

Abstract
Background:
Association between substance use and HIV-risk among gay and bisexual men (GBM) is well documented. However, their substance use patterns are diverse, and it is unknown whether self-reported use patterns are stable over time.
Methods:
Sexually-active GBM, aged >16 years, were recruited in Metro Vancouver using respondent-driven sampling and followed across 5 study visits at six-month intervals (n=449). To identify distinct patterns of substance use and their longitudinal stability, Latent Transition Analysis (LTA) was conducted for drugs reported by at least 30 participants. Intraclass correlation coefficients (ICC) quantified the stability of class assignments.
Results:
Six classes characterizing ‘limited drug use’ (i.e., low use of all drugs, except alcohol), ‘conventional drug use’ (i.e., use of alcohol, marijuana, and tobacco), ‘club drug use’ (i.e., use of alcohol, cocaine, and psychedelics), ‘sex drug use’ (i.e., use of alcohol, crystal meth, GHB, poppers, and erectile dysfunction drugs), ‘street drug use’ (i.e., use of alcohol and street opioids) and ‘assorted drug use’ (i.e., use of most drugs) were identified. Across five visits (2.5 years), 26.3% (n=118/449) of GBM transitioned between classes. The prevalence of limited use trended upwards (Baseline:24.5%, Visit 5:28.3%, p<0.0001) and assorted use trended downwards (13.4% to 9.6%, p=0.001). All classes had strong longitudinal stability (ICC>0.97).
Conclusion:
Stability of latent substance use patterns highlight the reliability of these measures in identifying patterns of substance use among people who use drugs – potentially allowing for better assessment of these groups and interventions related to their health.
Keywords: Latent Transition Analysis, Substance Use, Gay and Bisexual Men
1. Introduction
1.1. Background
Gay, bisexual, and other men who have sex with men (GBM) represent a priority population for public health intervention (Institute of Medicine, 2011) as they are known to be at elevated risk for a variety of deleterious health outcomes (Cochran and Mays, 2007; Coker et al., 2010). Among these, GBM is especially vulnerable to poorer mental and emotional health and have a greater risk for sexually transmitted infections (STIs), such as HIV (CDC, 2015; Plöderl and Tremblay, 2015). Concomitant with these priority health concerns, substance use has repeatedly been identified as a syndemic factor associated with adverse health – making it a priority concern for GBM communities (Halkitis et al., 2015; Lachowsky et al., 2017).
Recent examinations of GBM’s substance use have attempted to characterize heterogeneous patterns of use within their communities with the goal of targeting those patterns that are most strongly associated with adverse health outcomes, such as HIV transmission, problematic substance use, and poor mental health. In doing so, latent class analysis (LCA; Lazarsfeld and Henry, 1968) has emerged as an increasingly popular method to characterize GBM’s polysubstance use behavior (Lim et al., 2015a; McCarty-Caplan et al., 2014; Newcomb et al., 2014a; Tobin et al., 2015; Yu et al., 2015). These studies have shown that patterns of substance use are highly context and population dependent. Indeed, among various samples of GBM, three-class (Lim et al., 2015b; Newcomb et al., 2014b; Tobin et al., 2015), four-class (McCarty-Caplan, Jantz, and Swartz 2014), and six-class (Yu et al., 2015) latent models of substance use have been previously identified. These studies highlight not only a gradient in the number of substances used, but also distinct categories of substance use, such as sex drug use (McCarty-Caplan, Jantz, and Swartz 2014) and recreational drug use (Yu et al., 2015). However, while these studies can empower researchers to understand the complex substance use patterns of GBM, none have yet assessed the longitudinal stability of LCA classes among GBM.
Addressing this limitation, a closely related procedure called Latent Transition Analysis (LTA) has been developed to assess the stability of longitudinal class membership by examining whether individuals transition between classes over time (Collins and Lanza, 2013). While LTA is difficult to implement due to the relative scarcity of longitudinal data, previous studies have leveraged LTA to examine trends in GBM’s sexual behavior (Wilkinson et al., 2017), smoking habits (Gamarel et al., 2017), and sexual orientation (Fish and Pasley, 2015). Among other populations, LTA studies have found that while substance use classes are relatively stable, the transition does, in fact, occur even across relatively short study periods. For example, one study found that over the course of 18 months, 10% of German vocational students transitioned from “alcohol use” to “polysubstance use” (Tomczyk et al., 2016). Similarly, another study among women at risk for HIV reported that 10% of those initially classified as “smokers” transitioned to “crack, cocaine, and heroin use” after six-months (Lanza and Bray, 2010). Other epidemiological studies have likewise shown that among a subset of people who use drugs, individuals progress from relatively less harmful and more socially acceptable substances (e.g., alcohol, tobacco, and marijuana) to those which are less widely available and potentially more harmful (Cougle et al., 2016; Flórez-Salamanca et al., 2013; Kirby and Barry, 2012; Nkansah-Amankra and Minelli, 2016; Otten et al., 2017; Secades-Villa et al., 2015; Weinberger et al., 2016). Considering these findings, it is likely that some GBM also transitions between latent substance use classes over time.
1.2. Theoretical Framework
While substance use classes are believed to be largely stable due to personal and cultural attitudes and preferences towards substance use (e.g., drug of choice, social norms; Fast et al., 2009; Golub et al., 2005), two primary mechanisms have been proposed to explain transitions from less severe to more severe substance use. The first posits that commonly available drugs, such as alcohol, tobacco, and marijuana, act as neurobiological primers that predispose individuals to subsequent use of other drugs (Kandel, 2002; Kandel and Kandel, 2015; Kandel and Yamaguchi, 1993; Kirby and Barry, 2012; Secades-Villa et al., 2015; Weinberger et al., 2016). For example, Kandel and Kandel report that, in mice, nicotine exerts a non-reciprocal priming effect on cocaine-induced neurobiological addiction. Similar studies have shown priming effects of alcohol in both human and animal studies (Kirby and Barry, 2012). While by no means universal, these findings suggest that neurological primers can contribute to a gateway-like effect where exposure to less severe drugs (e.g., nicotine) predisposes one to increased risk for more severe drug use (e.g., cocaine). The second mechanism, known as the common liability hypothesis, disregards the temporal sequencing of using different substances and posits that shared risk-factors (referred to as liabilities) predispose individuals to substance use (Vanyukov et al., 2017). Proponents of this hypothesis argue that these common liabilities better explain the observed co-occurrence and temporal patterns of substance use behavior (Vanyukov et al., 2012; Vanyukov and Ridenour, 2012). These liabilities include genetic and biological propensities, as well as factors related to the social environment of individuals (e.g., access to healthcare, mental well-being, community connectedness, and social support). Of course, as is often the case with competing hypotheses, empirical investigations comparing these mechanisms show that both primer and liability effects likely contribute to substance use transition (Mayet et al., 2016).
Conversely, access to social and economic capital, access to care and social services, and better mental well-being might contribute to at least temporary transitions towards less severe substance use (Savic et al., 2017). Indeed, previous analyses of Momentum data have shown that GBM’s substance use is strongly associated with socioeconomic and mental health conditions (Card et al., 2017; Lachowsky et al., 2017). Therefore, increased access to health care and social services has the potential to reduce substance use by addressing these contributing factors. Further, several behavior change models highlight the role that communities and health care providers play in helping individuals recognize the potentially harmful effects of their substance use – thus providing motivations for these individuals to reduce their substance use (Chang et al., 2014; Prochaska and Velicer, 1997).
1.3. Objective
Recognizing (i) the limited research on substance use transitions among GBM, (ii) the strong theoretical and empirical support for shifting patterns of substance use, and (iii) the evidence that transition occurs between latent substance use classes in other populations, the present study examined the longitudinal stability of substance use classes among GBM to assess the utility of latent substance use analyses. We hypothesized that while the overall latent class structure would remain stable, a sizeable proportion of individuals would transition towards more frequent and severe substance use.
2. Methods
2.1. Study Protocol
Data for this study were collected as part of the Momentum Health Study, a longitudinal cohort of sexually active GBM, aged >16 years, in Metro Vancouver, British Columbia. Additional information about this cohort has been previously reported (Forrest et al., 2014, 2016; Lachowsky et al., 2016; Moore et al., 2016). In short, participants were recruited using respondent-driven sampling (RDS; Heckathorn, 1997). Eligible GBM presenting an RDS-voucher were screened for enrollment, provided informed consent, completed a 45-minute computer-administered questionnaire, and underwent STI screenings administered by a study nurse. Participants completed follow-up visits every six-months. At the completion of each visit, participants were provided a $50 honorarium and received an additional $10 for each eligible referee recruited into the study. Inclusion criteria for this analysis further restricted responses to those who were not lost to follow-up before the 5th study visit and who provided responses for outcome factors. Ethical approval was granted by the research ethics boards at the University of British Columbia, the University of Victoria, and Simon Fraser University.
2.2. Variables
2.2.1. Substance Use.
Participants reported their use (any vs. none) of alcohol, cannabis, tobacco, crystal meth, crack, cocaine, speed, heroin, poppers, erectile dysfunction drugs, gamma-Hydroxybutyric acid (GHB), ecstasy, ketamine, mushrooms, Lysergic acid diethylamide (LSD), benzodiazepines, codeine, oxycodone, and prescription steroids over the past six-months (P6M). For each substance, reported the frequency of use (more than weekly vs. weekly or less) was also assessed. Tobacco use (daily vs. less frequently) was assessed over the past six-months, and cannabis use (more than weekly vs. weekly or less) was also assessed over the past three months.
2.2.2. Descriptive Characteristics.
Descriptive characteristics were collected to assess the representativeness of sociodemographic and community connectedness variables in the study sample. Sociodemographic variables included age, race/ethnicity, sexual orientation, annual income, employment status, other income sources (i.e., welfare, disability, sex work, drug sales), current housing situation, level of educational attainment, relationship status, and HIV status. Community connectedness variables included attendance over the past six-months at gay bars or clubs, group sex events, and the most recent annual pride parade. Participants also reported whether they read gay newspapers, used gay apps and websites to find sexual partners, and how much of their social time they spent with other GBM.
2.3. Statistical Analysis
All statistical analyses were conducted in SAS (SAS, n.d.). Class membership, item response, and transition probabilities were calculated using the PROC LTA procedure (PROC LCA and PROC LTA, 2015). Indicator variables included all substances reported at any frequency by >30 participants. As few missing observations were observed (n = 115/2245), missing indicators due to a missing study visit were carried over from the previous visit to allow LCA models to include individuals who skipped only 1 study visit. This was necessary to ensure that our analysis was sufficiently powered to identify the correct number of latent classes. To assess whether this procedure impacted our results, we estimated the number of expected transitions based on the prevalence of observed transitions and number of missing events. Measurement invariance over time was confirmed by comparing class structure and item response probabilities at two separate visits. Final models were built using data from participant’s 1st (February 2012-February 2015) through 5th (March 2014 – February 2017) visits. The number of latent classes was identified based on model parsimony, class distinguishability, theoretical interpretability, and optimization of the Bayesian Information Criterion (BIC; (Dziak and Donna, 2012; Nylund et al., 2007). Supplemental Figure S11 provides the fit criterion used in selecting the number of classes. For each substance, intraclass correlation coefficients (ICC; Koo and Li, 2016) were also calculated to test the longitudinal stability of regular use (i.e., more than weekly use) with scores greater than 0.9 indicating excellent longitudinal stability. To assess statistical significance of trends, regression models were constructed with visit number as an explanatory factor.
3. Results
Among 774 GBM recruited, 698 enrolled in the longitudinal cohort. Of these, 519 completed second visits, 485 completed third visits, 452 completed fourth visits, and 451 completed fifth visits. In total, 449 participants provided all the data necessary to be included in the LTA (i.e., provided a response for each indicator variable). From these, 2130 observed visits were provided (with 115 visits missing, for which previous observations were carried forward). Supplemental Table S12 provides the distribution of missing visits by visit number and by latent class. At enrollment, the median age for this restricted sample was 35 years (Q1, Q3: 27, 48), 88.6% identified as gay (vs. 11.4% as bisexual/other), 76.8% were white, 40.8% had a current regular partner, 28.7% were HIV-positive, 84.4% had some post-secondary education, 66.6% were employed, 92.1% were stably housed, and 42.8% had incomes above $30,000 CAD. Other income sources included welfare (22.1%), disability (6.5%), sex work (4.2%), and drug sales (2.2%). Most participants read gay newspapers (84.2%), attended gay bars/clubs (80.2%), attended or participated in the most recent annual gay pride event (65.5%), and spent >50% of their social time with other GBM (53.5 %). Further, 55.2% sought partners on gay apps and 25.4% attended at least one group sex event in the past six-months.
The BIC value, which has been shown to be one of the best performing fit statistics for LCA models, was minimized at a six-class solution (Dziak and Donna, 2012; Nylund et al., 2007). Further, as the six-class model provided the best interpretability and distinguishability compared to other models, the six-class solution was selected. Table 1 shows the class-structure for each of the six substance use classes with the reported percentages representing the conditional response probability of individuals assigned to each class reporting use of each substance. Membership in Class 1 was characterized by the limited use of all substances, except alcohol (65.9% reported use in past six-months), compared to other classes. Membership in Class 2 was characterized by past six-month use of alcohol, tobacco, and marijuana. Membership in Class 3 was characterized by use of alcohol (100%), tobacco (63.6%), marijuana (85.3%), cocaine (63.5%), ecstasy (86.2%), mushrooms (34.3%), and LSD (15.7%). Membership in Class 4 was characterized by past six-month use of erectile drugs (88.0%), poppers (59.5%), ecstasy (23.5%), crystal methamphetamine (18.7%), and steroids (13.5%). Membership in Class 5 was characterized by high levels of tobacco use (76.8%) and by elevated use relative to other classes of crack (20.7%), crystal methamphetamine (29.4%), speed (3.5%), heroin (4.1%), codeine (10.9%), and oxycodone (10.8%). Membership in Class 6 was characterized by elevated overall and relative use of most drugs evaluated. Based on deductive interpretations of these classes, we described Class 1 as ‘limited drug use,’ Class 2 as ‘conventional drug use,’ Class 3 as ‘club drug use,’ Class 4 as ‘sex drug use,’ Class 5 as ‘street drug use,’ and Class 6 as ‘assorted drug use.’
Table 1.
Prevalence of Substance Use by LTA Class Among 449 Gay, Bisexual and MSM in the Momentum Health Study
| Baseline | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|
| Class Interpretability | - | Limited Drug Use | Conventional Drug Use | Club Drug Use | Sex Drug Use | Street Drug Use | Assorted Drug Use |
| N (%) | % | % | % | % | % | % | |
| Alcohol | 383 (85.3) | 65.9 | 99.0 | 100.0 | 83.2 | 64.4 | 93.1 |
| Marijuana A | 258 (57.5) | 11.2 | 66.1 | 85.3 | 66.1 | 59.8 | 80.7 |
| Tobacco B | 168 (37.4) | 4.7 | 39.1 | 63.6 | 2.3 | 76.8 | 61.6 |
| Erectile Drugs | 117 (26.1) | 10.3 | 0.8 | 13.5 | 88.0 | 23.8 | 70.3 |
| Poppers | 174 (38.8) | 8.9 | 22.3 | 39.9 | 59.5 | 28.9 | 75.3 |
| Crack | 31 (6.9) | 0.2 | 0.0 | 0.0 | 0.0 | 20.7 | 20.6 |
| Cocaine | 107 (23.8) | 0.0 | 9.1 | 63.5 | 2.4 | 20.5 | 60.4 |
| Crystal Methamphetamine | 78 (17.4) | 0.5 | 0.3 | 5.1 | 18.7 | 29.4 | 79.1 |
| Speed | 16 (3.6) | 0.1 | 0.0 | 7.2 | 0.0 | 3.5 | 11.3 |
| γ-Hydroxybutyric acid | 81 (18.0) | 0.0 | 0.6 | 15.0 | 14.4 | 6.2 | 87.2 |
| Benzodiazepine | 18 (4.0) | 0.4 | 0.0 | 5.2 | 3.0 | 9.1 | 16.0 |
| Ecstasy | 104 (23.2) | 0.3 | 5.8 | 86.2 | 23.5 | 1.1 | 66.1 |
| Ketamine | 56 (12.5) | 0.0 | 0.4 | 23.8 | 7.2 | 3.2 | 55.1 |
| Mushrooms | 43 (9.6) | 0.1 | 5.0 | 34.3 | 8.1 | 0.8 | 13.9 |
| Lysergic acid diethylamide | 16 (3.6) | 0.2 | 0.0 | 15.7 | 6.3 | 0.0 | 11.5 |
| Heroin | 8 (1.8) | 0.0 | 0.0 | 0.0 | 0.0 | 4.1 | 8.7 |
| Codeine | 25 (5.6) | 1.3 | 1.5 | 1.4 | 2.9 | 10.9 | 10.5 |
| Oxycodone | 17 (3.8) | 0.0 | 0.8 | 4.2 | 0.4 | 10.8 | 11.8 |
| Rx Steroids | 18 (4.0) | 0.3 | 5.7 | 0.0 | 13.5 | 4.3 | 5.1 |
BOLDED values indicate highest row prevalence; LTA=Latent transition analysis;
Past three months (All other drugs are reported over the past six months);
Daily vs. Less
Figure 1 shows the distribution of individuals across each of the six latent classes at each study visit. Overall, classes were relatively stable in the proportion of men assigned to each class. Following 449 men across all 5 visits revealed that 99.1% of GBM in Cass 1 (i.e., limited drug use) stayed in their originally assigned class, as did 93.4% of GBM in Class 2 (i.e., conventional drug use), 85.0% of GBM in Class 3 (i.e., club drug use), 93.4% of GBM in Class 4 (i.e., sex drug use), 84.3% of GBM in Class 5 (i.e., street drug use), and 82.1% of GBM in Class 6 (i.e., assorted drug use). In terms of trends, the prevalence of limited drug use increased over time from 24.5 to 28.3% (p < 0.0001), while assorted drug use declined (p = 0.001). Meanwhile, conventional drug use (p = 0.749), club drug use (p = 0.393), sex drug use (p = 0.550), and street drug use (p = 0.216) remained stable.
Figure 1.
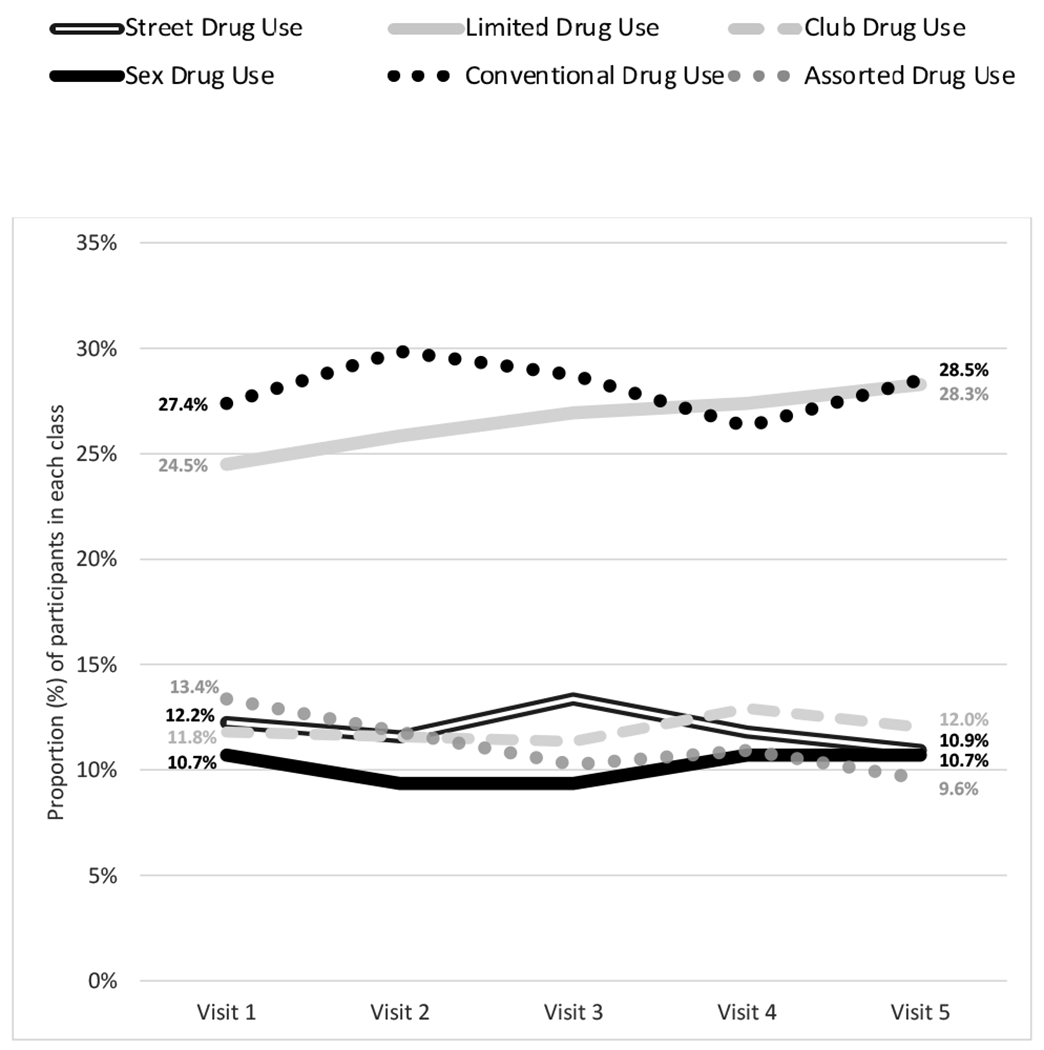
Distribution of Participants Across Study Visits, by LTA Class.
Table 2 shows the transition matrix aggregated across each of the 5 study visits. Summarizing these findings, 26.3% (n = 118) of GBM ever transitioned across classes, with most individuals transitioning either once (n = 96) or twice (n = 20). Notable transition pathways included reciprocal relationships between ‘conventional drug use’ (Class 2) and ‘club drug use’ (Class 3), ‘street drug use’ (Class 5) and ‘assorted drug use’ (Class 6); as well as unidirectional transitions from ‘street drug use’ (Class 5) to ‘limited drug use’ (Class 1), ‘assorted drug use’ (Class 6) to ‘conventional drug use’ (Class 1), ‘club drug use’ (Class 3) to ‘assorted drug use’ (Class 6), and ‘sex drug use’ (Class 4) to ‘conventional drug use’ (Class 2). No transition groups were large enough to power further analysis on predictors of class transition.
Table 2.
Transition Matrix Aggregating All Transitions Across All Observed Study Visits
| Participants | N = 449 | ||||||
|---|---|---|---|---|---|---|---|
| Observed Visits | N = 1,681 | ||||||
| Transitions | Transitions To… | ||||||
| 1 | 2 | 3 | 4 | 5 | 6 | ||
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | ||
| Transitions From… | 1 | 445 (99.1) | 1 (0.2) | 3 (0.7) | 0 (0) | 0 (0) | 0 (0) |
| 2 | 2 (0.4) | 441 (93.4) | 24 (5.1) | 5 (1.1) | 0 (0) | 0 (0) | |
| 3 | 6 (3) | 10 (5) | 170 (85) | 0 (0) | 5 (2.5) | 9 (4.5) | |
| 4 | 1 (0.6) | 8 (4.8) | 0 (0) | 155 (93.4) | 0 (0) | 2 (1.2) | |
| 5 | 11 (5.6) | 8 (4) | 1 (0.5) | 4 (2) | 167 (84.3) | 7 (3.5) | |
| 6 | 1 (0.5) | 9 (4.6) | 3 (1.5) | 2 (1) | 20 (10.2) | 161 (82.1) | |
1 = Limited Drug Use, 2 = Conventional Drug Use, 3 = Club Drug Use, 4 = Sex Drug Use, 5 = Street Drug Use, 6 = Assorted Drug Use; The cell values above are aggregated across all observed visits. Transitions occurred horizontally across the transition matrix, with each class on the left axis representing the class that a visit started in and each class on the top axis representing the class that a visit ended in.
Table 3 provides intraclass correlation coefficients for variables assessing the longitudinal stability of > weekly use of each substance along with the proportion of participants in each class who reported > weekly use of each substance at any of the five study visits. Generally, significantly fewer participants reported > weekly use of substances than reported any use of substances. Based on point estimates, > weekly use of erectile dysfunction drugs and GHB had “excellent” longitudinal stability (e.g., were internally consistent within individuals across time); tobacco, marijuana, prescription steroids, and benzodiazepines had “good” longitudinal stability; cocaine, alcohol, and crystal methamphetamine had “moderate” longitudinal stability; and codeine, poppers, crack, heroin, and oxycodone had “poor” longitudinal stability. Only a small number of participants reported > weekly use of speed, ecstasy, ketamine, mushrooms, or LSD. By class, limited drug use (ICC = 0.99, 95% CI: 0.99 – 1.00), conventional drug use (ICC = 0.98, 95% CI: 0.97 – 0.99), club drug use (ICC = 0.98, 95% CI: 0.95 – 0.98), sex drug use (ICC = 0.99, 95% CI: 0.97 – 0.99), street drug use (ICC = 0.97, 95% CI: 0.91 – 0.98), and assorted drug use (ICC = 0.97, 95% CI: 0.91 – 0.98) all had excellent longitudinal stability.
Table 3.
Intraclass correlation coefficients for the longitudinal stability of ≥ weekly use of each substance.
| Proportion of All Participants Who Used ≥ Weekly at Any Study Visit | Longitudinal Stability of ≥ Weekly Use | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall | Latent Class | ||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | ||||
| N (%) | % | % | % | % | % | % | ICC (95%CI) | Interpretation | |
| Alcohol | 652 (36.6) | 20.4 | 36.8 | 54.3 | 21.7 | 24.6 | 29.6 | 0.71 (0.66, 0.77) | Moderate – Good |
| Marijuana A | 445 (44.6) | 5.3 | 25.5 | 31.6 | 38.5 | 33.6 | 36.6 | 0.82 (0.75, 0.87) | Good |
| Tobacco B | 397 (51.8) | 1.7 | 16.5 | 19.8 | 0.9 | 56.8 | 39.3 | 0.87 (0.82, 0.97) | Good – Excellent |
| Erectile Drugs | 30 (5.8) | 1.2 | 0.0 | 0.0 | 7.0 | 0.8 | 2.5 | 0.95 (0.71,0.99) | Moderate - Excellent |
| Poppers | 61(9) | 0.6 | 1.0 | 3.1 | 11.1 | 1.2 | 6.7 | 0.59 (0.42, 0.72) | Poor – Moderate |
| Crack | 15 (14.4) | 0.0 | 0.0 | 0.0 | 0.0 | 3.6 | 2.2 | 0.57 (0.00, 0.91) | Poor – Excellent |
| Cocaine | 11 (2.6) | 0.0 | 0.2 | 0.0 | 0.0 | 1.1 | 3.0 | 0.72 (0.00, 0.97) | Poor – Excellent |
| Crystal Methamphetamine | 69 (21.4) | 0.2 | 0.0 | 0.8 | 3.3 | 6.3 | 17.8 | 0.70 (0.56, 0.79) | Moderate – Good |
| Speed | 2 (3.6) | 0.1 | 0.0 | 0.0 | 0.0 | 0.4 | 0.0 | - | Indeterminant |
| γ-Hydroxybutyric acid | 18 (6) | 0.0 | 0.0 | 0.0 | 0.5 | 0.0 | 7.0 | 0.92 (0.05, 0.99) | Poor – Excellent |
| Benzodiazepine | 11 (13.6) | 0.0 | 0.0 | 0.0 | 0.0 | 3.0 | 1.6 | 0.80 (0.00, 0.99) | Poor – Excellent |
| Ecstasy | 2 (0.4) | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.8 | - | Indeterminant |
| Ketamine | 1 (0.5) | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.4 | - | Indeterminant |
| Mushrooms | 0 (0) | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | - | Indeterminant |
| Lysergic acid diethylamide | 0 (0) | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | - | Indeterminant |
| Heroin | 9 (29) | 0.0 | 0.0 | 0.0 | 0.0 | 1.6 | 2.1 | 0.43 (0.00, 0.99) | Poor – Excellent |
| Codeine | 12 (15.6) | 0.2 | 0.0 | 0.0 | 0.5 | 4.2 | 0.0 | 0.63 (0.26, 0.99) | Poor – Excellent |
| Oxycodone | 7 (10.3) | 0.0 | 0.0 | 0.0 | 0.0 | 1.7 | 1.3 | 0.41 (0.00, 0.99) | Poor – Excellent |
| Rx Steroids | 22 (24.7) | 0.3 | 1.3 | 0.0 | 4.6 | 0.0 | 0.9 | 0.80 (0.43, 0.99) | Poor – Excellent |
ICC = intraclass correlation coefficient; Blanks indicate insufficient number of ≥ weekly users to calculate ICC; Bolded values indicated that more than 10% of the class engaged in ≥ weekly use for the given substance; GHB = gamma-hydroxybutyric acid; LSD = lysergic acid diethylamide; Stability Interpretation based on 95% Confidence Interval: < 0.5 (poor), 0.50 - 0.75 (moderate), 0.75 - 0.90 (good), ≥ 0.90 (excellent). 1 = Limited Drug Use, 2 = Conventional Drug Use, 3 = Club Drug Use, 4 = Sex Drug Use, 5 = Street Drug Use, 6 = Assorted Drug Use;
Past three months (All other drugs are reported over the past six months);
Daily vs. Less
4. Discussion
4.1. Primary Findings
The present study provides evidence supporting the longitudinal stability of latent substance use classes – a previously noted limitation of LCA studies among GBM (Lim et al., 2015a; McCarty-Caplan et al., 2014). While studies among other populations (e.g., heterosexual men and women) have previously shown that latent substance use classes are relatively stable (Lanza and Bray, 2010; Tomczyk et al., 2016), none, to our knowledge, have examined the stability of latent classes beyond a single follow-up visit (e.g., six to twelve months) or among GBM. However, our study supports these previous findings and suggests that latent classes in this population are relatively stable – at least over 2.5 years. This finding highlights the potential utility of using latent classes as explanatory factors in longitudinal studies, particularly for hierarchical models using repeated measures. However, while the latent classes themselves persisted at a population-level and most individuals within each class retained class membership, at the individual level approximately 25% of GBM underwent class transitions. This may be due to uncertainty in class assignment or actual changes in substance use behavior. As such, caution should be taken when interpreting cross-sectional relationships between person-level characteristics and latent class membership.
Regarding specific patterns of transition, our study shows that assorted drug use declined over time and limited drug use increased over time – potentially suggesting an overall decline in the severity of substance use patterns within this cohort. This finding is likely reflective of long-standing evidence suggesting that substance use varies with period (i.e., changes in substance use patterns in society), age (i.e., changes in substance use patterns across the life course), and cohort (i.e., changes in age cohorts) effects (O’Malley et al., 1984). Indeed, the increasing proportion of participants who reported limited drug use and attrition from the assorted drug use class is likely indicative of a curvilinear relationship between substance use patterns and the life course – with younger participants increasing their substance use and older participants limiting their use as they age (Hser et al., 2007, 2009). Furthermore, previous research has found that severity of substance use is a strong predictor of individuals obtaining substance use treatment (Evans-Polce et al., 2014). Therefore, assorted drug use class members may be more likely to access care, seek to intentionally scale back their use, or substitute less harmful drugs for more harmful ones (Grella and Lovinger, 2011). However, the lack of specific analyses examining the underlying factors predicting class transitions makes it difficult to speak directly to these phenomena. As such, larger scale quantitative studies and carefully targeted qualitative studies are needed to assess specific patterns of substance use transition.
With that said, several transitions observed in the present study merit attention. First, the largest transition pathway (n = 24) was among individuals transitioning from the conventional drug use class to the club drug use class – with a smaller number (n = 10) transitioning from club drug use to conventional drug use. While both classes were characterized by prevalent alcohol use, the club drug use class was characterized by the increased use of cocaine and a number of other party drugs (Lea et al., 2016; Noor et al., 2017). This provides some empirical support to biological studies demonstrating a gateway effect of alcohol on cocaine priming (Griffin et al., 2017; Kecojevic et al., 2017), as well as behavioral economic studies showing alcohol substitution for cocaine (Petry, 2001). Furthermore, the link between conventional drug use and club drug use is likely reflective of common liabilities as a previous cross-sectional analysis from our study has shown that membership in these classes is associated with patronage of gay bars and clubs (Card et al., 2017). Together, the transitions mentioned above underscore the influence of biological (e.g., related biological pathways) and socio-ecological factors (e.g., social environments) on both typology and transition patterns of substance use (Terry-McElrath et al., 2009).
Reinforcing the saliency of these factors, the next largest transition pathway (n = 20) was among those transitioning from the assorted drug use class to the street drug use class – with an additional 7 transitioning in the opposite direction. Transition from assorted drug use to a narrower subset of addictive substance (i.e., street drug use) may be reflective of the financial and market-related barriers to assorted drug use. Indeed, previous studies have discussed the profound implications of socioeconomic status and resource availability on peoples substance use patterns (Bourgois, 2003; Carpenter et al., 2017; Chalmers et al., 2010; Dwyer and Moore, 2010; Fast et al., 2009; Petry, 2001). Additionally, there is likely a naturally tendency for heroin users to maintain membership in these classes (where heroin use is the highest) – as heroin has previously been shown to be highly addictive, even compared to other drugs (Hser et al., 2008; Nutt et al., 2007). This is despite our observation that frequent heroin use (i.e., weekly or more) had poor reliability – which is supportive of the erratic nature of substance use. Indeed, previous studies have demonstrated that even addictive substances are characterized by transitions between periods of treatment, abstinence, non-daily, and daily use (Nosyk et al., 2014). These erratic usage patterns may also underlie the transition from the street drug use class to the limited (n = 11) and conventional drug use classes (n = 8). While these transitions may very well reflect intentional, health-motivated, or legally-mandated abstention from drug use (Klingemann, 1991; Klingemann et al., 2010), they may also reflect the natural volatility associated with specific substance use patterns. This suggests that latent class analysis may be relatively less reliable for some typologies of substance use than for others. Therefore, additional assessment of the individual and circumstantial factors that contribute to periods of sobriety among GBM are needed. Among several factors meriting future interest, these assessments should examine the impact of drug treatment and support group participation. Such studies may also provide learning opportunities for researchers and public health leaders hoping to instigate transitions from harmful use to abstinence or managed use.
4.2. Limitations
With consideration to the findings outlined above, readers should be aware of several important limitations. First, generalizability of these findings may be limited due to loss to follow up. However, the relationships we observed are likely still robust (i.e., internally valid). Second, to increase the flexibility of our analytic design we included participants who had missed 1 study visit, carrying forward responses from their previous visit into the missed visit. This may partially have underestimated the number of latent transitions observed (Lachin, 2016). Indeed, if transition probabilities were stable across all periods, we might expect that as many as 9 additional transitions would have been observed. However, given this small number, it seems unlikely that our conclusions would have changed. Yet, because the distribution of carried over observations was higher among those classified as engaging in conventional drug use, readers should be alert to the potential that transitions might have been higher than we report here. Third, due to the length of our follow-up periods (i.e., six-month intervals) and the use of period prevalence measures of substance use, it is possible that our study design does not provide sufficient nuance to understand how GBM transition between latent classes (Cooper, 2010). It is possible for instance that individuals transition ‘back-and-forth’ between classes multiple times within a single six-month period. Though given the infrequency of transitions, this seems unlikely. Fourth, use of any one substance in the past six-months is not necessarily indicative of frequency of use – even for addictive maintenance drugs. Fifth, readers should be aware that the naming and interpretation of latent classes is subjective. Given that the present analysis focuses on the stability rather than the composition of latent classes, readers should cautiously examine the conditional response probabilities presented in Table 1 in order to get a better sense of which groups they might represent. Similarly, readers should pay careful attention to the underlying latent variable being assessed by this analysis. Indeed, the indicators used in constructing our latent model represent not only a diverse sampling of psychoactive drugs (e.g., erectile dysfunction drugs, steroids, amphetamines, opioids) but also a broad spectrum of social ambiguities (e.g., legality, social acceptability). Given this, readers should be careful in comparing the results of the present study to those which have been conducted using a more restrictive or targeted selection of indicators.
5. Conclusion
In conclusion, the present study supports the longitudinal stability of latent substance use classes and highlights several notable transition pathways worth exploring in future research of GBM’s substance use. Overall, transitions do not represent a progression from less severe to more severe substance use as we initially hypothesized. Rather, transitions reflect the biological and socio-ecological propensities and vulnerabilities that underlie specific substance use patterns. Future qualitative studies are therefore needed to better describe the biological and social motivators that instigate transition between classes across the life course.
Supplementary Material
Highlights.
Heterogenous patterns of substance use among gay and bisexual men were observed.
Substance use latent classes were generally stable over 2.5 years of follow-up.
Over time, substance use trended towards limited use.
Acknowledgements
The authors would like to thank the Momentum Health Study participants, office staff and community advisory board, as well as our community partner agencies, Health Initiative for Men, YouthCO HIV & Hep C Society, and Positive Living Society of BC.
Role of Funding Source
Momentum is funded through the National Institute on Drug Abuse (R01DA031055-01A1) and the Canadian Institutes for Health Research (MOP-107544, 143342, PJT-153139). NJL was supported by a CANFAR/CTN Postdoctoral Fellowship Award. DMM and NJL are supported by Scholar Awards from the Michael Smith Foundation for Health Research (#5209, #16863). HLA is supported by a Postdoctoral Fellowship Award from the Canadian Institutes of Health Research (Grant # MFE-152443). KGC is supported by a University Without Walls-Engage Fellowship.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Supplementary material can be found by accessing the online version of this paper at http://dx.doi.org and by entering doi: https://doi.org/10.1016/j.drugalcdep.2018.04.019.
Supplementary material can be found by accessing the online version of this paper at http://dx.doi.org and by entering doi: https://doi.org/10.1016/j.drugalcdep.2018.04.019.
Conflict of Interest
No conflicts declared
References
- Bourgois P, 2003. In search of respect: Selling crack in el barrio. Cambridge University Press. [Google Scholar]
- Card KG, Armstrong H, Cui Z, Zhu J, Lachowsky NJ, Moore DM, Rother EA, 2017. A Latent Class Analysis of Substance Use and Culture among Gay, Bisexual, and Other Men Who Have Sex with Men. Cult. Health Sex. 28, 1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carpenter CS, McClellan CB, Rees DI, 2017. Economic conditions, illicit drug use, and substance use disorders in the United States. J. Health Econ 52, 63–73. 10.1016/j.jhealeco.2016.12.009 [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention, 2015. CDC fact sheet: HIV Among Gay and Bisexual Men.
- Chalmers J, Bradford D, Jones C, 2010. The effect of methamphetamine and heroin price on polydrug use: A behavioural economics analysis in Sydney, Australia. Int. J. Drug Policy 21, 381–389. 10.1016/j.drugpo.2010.06.002 [DOI] [PubMed] [Google Scholar]
- Chang SJ, Choi S, Kim S-A, Song M, 2014. Intervention strategies based on information-motivation-behavioral skills model for health behavior change: A systematic review. Asian Nurs. Res 8, 172–181. 10.1016/j.anr.2014.08.002 [DOI] [Google Scholar]
- Cochran SD, Mays VM, 2007. Physical health complaints among lesbians, gay men, and bisexual and homosexually experienced heterosexual individuals: Results from the California Quality of Life Survey. Am. J. Public Health 97, 2048–2055. 10.2105/AJPH.2006.087254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coker TR, Austin SB, Schuster MA, 2010. The health and health care of lesbian, gay, and bisexual adolescents. Annu. Rev. Public Health 31, 457–477. 10.1146/annurev.publhealth.012809.103636 [DOI] [PubMed] [Google Scholar]
- Collins LM, Lanza ST, 2013. Latent class and latent transition analysis: With applications in the social, behavioral, and health sciences. John Wiley and Sons. [Google Scholar]
- Cooper ML, 2010. Toward a person x situation model of sexual risk-taking behaviors: Illuminating the conditional effects of traits across sexual situations and relationship contexts. J. Pers. Soc. Psychol 98, 319–341. 10.1037/a0017785 [DOI] [PubMed] [Google Scholar]
- Cougle JR, Hakes JK, Macatee RJ, Zvolensky MJ, Chavarria J, 2016. Probability and correlates of dependence among regular users of alcohol, nicotine, cannabis, and cocaine: Concurrent and prospective analyses of the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 77, e444–450. 10.4088/JCP.14m09469 [DOI] [PubMed] [Google Scholar]
- Dwyer R, Moore D, 2010. Beyond neoclassical economics: Social process, agency and the maintenance of order in an Australian illicit drug marketplace. Int. J. Drug Policy 21, 390–398. 10.1016/j.drugpo.2010.03.001 [DOI] [PubMed] [Google Scholar]
- Dziak J, Donna L, 2012. Sensitivity and specificity of information criteria (Technical Report No. #12-119), Technical Report Series The Methodology Center, The Pennsylvania State University, Pennsylvania. [Google Scholar]
- Evans-Polce RJ, Doherty EE, Ensminger ME, 2014. Taking a life course approach to studying substance use treatment among a community cohort of African American substance users. Drug Alcohol Depend. 142, 216–223. 10.1016/j.drugalcdep.2014.06.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fast D, Small W, Wood E, Kerr T, 2009. Coming “down here”: Young people’s reflections on becoming entrenched in a local drug scene. Soc. Sci. Med. 1982 69, 1204–1210. 10.1016/j.socscimed.2009.07.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fish JN, Pasley K, 2015. Sexual (minority) trajectories, mental health, and alcohol use: A longitudinal study of youth as they transition to adulthood. J. Youth Adolesc 44, 1508–1527. 10.1007/s10964-015-0280-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flórez-Salamanca L, Secades-Villa R, Hasin DS, Cottier L, Wang S, Grant BF, Blanco C, 2013. Probability and predictors of transition from abuse to dependence on alcohol, cannabis, and cocaine: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Am. J. Drug Alcohol Abuse 39, 168–179. 10.3109/00952990.2013.772618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forrest JI, Lachowsky NJ, Lal A, Cui Z, Sereda P, Raymond HF, Ogilvie G, Roth EA, Moore D, Hogg RS, 2016. Factors associated with productive recruiting in a respondent-driven sample of men who have sex with men in Vancouver, Canada. J. Urban Health 93, 379–387. 10.1007/s11524-016-0032-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forrest JI, Stevenson B, Rich A, Michelow W, Pai J, Jollimore J, Raymond HF, Moore D, Hogg RS, Roth EA, 2014. Community mapping and respondent-driven sampling of gay and bisexual men’s communities in Vancouver, Canada. Cult. Health Sex. 10.1080/13691058.2014.881551 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gamarel KE, Neilands TB, Conroy AA, Dilworth SE, Lisha N, Taylor JM, Darbes LA, Johnson MO, 2017. A longitudinal study of persistent smoking among HIV-positive gay and bisexual men in primary relationships. Addict. Behav. 66, 118–124. 10.1016/j.addbeh.2016.11.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Golub A, Johnson BD, Dunlap E, 2005. Subcultural evolution and illicit drug use. Addict. Res. Theory 13, 217–229. 10.1080/16066350500053497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grella CE, Lovinger K, 2011. 30-year trajectories of heroin and other drug use among men and women sampled from methadone treatment in California. Drug Alcohol Depend. 118, 251–258. 10.1016/j.drugalcdep.2011.04.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin EA, Melas PA, Zhou R, Li Y, Mercado P, Kempadoo KA, Stephenson S, Colnaghi L, Taylor K, Hu M-C, Kandel ER, Kandel DB, 2017. Prior alcohol use enhances vulnerability to compulsive cocaine self-administration by promoting degradation of HDAC4 and HDAC5. Sci. Adv 3, e1701682 10.1126/sciadv.1701682 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halkitis PN, Kapadia F, Bub KL, Barton S, Moreira AD, Stults CB, 2015. A longitudinal investigation of syndemic conditions among young gay, bisexual, and other msm: The P18 Cohort Study. AIDS Behav. 19, 970–980. 10.1007/s10461-014-0892-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heckathorn D, 1997. Respondent-driven sampling: A new approach to the study of hidden populations. Soc. Probl 44, 174–199. [Google Scholar]
- Hser YI, Evans E, Huang D, Brecht ML, Li L, 2008. Comparing the dynamic course of heroin, cocaine, and methamphetamine use over 10 years. Addict. Behav 33, 1581–1589. 10.1016/j.addbeh.2008.07.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hser YI, Hamilton A, Niv N, 2009. Understanding drug use over the life course: Past, present, and future. J. Drug Issues 31, 231–236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hser YI, Longshore D, Anglin MD, 2007. The life course perspective on drug use: a conceptual framework for understanding drug use trajectories. Eval. Rev 31, 515–547. 10.1177/0193841X07307316 [DOI] [PubMed] [Google Scholar]
- Institute of Medicine (US) Committee on Lesbian, Gay, Bisexual, and Transgender Health Issues and Research Gaps and Opportunities, 2011. The health of lesbian, gay, bisexual, and transgender people: Building a foundation for better understanding, the national academies collection: Reports funded by National Institutes of Health. National Academies Press (US), Washington (DC). [PubMed] [Google Scholar]
- Kandel D (Ed.), 2002. Stages and pathways of drug involvement: Examining the gateway hypothesis, 1 edition Cambridge University Press, Cambridge, UK; New York. [Google Scholar]
- Kandel D, Kandel E, 2015. The gateway hypothesis of substance abuse: Developmental, biological and societal perspectives. Acta Paediatr. Oslo Nor 1992 104, 130–137. 10.1111/apa.12851 [DOI] [PubMed] [Google Scholar]
- Kandel D, Yamaguchi K, 1993. From beer to crack: Developmental patterns of drug involvement. Am. J. Public Health 83, 851–855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kecojevic A, Jun H-J, Reisner SL, Corliss HL, 2017. Concurrent polysubstance use in a longitudinal study of US youth: Associations with sexual orientation. Addiction 112, 614–624. 10.1111/add.13681 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirby T, Barry AE, 2012. Alcohol as a gateway drug: A study of U.S. 12th Graders. J. Sch. Health 82, 371–379. 10.1111/j.1746-1561.2012.00712.x [DOI] [PubMed] [Google Scholar]
- Klingemann H, 1991. The motivation for change from alcohol and heroin use. Br. J. Addict 86, 727–44. 10.1111/j.1360-0443.1991.tb03099.x [DOI] [PubMed] [Google Scholar]
- Klingemann H, Sobell MB, Sobell LC, 2010. Continuities and changes in self-change research. Addict. Abingdon Engl 105, 1510–1518. 10.1111/j.1360-0443.2009.02770.x [DOI] [PubMed] [Google Scholar]
- Koo ΤΚ, Li ΜΥ, 2016. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med 15, 155–163. 10.1016/j.jcm.2016.02.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lachin JM, 2016. Fallacies of last observation carried forward analyses. Clin. Trials Lond Engl 13, 161–168. 10.1177/1740774515602688 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lachowsky NJ, Dulai JJS, Cui Z, Sereda P, Rich A, Patterson TL, Corneil TT, Montaner JSG, Roth EA, Hogg RS, Moore DM, 2017. Lifetime doctor-diagnosed mental health conditions and current substance use among gay and bisexual men living in Vancouver, Canada. Subst. Use Misuse 52, 785–797. 10.1080/10826084.2016.1264965 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lachowsky NJ, Lal A, Forrest JI, Card KG, Cui Z, Sereda P, Rich A, Raymond HF, Roth EA, Moore DM, Hogg RS, 2016. Including online-recruited seeds: A respondent-driven sample of men who have sex with men. J. Med. Internet Res 18, e51 10.2196/jmir.5258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanza ST, Bray BC, 2010. Transitions in drug use among high-risk women: An application of latent class and latent transition analysis. Adv. Appl. Stat. Sci 3, 203–235. [PMC free article] [PubMed] [Google Scholar]
- Lazarsfeld PF, Henry NW, 1968. Latent structure analysis. Houghton, Mifflin. [Google Scholar]
- Lea T, Mao L, Hopwood M, Prestage G, Zablotska I, de Wit J, Holt M, 2016. Methamphetamine use among gay and bisexual men in Australia: Trends in recent and regular use from the Gay Community Periodic Surveys. Int. J. Drug Policy 29, 66–72. 10.1016/j.drugpo.2016.01.003 [DOI] [PubMed] [Google Scholar]
- Lim SH, Cheung DH, Guadamuz TE, Wei C, Koe S, Altice FL, 2015a. Latent class analysis of substance use among men who have sex with men in Malaysia: Findings from the Asian Internet MSM Sex Survey. Drug Alcohol Depend. 151, 31–37. 10.1016/j.drugalcdep.2015.02.040 [DOI] [PubMed] [Google Scholar]
- Lim SH, Cheung DH, Guadamuz TE, Wei C, Koe S, Altice FL, 2015b. Latent class analysis of substance use among men who have sex with men in Malaysia: Findings from the Asian Internet MSM Sex Survey. Drug Alcohol Depend. 151, 31–37. 10.1016/j.drugalcdep.2015.02.040 [DOI] [PubMed] [Google Scholar]
- Mayet A, Legleye S, Beck F, Falissard B, Chau N, 2016. The gateway hypothesis, common liability to addictions or the route of administration model? A modelling process linking the three theories. Eur. Addict. Res. 22, 107–117. 10.1159/000439564 [DOI] [PubMed] [Google Scholar]
- McCarty-Caplan D, Jantz I, Swartz J, 2014. MSM and drug use: A latent class analysis of drug use and related sexual risk behaviors. AIDS Behav. 18, 1339–1351. 10.1007/s10461-013-0622-x [DOI] [PubMed] [Google Scholar]
- Moore DM, Cui Z, Lachowsky NJ, Raymond HF, Roth E, Rich A, Sereda P, Howard T, McFarland W, Lal A, Montaner J, Corneil T, Hogg RS, 2016. HIV community viral load and factors associated with elevated viremia among a community-based sample of men who have sex with men in Vancouver, Canada. J. Acquir. Immune Defic. Syndr 72, 87–95. 10.1097/QAI.0000000000000934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newcomb ME, Ryan DT, Greene GJ, Garofalo R, Mustanski B, 2014a. Prevalence and patterns of smoking, alcohol use, and illicit drug use in young men who have sex with men. Drug Alcohol Depend. 141, 65–71. 10.1016/j.drugalcdep.2014.05.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newcomb ME, Ryan DT, Greene GJ, Garofalo R, Mustanski B, 2014b. Prevalence and patterns of smoking, alcohol use, and illicit drug use in young men who have sex with men. Drug Alcohol Depend. 141, 65–71. 10.1016/j.drugalcdep.2014.05.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nkansah-Amankra S, Minelli M, 2016. “Gateway hypothesis” and early drug use: Additional findings from tracking a population-based sample of adolescents to adulthood. Prev. Med. Rep 4, 134–141. 10.1016/j.pmedr.2016.05.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Noor SW, Adam BD, Brennan DJ, Moskowitz DA, Gardner S, Hart TA, 2017. Scenes as micro-cultures: Examining heterogeneity of HIV risk behavior among gay, bisexual, and other men who have sex with men in Toronto, Canada. Arch. Sex. Behav 47, 309–321. 10.1007/s10508-017-0948-y [DOI] [PubMed] [Google Scholar]
- Nosyk B, Li L, Evans E, Huang D, Min J, Kerr T, Brecht M, Hser Y, 2014. Characterizing longitudinal health state transitions among heroin, cocaine, and methamphetamine users. Drug Alcohol Depend. 140, 69–77. 10.1016/j.drugalcdep.2014.03.029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nutt D, King LA, Saulsbury W, Blakemore C, 2007. Development of a rational scale to assess the harm of drugs of potential misuse. The Lancet 369, 1047–1053. 10.1016/S0140-6736(07)60464-4 [DOI] [PubMed] [Google Scholar]
- Nylund KL, Asparouhov T, Muthén BO, 2007. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Model. Multidiscip. J 14, 535–569. 10.1080/10705510701575396 [DOI] [Google Scholar]
- O’Malley PM, Bachman JG, Johnston LD, 1984. Period, age, and cohort effects on substance use among American youth, 1976-82. Am. J. Public Health 74, 682–688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Otten R, Mun CJ, Dishion TJ, 2017. The social exigencies of the gateway progression to the use of illicit drugs from adolescence into adulthood. Addict. Behav 73, 144–150. 10.1016/j.addbeh.2017.05.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petry NM, 2001. A behavioral economic analysis of polydrug abuse in alcoholics: Asymmetrical substitution of alcohol and cocaine. Drug Alcohol Depend. 62, 31–39. [DOI] [PubMed] [Google Scholar]
- Plöderl M, Tremblay P, 2015. Mental health of sexual minorities. A systematic review. Int. Rev. Psychiatry Abingdon Engl 1–19. 10.3109/09540261.2015.1083949 [DOI] [PubMed] [Google Scholar]
- Lanza ST, Dziak JJ, Huang L, Wagner AT., Collins LM, 2015. PROC LCA and PROC LTA user’s guide (Version 1.3.2). University Park: The Methodology Center, Penn State; Available from https://methodology.psu.edu/sites/default/files/software/proclcalta/proc_lca_lta_1-3-2-1_users_guide.pdf [Google Scholar]
- Prochaska JO, Velicer WF, 1997. The transtheoretical model of health behavior change. Am. J. Health Promot. AJHP 12, 38–48. [DOI] [PubMed] [Google Scholar]
- SAS, n.d. SAS Institute Inc., Cary, NC, USA. [Google Scholar]
- Savic M, Best D, Manning V, Lubman DI, 2017. Strategies to facilitate integrated care for people with alcohol and other drug problems: a systematic review. Subst. Abuse Treat. Prev. Policy 12, 19 10.1186/s13011-017-0104-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Secades-Villa R, Garcia-Rodríguez O, Jin CJ, Wang S, Blanco C, 2015. Probability and predictors of the cannabis gateway effect: a national study. Int. J. Drug Policy 26, 135–142. 10.1016/j.drugpo.2014.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terry-McElrath YM, O’Malley PM, Johnston LD, 2009. Reasons for Drug Use among American Youth by Consumption Level, Gender, and Race/Ethnicity: 1976–2005. J. Drug Issues 39, 677–714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tobin KE, Yang C, King K, Latkin CA, Curriero FC, 2015. Associations Between Drug and Alcohol Use Patterns and Sexual Risk in a Sample of African American Men Who Have Sex with Men. AIDS Behav. 10.1007/s10461-015-1214-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomczyk S, Pedersen A, Hanewinkel R, Isensee B, Morgenstern M, 2016. Polysubstance use patterns and trajectories in vocational students--a latent transition analysis. Addict. Behav 58, 136–141. 10.1016/j.addbeh.2016.02.027 [DOI] [PubMed] [Google Scholar]
- Vanyukov M, Cornelius M, Genna ND, Reynolds M, Kirillova G, Maher B, Kirisci L, 2017. Measurement of Liability to Addiction: Dimensional Approaches. Int. J. Pers. Centered Med 6 10.5750/ijpcm.v6i4.612 [DOI] [Google Scholar]
- Vanyukov M, Ridenour TA, 2012. Common liability to drug addictions: Theory, research, practice. Drug Alcohol Depend. 123, S1–S2. 10.1016/j.drugalcdep.2012.01.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vanyukov M, Tarter RE, Kirillova GP, Kirisci L, Reynolds MD, Kreek MJ, Conway KP, Maher BS, Iacono WG, Bierut L, Neale MC, Clark DB, Ridenour TA, 2012. Common liability to addiction and “gateway hypothesis”: Theoretical, empirical and evolutionary perspective. Drug Alcohol Depend. 123, S3–S17. 10.1016/j.drugalcdep.2011.12.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weinberger AH, Platt J, Goodwin RD, 2016. Is cannabis use associated with an increased risk of onset and persistence of alcohol use disorders? A three-year prospective study among adults in the United States. Drug Alcohol Depend. 161, 363–367. 10.1016/j.drugalcdep.2016.01.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilkinson AL, El-Hayek C, Fairley CK, Roth N, Tee BK, McBryde E, Hellard M, Stoové M, 2017. Measuring Transitions in Sexual Risk Among Men Who Have Sex With Men: The Novel Use of Latent Class and Latent Transition Analysis in HIV Sentinel Surveillance. Am. J. Epidemiol 185, 627–635. 10.1093/aje/kww239 [DOI] [PubMed] [Google Scholar]
- Yu G, Wall MM, Chiasson MA, Hirshfield S, 2015. Complex drug use patterns and associated HIV transmission risk behaviors in an Internet sample of U.S. men who have sex with men. Arch. Sex. Behav 44, 421–428. 10.1007/s10508-014-0337-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.