

Abstract
The characteristic features of Class III malocclusion are present at an early age, usually between 3 and 5 years of age. If left untreated, the Class III malocclusion or severe anterior crossbite may worsen, with the majority of these patients ultimately requiring orthognathic surgery as adults. The treatment in all developing Class III cases should be undertaken as soon as the abnormality is diagnosed to prevent it from becoming permanent and resulting in a full-blown Class III malocclusion. It provides more pleasing facial esthetics (the lip posture and facial appearance), thus improving the psychosocial development of a child. Various treatment options available for the management of developing Class III malocclusion are as follows: (1) functional appliances such as reverse twin block, Frankel appliance, and the removable mandibular retractor; (2) orthopedic appliances such as chin cap and face mask; and (3) orthodontic appliances, namely removable maxillary expansion plate or fixed orthodontic appliance with expanded upper arch wire. A treatment plan may be chosen depending on the amount of maxillary growth restriction, mandibular plane angle, the soft-tissue profile, and the age of the patient. This article discusses the various treatment options and the decision-making for different clinical cases based on the clinical features with a description of four different treatment approaches.
Keywords: Anterior expansion appliance, Class III malocclusion, facemask, reverse twin block, two by six appliances
Introduction
Due to increasing awareness regarding malocclusion and more concern about esthetic in the general population in present days, it is necessary for a dentist to have immense knowledge and skills about the diagnosis and treatment planning of the malocclusion to meet patient's expectations. Nowadays, the patient reports to a clinician at very early age for the correction of malocclusion. The prevalence rate of Class III malocclusion varies according to different racial categories. The mean incidence rate in Caucasians is 1%–4%,[1] with higher being found in Asians (4%–14%).[2] The etiology of Class III malocclusion is multifactorial. However, hereditary is the main etiological factor. Other factors include environment, habits, and race. Class III malocclusion is mainly due to skeletal component, dentoalveolar component, and combination of both. Prognathic mandible, retrognathic maxilla, or combinations of both are the features of skeletal Class III malocclusion. Dentoalveolar component presents with retruded mandibular incisors and protruded maxillary incisors for dentoalveolar compensation.[3]
Class III malocclusion is of two types: (1) True Class III malocclusion and (2) Pseudoclass III/functional Class III malocclusion. PseudoClass III malocclusion may be due to high points while occluding teeth or functional shift. The diagnosis and treatment planning can be done considering the following: (a) centric relation (CR), (b) family history, (c) interincisal relationship, and (d) cephalometric findings.[4] True Class III malocclusion mostly has a positive family history. Cephalometric findings may present with increased Sella–Nasion–B point (SNB) angle and small or decreased Sella–Nasion–A Point (SNA) angle, retroclination of lower incisors, and less incisor mandibular plane (MP) angle. Cephalometric findings of pseudo/functional Class III malocclusions show normal SNA, slight increase in SNB angle, retroclined maxillary incisors, and normal lower incisors. Family history is usually absent. The functional shift can be seen.[5]
Case Reports
Case report 1: Anterior expansion appliance
A 9-year-old boy reported with permanent maxillary incisors in reverse overjet relation with anterior deep bite of 4.1 mm. 11, 12, and 21 were lingually tipped, and 22 was labially protruded. Functional shift and positive family history were absent. Cephalometrically, child showed a skeletal Class III malocclusion which could be due to dentoalveolar maxillary deficiency. Sagittal expansion with posterior bite plane along with segmental fixed orthodontic treatment was planned. A maxillary appliance with a posterior bite plane was delivered, and segmental fixed orthodontics was done on four maxillary anteriors. Parents were instructed about the activation schedule of a quarter turn every 3rd day and to report after 3rd week to change wire for fixed treatment. After the correction of crossbite in 3 months, further activation of expansion appliance was stopped. Fixed orthodontic treatment was continued for space closure of anteriors, which was removed after correction. The patient was advised for regular follow-up. Cephalometric pre-values and postvalues are shown in Table 1 (Case 1), and pre-operative and postoperative results are shown in Figure 1.
Table 1.
Cephalometric Analysis
| Case 1 | Case 2 | Case 3 | Case 4 | |||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| SNA (°) | 79 | 82 | 78 | 82 | 82 | 82 | 78 | 82 |
| SNB (°) | 81 | 81 | 79.8 | 80.2 | 81 | 80 | 80 | 80 |
| ANB (°) | −2 | 1 | −1.8 | 1.8 | 1 | 2 | −2 | 2 |
| Wit’s appraisal (mm) | −8 | −2 | −3.9 | −1 | −6 | −2 | −5 | −1.2 |
| FMA (°) | 26 | 25.8 | 24 | 27.6 | 24.5 | 24.8 | 26.6 | 29 |
| IMPA (°) | 84 | 81 | 80 | 81.9 | 86 | 88 | 95.3 | 97.2 |
| Angle of convexity (mm) | −3 | 0 | −4 | −1 | −2 | 0 | −3 | −1 |
| Y axis (°) | 58.6 | 60.2 | 60 | 64 | 60 | 61 | 58.2 | 60 |
| SN length (mm) | 60.6 | 64 | 59 | 65 | 67 | 68 | 66.4 | 68.2 |
| Inter-incisal angle (°) | 126 | 127.2 | 128 | 126.8 | 129 | 130.6 | 130 | 131 |
Figure 1.

(a and b) Preoperative frontal and lateral extraoral profile. (c) Preoperative intraoral view. (d) Sagittal expansion appliance. (e and f) Postoperative frontal and lateral extraoral profile view. (g) Postoperative intraoral view
Case report 2: Face mask patient
An 8-year-old boy presented with a chief complaint of abnormal upper and lower anterior teeth. On extraoral examination, a concave profile was evident with mild eversion of the lower lip. Intraoral examination revealed a mixed dentition period, with permanent maxillary central incisors in reverse overjet relation revealing a reverse overbite of 3 mm. No premature incisal contacts were observed, and functional shift was absent. There was a familial history of Class III malocclusion. The cephalometric analysis revealed a deficient SNA angle and increase in SNB angle. A decision to correct the anterior interlock by bringing the maxilla forward with facemask therapy was made. An intraoral splint was fabricated on the cast. The splint was cemented, and the facemask was adjusted after 24 h of cementation. The patient was instructed to wear it for 14–16 h/day and change the elastics daily. Adequate maxillary protraction was achieved within 5½ months. Facemask was used for further 3 months for retention. Pre-operative and postoperative cephalometric values and images are shown in Table 1 (Case 2) and Figure 2, respectively.
Figure 2.
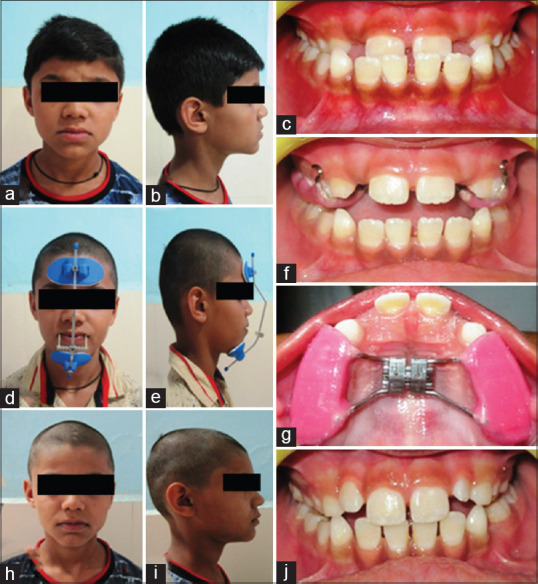
(a-c) Preoperative extraoral and intraoral photographs. (d and e) Extraoral view showing petite facemask. (f and g) Intraoral frontal and upper occlusal view showing intraoral cemented appliance. (h-j) Postoperative extraoral and intraoral pictures
Case report 3: Two-by-six fixed orthodontic appliance
A 9-year-old boy reported with abnormal upper and lower teeth. On intraoral examination, permanent incisors and deciduous canines were in 1-mm crossbite, and spaces were present between both set of incisors. The profile was straight. SNA and SNB were in the normal range; however, SNB was on a slightly higher side. 2 × 4 segmental orthodontics was undertaken in the lower arch to close the spaces present between incisors and deciduous canines. Deciduous canines were also bonded considering the space between lower lateral incisor and deciduous canine. Upper expansion with a posterior bite plane was given for the correction of crossbite in the canine region. After the closure of spaces between incisors in 3 months time, upper arch was also banded and bonded (2 × 4) along with deciduous canines for the closure of space between upper incisor and canines. The upper arch space closure occurred in 2 months. The pre-treatment and posttreatment results are shown in Table 1; case 3 and images are shown in Figure 3.
Figure 3.

(a-c) Preoperative extraoral and intraoral photographs. (d and e) Intraoral frontal views showing two-by-six fixed orthodontic appliance. (f-h) Postoperative extraoral and intraoral pictures
Case report 4: Reverse twin block
A child aged 6 years reported with inwardly placed upper front teeth. There was no family history of Class III malocclusion. The lower deciduous first molars were extracted by some private practitioner 5 months ago. On examination, anterior crossbite due to postural shift of the mandible in a Class III position was present. Lateral cephalometric revealed SNA in normal range and SNB slightly greater than normal values [Table 1 case 4]. A diagnosis of pseudoClass III malocclusion was made. Reverse twin-block appliance was fabricated and activation every 2–3 weeks by acrylic resin addition on inclines of blocks was done. The correction of anterior crossbite within 1 month of appliance wear and another 6 weeks was continued for retention. The pre-operative and postoperative results are shown in Figure 4.
Figure 4.

(a) Preoperative intraoral frontal view. (b) Reverse twin-block appliance. (c) Postoperative intraoral frontal view
Discussion
The purpose of early orthodontic treatment is to intercept the developing malocclusion and redirecting it to physiological development. Interception of Class III malocclusion can prevent irreversible soft- and hard-tissue changes, which includes labial plate thinning in anterior region, gingival recession, interincisal compensation, labial wearing of mandibular incisors, overclosure of mandible, simplification of comprehensive treatment, and eliminate the necessity of orthognathic surgery in some cases. Facemask or chin cup orthopedic therapies improve the skeletal component, decrease dentoalveolar compensation, improve occlusal harmony, and provide psychological benefits to the patient by achieving esthetics.[3]
For the correction of developing Class III malocclusion, appliances are categorized as follows: (a) functional appliances, for example, reverse twin block, Frankel appliance, and removable mandibular retractor (RMR); (b) orthopedic appliances, for example, facemask and chin cup; and (c) orthodontic appliances, for example, removable maxillary expansion plate. The choice of appliance depends on the age of the patient, soft-tissue profile, and growth of maxilla. For the correction of retrognathic maxilla and prognathic mandible, facemask and chin cup can be used, respectively.[5]
The types of primary anterior teeth crossbites include Type 1 – Pseudo/Functional Class III malocclusion and Type 2 – True Class III malocclusion. Type 1 Class III malocclusion includes occlusal prematurities leading to CR-centric occlusion (CO) deviation. Type 2 Class III malocclusion includes clinical features (retrognathic maxilla, prognathic mandible, and concave profile) with no CR-CO deviation with supporting cephalometrics. Family history is mostly positive. Type 1 is further classified into Type 1a and Type 1b. Type 1a is also known as simple malocclusion (presence of functional shift with normally inclined anterior teeth). Type 1b is also called complex malocclusion, presents with abnormal dentoalveolar relations that imitate true Class III malocclusion.[6]
The treatment modalities for Type 1a include simple disocclusion maxillary appliance such as posterior bite plane or reverse twin block. For Type 1b malocclusion, sagittal expansion appliance with posterior bite plane is the treatment of choice. Treatment option for Type 2 mainly depends upon the inter-incisal relationship. If edge-to-edge bite is present, RMR is the treatment of choice. In case of anterior deep bite, face mask can be used.[6]
The following two things are important for a case to be treated with functional appliance: (1) mild retrognathic maxilla and (2) absence of very steep MP angle. For treatment planning, esthetic and soft-tissue profile plays an important role, as poor case selection may cause inadvertent results. Patient's compliance and unpredictable mandibular growth are the challenging factors for the pediatric dentist. Facemask and expansion plates with posterior bite plane lead to steeper MP angle, which will cause increase in vertical facial height.[5,6]
Various appliances have been reported in the literature for the correction of developing Class III malocclusion.[4]
Detail of appliances
Facemask with or without expansion screw
Cases that show skeletal maxillary retrognathism with low MP angle are the cases opt for treatment with facemask. Family history is positive along with the absence of mandibular shift. The ideal age for facemask therapy is 6–8 years, and it can be started as soon as the patient can handle the appliance and have good compliance. Facemask can be used with skeletal anchorage such as titanium screw/osseointegrated implants, and facemask acts by promoting maxillary growth and restricting mandibular growth. Problems associated with facemask therapy are patient compliance, chances of relapse as a result of late mandibular growth. A case report by Bedolla et al.[7] related to the early treatment of skeletal Class III during primary dentition stage concluded that facemask plus a rapid maxillary expansion appliance with posterior bite blocks results in satisfactory and long term, functional, and esthetic changes and can decrease the need of future orthognathic surgery.
Anterior expansion appliance
In developing class III malocclusion in which maxillary and mandibular skeletal bases are normal but anterior shift of mandible results in dentoalveolar crossbite. In these cases sagittal anterior expansion appliance is used to correct anterior maxillary interlock. Observation for true Class III pattern till growth spurt at 18 years of age is needed. Machado et al.[8] in a case report summarized that efforts should be made toward an early correction of a developing Class III malocclusion, especially when associated with anterior crossbite.
Chin cap
Chin cap indicated primarily in deciduous and early mixed dentition phase with low MP angle cases. It causes a downward and backward rotation of mandible and controls mandibular growth at chin. Compliances needed. The results are unpredictable. The results depend on the account of force applied and the duration of daily wear. A cephalometric study performed by Graber showed that the use of a chin cup promoted a backward movement of Point B, due to a clockwise rotation of the mandible. The length of the mandible also decreased by about 1 mm due to the pressure transmitted by the chin cup to the condyle, which generated, on the other hand, a delay in vertical growth.[9] In another study, Sakamoto et al. evaluated the skeletal changes produced before, during, and after chin cup therapy. The authors concluded that chin cup therapy would be a very useful and efficient method for correcting Class III malocclusion with mandibular prognathism.[10] In addition, Sugawara described that an early treatment with a chin cup produced positive orthopedic effects on the mandible.[11] Singh et al. reported a case report of developing Class III malocclusion, treated with chin cup therapy followed by fixed orthodontic treatment and Class III elastics. The author concluded that chin cup therapy is beneficial if it is started at the right time.[12]
Reverse twin block and Frankel appliance
Clark has described reverse twin block version of twin block that may be used for Class III malocclusion. Inclined planes angulations are reversed, and it works on harnessing of occlusal forces to facilitate maxillary advancement. A three-way expansion screw is used for both sagittal and transverse expansion of the maxilla. Ideal cases with minimal maxillary skeletal deficiency and edge-to-edge inter-incisors relation are the cases of choice for reverse twin block. The maxillary advancement starts within 4–6 weeks, and average treatment time is generally 6 months to establish a positive overjet. The addition of acrylic to inclined planes is needed to increase to forces over the maxilla and mandible. Sargod et al. reported a case of Class III malocclusion in primary dentition and treated with reverse twin block concluded that reverse twin block can be used successfully for early treatment of Class III malocclusion in primary dentition.[13] Ulgen and Firatli studied the effect of Frankel functional regulator on 40 functional Class III malocclusion patients, with a mean age of 9.5 years and found a significant increase in A point, Nasion and B point (ANB) angle as a result of decrease in SNB angle due to downward and backward rotation of the mandible.[14]
Removable mandibular retractor
Maxillary resin plate with labial archwire extending to the labial surfaces of mandibular incisors acts by providing proprioceptive stimuli to restrict the forward movement of mandible. It can be used with expansion screw, with minimal overbite and steep MP angle. A randomized controlled trail done by Majanni and Hajeer with an objective to evaluate skeletal, dental, and soft tissue changes following early Class III treatment and compared between removable mandibular RMR group and bone anchored intermaxillary traction (BAIMT) group. Thirty-eight participants with a mean age of 11.46 were included. The author concluded that BAIMT is more effective than RMR in treating early Class III malocclusion.[15] Furthermore, Baccetti and Tollaro performed a retrospective study compared the effectiveness of RMR in correcting Class III malocclusion in primary (20 participants) and mixed dentition (18 participants) groups and concluded that skeletal and dentoalveolar changes are more evident in deciduous and mixed dentitions, respectively.[16]
Eschler appliance or progenic appliance
Eschler appliance has an Adam clasp for retention, a modified Eschler labial bow made of 0.9 mm wire, which will gently touch the labial surface of lower incisors and a 2–3 mm acrylic occlusal bite-raising appliance, which affords normal growth of the maxilla, finger springs for correction of upper incisors proclination, or expansion screw can be added. Almeida et al. in a case report of a 10-year clinical follow-up used combination of Eschler appliance with chin cup during interceptive phase in treating Class III malocclusion and concluded that correct diagnosis and early intervention are necessary to allow proper facial growth and development.[17]
Two-by-four and two-by-six appliance with posterior bite plane
Two-by-four and two-by-six fixed orthodontic appliance corrects the dental problems which may be the cause for the development of skeletal Class III malocclusion. By the correction of dental origin of problem, skeletal problem can be minimized or reduced if diagnosed at an early stage.
Conclusion
The basic goal of early treatment of Class III skeletal malocclusion is to enable the child to close the mouth in CR by improving anterior teeth relation thus permitting normal growth of maxilla and mandible and their normal relationship. The choice of the appliance should be based on the age of the patient, soft-tissue analysis, growth of maxilla, inter-incisal relationship, and cephalometric findings.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Newman GV. Prevalence of malocclusion in children six to fourteen years of age and treatment in preventable cases. J Am Dent Assoc. 1956;52:566–75. doi: 10.14219/jada.archive.1956.0092. [DOI] [PubMed] [Google Scholar]
- 2.Ishii H, Morita S, Takeuchi Y, Nakamura S. Treatment effect of combined maxillary protraction and chincap appliance in severe skeletal Class III cases. Am J Orthod Dentofacial Orthop. 1987;92:304–12. doi: 10.1016/0889-5406(87)90331-3. [DOI] [PubMed] [Google Scholar]
- 3.Singh K, Verma VK, Panda S, Sachan A. Management of skeletal Class III malocclusion in an early mixed dentition with face mask therapy: A case report. J Dent Res Updates. 2014;1:55–60. [Google Scholar]
- 4.Azamian Z, Shirban F. Treatment options for Class III malocclusion in growing patients with emphasis on maxillary protraction. Scientifica (Cairo) 2016;2016:1–9. doi: 10.1155/2016/8105163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kapur A, Chawla HS, Utreja A, Goyal A. Early Class III occlusal tendency in children and its selective management. J Indian Soc Pedod Prev Dent. 2008;26:107–13. doi: 10.4103/0970-4388.43191. [DOI] [PubMed] [Google Scholar]
- 6.Kapur A, Chawla HS, Utreja A, Goyal A. Guiding the child's teeth with Class III dental malocclusion into correct occlusion: A clinician's parenting. J Clin Pediatr Dent. 2018;42:72–8. doi: 10.17796/1053-4628-42.1.13. [DOI] [PubMed] [Google Scholar]
- 7.Bedolla H, Garrigós D, Hernández J, Rosales M, Pozos A, Garrocho J. Quick correction of a skeletal Class III maloclussion in primary dentition with face mask plus rapid maxillary expansion therapy. Int J Dent Sci. 2018;20:31–7. [Google Scholar]
- 8.Machado AW, Caldas SG, Maia LG. Early correction of a developing Class III malocclusion with a removable appliance. Dent Oral Craniofac Res. 2016;2:359–61. [Google Scholar]
- 9.Graber LW. Chin cup therapy for mandibular prognathism. Am J Orthod. 1977;72:23–41. doi: 10.1016/0002-9416(77)90122-1. [DOI] [PubMed] [Google Scholar]
- 10.Sakamoto T, Iwase I, Uka A, Nakamura S. A roentgenocephalometric study of skeletal changes during and after chin cup treatment. Am J Orthod. 1984;85:341–50. doi: 10.1016/0002-9416(84)90191-x. [DOI] [PubMed] [Google Scholar]
- 11.Sugawara J. Clinical practice guidelines for developing Class III malocclusion. In: Nanda R, editor. Biomechanics and Esthetic Strategies in Clinical Orthodontics. US: Saunders; 2005. pp. 211–63. [Google Scholar]
- 12.Singh SP, Kumar V, Verma R, Singh S. Management of developing skeletal Class III malocclusion in a prepubertal girl with prognathic mandible in late mixed dentition. Contemp Clin Dent. 2017;8:139–44. doi: 10.4103/ccd.ccd_1078_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sargod SS, Shetty N, Shabbir A. Early Class III management in deciduous dentition using reverse twin block. J Indian Soc Pedod Prev Dent. 2013;31:56–60. doi: 10.4103/0970-4388.112418. [DOI] [PubMed] [Google Scholar]
- 14.Ulgen M, Firatli S. The effects of the Fränkel's function regulator on the Class III malocclusion. Am J Orthod Dentofacial Orthop. 1994;105:561–7. doi: 10.1016/S0889-5406(94)70140-7. [DOI] [PubMed] [Google Scholar]
- 15.Majanni AM, Hajeer MY. The removable mandibular retractor vs. the bone-anchored intermaxillary traction in the correction of skeletal Class III malocclusion in children: A randomized controlled trial. J Contemp Dent Pract. 2016;17:361–71. doi: 10.5005/jp-journals-10024-1856. [DOI] [PubMed] [Google Scholar]
- 16.Baccetti T, Tollaro I. A retrospective comparison of functional appliance treatment of Class III malocclusions in the deciduous and mixed dentitions. Eur J Orthod. 1998;20:309–17. doi: 10.1093/ejo/20.3.309. [DOI] [PubMed] [Google Scholar]
- 17.Almeida MR, Almeida RR, Oltramari-Navarro PV, Conti AC, Navarro Rde L, Camacho JG. Early treatment of Class III malocclusion: 10-year clinical follow-up. J Appl Oral Sci. 2011;19:431–9. doi: 10.1590/S1678-77572011000400022. [DOI] [PMC free article] [PubMed] [Google Scholar]