legislation (2010–2013 vs. 2015–2016). All other variables were not significantly related to neighbourhood mobility (Table 2).
Table 2.
Variables correlated with moving primary neighbourhood of solicitation/service among sex workers in Metro Vancouver over time (n=543, 2199 observations), 2010–2016.
| Variables | Odds Ratio (OR) | |
|---|---|---|
| Unadjusted OR (95% CI) | Adjusted OR (95% CI) | |
| INDIVIDUAL | ||
| Younger Age | 0.98(0.97–0.99) | 0.99(0.97–1.00) |
| Gender / sexual minority | 1.41(1.11–1.81) | 1.31(1.02–1.67) |
| Indigenous | 1.11(0.87–1.41) | - |
| Im/migrant to Canada | 0.70(0.52–0.94) | - |
| Education | 1.13(0.89–1.43) | - |
| Non-injection drug use * | 1.13(0.90–1.42) | - |
| Injection drug use * | 1.11(0.91–1.36) | - |
| Self-rated health is better/same than six months ago * | 0.85(0.69–1.06) | - |
| STRUCTURAL | ||
| Income (per $1000 CAD) * | 1.02(1.00–1.04) | - |
| Physical/sexual workplace violence * | 1.30(1.01–1.69) | |
| Client condom refusal * | 1.14(0.92–1.42) | - |
| Homeless * | 1.62(1.28–2.04) | 1.41(1.11–1.79) |
| Have access to health services when needed* | 0.87(0.63–1.20) | - |
| Primary place of service: outdoor (vs. Informal indoor or formal indoor)* | 1.62(1.35–1.96) | 1.48(1.21–1.81) |
| Police harassment (without arrest) * | 1.24(1.03–1.51) | 1.19(0.96–1.48) |
| Rushed negotiation with client because of police presence * | 1.17(0.96–1.42) | - |
| Police presence affected where you worked * | 1.29(1.06–1.57) | - |
| Red zones/ legal restrictions affected where you worked* | 0.95(0.58–1.54) | - |
| Moved neighbourhood of work because of safety concerns ** | 1.53(1.08–2.18) | 1.37(0.94–2.00) |
Refers to 6 months prior to the interview
Gender/sexual minority: LGBTQ2S(gay, lesbian, bisexual, two-spirit, asexual, transgender, transsexual, intersex, genderqueer) or others vs straight and cisgender woman
In multivariable GEE analysis (Table 2), neighbourhood mobility was correlated with younger age (adjusted odds ratio (AOR) 0.98, 95%, confidence interval (CI) 0.97–0.99), whereas homelessness (AOR 1.43, 95% CI 1.12–1.82), identifying as a gender/sexual minority (AOR 1.31, 95% CI 1.04–1.70), and servicing clients in outdoor/public places (AOR 1.48, 95% CI 1.21–1.81) were correlated with increased odds of neighbourhood mobility. Finally, exposure to police harassment (AOR 1.19, 95% CI 0.96–1.48, p=0.11) was marginally correlated with neighbourhood mobility.
The spatial analysis of neighbourhood mobility patterns indicated that the City of Burnaby (a suburban community adjacent to the City of Vancouver) experienced the most in- and out-migration (i.e. instances of mobility), during the study period (n=84 vs. n=64) (Figure 1). Other municipalities with high rates of participant in- and out-migration included Kensington-Cedar Cottage (n=112 vs. n=88) and the DTES (n=267 vs. n=230). Figure 1 show a kernel density map of participants who moved in and out of the City of Burnaby. Among those participants soliciting/servicing in Burnaby, those that relocated had primarily moved back to neighbourhoods within the City of Vancouver, including downtown, the DTES, or the Kingsway Corridor. Figure 2 shows a kernel density map of participant in-and out-migration within the City of Vancouver. The City of Vancouver, and particularly the DTES neighborhood, experienced the greatest amount of mobility in absolute numbers.
Figure 1.

Kernel density map illustrating hotspots of workplace neighbourhood mobility amongst sex workers who worked within the City of Burnaby (2010–2016, N=183).
Note: Data in this figure includes only those sex workers who solicited and/or serviced in the City of Burnaby between 2010–2016. Red hotspots indicate areas with the highest net rate of outward mobility while the green hotspots depict areas with the greatest net rate of in-migration during the study period. This figure shows high rates of work-related out-migration from the City of Burnaby into the City of Vancouver. As our modeling shows, out-migration was likely due to police harassment and unsafe environment. The Downtown Eastside (DTES) neighborhood is characterized by high rates of urban poverty, marginalized or unstable housing, and highly concentrated and visible substance use and indoor and outdoor sex work scenes. In contrast, the suburban community of Burnaby is home to large immigrant/newcomer populations, and has more dispersed sex work and drug use scenes, with a greater proportion of sex work taking place in formal indoor environments (e.g., massage parlours).
Figure 2.
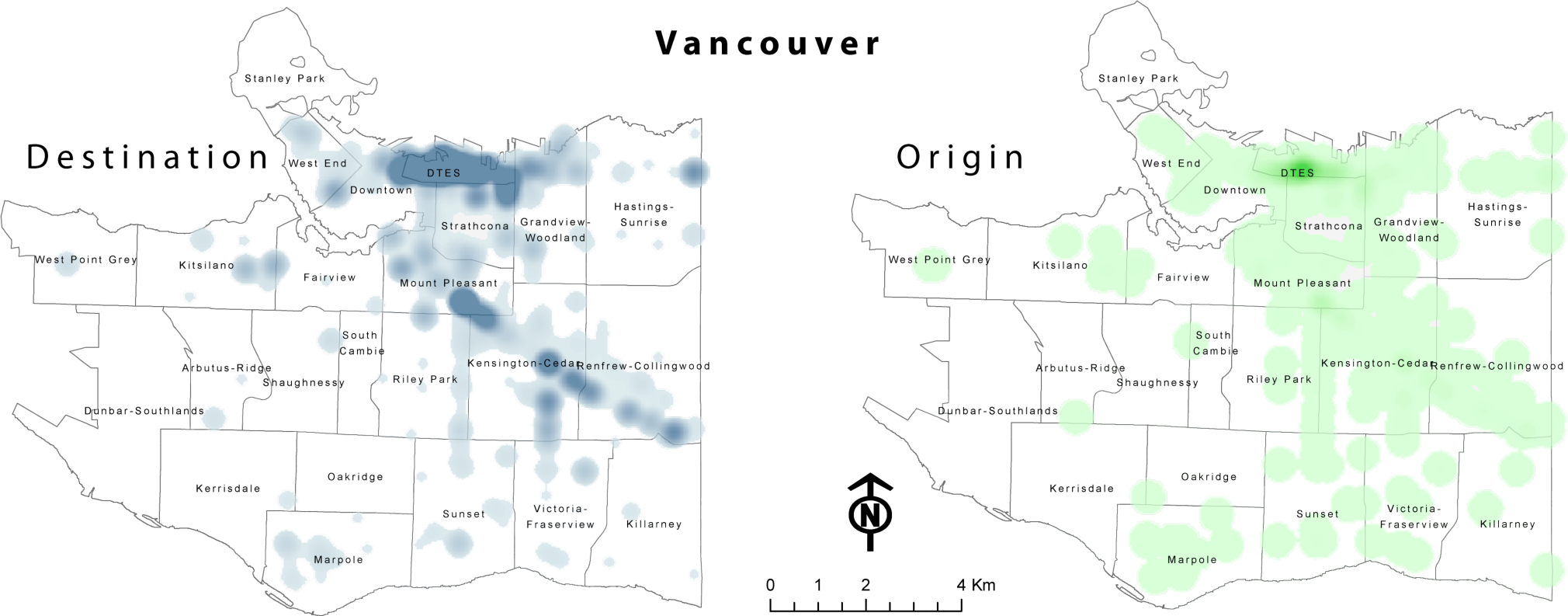
Kernel density map illustrating hotspots of workplace neighbourhood mobility amongst sex workers who worked within the City of Vancouver (2010–2016; N=543, 2199 observations)
This figure includes only those sex workers who solicited and/or serviced within the City of Vancouver from 2010–2016. Blue hotspots indicate areas of inward mobility while green hotspots depict areas of outward mobility within the study period. Most Inward mobility is concentrated in the Downtown Eastside (DTES) neighborhood. The DTES neighborhood is characterized by high rates of urban poverty, marginalized or unstable housing, and highly concentrated and visible substance use and indoor and outdoor sex work scenes.
Discussion
Over the course of this six-year study, about 74.0% of sex workers changed the primary neighbourhood where they solicited or serviced at least once between study visits between 2010 and 2016. Those who changed the neighbourhood of their primary place of work were more likely to be younger, homeless, identify as a gender/sexual minority and more likely to service in outdoor/public settings. They were also more likely to experience police harassment. Similarly to other studies, the results of our study indicate that while many sex workers may engage in work-related mobility for new opportunities, including youth, others may be mobile due to ‘push’ factors associated with displacement stemming from concerns related to policing and unsafe working conditions. (S. M. Goldenberg et al., 2014; Ramesh et al., 2012; Reed et al., 2012; Shannon et al., 2008) Finally, no difference in mobility patterns was found post-implementation of end-demand sex work criminalization(OR 0.79, 95% CI 0.57–1.08, p-value = 0.13), which may be explained by prior research showing sex work criminalization, including criminalizing clients, continue to displace sex workers to isolated areas where they face high rates of violence and police harassment(Krüsi et al., 2014). This suggests that despite the purported aim of this legislation to protect the welfare of marginalized communities, the implementation of the news laws did not reduce displacement experiences amongst sex workers during our study.
Younger sex workers within our study were more likely to experience workplace neighbourhood mobility. Prior studies have shown that youth often engage in mobility to seek out new experiences, improved working conditions, enhanced earnings, and new employment opportunities. (Althorp, 2013; S. M. Goldenberg et al., 2014). Our study also found that identifying as a gender/sexual minority was highly correlated with increased odds of workplace neighbourhood mobility, which is supported by previous studies highlighting similar findings. Our findings echo results from qualitative work conducted in the Vancouver area, and two-spirit sex workers experienced displacement as a result of criminalization, gentrification, unsafe working conditions, and broader experiences of social exclusion. (Lyons, Krüsi, Pierre, Small, & Shannon, 2017) Studies from other settings have also demonstrated that sex workers who identify as gender/sexual minorities tend to experience higher levels of mobility (Cai et al., 2016; Husakouskaya, 2017; Rana et al., 2016); this has been previously linked to the fact that trans workers often operate across relatively large geographical areas and may travel further to see clients. Trans sex workers also often experience high levels of stigma, discrimination, poverty, social exclusion, and social isolation, and a lack of acceptance within local communities (e.g., cisgender and/or gay communities) may contribute to enhanced mobility. (Husakouskaya, 2017) Research has also documented that trans sex workers often face distinct restrictions on the geographical areas in which they can work; for example, in Vancouver there exist ‘designated’ areas for trans workers which may limit this population’s ability to move about within the immediate area in search of work; (Lyons et al., 2017) Interestingly, although LGBTQ2S people make up only 10% of the general population, 33.7% of the participants in our study identified as LGBTQ2S. Further research and efforts to understand experiences of mobility and displacement among this population and links to health and safety remain needed to inform evidence-based programmes.
In addition, our analysis showed that moving due to a perceived lack of safety, workplace physical/sexual violence, and exposure to police harassment (without arrest) were marginally correlated with increased odds of neighbourhood mobility among sex workers. These findings suggest that sex workers who change the neighbourhood in which they work may do so largely due to displacement to more unsafe and isolated spaces resulting from criminalized interactions with law enforcement, which has been previously shown to be a critical barrier to health and safety. (S. M. Goldenberg et al., 2017; Shannon et al., 2008) It is possible that those engaged in work-related mobility may also experience reduced access to peer supports upon arrival to new work areas as well as less information or familiarity with local workspaces, which may contribute to unsafe working conditions. (S. M. Goldenberg et al., 2014) Several other studies suggest that sex workers who are highly mobile may experience unsafe working conditions and enhanced susceptibility to violence. (Ramesh et al., 2012; N Saggurti et al., 2008; Niranjan Saggurti et al., 2012) Previous epidemiological research with sex workers in Canada demonstrated that sex workers who engaged in short-term sex work-related mobility outside of Vancouver faced almost twice the odds of workplace violence as their non-mobile counterparts (S. M. Goldenberg et al., 2014); however, this study did not include mapping and did not focus on urban mobility patterns. In lower-income contexts, including India, studies have also shown associations between work-related mobility and workplace violence (Swain et al., 2011), as well as between migration for sex work and violence. (Ramesh et al., 2012)
Complementing results of our statistical analysis, our mapping analysis provides unique insight into the social geography of neighbourhood mobility and displacement patterns among sex workers in Metro Vancouver between 2010 and 2016. Mapping results indicate that the City of Burnaby experienced the highest rate of outward mobility of all the cities/neighbourhoods included in our study, and that the City of Vancouver, and particularly the DTES neighbourhood experienced the most mobility activity in absolute numbers. The observed movement from Burnaby to Vancouver may partly be explained by differences in criminalized enforcement patterns between municipalities, including those related to the introduction of end-demand legislation in 2014. (Chu et al., 2014; Initiative;, 2014; Perrin, 2014). The Vancouver Police Department has adopted sex work enforcement guidelines that consider sex work between consenting adults to no longer be an enforcement priority, and announced that it would not enforce the federal law; although these policy-level decisions have not always translated to improvements at a street-level, it is possible that the absence of such policies in surrounding municipalities, such as Burnaby, could potentially render the City of Vancouver to be a relatively less punitive environment for sex work than its surrounding municipalities. (Pablo, 2015)
To promote sex workers’ occupational safety and human rights, steps to promote safer and more supportive working conditions remain critically needed, particularly for marginalized sub-populations of youth, gender/sexual minorities, and those experiencing homelessness; policy reforms to shift away from enforcement-based approaches and end-demand criminalization towards community-based and sex worker-led initiatives that focus on protecting sex workers’ rights and workplace safety are needed. Special efforts to address the unique needs of mobile sex workers who are operating in new environments or neighbourhoods are also recommended to promote wellbeing and reduce isolation, including through peer-based outreach to workspaces and linkage to supportive and sex worker-friendly community-based health and social supports.
The use of mapping techniques such as those used in this study, can assist in targeting programs and policies to the areas of greatest need.
Strengths and Limitations
This study has several strengths and limitations that should be noted. Our prospective design allowed us to examine correlates of neighbourhood mobility over a six-year observation period, whereas most prior research on mobility among marginalized populations rely upon cross-sectional designs. Variables originated from self-reported data, which are often cited to be subject to reporting bias. However, community-based relationships with the participants are likely to minimize this bias, as our frontline staff receive extensive training and have ample experience in building rapport and maintaining meaningful connections with participants. Our analysis adopted a unique spatial epidemiological approach in order to understand not only the characteristics of sex workers who engage in workplace mobility, but also the social geography of work-related mobility patterns across Metro Vancouver neighbourhoods.
Furthermore, the study utilizes highly accurate locational data combined with personal information measured over a relatively long time span to understand sex workers’ mobility patterns and correlates. As such, our sample was restricted to those who provided valid spatial data across at least two study visits on places of servicing and/or soliciting clients, thereby reducing power for some analyses. As our locational data captured only those movements that occurred within the last month and which involved a move from primary place of solicitation and/or service, further longitudinal research focused on longer-term experiences of displacement as well as other forms of displacement (e.g., place of residence) are recommended. Additionally, future studies focused on assessing the impact of mobility-related processes on health care utilization and health outcomes amongst sex workers within urban environments remain needed to inform health services delivery efforts.
CONCLUSIONS
Over the course of this six-year study, almost three-quarters of our study participants changed the neighbourhood within which they primarily worked at least once; these women were more likely to be younger, homeless, identify as a gender/sexual minority and service clients in outdoor/public settings. They were also marginally more likely to experience police harassment, and to report moving work neighbourhoods because they felt unsafe. To ensure sex workers’ occupational safety and rights, steps to reduce vulnerability to violence and ensure access to safer indoor workspaces remain critically needed, including moving away from enforcement-based criminalization towards community-based and sex workers-led initiatives that focus on protecting sex workers’ rights and safety. Special efforts to address the needs of youth, gender/sexual minorities, and precariously housed women, as well as mobile sex workers who are operating in new work environments or neighbourhoods, are also recommended to promote wellbeing and reduce isolation.
ACKNOWLEDGEMENT
Study concept and design: OA, SG; acquisition of data: MB,KS,SG; analysis and interpretation of data: OA,SG,MB; Data preparation: OA,SG,MB; drafting of the manuscript: OA, SG; critical revision of the manuscript for important intellectual content and for final approval: OA, SG,KS,MB,SM,SM,TL; analysis: MB,OA; Obtained funding: OA,KS, SG; study supervision: SG,KS. All authors have read and approved the final version.
We thank all those who contributed their time and expertise to this project, particularly participants, AESHA community advisory board members and partner agencies, and the AESHA team, including: Sarah Moreheart, Jennifer Morris, Sylvia Machat, Jane Li, Minshu Mo, Sherry Wu, Sylvia Machat, Emily Leake, Anita Dhanoa, Meaghan Thumath, Alka Murphy, Jenn McDermid, Tave Cole, Jaime Adams. We also thank Abby Rolston, Peter Vann, Erin Seatter and Patricia McDonald for their research and administrative support. This research is supported by the US National Institutes of Health (R01DA028648), a Canadian Institutes of Health Research Foundation Grant, the Canadian Institutes of Health Research and Public Health Agency of Canada (HEB-330155), and MacAIDS. SG is partially supported by NIH (R01DA028648) and a CIHR New Investigator Award (MSH- 340057). KS is partially supported by a Canada Research Chair in Global Sexual Health, NIH (R01DA028648), and HIV/AIDS and Michael Smith Foundation for Health Research. OA received postdoctoral fellowship support from the Michael Smith Foundation for Health Research and the Canadian Institutes of Health Research.
REFERENCES:
- Althorp Janine Christa Mary. (2013). Beyond the Stage: A gaze into the working lives of exotic stage dancers in Western Canada. Arts & Social Sciences: School of Criminology. [Google Scholar]
- Anderson Solanna, Jia Jessica Xi, Liu Vivian, Chattier Jill, Krüsi Andrea, Allan Sarah, … Shannon Kate. (2015). Violence prevention and municipal licensing of indoor sex work venues in the Greater Vancouver Area: narratives of migrant sex workers, managers and business owners. Culture, health & sexuality, 17(7), 825–841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ballinger Gary A. (2004). Using generalized estimating equations for longitudinal data analysis. Organizational research methods, 7(2), 127–150. [Google Scholar]
- Cai Yong, Wang Zixin, Lau Joseph TF, Li Jinghua, Ma Tiecheng, & Liu Yan. (2016). Prevalence and associated factors of condomless receptive anal intercourse with male clients among transgender women sex workers in Shenyang, China. Journal of the International AIDS Society, 19(3Suppl 2). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choi Jin Young. (2009). Contextual effects on health care access among immigrants: Lessons from three ethnic communities in Hawaii. Social science & medicine, 69(8), 1261–1271. [DOI] [PubMed] [Google Scholar]
- Choi Susanne YP. (2011). Heterogeneous and vulnerable: the health risks facing transnational female sex workers. Sociology of health & illness, 33(1), 33–49. [DOI] [PubMed] [Google Scholar]
- Chu Sandra Ka Hon, Canadian HIV, & Network AIDS Legal. (2014). Brief to the House of Commons Standing Committee on Justice and Human Rights regarding its study of Bill C-36, the Protection of Communities and Exploited Persons Act. [Google Scholar]
- Chu Sandra Ka Hon, & Glass Rebecca. (2013). Sex work law reform in Canada: Considering problems with the Nordic model. Alta. L. Rev, 51, 101. [Google Scholar]
- Collinson Mark A. (2010). Striving against adversity: the dynamics of migration, health and poverty in rural South Africa. Global health action, 3(1), 5080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Decker Michele R, Crago Anna-Louise, Chu Sandra KH, Sherman Susan G, Seshu Meena S, Buthelezi Kholi, … Beyrer Chris. (2015). Human rights violations against sex workers: burden and effect on HIV. The Lancet, 385(9963), 186–199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ESRI. (2012). ArcGIS Desktop: Release 10. Redlands, CA: Environmental Systems Research Institute. [Google Scholar]
- Ferguson Alan G, & Morris Chester N. (2007). Mapping transactional sex on the Northern Corridor highway in Kenya. Health & place, 13(2), 504–519. [DOI] [PubMed] [Google Scholar]
- Goldenberg Shira M, Chettiar Jill, Nguyen Paul, Dobrer Sabina, Montaner Julio, & Shannon Kate. (2014). Complexities of short-term mobility for sex work and migration among sex workers: violence and sexual risks, barriers to care, and enhanced social and economic opportunities. Journal of Urban Health, 91(4), 736–751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldenberg Shira M, Deering Kathleen, Amram Ofer, Guillemi Silvia, Nguyen Paul, Montaner Julio, & Shannon Kate. (2017). Community mapping of sex work criminalization and violence: impacts on HIV treatment interruptions among marginalized women living with HIV in Vancouver, Canada. International journal of STD & AIDS, 0956462416685683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldenberg Shira M, Strathdee Steffanie A, Perez-Rosales Maria D, & Sued Omar. (2012). Mobility and HIV in Central America and Mexico: a critical review. Journal of immigrant and minority health, 14(1), 48–64. [DOI] [PubMed] [Google Scholar]
- Goldenberg Shira, Strathdee Steffanie A, Gallardo Manuel, & Patterson Thomas L. (2010). “People Here Are Alone, Using Drugs, Selling their Body”: Deportation and HIV Vulnerability among Clients of Female Sex Workers in Tijuana. Field Actions Science Reports. The journal of field actions (Special Issue 2). [Google Scholar]
- Goldenberg SM, Silverman Jay G, Engstrom David, Bojorquez-Chapela I, & Strathdee Steffanie A. (2014). “Right Here is the Gateway”: mobility, sex work entry and HIV risk along the Mexico–US Border. International Migration, 52(4), 26–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanley James A, Negassa Abdissa, & Forrester Janet E. (2003). Statistical analysis of correlated data using generalized estimating equations: an orientation. American journal of epidemiology, 157(4), 364–375. [DOI] [PubMed] [Google Scholar]
- Husakouskaya Nadzeya. (2017). Queering Mobility in Urban Gauteng: Transgender Internal Migrants and Their Experiences of “Transition” in Johannesburg and Pretoria. Urban Forum, 28(1), 91–110. doi: 10.1007/s12132-016-9286-8 [DOI] [Google Scholar]
- Initiative;, Gender and Sexsual Health. (2014). Open Letter Calling for Decriminalization of Sex Work in Canada and Opposition to Criminalizing the Purchasing of Sex.
- Jie Wu, Xiaolan Zhou, Ciyong Lu, Moyer Eileen, Hui Wang, Lingyao Hong, & Xueqing Deng. (2012). A qualitative exploration of barriers to condom use among female sex workers in China. PloS one, 7(10), e46786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krüsi Andrea, Pacey Katrina, Bird Lorna, Taylor Chrissy, Chettiar Jill, Allan Sarah, … Shannon Kate. (2014). Criminalisation of clients: reproducing vulnerabilities for violence and poor health among street-based sex workers in Canada—a qualitative study. BMJ open, 4(6), e005191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lippman Sheri A, Pulerwitz Julie, Chinaglia Magda, Hubbard Alan, Reingold Arthur, & Díaz Juan. (2007). Mobility and its liminal context: exploring sexual partnering among truck drivers crossing the Southern Brazilian border. Social science & medicine, 65(12), 2464–2473. [DOI] [PubMed] [Google Scholar]
- Lyons Tara, Krüsi Andrea, Pierre Leslie, Small Will, & Shannon Kate. (2017). The impact of construction and gentrification on an outdoor trans sex work environment: Violence, displacement and policing. Sexualities, 1363460716676990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lyttleton Chris, & Amarapibal Amorntip. (2002). Sister cities and easy passage: HIV, mobility and economies of desire in a Thai/Lao border zone. Social science & medicine, 54(4), 505–518. [DOI] [PubMed] [Google Scholar]
- Pablo Carlito. (2015, February 20th, 2015). “Little” enforcement of Canada’s new prostitution laws, says lawyer, The Georgia Straight. Retrieved from http://www.straight.com/news/396106/little-enforcement-canadas-new-prostitution-laws-says-lawyer [Google Scholar]
- Pan Wei. (2001). Akaike’s information criterion in generalized estimating equations. Biometrics, 57(1), 120–125. [DOI] [PubMed] [Google Scholar]
- Parrado Emilio A, & Flippen Chenoa. (2010). Community attachment, neighborhood context, and sex worker use among Hispanic migrants in Durham, North Carolina, USA. Social Science & Medicine, 70(7), 1059–1069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perrin Benjamin. (2014). How to Make Canada’s New Prostitution Laws Work. [Google Scholar]
- Platt Lucy, Bobrova Natalia, Rhodes Tim, Uusküla Anneli, Parry John V, Rüütel Kristi, … Judd Ali. (2006). High HIV prevalence among injecting drug users in Estonia: implications for understanding the risk environment. Aids, 20(16), 2120–2123. [DOI] [PubMed] [Google Scholar]
- Platt Lucy, Grenfell Pippa, Fletcher Adam, Sorhaindo Annik, Jolley Emma, Rhodes Tim, & Bonell Chris. (2012). Systematic review examining differences in HIV, sexually transmitted infections and health-related harms between migrant and non-migrant female sex workers. Sexually Transmitted Infections, sextrans-2012–050491. [DOI] [PubMed] [Google Scholar]
- Ragsdale Kathleen, Anders Jessica T, & Philippakos Effie. (2007). Migrant Latinas and brothel sex work in Belize: Sexual agency and sexual risk. Journal of Cultural Diversity, 14(1), 26. [PubMed] [Google Scholar]
- Ramesh Sowmya, Ganju Deepika, Mahapatra Bidhubhusan, Mishra Ram Manohar, & Saggurti Niranjan. (2012). Relationship between mobility, violence and HIV/STI among female sex workers in Andhra Pradesh, India. BMC Public Health, 12(1), 764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rana AKM Masud Reza Md. Masud Alam Md. Shah Khatun, Mahmuda Khan, Sharful Islam, & Azim Tasnim. (2016). Effects of In-country and Cross-Border Mobility on Condom Use Among Transgender Women (hijras) in Bangladesh: A Cross-Sectional Study. AIDS and Behavior, 20(10), 2165–2177. doi: 10.1007/s10461-015-1275-8 [DOI] [PubMed] [Google Scholar]
- Reed Elizabeth, Gupta J, Biradavolu M, & Blankenship KM. (2012). Migration/mobility and risk factors for HIV among female sex workers in Andhra Pradesh, India: implications for HIV prevention. International journal of STD & AIDS, 23(4), e7–e13. [DOI] [PubMed] [Google Scholar]
- Richter Marlise, Chersich Matthew F, Vearey Jo, Sartorius Benn, Temmerman Marleen, & Luchters Stanley. (2014). Migration status, work conditions and health utilization of female sex workers in three South African cities. Journal of Immigrant and Minority Health, 16(1), 7–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rushing Rosanne, Watts Charlotte, & Rushing Sharon. (2005). Living the reality of forced sex work: perspectives from young migrant women sex workers in northern Vietnam. Journal of Midwifery & Women’s Health, 50(4), e41–e44. [DOI] [PubMed] [Google Scholar]
- Saggurti N, Verma RK, Reddy H, RamaRao S, Singh AK, Mahendra VS, & Jain A (2008). Patterns of migration/mobility and HIV risk among female sex workers: Andhra Pradesh 2007–08. Population Council, New Delhi. [Google Scholar]
- Saggurti Niranjan, Jain Anrudh K, Sebastian Mary Philip, Singh Rajendra, Modugu Hanimi Reddy, Halli Shiva S, & Verma Ravi K. (2012). Indicators of mobility, socio-economic vulnerabilities and HIV risk behaviours among mobile female sex workers in India. AIDS and Behavior, 16(4), 952–959. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SAS inc. (2015). SAS (Version 9.4)
- Shannon Kate, Bright Vicki, Allinott Shari, Alexson Debbie, Gibson Kate, & Tyndall Mark W. (2007). Community-based HIV prevention research among substance-using women in survival sex work: The Maka Project Partnership. Harm reduction journal, 4(1), 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shannon Kate, Rusch Melanie, Shoveller Jean, Alexson Debbie, Gibson Kate, & Tyndall Mark W. (2008). Mapping violence and policing as an environmental-structural barrier to health service and syringe availability among substance-using women in street-level sex work. International Journal of Drug Policy, 19(2), 140–147. [DOI] [PubMed] [Google Scholar]
- Shannon Kate, Strathdee Steffanie A, Goldenberg Shira M, Duff Putu, Mwangi Peninah, Rusakova Maia, … Pickles Michael R. (2015). Global epidemiology of HIV among female sex workers: influence of structural determinants. The Lancet, 385(9962), 55–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sou Julie, Goldenberg Shira M, Duff Putu, Nguyen Paul, Shoveller Jean, & Shannon Kate. (2017). Recent im/migration to Canada linked to unmet health needs among sex workers in Vancouver, Canada: Findings of a longitudinal study. Health Care for Women International, 1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swain Suvakanta, Saggurti Niranjan, Battala Madhusudana, Verma Ravi K, & Jain Anrudh. (2011). Experience of violence and adverse reproductive health outcomes, HIV risks among mobile female sex workers in India. BMC public health, 11(1), 357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verma Ravi K, Saggurti Niranjan, Singh Ajay K, & Swain Suvakanta N. (2010). Alcohol and sexual risk behavior among migrant female sex workers and male workers in districts with high in-migration from four high HIV prevalence states in India. AIDS and Behavior, 14(1), 31–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolffers Ivan, & Fernandez Irene. (1995). Migration and AIDS. Lancet, 346(8985), 1303. [PubMed] [Google Scholar]
- Yi Huso, Mantell Joanne E, Wu Rongrong, Lu Zhao, Zeng Jing, & Wan Yanhai. (2010). A profile of HIV risk factors in the context of sex work environments among migrant female sex workers in Beijing, China. Psychology, health & medicine, 15(2), 172–187. [DOI] [PMC free article] [PubMed] [Google Scholar]