

Abstract
Objective To verify whether, regardless of the screw placement technique, there is a safe distance or angle in relation to the facets that can prevent violation of the facet joint when the screws are placed.
Methods Retrospective, single, comparative, non-randomized center. We evaluated by axial computed tomography: the angle of the screw/rod in relation to the midline, the angle of the center of the facets in relation to the midline, the distance between the head of the screw/rod to the midline, and the distance from the center of the facets to the midline; the violation of the facet joint will be evaluated in a gradation of 0 to 2. Also will be measured the difference between the angle os the facets and the angle of the screws (Δ Angle) and, the difference between the facet distance and the screw distance (Δ Distance).
Results A total of 212 patients and 397 facets were analyzed (196 on the left and 201 on the right). Of these, 303 were not violated (grade 0), corresponding to 76,32%, and 94 suffered some type of violation (grade 1 and 2), corresponding to 23,68%. The mean of Δ angle was 9.87° +/− 4.66° (grade 0), and of 3.77° +/− 4.93° in facets (grade 1 and 2) ( p < 0.001), and the Δ mean distance in cases in which there was no violation was 0.94 arbitrary units (a.u.) +/− 0.39 a.u., while the Δ distance in G1 and G2 cases was 0.56 a.u. +/− 0.25 a.u. ( p < 0.001).
Conclusion The measurements of angle and distance between facet and screw can help in the placement of screws. These parameters can be used as safety measures with the most frequent use of surgical navigation techniques.
Keywords: pedicle screws, spinal fusion, x-ray computed tomography, retrospective studies
Introduction
Problems related to the lumbar spine are becoming more and more frequent with the increase in life expectancy and the consequent ageing of the population. 1 Because they cause reduced mobility, mechanical pain, and reduced quality of life, these have become one of the main causes of disability in the world population. 2 Sometimes, the treatment of these pains can be conservative; however, many patients are sometimes refractory to these treatments, with most of them requiring, therefore, surgical treatment to resolve their symptoms. 3
Depending on the type of condition to be treated, it is necessary to use supplementation/posterior fixation. 4 5 Multiple techniques for lumbar supplementation/fixation have been proposed and used and, for reducing the risk of neurovascular injuries and for promoting great stabilization of the construction, pedicle screws have become the preferred method for posterior fixation in lumbar surgeries allowing the stability of the operated level. 6 7 8
Several techniques are proposed for the placement of pedicle screws, including the techniques of Magerl, 9 Roy-Camille et al., 10 and Weinstein et al., 11 among others. 12 In addition, with the popularization of minimally-invasive techniques for spine surgery, the quantity of pedicle screws placement by percutaneous technique is increasing. 13 14
However, a problem that is often not taken into account in relation to the placement of these screws is the violation of the facet capsule. 6 8 14 Recent studies show rates ranging from 0 to 80% of facet violation of the adjacent level to the more cranial instrumented vertebra, which vary according to the technique used and the surgeon's experience. 15 16
This facet violation of the most instrumented cranial level is one of the factors that is pointed out by studies as a risk factor for the development of disease of the adjacent level, which can lead to degeneration of the adjacent level, and may result in worsening quality of life, and future need for reoperation for the treatment of this level. 8 17
Thus, the objective of our work is to verify whether, regardless of the screw placement technique, there is a safe distance or angulation in relation to the facets, so that violation of the facet joint can be avoided when the screws are placed.
Materials and Methods
Retrospective, single, comparative, non-randomized study. Approved by the institutional committee of ethics in research under the number 91876318.0.0000.8098.
The study included patients who had fixation by pedicle screws in the lumbar spine and who had computed tomography exams with axial sections of bone window. Patients whose computed tomography exams were of poor quality, not allowing good visualization of the structures necessary for the study, were excluded. Cases involving fractures, malformations or other conditions that would not allow a good visualization of the structures necessary for the study were also excluded.
The evaluation was carried out by two different researchers, with a third evaluator being called to resolve the discrepancies between the measures. The following parameters were measured in the radiological images of computed tomography in axial section in bone window, screw/rod angle to the midline, angle of the center of the facets to the midline and the difference between the screw angle and facet angle (Δ angle) ( Figure 1 A-C ), distance between the head of the screw/rod to the midline, distance from the center of the facets to the midline*(* distances will be measured in arbitrary units with the distance between the center of the facets and the midline of the vertebra equal to 1 arbitrary unit [a.u.]), and the difference between the value of screw distance and the facet distance (Δ distance) ( Figure 1 D-F ).
Fig. 1.

Figure representing the measurements taken during work. ( A ) Facet angulation; ( B ) Screw/rod angulation; ( C ) Δ facets; ( D ) facet distance; ( E ) Screw/rod distance; ( F ) Δ distance. (Blue: facet measurements; Green: the screws/rods measures).
The violation of the facet joint was evaluated in a gradation of 0 to 2, according to the classification proposed by Tannous et al. 18
The data were compiled in the Excel program and analyzed statistically through the GraphPad Prism 8 (GraphPad Software Inc, La Jolla, CA, USA) software. Student's t-test was used to test differences between quantitative parametric measures and the Mann-Witney test was used for values outside the normal distribution. To compare qualitative measures, the Fischer test or the Chi-squared test was used. Results with p -values lower than 0.05 were considered as statistically significant.
Results
Demographic
A total of 212 patients were included in the study, with a total of 397 facets analyzed (196 on the left and 201 on the right). There was no difference in the number of violations between the left and the right side. Of these, 303 (77%) facets were not violated (grade 0); in 52 (13%) cases, the screw touched the facet slightly (grade 1); and in 42 (10%) cases, there was a facet violation (grade 2) ( p > 0.05) ( Table 1 ).
Table 1. Table showing the number of violations identified during the study.
| Left | Right | Total | |
|---|---|---|---|
| Total | 196 | 201 | 397 |
| Violation grade 0 (%) | 151 (77%) | 152 (76%) | 303 (76%) |
| Violation grade 1 (%) | 22 (11%) | 30 (15%) | 52 (13%) |
| Violation grade 2 (%) | 23 (12%) | 19 (9%) | 42 (11%) |
It was also seen that levels T1-L1 were the levels most susceptible to facet violation ( p < 0.05) ( Table 2 and Figure 2 ).
Table 2. Table showing the number of violations identified by level during the study.
| Violation G0 | Violation G1 and G2 | % of violation | |
|---|---|---|---|
| Thoracic | 11 | 7 | 39.9 |
| L1 | 11 | 10 | 47.6 |
| L2 | 30 | 5 | 14.3 |
| L3 | 50 | 20 | 28.6 |
| L4 | 131 | 31 | 19.1 |
| L5 | 70 | 21 | 23.1 |
Fig. 2.

Graph representing the amount of violation between levels T-L1 and L2-L5. * p < 0.05.
Screw Angulation and Facet Angulation
The mean angulation of the facets in relation to the midline was 18.9° +/− 3.95°; the mean angulation of the screws in relation to the midline was 27.5° +/− 5.7°; and the mean Δ facets was + 8.5°. Since the mean Δ angle was 9.87° +/− 4.66° in facets without violation (grade 0) and of 3.77° +/− 4.93° in facets in which there was violation (grade 1 and 2) ( p < 0.001) ( Table 3 ).
Table 3. Table showing the mean of the facet angulation, screw angulation and Δ angle.
| Facet angulation | Screw angulation | Δ Angle | |
|---|---|---|---|
| Mean (SD) | 18° +/− 3.95° | 27.5° +/− 5.7° | 8.5° +/− 5.28° |
| Δ angle and violation | |||
| Grade 0 | Grades 1 and 2 | P | |
| Mean (SD) | 9.87° +/− 4.66° | 3.77° +/− 4.93° | < 0.001 |
Abbreviation: SD, standard deviation.
For the purpose of better analysis and stratification, 3 points were defined for the analysis: Δ smaller than 5°, Δ angle between 5° and 15°, and Δ angle greater than 15°. When Δ facet was less than 5°, there was violation of facets in 65% (63/96) of the cases, while with Δ between 5 and 15°, there was violation of facets in 11% (30/265) of the cases, and with an angle greater than 15°, there was a violation of facets in only 2.7% of the cases (1/36) ( Figure 3 ).
Fig. 3.

Image showing the proportion of violation in relation to Δ angle. Green: represents non-violation. Red: represents violation.
Screw Distance and Facet Distance
The average distance between the screws and the midline was 1.85 a.u. +/− 0.40 a.u.; thus, the Δ distance was 0.85 a.u. +/− 0.40 a.u. The Δ mean distance in cases in which there was no violation was 0.94 a.u. +/− 0.39 a.u., while the Δ distance in cases of violation (g1 and g2) was 0.56 a.u. +/− 0.25 a.u. ( p < 0.001) ( Table 4 ).
Table 4. Table showing the mean screw distance and the Δ distance.
| Screw distance | Δ Distance | ||
|---|---|---|---|
| Mean (+/− SD) | 1.85 +/− 0.40 a.u. | 0.85 +/− 0.40 a.u. | |
| Δ distance and violation | |||
| Grade 0 | Grades 1 and 2 | P | |
| Mean (+/− SD) | 0.94 +/− 0.39 a.u. | 0.56 +/− 0.25 a.u. | < 0.001 |
Abbreviations: a.u., arbitrary units; SD, standard deviation.
Three points were defined for better data analysis: 0.5 a.u.; 0.5 to 1.5 a.u., greater than 1.5 a.u. As evident in cases of screws placed at a distance of less than 0.5 a.u. from the center of the facets, there was a violation in 65% of the cases (38/59), while on screws placed at a distance between 0.5 and1.5 a.u., there was a violation in 17% of cases (56/319), and on screws placed with more than 1.5 a.u., there was no facet violation (0/19) ( p < 0.001) ( Figure 4 ).
Fig. 4.
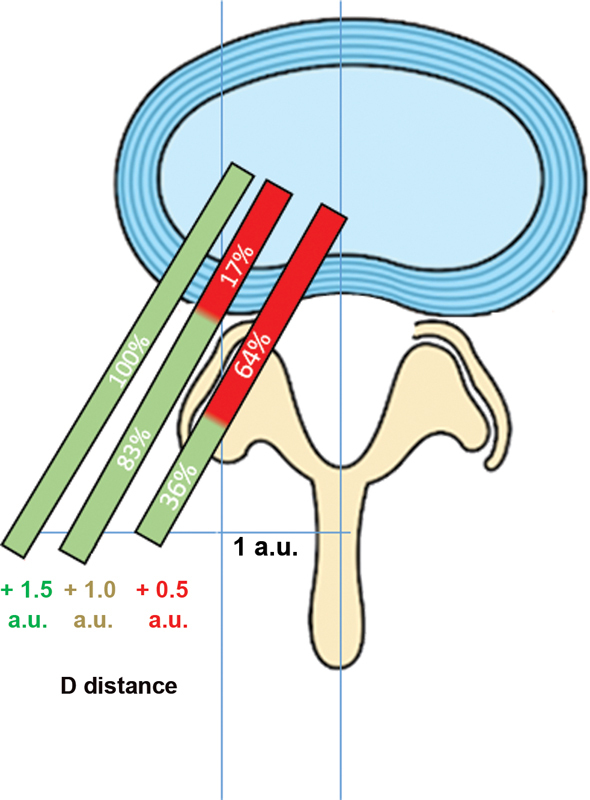
Image showing the proportion of violation in relation to Δ distance. Green: represents non-violation. Red: represents violation.
Receiver Operating Characteristic (ROC) Curve
To verify the ability of the measures to indicate when there was or not a facet violation, the ROC curves method was used. The measures of the angles of the facets, Δ angle and Δ distance presented the following areas under the curve (AUCs): 0.5848; 0.8599; and 0.8195 ( Figure 5 ).
Fig. 5.

Images demonstrating the receiver-operating characteristic (ROC) curve of the various measures demonstrated in the study. ( A ) Angle of facets; ( B ) Δ angle, and ( C ) Δ distance.
Discussion
Despite being considered the gold standard of posterior fixation for lumbar spine, pedicle screws can cause violation of facet capsules if they are not placed correctly, a factor that can start or accelerate the degeneration process of the adjacent level. 7 19
Facet Violation versus Pedicle Screw Technique
In one of the 1 st studies to compare the risk of facet violation between percutaneous and open techniques, Babu et al. 20 demonstrated that the use of percutaneous screws brought a greater risk of facet violation than the use of open techniques (8.5% versus 2%, p < 0.05; OR 8.55). These results were similar to those found by Jones-Quaidoo et al., 13 who reported a 13% rate of facet violation with the percutaneous technique against 6% with the use of the open technique. Taking a step forward, researchers performed a meta-analysis comparing the rate of facet violation between the use of robotic surgery versus the manual screw placement, demonstrating that the aid of the robot reduced the number of facet violations by pedicle screws. 21
Some researchers also sought to verify the risk of violation of the facet capsule among the different types of pedicle screw insertion. Matusakawa et al. 8 reported an 11% rate of facet violation using the cortical bone trajectory technique. Another study compared the rate of facet violation between the lateral-to-medial technique (LMT), and the owl's eye technique (OET), demonstrating that patients undergoing OET had more violated superior facets. 18
Anatomical Landmarks and Facet Violation
Despite the identification of techniques that can bring more risks of violation, another point is to identify structures and parameters that can serve as a reference for location, and, theoretically, for the reduction of facet violation. 6 17 22 Among the factors pointed out as having a relation to the facet violation, Jia et al. 23 showed that the lower the location, the higher the rate of facet violation, similar to the findings of Teles et al., 6 who reported 100% of facet violations at levels L4 and L5. These results are different from those indicated by our study, which identified the thoracic and L1 levels as more susceptible to facet violation.
It is also speculated in the literature whether the facet angle could influence the risk of facet violation. Two recent studies have assessed the relationship between facet angulation and facet violation, Teles et al. 6 demonstrated that the greater the facet angle, the greater the risk of violation (49° versus 34°; p < 0.001), as reported by Xu et al., 17 who described an average of 39° in cases in which there was violation, and 33° in cases without violation ( p < 0.001). These results are similar to those presented by our study, in which the group without violation had an average of 18° against 19° in the group that presented violation ( p < 0.05). However, we also compared the relationship of the facet angle to the screw angle (Δ angle), and we identified that the lower the proportion between the two, the greater the risk of violation of the facet capsule (g0 9.8° vs g1/2 3.7°; p < 0.0001). Furthermore, our study demonstrated that the difference in angle between the screw and the center of the facets (Δ angle) could more accurately indicate the risk of violation, or not, of the facet capsule, as demonstrated in Figure 5 , which compares the ROC curve obtained both by using the facet angle and using the measurement of Δ angle (AUC = 0.5848 versus AUC = 0.8599, p < 0.001).
The distance from the facets at which the pedicle screw was placed was also analyzed in our study, as we demonstrated that the greater the distance of the screw from the center of the facets, the lower the risk of facet violation (g0: 0.94 a.u. versus g1/2: 0.56 a.u.; p < 0.001). This result was similar to the one obtained in a study that analyzed the risk of facet violation after placing pedicle screws in a cortical bone path; however, in this study the distance from the screw to the upper facet was measured vertically. 8
The present study has several limitations, one of which is that it was a retrospective study. In addition, no distinction was made between the technique used or the method for inserting the pedicle screw. Points such as center of the facet, and center of the head of the Finally, we must mention the use of arbitrary units. Despite of how much they may assist in the standardization of measures, they are not validated units, and their generalization may be restricted.
In spite of these limitations, the present study can point out paths for the future because these reference values (Δ angle e Δ distance) can be added to the use of intraoperative images, new technologies, such as robotics, or surgical navigation, to increase safety when placing pedicle screws.
Conclusion
This work demonstrated that the use of measures that relate facets and pedicle screws (Δ angle e Δ distance) are effective to indicate, and perhaps in the future decrease, the risk of facet violation. However, further studies with different populations using the proposed measures are needed to verify its real applicability.
Footnotes
Conflitos de interesse Os autores declaram não haver conflitos de interesse.
Referências
- 1.Waldrop R, Cheng J, Devin C, McGirt M, Fehlings M, Berven S. The Burden of Spinal Disorders in the Elderly. Neurosurgery. 2015;77 04:S46–S50. doi: 10.1227/NEU.0000000000000950. [DOI] [PubMed] [Google Scholar]
- 2.Buser Z, Ortega B, D'Oro A. Spine Degenerative Conditions and Their Treatments: National Trends in the United States of America. Global Spine J. 2018;8(01):57–67. doi: 10.1177/2192568217696688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Narain A S, Hijji F Y, Markowitz J S, Kudaravalli K T, Yom K H, Singh K. Minimally invasive techniques for lumbar decompressions and fusions. Curr Rev Musculoskelet Med. 2017;10(04):559–566. doi: 10.1007/s12178-017-9446-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tamburrelli F C, Meluzio M C, Burrofato A, Perna A, Proietti L. Minimally invasive surgery procedure in isthmic spondylolisthesis. Eur Spine J. 2018;27 02:237–243. doi: 10.1007/s00586-018-5627-8. [DOI] [PubMed] [Google Scholar]
- 5.Mobbs R J, Phan K, Malham G, Seex K, Rao P J. Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015;1(01):2–18. doi: 10.3978/j.issn.2414-469X.2015.10.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Teles A R, Paci M, Gutman G. Anatomical and technical factors associated with superior facet joint violation in lumbar fusion. J Neurosurg Spine. 2018;28(02):173–180. doi: 10.3171/2017.6.SPINE17130. [DOI] [PubMed] [Google Scholar]
- 7.Kim H-J, Chun H J, Kang K T. The biomechanical effect of pedicle screws' insertion angle and position on the superior adjacent segment in 1 segment lumbar fusion. Spine (Phila Pa 1976) 2012;37(19):1637–1644. doi: 10.1097/BRS.0b013e31823f2115. [DOI] [PubMed] [Google Scholar]
- 8.Matsukawa K, Kato T, Yato Y. Incidence and Risk Factors of Adjacent Cranial Facet Joint Violation Following Pedicle Screw Insertion Using Cortical Bone Trajectory Technique. Spine (Phila Pa 1976) 2016;41(14):E851–E856. doi: 10.1097/BRS.0000000000001459. [DOI] [PubMed] [Google Scholar]
- 9.Magerl F P. Stabilization of the lower thoracic and lumbar spine with external skeletal fixation. Clin Orthop Relat Res. 1984;(189):125–141. [PubMed] [Google Scholar]
- 10.Roy-Camille R, Saillant G, Mazel C. Internal fixation of the lumbar spine with pedicle screw plating. Clin Orthop Relat Res. 1986;(203):7–17. [PubMed] [Google Scholar]
- 11.Weinstein J N, Spratt K F, Spengler D, Brick C, Reid S. Spinal pedicle fixation: reliability and validity of roentgenogram-based assessment and surgical factors on successful screw placement. Spine (Phila Pa 1976) 1988;13(09):1012–1018. doi: 10.1097/00007632-198809000-00008. [DOI] [PubMed] [Google Scholar]
- 12.Zhang D, Gao X, Jiang J, Shen Y, Ding W, Cui H. Safe placement of pedicle screw in lumbar spine with minimum three year follow-up: a case series and technical note. Int Orthop. 2018;42(03):567–573. doi: 10.1007/s00264-018-3806-1. [DOI] [PubMed] [Google Scholar]
- 13.Jones-Quaidoo S M, Djurasovic M, Owens R K, 2nd, Carreon L Y. Superior articulating facet violation: percutaneous versus open techniques. J Neurosurg Spine. 2013;18(06):593–597. doi: 10.3171/2013.3.SPINE12829. [DOI] [PubMed] [Google Scholar]
- 14.Knox J B, Dai J M, III, Orchowski J R. Superior segment facet joint violation and cortical violation after minimally invasive pedicle screw placement. Spine J. 2011;11(03):213–217. doi: 10.1016/j.spinee.2011.01.024. [DOI] [PubMed] [Google Scholar]
- 15.Archavlis E, Amr N, Kantelhardt S R, Giese A. Rates of Upper Facet Joint Violation in Minimally Invasive Percutaneous and Open Instrumentation: A Comparative Cohort Study of Different Insertion Techniques. J Neurol Surg A Cent Eur Neurosurg. 2018;79(01):1–8. doi: 10.1055/s-0037-1603631. [DOI] [PubMed] [Google Scholar]
- 16.Wang L, Wang Y, Yu B, Li Z, Li Y. Comparison of cranial facet joint violation rate between percutaneous and open pedicle screw placement: a systematic review and meta-analysis. Medicine (Baltimore) 2015;94(05):e504. doi: 10.1097/MD.0000000000000504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Xu Z, Tao Y, Li H, Chen G, Li F, Chen Q. Facet angle and its importance on joint violation in percutaneous pedicle screw fixation in lumbar vertebrae: A retrospective study. Medicine (Baltimore) 2018;97(22):e10943. doi: 10.1097/MD.0000000000010943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tannous O, Jazini E, Weir T B. Facet Joint Violation During Percutaneous Pedicle Screw Placement: A Comparison of Two Techniques. Spine (Phila Pa 1976) 2017;42(15):1189–1194. doi: 10.1097/BRS.0000000000002001. [DOI] [PubMed] [Google Scholar]
- 19.Wang H, Ma L, Yang D. Incidence and risk factors of adjacent segment disease following posterior decompression and instrumented fusion for degenerative lumbar disorders. Medicine (Baltimore) 2017;96(05):e6032. doi: 10.1097/MD.0000000000006032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Babu R, Park J G, Mehta A I. Comparison of superior-level facet joint violations during open and percutaneous pedicle screw placement. Neurosurgery. 2012;71(05):962–970. doi: 10.1227/NEU.0b013e31826a88c8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gao S, Lv Z, Fang H. Robot-assisted and conventional freehand pedicle screw placement: a systematic review and meta-analysis of randomized controlled trials. Eur Spine J. 2018;27(04):921–930. doi: 10.1007/s00586-017-5333-y. [DOI] [PubMed] [Google Scholar]
- 22.Celik S E, Celik S, Kara A, Ince I, Göksu K. Lumbar facet joint angle and its importance on joint violation in lumbar microdiscectomy. Neurosurgery. 2008;62(01):168–172. doi: 10.1227/01.NEU.0000311074.79357.1C. [DOI] [PubMed] [Google Scholar]
- 23.Jia L, Yu Y, Khan K. Superior Facet Joint Violations during Single Level Minimally Invasive Transforaminal Lumbar Interbody Fusion: A Preliminary Retrospective Clinical Study [Internet] Biomed Res Int. 2018;2018:6.152769E6. doi: 10.1155/2018/6152769. [DOI] [PMC free article] [PubMed] [Google Scholar]




