

Abstract
Aim:
The update World Health Organization guidelines recommend efavirenz (EFV) 400 mg as the preferred alternate first-line antiretroviral therapy (ART) to dolutegravir, with EFV 600 mg recommended only in special situations. We examined the pharmacokinetics (PK) of EFV 600 mg/day during pregnancy and postpartum to inform EFV dosing decisions in pregnant women.
Methods:
Ghanaian pregnant women with HIV infection initiating tenofovir disoproxil fumarate 300mg/lamivudine 300 mg/EFV 600 mg once daily were enrolled. Efavirenz concentrations were measured at 4 weeks of ART initiation during pregnancy and 6 weeks postpartum using validated LC/MS/MS assays. Efavirenz PK parameters were calculated using noncompartmental analysis and within group parameters between the two periods were compared.
Findings:
Of 25 enrolled women, 19 completed PK sampling during pregnancy and postpartum. The geometric mean EFV peak concentration (Cmax), trough concentration (Cmin), area under the curve (AUC0-24h) and apparent clearance (CL/F) during pregnancy were similar to values at 6 weeks postpartum. Geometric mean ratio pregnancy/postpartum (90% confidence interval) for EFV Cmax, Cmin, AUC0-24h and CL/F were 1.10 (0.93 – 1.31), 0.88 (0.67 – 1.17), 0.84 (0.71 – 0.98) and 1.20 (1.02 – 1.40), respectively. Viral load suppression (HIV RNA <200 c/mL) was achieved in 16 (94%) of 17 participants by the time of delivery. There was one maternal-to-child transmission.
Implications:
We found the PK of EFV 600 mg once daily during pregnancy to be similar to that in the postpartum period. Our findings suggest that EFV dose adjustment during pregnancy is not necessary in our study population.
Keywords: Standard-dose efavirenz, pharmacokinetics, pregnancy, postpartum, maternal-to-child transmission
INTRODUCTION
Effective antiretroviral therapy (ART) during pregnancy is essential for maternal health and prevention of maternal-to-child transmission (PMTCT) of human immunodeficiency virus (HIV). Current World Health Organization (WHO) HIV treatment guidelines recommend dolutegravir (DTG)-containing regimen as the preferred first-line ART for adults and adolescents living with HIV,1 with efavirenz (EFV) 400mg as alternate first-line ART regimen and the standard 600 mg EFV dose to be used only special circumstances.1 While the ENCORE1 double-blind, placebo-controlled trial showed that EFV 400 mg was virologically non-inferior to the standard dose EFV 600 mg over 96 weeks of follow-up,2 pregnant women were not included in the trial. Altered physiology changes during pregnancy such as increases in total body water and fat stores, reduction in plasma albumin and enhanced activities of drug metabolizing enzyme transporters may lead to reduction in drug concentrations and clinical effects.3,4 In addition, EFV is metabolized primarily by hepatic CYP2B6 enzyme,5 and genetic polymorphisms of CYP2B6 (with varying frequency in different populations) is associated with wide interindividual variability in EFV exposure and clearance.6
It is currently not clear whether EFV 400 mg or 600 mg should be preferred in pregnant women. While pharmacokinetic (PK) studies in the absence of clinical trial data may be helpful in clinical decision making, there are limited published PK studies in pregnant women from diverse populations. Among Thai women treated with EFV 600 mg once daily, an intensive PK study showed that median EFV area under the curve from time 0 to 24 hours (AUC0–24h) did not differ during third trimester of pregnancy and postpartum, but median EFV concentration at 24 hours post-dose (C24h) was lower during pregnancy.7 Among women enrolled in a PMTCT program in Nigeria treated with EFV 600 mg daily, EFV clearance was significantly increased and AUC0–24h and trough concentration (Cmin) were reduced in pregnant women compared to postpartum controls with CYPB26 extensive metabolizer genotype.8 In a study that enrolled 42 pregnant women from Europe, US, South America and Africa on EFV 600 mg/day, EFV AUC0-24h during second and third trimesters of pregnancy were similar to that during early postpartum.9 Although EFV C24h were lower during second and third trimesters of pregnancy compared to postpartum,9 the authors reported that EFV C24h in pregnancy in their study were similar to EFV C24h in non-pregnant adults treated with EFV 400 mg /day that was found to be effective in the ENCORE1 trial.10 In the only published PK study of EFV 400 mg during pregnancy that enrolled women who were virologically suppressed on EFV 600 mg once daily, the median EFV trough concentration (C24h) was 23% lower median during third trimester of pregnancy compared with the postpartum period but HIV viral load remained suppressed and no MTCT was observed.11 However, there is no evidence that EFV 400 mg once daily used as initial therapy in ART-naive pregnant women would have achieved similar viral suppression.
As EFV PK data in pregnant women is currently limited and dose reduction could pose a risk of ineffective ART for pregnant mothers and the developing child, additional evidence of adequacy of standard or reduced dose in different populations is essential. To date, no studies have evaluated EFV PK in Ghanaian pregnant or postpartum women. In addition, among 65 Ghanaian HIV-infected adults treated with EFV 600 mg/day, 30% had CYP2B6 extensive metabolizer genotype, with a higher risk of low EFV mid-dose concentrations and 19% were slow metabolizers.12 Thus, the primary objective of our study was to determine and compare EFV PK during pregnancy and postpartum in Ghanaian women living with HIV treated with EFV 600 mg once a daily. At the time of our study between 2014 and 2016, WHO guidelines recommended a simplified once daily FDC tablet of tenofovir disoproxil (TDF) 300mg/lamivudine (3TC) 300 mg /EFV 600 mg (TLE-600) for pregnant women for the PMTCT.13 At the time, EFV 600 mg/day was the preferred dose and EFV 400 mg/day was not yet introduced.13
Methods
Study design
A single-arm within-patient PK study was performed at Korle-Bu Teaching Hospital, Accra between 2014 and 2016. Pregnant women living with HIV, aged 18 years or older, ART-nai’ve without opportunistic infections and eligible to initiate EFV-based ART for PMTCT irrespective of CD4 count were enrolled. The institutional Review Boards (IRBs) of University of Ghana Medical School, Accra and that of Lifespan Hospitals, Providence, Rhode Island reviewed and approved the study. All study participants provided written informed consent.
At enrolment, a complete medical and obstetric history and physical examination and relevant data were collected using standardized forms. Baseline measurements prior to initiation of ART included complete blood count (CBC), blood urea nitrogen, serum creatinine, liver function tests (LFTs), as well as CD4 cell count determination and plasma HIV-1 RNA levels and abdominal ultrasonogram reports. All study participants were followed up to assess adverse events and clinical response to therapy. Self-report of missed doses in the last 7 days before follow-up visit was used to assess adherence; 3 or more missed dose was deemed as poor adherence.
Pharmacokinetic Sampling and analysis
Pharmacokinetic blood sampling was performed after at least 4 weeks of ART during pregnancy and at least 6 weeks postpartum. In addition, a random blood sample (when feasible) from mother and cord blood were collected at delivery. Given the CNS side effects of EFV, ART was administered at night but on the day of PK sampling, ART was administered in the morning after an overnight fast. Blood samples were collected at times 0, 1, 2, 3, 12 and 24 hours post-dose for determination of EFV concentrations. Blood samples collected in EDTA-coated tubes were centrifuged within 30 minutes at 3000 g for 10 minutes. Plasma was stored at −80°C until shipment on dry ice to University of Cape Town, Cape Town, South Africa for EFV concentrations assays. Efavirenz plasma concentrations were measured using validated liquid chromatography tandem with mass spectrometry (LC/MS/MS) methods.14 Lower limit of quantification (LLOQ) for the assay was 0.0844 μg/ml. The maximum or peak EFV concentration (Cmax), time to Cmax (Tmax) and Cmin were determined by inspection of the plasma concentration-time graphs. The calculations of AUC0–24h, estimated and apparent oral clearance (CL/F) were performed using noncompartmental analysis (Phoenix Software; Pharsight Corporation, Mountain View, CA).
Statistical analysis
Efavirenz PK parameters were summarized by geometric mean with 95% confidence interval (CI). Within-group change between pregnancy and 6 weeks postpartum periods was based on the Signed-rank test nominal PK parameters and the McNemar’s test for PK parameters less than a threshold. Bioequivalence between the two periods was assessed by 90% CI for geometric means and t-test applied to lognormal data. For all analyses, a P value < 0.05 was considered significant. Statistical analyses were performed using Software SAS 9.4 (SAS Institute Inc, Cary, NC).
RESULTS
Study population
A total of 25 pregnant women living with HIV were enrolled during the study period, of whom two withdrew from the study and two were lost to follow-up prior to any PK sampling. One of the participants who withdrew had sever psychosis on EFV-based ART. Of the remaining 21 participants, HIV diagnosis was made during the current pregnancy and all initiated ART for PMCT. Overall, 13 patients were enrolled in the first trimester, 12 in the second trimesters and 6 in the third trimester. Two participants were excluded from the PK analysis because they could not undergo PK sampling during pregnancy because of premature delivery in one patient and emergent caesarian section in the other. Among the 19 participants who completed paired PK sampling, the median (range) age was 28 (22 – 34) years, body weight was 76 (48 – 87) kg and gestational age was 18 (8 – 32) weeks. The median (range) baseline CD4 count was 594 (187 – 1239) cell/μL and HIV-1 RNA level ranged from ranged from 41 – 29,800 copies/mL (N=14). The median duration of ART to PK sampling was 28.5 (28 – 43) days and to delivery was 111 (3 – 181) days.
Efavirenz pharmacokinetics
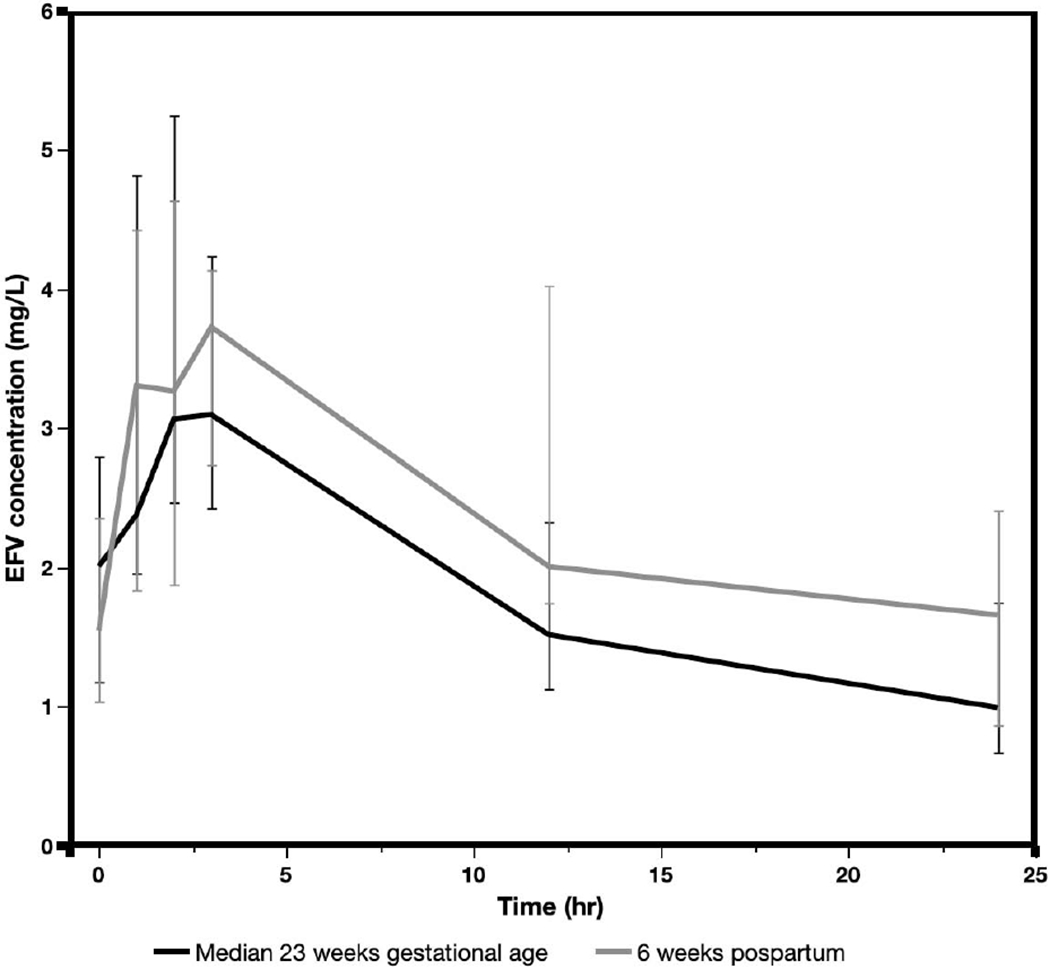
The median EFV plasma concentration at each sampled time point during pregnancy (median, 23 weeks GA, range, 12 – 37 weeks) were slightly lower than that at 6 weeks postpartum (Fig. 1). The GM and 95% confidence interval (CI) of EFV Cmax, C12h, Cmin, AUC0-24h and CL/F during pregnancy were similar to that at 6 weeks postpartum (Table 1). The pairwise analysis also showed that the median change in EFV PK parameters between the periods, during pregnancy and 6 weeks postpartum were not statistically different (Fig. 2). While we did not do CYP2B6 genotyping, two participants had EFV Cmin > 4 during both periods and were likely to be slow metabolizers but they tolerated EFV well.
Fig. 1.

Median efavirenz plasma concentrations during pregnancy (median 23 weeks gestation) and median 6 weeks postpartum plotted by sampling time after dosing among Ghanaian women.
Table 1.
Efavirenz pharmacokinetic parameter during pregnancy and postpartum and geometric mean ratio pregnant/postpartum among 19 women who completed paired sampling between 2014-2016, Accra, Ghana.
| Parameter | GM (95% CI) Pregnant |
GM (95% CI) Postpartum |
GMR P/PP (90% CI) | P value |
|---|---|---|---|---|
| Tmax (hr) | 2.11 (1.60 – 2.78) | 2.92 (1.90 – 4.48) | 0.75 (0.45 – 1.26) | 0.578 |
| Cmax (mg/L) | 4.33 (3.42 – 5.48) | 3.93 (3.08 – 5.02) | 1.10 (0.93 – 1.31) | 0.107 |
| C12h (mg/L) | 1.79 (1.24 – 2.59) | 2.47 ((1.81 – 3.37) | 0.73 (0.56 – 0.94) | 0.738 |
| Cmin (mg/L) | 1.12 (0.75 – 1.67) | 1.27 (0.84 – 1.92) | 0.88 (0.67 – 1.17) | 0.277 |
| CL/F (mL/hr) | 11.47 (8.56 – 15.36) | 9.59 (7.28 – 12.63) | 1.20 (1.02 – 1.40) | 0.317 |
| AUC0-24h (mg *hr/L) | 52.32 (39.07 – 70.06) | 62.56 (47.51 – 82.37) | 0.84 (0.71 – 0.98) | 0.317 |
IQR = interquartile range, GM = geometric mean, 95%CI = 95% confidence interval, GMR = geometric mean ratio pregnant/postpartum, P = pregnant, PP = postpartum, Tmax = time to Cmax, Cmax = peak concentration, C12h = concentration at 12 hours post-dose or mid-dose concentration, Cmin = minimum concentration, CL/F = apparent oral clearance, AUC0-24h = total area under the curve from time 0-24 hours.
Fig. 2.
Change in efavirenz CL/F (A), AUC0-24h (B), Cmin (C) and C12h during pregnancy and postpartum in 19 Ghanaian women with paired samples. Signed-rank test P value for median change in pharmacokinetic parameters between the two periods (dotted line) is reported.
At delivery, 15 pairs of maternal and cord blood samples were available as maternal or cord blood samples were not collected in some participants.. The median (range) maternal and cord blood EFV concentrations were 1.33 (0.19 – 2.76) mg/L and 1.02 (0.45 – 2.76) mg/L, respectively. The median (range) cord blood/maternal EFV concentration ratio was 0.85 (0.51 – 3.58), with 7 pairs having a ratio > 1.
Maternal and infant outcome
Of the 21 participants who delivered while in the study (this included 2 participants with PK sampling at only one period), 14 had normal vaginal delivery (with one stillbirth), 6 were delivered by caesarian section and one had a pre-term vaginal delivery. The median (range) gestational age at deliver was 37 (35 – 41) weeks. At delivery, 16 (94.1%) of 17 women with available data had HIV-1 RNA level < 200 copies/mL and only one woman had HIV-1 RNA level of 5080 copies/mL. The patient with high viral load at delivery presented late and was enrolled at 37 weeks gestation and started ART immediately but was delivered by caesarian section 3 days after initiation of ART; the infant HIV DNA test at birth was negative. At 6 weeks postpartum, all 18 participants with available data had HIV-1 RNA level < 200 copies/mL and 17 (94.4%) of the 18 participants had HIV-1 RNA < 50 copies/mL. Medication adherence by self-report was excellent in all patients.
Among newborns with available data (N=15), the median (IQR range) infant birth weight, length and head circumference were 3.0 (2.8 – 3.2) kg, 50 (48.0 – 51.0) cm and 34 (33.0 – 34.0) cm, respectively. At 6 weeks post-delivery follow up (N=18), the median (range) infant weight, length and head circumference were 4.5 (3.6 – 5.2) kg, 53.5 (51.0 – 58.0) cm and 37.0 (36.0 – 38.0) cm, respectively. Of the 20 live deliveries, one infant had detectable HIV-1 DNA in dried blood spot from the infant. The mother of this infant (PK16) was enrolled at 17 weeks of gestation with a baseline CD4 count of 555 cell/μL, viral load of 841 copies/mL. Efavirenz Cmin during pregnancy and postpartum were 0.67 mg/L and 0.432 mg/L, respectively and at delivery, she had undetectable plasma HIV-1 RNA < 50 copies/mL, a random plasma EFV concentration of 0.85 mg/L, cord blood EFV concentration of 0.51mg/L. Overall, no fetal malformations were observed in the 20 live births in our study and there was 1 still birth.
DISCUSSION
In this study in which pregnant women were treated with FDC TLE-600 once daily during pregnancy through early postpartum, pregnancy had no significant effect on EFV PK and mother-to-child HIV transmission was rare. Overall, GM values of EFV PK parameters during pregnancy were similar to that at 6 weeks postpartum among the women. We found only a 16% decrease in mean EFV AUC0-24h, 12% decrease in Cmin, 10% increase in Cmax and a 20% increase in CL/F during pregnancy compared with parameters at 6 weeks postpartum. The lack of significant effect of pregnancy on EFV plasma exposure or clearance in our study is consistent with what was reported in other published studies in women from different parts of the world.7, 9, 15 In contrast, other studies have reported increased EFV CL/F associated with increased risk of EFV Cmin < 1 μg/mL during pregnancy compared to postpartum period that occurred predominantly in women with CYP2B6 extensive metabolizer genotype.8,14 In one of these studies in which 72% of the pregnant women with CYP2B6 extensive genotype had EFV Cmin < 1 μg/mL, only one participant had MTCT.14 In our study, there was one in-utero MTCT in child with detectable HIV DNA on dried blood spot sample taken at birth. The mother of this child had EFV Cmin levels < 1 mg/L at all measured points but had undetectable viral load at the time of delivery and the postpartum visit. Overall, the current study showed that pregnancy had no significant effect on EFV PK when dosed at 600 mg once daily, suggestion that dose adjustment is not necessary during pregnancy in our population. The one episode of MTCT occurred despite viral suppression in the mother by the time of delivery.
The mean EFV AUC0-24h, Cmax and Cmin values in our study were are lower than the values reported by other studies that measured EFV concentrations during the third trimester.7,9 In our study, PK sampling was performed during the second trimesters in most of the participants, which might explain the lower values compared to those that sampled during the third trimester.7,9 In one of the studies in which EFV concentrations were measured during the second trimester9, the mean EFV AUC0–24h was comparable that observed in our study. In the participants with paired maternal and cord blood, we found a higher median cord blood to maternal EFV concentration ratio (range) of 0.85 (0.51 to 3.58) compared to the reported ratios (range) of 0.49 (0.37 – 0.74) in one prior study,7 and 0.67 (0.36 – 0.95) in another.9 The differences in ratios observed between the prior studies and ours may be due to differences in the time of sampling relative to dosing or difference in frequency of CYP2B6 516G>T genotypes. The high median ratio of 0.85 in our study confirms that EFV readily crosses the placenta and achieve high levels in infants at birth. The GM values of EFV AUC0-24h and Cmax of 52.3 mg*h/L and 4.3 mg/L, respectively in our study were higher than values of 39.9 mg*h/L and 2.8 mg/L, respectively in pregnant women treated with EFV 400 mg once daily,11 but the GM Cmin of 1.1 mg/L in our study was similar to the 1.2 mg/L observed by Lamorde M et al.11 Despite relatively low EFV Cmin during pregnancy and postpartum 16 (94%) of the 17 participants with viral load data had HIV-1 RNA < 200 copies/mL at delivery and all had suppressed viral load at the 6 weeks postpartum visit. In the one case of MTCT, the underlying reason was unclear as the mother reported excellent ART adherence but had low Cmin throughout the study but viral load was suppressed by the time of delivery. It is possible HIV transmission could have occurred earlier on during pregnancy prior to initiation of effective ART.
Our study has some limitations. The study enrolled participants at a time when EFV 600 mg was recommended for all adults as the preferred first-line therapy. Thus, our findings does not provide comparative PK data for the currently preferred EFV dose of 400 mg daily. We did not perform CYP2B6 genotyping and analysis by metabolizing status but we do not expect that CYP2B6 genotype dependent effect on EFV clearance and plasma exposure during pregnancy will differ from what is already reported by other studies.8,14
In conclusion, we found that pregnancy had no significant effect on EFV PK compared to that during early postpartum period. Our findings are consistent with prior reports that evaluated EFV 600 mg once daily dose.7,9,15 Thus, EFV dose adjustment during pregnancy is not necessary in our population as well. While current WHO guidelines recommend EFV 400 mg daily as the preferred alternate to DTG-based ART and EFV 600 mg once daily to be used only in special circumstances, the high prevalence of low EFV Cmin during pregnancy in our study suggest that the use of lower EFV dose in pregnant women should be approached with caution, especially given that routine viral load monitoring or TDM is lacking in our setting.
AKNOWLEDGEMENTS
We thank the patients for participation in this study. The study was funded by a CFAR International Developmental Grant from the CFAR (P30AI042853), with additional support from NICHD grant number HD071779 and NIAID-funded program (P30 AI078498). The Clinical PK Laboratory is supported in part via the Adult Clinical Trial Group (ACTG), by the National Institute of Allergy and Infectious Diseases (NIAID) of the National Institutes of Health under award numbers UM1 AI068634, UM1 AI068636, and UM1 AI106701; as well as the Infant Maternal Pediatric Adolescent AIDS Clinical Trials Group (IMPAACT), funding provided by National Institute of Allergy and Infectious Diseases (U01 AI068632).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
All authors report no conflicts of interest.
Declaration of interest: none.
References
- 1.WHO. Update of recommendations on first- and second-line antiretroviral regimens. July 2019. Geneva, Switzerland: World Health Organization; 2019 (WHO/CDS/HIV/19.15). Avialable at: https://apps.who.int/iris/bitstream/handle/10665/325892/WHO-CDS-HIV-19.15-eng.pdf. Accessed on January 13 2020. [Google Scholar]
- 2.Group ES, Carey D, Puls R, et al. Efficacy and safety of efavirenz 400 mg daily versus 600 mg daily: 96-week data from the randomised, double-blind, placebo-controlled, non-inferiority ENCORE1 study. Lancet Infect Dis. 2015;15:793–802. [DOI] [PubMed] [Google Scholar]
- 3.Thomas SH, Yates LM. Prescribing without evidence - pregnancy. British journal of clinical pharmacology. 2012;74:691–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Anderson GD. Pregnancy-induced changes in pharmacokinetics: a mechanistic-based approach. Clin Pharmacokinet. 2005;44:989–1008. [DOI] [PubMed] [Google Scholar]
- 5.Ward BA, Gorski JC, Jones DR, Hall SD, Flockhart DA, Desta Z. The cytochrome P450 2B6 (CYP2B6) is the main catalyst of efavirenz primary and secondary metabolism: implication for HIV/AIDS therapy and utility of efavirenz as a substrate marker of CYP2B6 catalytic activity. J Pharmacol Exp Ther. 2003;306:287–300. [DOI] [PubMed] [Google Scholar]
- 6.Holzinger ER, Grady B, Ritchie MD, et al. Genome-wide association study of plasma efavirenz pharmacokinetics in AIDS Clinical Trials Group protocols implicates several CYP2B6 variants. Pharmacogenet Genomics. 2012;22:858–867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cressey TR, Stek A, Capparelli E, et al. Efavirenz pharmacokinetics during the third trimester of pregnancy and postpartum. J Acquir Immune Defic Syndr. 2012;59:245–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Olagunju A, Bolaji O, Amara A, et al. Pharmacogenetics of pregnancy-induced changes in efavirenz pharmacokinetics. Clin Pharmacol Ther. 2015;97:298–306. [DOI] [PubMed] [Google Scholar]
- 9.Kreitchmann R, Schalkwijk S, Best B, et al. Efavirenz pharmacokinetics during pregnancy and infant washout. Antivir Ther. 2019;24:95–103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dickinson L, Amin J, Else L, et al. Pharmacokinetic and Pharmacodynamic Comparison of Once-Daily Efavirenz (400 mg vs. 600 mg) in Treatment-Naive HIV-Infected Patients: Results of the ENCORE1 Study. Clin Pharmacol Ther. 2015;98:406–416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lamorde M, Wang X, Neary M, et al. Pharmacokinetics, Pharmacodynamics, and Pharmacogenetics of Efavirenz 400 mg Once Daily During Pregnancy and Post-Partum. Clin Infect Dis. 2018;67:785–790. [DOI] [PubMed] [Google Scholar]
- 12.Kwara A, Lartey M, Sagoe KW, Rzek NL, Court MH. CYP2B6 (c.516G-->T) and CYP2A6 (*9B and/or *17) polymorphisms are independent predictors of efavirenz plasma concentrations in HIV-infected patients. Br J Clin Pharmacol. 2009;67:427–436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.WHO. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach June 2013. Available at: https://apps.who.int/iris/bitstream/handle/10665/85321/9789241505727_eng.pdf;jsessionid=85D502E19BA1DE5A6F3967F3D909E4B4?sequence=1. Last accessed on June 5, 2020 2013. [PubMed] [Google Scholar]
- 14.Dooley KE, Denti P, Martinson N, et al. Pharmacokinetics of efavirenz and treatment of HIV-1 among pregnant women with and without tuberculosis coinfection. J Infect Dis. 2015;211:197–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bartelink IH, Savic RM, Mwesigwa J, et al. Pharmacokinetics of lopinavir/ritonavir and efavirenz in food insecure HIV-infected pregnant and breastfeeding women in Tororo, Uganda. J Clin Pharmacol. 2014;54:121–132. [DOI] [PMC free article] [PubMed] [Google Scholar]