

Abstract
The extraction of periodontally compromised teeth in the anterior esthetic region is a challenging situation due to patients' psychological and esthetic demands. Irrespective of the replacement of missing teeth with the final prosthesis, the first line of management would be to provisionally restore the teeth at the earliest. Routine treatment options for replacement are time-consuming and expensive. Using the patient's natural tooth as a pontic offers the benefits of the same size, shape, color, and preservation of the gingival architecture. Using the patient's platelet concentrate (platelet-rich fibrin) facilitates early wound healing and preservation of the alveolar ridge shape following tooth extraction. With minimal or no preparation, the technique can be completed at the chairside, thereby avoiding laboratory costs. This case report details the procedure with a follow-up of a case where the natural extracted tooth of the patient was used as pontic to replace a missing anterior tooth.
Keywords: Esthetics, gingival contour, natural tooth pontic, periodontitis, platelet-rich fibrin, resin-bonded bridges
Introduction
Advanced periodontal disease is one of the reasons for the removal of teeth in the anterior region. Restoration of these lost teeth in the anterior region is a prime concern due to esthetics and maintenance of gingival contour.[1] Cast partial dentures, removable partial dentures, fixed partial dentures, and implants may be planned as a permanent replacement after the tissues have healed. Limited options are available for an excellent esthetic temporary prosthesis. Removable partial dentures delay wound healing due to bulky nature if placed right away after tooth extraction.[2] Immediate implants can be chosen whenever there are good quality bone and no residual infection after extraction.[3]
Considering all the possibilities, natural tooth pontics (NTP) are the best alternatives to maintain soft-tissue contour during healing, and due to the perfect color match, size, and shape. NTP satisfy the esthetic and psychological demands of the patient.[4] With the emergence of various composite materials, NTP can be modified and bonded to the adjacent natural teeth using these composite materials solely or in combination with orthodontic wires.[5]
Case Report
A 39-year-old female patient with complaints of the loose tooth and swollen gums in the upper front tooth region associated with difficulty while mastication reported to the Department of Periodontics. On examination, Grade III mobility with a probing pocket depth of >10 mm and suppuration was observed in relation to the maxillary right central incisor [Figure 1a]. Orthopantomogram (OPG) revealed an extensive bone loss in relation to 11, suggesting a hopeless prognosis [Figure 1b]. Both clinical and radiographic examination indicated an extraction of 11. Scaling and root planing was done and the patient was recalled after 1 week for extraction of 11 as the patient was not willing for any endodontic treatment. Before the procedure, the position of the tooth in the arch and its relationship with the adjacent teeth was evaluated. Atraumatic extraction of the tooth was done under local anesthesia. The extraction socket was curetted and irrigated with antiseptic povidone-iodine to remove the granulation tissue [Figure 1c]. Care was taken to remove the granulation tissue completely and to create fresh bleeding in the socket. Five milliliter venous blood was collected from the antecubital fossa, platelet-rich fibrin (PRF) membrane was prepared using a centrifuge machine, and this membrane was placed in the extraction socket [Figure 1d].
Figure 1.
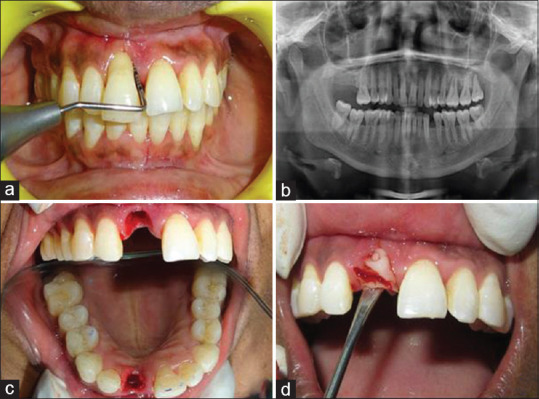
(a) Preoperative clinical view. (b) Preoperative radiographic view. (c) Atraumatic extraction of tooth done and the socket is curetted. (d) Platelet-rich fibrin membrane placed in the extraction socket
Preparation of the extracted tooth
The extracted tooth was cleansed using an ultrasonic scaler to remove any surface debris and adherent granulation tissue. The root portion of the tooth was reduced using airotor to the desired length [Figure 2a]. An access cavity was prepared, and all the pulpal remnants were removed and irrigated using a sodium hypochlorite solution. Then, the orifice was closed with composite resin. At the cervical region of the extracted tooth modified ridge lap pontic was designed to facilitate self-cleansing and appearance of an emergence profile.
Figure 2.
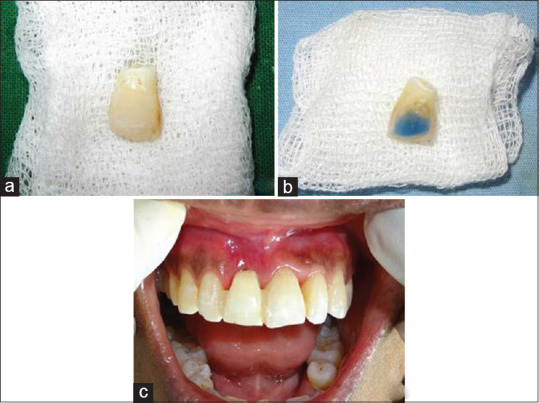
(a) Preparation of natural tooth pontic. (b) Etching of pontic with 37% phosphoric acid. (c) Splinting of natural tooth pontic to abutment tooth by composite resin
On the lingual side, at the level of cingulum, a groove was created with the bur to accommodate the orthodontic wire. The NTP and abutment teeth were etched with 37% phosphoric acid for 30 s and washed off [Figure 2b]. Then, the bonding agent was applied to the tooth and splinted the NTP to the adjacent teeth using light-cured composite resin [Figure 2c]. The following finishing and polishing the occlusal relationship was evaluated, and occlusal interferences were removed if any.
Oral hygiene instructions were reinforced to the patient and followed up for 1 year [Figure 3a and b].
Figure 3.
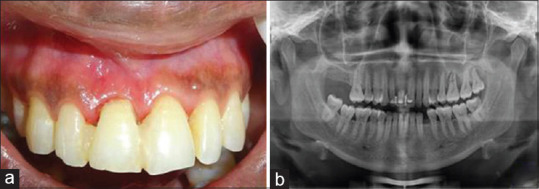
(a) Postoperative clinical view after 1 year. (b) Postoperative radiographic view after 1 year
Discussion
Tooth loss due to trauma, periodontal disease, and failed endodontic therapy in the esthetic zone creates a challenging situation to the dentist and requires immediate treatment due to the psychological and esthetic demands of the patient.[6] When the tooth is planned for extraction due to periodontal disease in the anterior region, the primary concern is esthetics. Due to increased esthetic demands from the patient, the dentist relies on esthetic principles while operating in esthetic areas considering patients' economic status.[7] Quirynen et al. conducted a study by comparing the acrylic tooth pontics and NTP placed after the loss of tooth due to periodontal disease and followed for 5 years. They concluded that NTP can be regarded as a semipermanent solution for the replacement of the lost natural tooth.[8] The major concern of placement of NTP is the psychological advantage of the patient and maintaining the soft-tissue profile for further permanent restoration.
In the present case, a NTP was planned as an immediate replacement for the missing anterior tooth because of patient esthetic demands and considering her socioeconomic status. Immediately after extraction, the NTP was splinted to the adjacent teeth for the preservation of gingival architecture. Composite resin and orthodontic wire were used to splint the pontic to the abutment teeth. The rationale for placing PRF membrane in the extracted socket is that platelet growth factors in PRF exhibit chemotactic and mitogenic properties, which promote cellular functions involved in tissue healing and cell proliferation. The patient reported again after 1 year with no complications. Bhandari et al. conducted a study in 15 patients, in which they have placed NTP soon after extraction of periodontally compromised teeth and concluded that NTP serve as the better option for immediate replacement, provides esthetic, and psychologic benefit to the patient.[9] Walsh et al. reported a case using NTP and concluded that NTP provides an excellent psychological benefit, with less treatment cost, maintenance of gingival profile, and no extensive surgical procedures.[10]
Conclusion
NTP serves as an excellent replacement immediately after extraction in the esthetic zone. Even though good oral hygiene maintenance and appropriate case selection are needed for this treatment option, NTP provides good psychological benefits following extraction and also provides time for permanent treatment options.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Vaghani KN, Nadig PS, Shah MA, Dave DH. Natural tooth pontic: An interim restoration for compromised aesthetic conditions. Adv Hum Biol. 2019;9:173–6. [Google Scholar]
- 2.Srinidhi G, Raghavendra SS. Natural tooth pontic with splinting of periodontally weakened teeth using fiber-reinforced composite resin. J Dent Allied Sci. 2014;3:43–6. [Google Scholar]
- 3.Tandon B, Suneja ES, Suneja B, Kaura S. Immediate temporization with natural tooth pontic. Saint Int Dent J. 2017;3:18–20. [Google Scholar]
- 4.Pant VA, Rathore M. Natural tooth pontic: An instant esthetic solution for hopeless tooth. Asian J Oral Heal Allied. 2011;1:147–51. [Google Scholar]
- 5.Ulusoy AT, Cehreli ZC. Provisional use of a natural tooth crown following failure of replantation: A case report. Dent Traumatol. 2008;24:96–9. doi: 10.1111/j.1600-9657.2006.00486.x. [DOI] [PubMed] [Google Scholar]
- 6.Raj R, Mehrotra K, Narayan I, Gowda TM, Mehta DS. Natural tooth pontic: An instant esthetic option for periodontally compromised teeth – A Case Series. Case Rep Dent. 2016;2016:1–6. doi: 10.1155/2016/8502927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Khetarpal A, Talwar S, Verma M. Creating a single-visit, fibre-reinforced, composite resin bridge by using a natural tooth pontic: A viable alternative to a PFM bridge. J Clin Diagn Res. 2013;7:772–5. doi: 10.7860/JCDR/2013/4698.2909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Quirynen M, Mongardini C, Lambrechts P, De Geyseleer C, Labella R, Vanherle G, et al. A long-term evaluation of composite-bonded natural/resin teeth as replacement of lower incisors with terminal periodontitis. J Periodontol. 1999;70:205–12. doi: 10.1902/jop.1999.70.2.205. [DOI] [PubMed] [Google Scholar]
- 9.Bhandari S, Chaturvedi R. Immediate natural tooth pontic: A viable yet temporary prosthetic solution: A patient reported outcome. Indian J Dent Res. 2012;23:59–63. doi: 10.4103/0970-9290.99040. [DOI] [PubMed] [Google Scholar]
- 10.Walsh LJ, Liew VP. The natural tooth pontic – A compromise treatment for periodontally involved anterior teeth. Aust Dent J. 1990;35:405–8. doi: 10.1111/j.1834-7819.1990.tb05419.x. [DOI] [PubMed] [Google Scholar]