

Abstract
Background and study aims Lumen-apposing metal stents (LAMS) are increasingly used for drainage of walled-off pancreatic necrosis (WON). Recent studies suggested greater adverse event (AE) rates with LAMS for WON. We conducted a systematic review and meta-analysis to compare the safety and efficacy of LAMS with double-pigtail plastic stents (DPPS) for endoscopic drainage of WON. The primary aim was to evaluate stent-related AEs.
Methods In October 2019, we searched the Ovid (Embase, MEDLINE, Cochrane) and Scopus databases for studies assessing a specific LAMS or DPPS for WON drainage conducted under EUS guidance. Safety outcomes were AE rates of bleeding, stent migration, perforation, and stent occlusion. Efficacy outcomes were WON resolution and number of procedures needed to achieve resolution. A subanalysis including non-EUS-guided cases was performed.
Results Thirty studies including one randomized controlled trial (total 1,524 patients) were analyzed. LAMS were associated with similar bleeding (2.5 % vs. 4.6 %, P = 0.39) and perforation risk (0.5 % vs. 1.1 %, P = 0.35) compared to DPPS. WON resolution (87.4 % vs. 87.5 %, P = 0.99), number of procedures to achieve resolution (2.09 vs. 1.88, P = 0.72), stent migration (5.9 % vs. 6.8 %, P = 0.79), and stent occlusion (3.8 % vs. 5.2 %, P = 0.78) were similar for both groups. Inclusion of non-EUS-guided cases led to significantly higher DPPS bleeding and perforation rates.
Conclusions LAMS and DPPS were associated with similar rates of AEs and WON resolution when limiting analysis to EUS-guided cases. Higher bleeding rates were seen in historical studies of DPPS without EUS guidance. Additional high-quality studies of WON treatment using consistent outcome definitions are needed.
Introduction
Acute pancreatitis is the third most common gastrointestinal discharge diagnosis from hospitals in the United States, with aggregate annual costs of $ 2.6 billion 1 and with increasing incidence 2 . Necrotizing pancreatitis develops in 5 % to 10 % of patients with acute pancreatitis 3 , and is associated with notable morbidity and hospital stays averaging 22 days 4 5 . Necrotizing pancreatitis is also associated with high mortality rates, varying from 11 % in patients with sterile necrosis 6 , to 32 % in patients with infected necrosis, and 43 % in patients with infected necrosis plus organ failure 7 .
Pancreatic fluid collections may occur as a result of acute pancreatitis, and many spontaneously resolve 8 . However, a subset of patients with necrotizing pancreatitis may develop symptomatic well-defined necrotic collections, classified as walled-off necrosis (WON) 3 . Endoscopic management of WON has typically been performed with double pigtail plastic stents (DPPS). Lumen-apposing metal stents (LAMS) have been increasingly used to treat symptomatic WON because they may allow better drainage of solid necrosis and also permit through-the-LAMS direct endoscopic necrosectomy due to their larger diameter compared to plastic stents.
Recently, various studies assessing LAMS have published disparate safety findings, with overall adverse event (AE) rates ranging from 0 % to 50 % 9 10 11 12 . Specific adverse events (AEs) such as bleeding also have widely varying reported rates, ranging from 0 % to 25 %, with some studies (including those with small sample size) suggesting a higher rate of bleeding with LAMS compared to DPPS 9 13 14 15 16 . In addition, the relatively large variations in reported complication rates may be partially attributable to their different definitions 17 . Given the recent concern for increased AEs with LAMS, further evaluation of LAMS is necessary. Examination of the uniformity of outcome definitions is also warranted to better interpret study results.
In the present systematic review and meta-analysis, we aimed to assess safety and efficacy of a specific LAMS compared to DPPS for the endoscopic drainage of WON under endoscopic ultrasound (EUS) guidance. Consistency of outcome definitions reported across studies was also examined.
Methods
Search strategy
We examined the references from a previous 2018 systematic review of metal stents (including LAMS) compared to plastic stents for WON management 18 , which applied similar eligibility criteria and was co-authored by two authors (FB, BA) of the current analysis. An expert librarian conducted searches of the Ovid Evidence-Based Medicine Reviews (Embase, MEDLINE, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews) and Scopus databases to identify studies published in English between database inception for the 2018 review and extended to October 9, 2019 ( Supplementary Table 1 ). Controlled trials, retrospective and prospective cohort studies, case-control studies, and case series that assessed LAMS or DPPS for WON drainage were included. We excluded publications that did not use the 2012 Atlanta criteria for WON diagnosis, lacked information to allow evaluation of the Atlanta criteria 3 , used surgical or percutaneous drainage in addition to endoscopic drainage, represented interim analyses of ongoing studies, reported on ≤ 5 patients, or had study populations that were not mutually exclusive. With regard to LAMS, only publications that investigated the AXIOS TM stent (Boston Scientific, Marlborough, Massachusetts, United States) were included as this is the only globally available LAMS and is the LAMS most commonly described in the literature 16 . The primary analysis was limited to cases conducted under EUS guidance. For reference, a subanalysis included all eligible studies, regardless of use of EUS guidance. For one study 19 , use of EUS in 100 % of LAMS cases was confirmed by direct communication with an author (B Abu Dayyeh, personal communication).
Data extraction and assessment for risk of bias
For all manuscripts identified by the literature search, three authors (OG, EM and MG) independently reviewed studies for eligibility and/or extracted data from selected publications for pre-identified safety and efficacy endpoints. Discrepancies were resolved by consensus. Baseline information consisted of study characteristics (design, sample size, year published, stent type), patient characteristics (age, sex), and WON characteristics (size and infection status). Reasons for study exclusion were documented.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to conduct this analysis 20 . The Newcastle-Ottawa Scale (NOS) was employed to review the methodologic quality of non-randomized studies and assess for bias. An adapted NOS ( Supplementary Table 2 ) was used that assessed the selection and representativeness of the study population, and the ascertainment of outcomes and exposures. Items from the NOS that made comparative assessments (e. g. exposed vs. non-exposed cohorts) were removed, as they did not apply to single-arm studies. This adaptation of the NOS has been used previously 21 22 23 , and for the purposes of this study, one question (“Were other important diagnoses excluded?”) was replaced (“Was follow-up long enough for outcomes to occur? Reported adequate follow-up time”) to make it more appropriate for this systematic review. Yes/no responses were required for each of five questions, and the quality of each study was ranked as good (5 yes responses), moderate (4 yes responses), or poor (≤ 3 yes responses).
Endpoint assessment and definition
LAMS were compared with DPPS for all outcomes for the drainage of WON based on the revised Atlanta classification for acute pancreatitis 3 . WON that were not assessed with the revised Atlanta classification but included a description of a pancreatic fluid collection containing solid necrosis with a defined wall were permitted. Any indication of surgical intervention or percutaneous drainage after endoscopic treatment was considered a failure of endoscopic WON resolution.
Safety outcomes assessed were rates of bleeding, perforation, stent migration, and stent occlusion. Efficacy outcomes assessed were rates of WON resolution and number of procedures needed to achieve WON resolution. Definitions of AEs were collected across studies to evaluate consistency reporting these outcomes. After the index procedure, any additional intervention performed to aid the removal of necrotic material was counted as a procedure, including irrigations, lavages, necrosectomies/debridements, additional stent placements, or other interventions.
Statistical methods
Safety and efficacy outcomes were assessed using a random-effects meta-analysis to estimate the proportion of patients with the measure or mean of the measure. Due to the small number of comparative studies, both arms from comparative studies were treated as independent studies and combined with non-comparative studies. The arcsine transformation was used to compute weighted pooled random-effects estimates for all endpoints; thus, an adjustment for proportions of 0 % and 100 % was not needed. Heterogeneity was assessed across studies using the I 2 statistic 24 . Funnel plots were created to assess for bias across studies. The Begg and Mazumdar rank correlation test of funnel plot asymmetry and Egger’s linear regression test of funnel plot asymmetry were also used to assess publication bias 25 26 . All meta-analyses were performed using R (version 3.6.1); SAS (version 9.4, SAS Inc., Cary, North Carolina, United States) was used for plotting and all other analyses.
Sensitivity analysis
Some endoscopists use DPPS concomitantly with LAMS for various purposes. To account for potential confounding of safety and efficacy outcomes of LAMS, a sensitivity analysis was performed that removed all studies mentioning concomitant use of DPPS and LAMS. These results were compared with the main analyses of the overall cohort to assess for differences in safety or efficacy.
Results
Study selection and characteristics
The systematic literature search identified 628 unique articles, of which 30 studies representing 1,524 subjects met the inclusion criteria ( Fig. 1 ). Twenty-six eligible studies were retrospective; and 4 were prospective, including one randomized controlled trial (RCT) comparing DPPS to the specific LAMS. Twenty-six of the 41 studies from the prior 2018 review were excluded, most often for lack of data on the LAMS under study, having an patient population that were not mutually exclusive (the most comprehensive study was included), or duplicating another study ( Supplementary Table 3 ). In total, 598 articles were excluded ( Fig. 1 ), most often for lack of data on the intervention or outcomes under study (n = 211), or because they were review articles (n = 181) or case reports (n = 131). Median duration of follow-up for all eligible studies ranged from 5.5 weeks to 62.3 weeks.
Fig. 1.
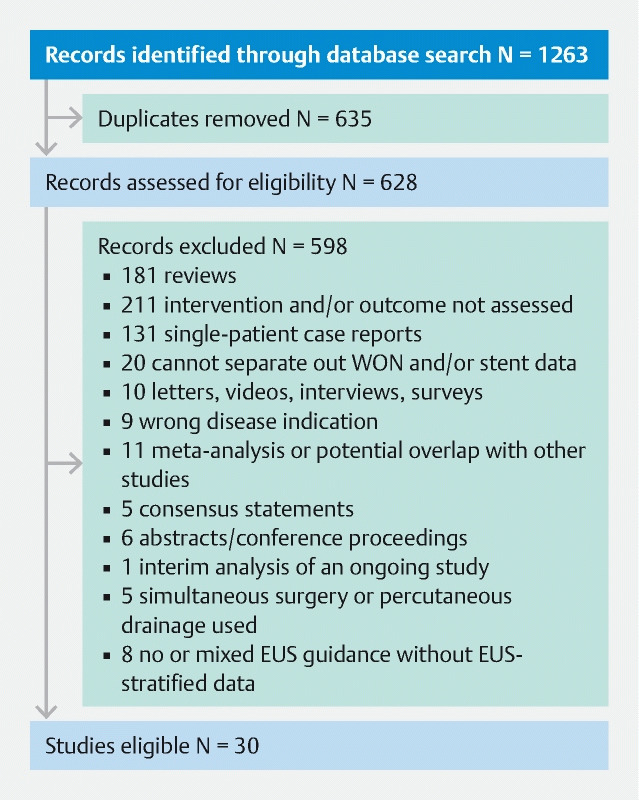
Flow diagram of literature search and study selection.
Study and patient characteristics are summarized in Table 1 . Seventeen studies including LAMS (all EUS-guided) and 16 studies with EUS – guided DPPS (including three studies that also had LAMS patients) were analyzed. Of these 30 studies, 25 reported endoscopic necrosectomy in at least one patient. Twenty-two studies reported a nasocystic drain in at least one patient, seven did not employ nasocystic drains, and one did not report on nasocystic drain usage. Thirteen studies reported WON infection status prior to the index procedure. Eleven studies did not define or describe WON dimensions, four did not collect and/or record WON size, and 15 reported specific WON size metrics ( Supplementary Table 4 ).
Table 1. Publications and extracted data.
| Study | Year | Design | Country | Patients with LAMS N = 899 |
Patients with DPPS N = 625 |
Follow – Up Time LAMS | Follow – Up Time DPPS | WON Size, cm Mean ± SD or [range] 1 |
Male Sex % |
Age (years) Mean ± SD |
| Kumar 41 | 2014 | Retrospective, single center, single-arm | USA | – | 12 | – | 1.9 ± 0.3 years | 13.1 ± 5.1 | 66 % | 58.9 ± 3.9 |
| Lin 42 | 2014 | Retrospective, multicenter, single-arm | China | – | 17 | – | NR for patients with WON only | Median 11.9 ± 5.2 | 47 % | Median 53 [range 32–79] |
| Rana 43 | 2014 | Retrospective, single center, single-arm | India | – | 43 | – | NR | 9.95 ± 2.75 | 83.7 % | 36.0 ± 10.1 |
| Rana 44 | 2015 | Retrospective, single center, single-arm | India | – | 35 | – | Mean 28.2 ± 14.0 months (range 6–50) | NR | 82.8 % | 37 ± 7.6 |
| Rinninella 45 | 2015 | Retrospective, multicenter, single-arm | Italy, Denmark, Spain, Germany, France, Netherlands | 52 | – | NR for patients with WON only | – | NR | NR | NR |
| Smoczynski 46 | 2015 | Retrospective, single center, single-arm | Poland | – | 64 | – | ≥ 12 Months | 14.6 [10.6–22] | NR | NR |
| Walter 47 | 2015 | Prospective, multicenter, single-arm | Germany, Spain, Denmark, Netherlands | 43 | – | – | – | NR for patients with WON only | NR | NR |
| Sharaiha 48 | 2016 | Retrospective, multicenter, single-arm | USA | 124 | – | – | Median 4 months [range 1–34] | 9.5 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 | 60 % | 54.2 ± 15.5 |
| Siddiqui 49 | 2016 | Retrospective, multicenter, single-arm | USA | 68 | – | – | NR | 12.12 ± 5.32 | 60.3 % | 51.7 ± 14.3 |
| Storm 39 | 2016 | Retrospective, single center, single-arm | USA | – | 15 | – | NR | NR | 60 % | 47.1 [range 27–62] |
| Thompson 50 | 2016 | Retrospective, single center, single-arm | USA | – | 60 | – | Mean 67.8 ± 9.9 weeks | NR | 60 % | 52.8 ± 2 |
| Adler 27 | 2017 | Retrospective, multicenter, single-arm | USA | 9 | – | Median 3 months | – | NR | NR | NR for patients with WON only |
| Bang 51 | 2017 | Retrospective, single center, matched comparative | USA | 13 | 26 (not eligible) | ≥ 90 Days | ≥ 90 Days | NR | NR | NR |
| Bapaye 52 | 2017 | Retrospective, single center, single-arm | India | – | 61 | – | ≥ 6 Weeks | 11.7 ± 30.1 70–200 | 87 % | 42.2 ± 12.8 |
| Bekkali 28 | 2017 | Retrospective, single center, single-arm | United Kingdom | 32 | – | Median 9.0 weeks (95 % CI 6.0–13.6) | – | 15 (95 % CI 7.7–21.7) | 56.3 % | Median 57 (range 19–81) |
| He 34 | 2017 | Prospective, single center, single-arm | China | – | 11 | – | 1 Year | NR | 45.5 % | Median 48 (IQR 27–55) |
| Rana 40 | 2017 | Retrospective, single center, single-arm | India | – | 6 | – | 14.5 ± 7.1 months | 8.33 | 100 % | 41 |
| Ren 53 | 2017 | Retrospective, single center, single-arm | China | – | 17 | – | Median 258 days | NR | 52.9 % | 51.1 |
| Siddiqui 54 | 2017 | Retrospective, multicenter, comparative | USA | 86 | 106 | ≥ 6 Months | ≥ 6 Months | LAMS: 11.4 DPPS: 10.6 |
LAMS: 90 % DPPS: 64 % |
LAMS: 51.5 DPPS: 56.3 |
| Tarantino 10 | 2017 | Retrospective, single center, single-arm | Italy | 19 | – | Mean 554.7 days (range 70–986) | – | 12.5 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 | 70 % | 58.7 ± 16 |
| Watanabe 55 | 2017 | Retrospective, single center, single-arm | Japan | – | 40 | NR for patients with WON only. | – | NR | NR | NR for patients with WON only |
| Yoo 56 | 2017 | Retrospective, multicenter, single-arm | USA | 22 | – | NR for patients with WON only. | – | NR | NR | NR for patients with WON only |
| Abu Dayyeh 19 | 2018 | Retrospective, single center, comparative | USA | 46 | 36 (not eligible) | NR | NR | LAMS: NR DPPS: 12.8 ± 5.8 |
LAMS: NR DPPS: 78 % |
LAMS: NR DPPS: 59.7± 16 |
| Garcia – Alonso 14 | 2018 | Prospective, single center, single-arm | Spain | 72 | – | Median 75 days | 78.5 days | NR | NR | NR |
| Law 29 | 2018 | Retrospective, single center, single-arm | NR | 46 | – | NR | – | Median 9.0 (IQR 4.5) | 69.6$ | Median 70 (IQR 26) |
| Shekhar 57 | 2018 | Retrospective, single center, single-arm | United Kingdom | – | 22 | – | NR for patients with WON only | NR | NR | NR for patients with WON only |
| Venkatachalapathy 58 | 2018 | Retrospective, multicenter, single-arm | United Kingdom | 70 | – | Median 45 days (range 8–206) | – | NR for patients with WON only | NR for patients with WON only | NR for patients with WON only |
| Yang 30 | 2018 | Retrospective, multicenter, single-arm | USA | 64 | – | Median 5.5 weeks | – | 13.08 ± 4.40 cm | 67 % | 51.8 ±14.4 |
| Bang 32 | 2019 | Prospective, single center, RCT | USA | 31 | 29 | 6 Months | 6 Months | LAMS: 10.2±4.6 DPPS: 10.7±6.8 |
LAMS: 69 % DPPS: 55 % |
LAMS: 55.8±15.6 DPPS: 60.3±13.0 |
| Chen 59 | 2019 | Retrospective, multicenter, comparative | USA | 102 | 87 | Median 144 days | Median 436 days | LAMS: 11.14 ± 4.36 DPPS: 13.5±5.8 |
LAMS:45 % DPPS: 53 % |
LAMS: 54 ± 16 DPPS: 57 + 15 |
LAMS, lumen-apposing metal stent; DPPS, double-pigtail plastic stent; IQR, interquartile range; NR, not reported; USA, United States of America; WON, walled-off necrosis.
Unless reported otherwise.
Study quality
All 30 publications were assessed for quality with the modified NOS. Fifteen studies were judged to be good-quality, eight moderate-quality, and seven poor-quality ( Supplementary Table 2 ).
Assessment of heterogeneity
Heterogeneity was found in the analyses of bleeding and stent migration in both LAMS and DPPS ( Supplementary Table 5 ), and in the analyses of stent occlusion and WON resolution in the DPPS group. No heterogeneity was found in the analyses of perforation for either group nor in the analyses of stent occlusion and WON resolution for the LAMS group.
Safety outcomes
Bleeding during or after drainage
Two studies defined bleeding as any bleed requiring transfusion, and five different studies used five different definitions of bleeding ( Supplementary Table 6 ). Eleven studies did not define bleeding but did describe incident bleeding events; four did not collect and/or record bleeding events; and seven did not provide a definition in the methods section.
Among 22 studies including 1,122 patients with analyzable bleeding data, bleeding rates were not significantly different in the LAMS group compared to the DPPS group (2.5 % vs. 4.6 % respectively, P = 0.39) ( Table 2 , Fig. 2a ).
Table 2. Summary of efficacy and safety meta – analytic outcomes for EUS – guided LAMS and DPPS treatment of WON.
| LAMS – EUS | DPPS – EUS | P value 1 | |||||
| N studies | N patients | % (95 % CI) | N studies | N patients | % (95 % CI) | ||
| Safety Outcomes | |||||||
| Bleeding | 14 | 741 | 2.5 % (0.7 %, 5.5 %) |
10 | 381 | 4.6 % (1.2 %, 10.0 %) |
0.39 |
| Perforation | 12 | 545 | 0.5 % (0.0 %, 1.3 %) |
6 | 287 | 1.1 % (0.2 %, 2.6 %) |
0.35 |
| Stent migration | 15 | 788 | 5.9 % (2.6 %, 10.6 %) |
5 | 318 | 6.8 % (2.6 %, 12.8 %) |
0.79 |
| Stent occlusion | 13 | 730 | 3.8 % (0.9 %, 8.7 %) |
4 | 239 | 5.2 % (0.0 %, 19.0 %) |
0.78 |
| Efficacy Outcomes | |||||||
| Resolution of WON | 16 | 827 | 87.4 % (83.0 %, 91.3 %) |
15 | 614 | 87.5 % (80.1 %, 93.4 %) |
0.99 |
| Number of procedures to achieve resolution | 2 | 115 | 2.09 (1.05, 3.13) |
6 | 191 | 1.88 (1.48, 2.29) |
0.72 |
| Total unique studies or patients | 17 | 899 | 16 | 625 | |||
CI, confidence interval; LAMS, lumen-apposing metal stents; DPPS, double-pigtail plastic stents; WON, walled-off necrosis; EUS, endoscopic ultrasound.
P value for comparison of DPPS to LAMS
Fig. 2 .
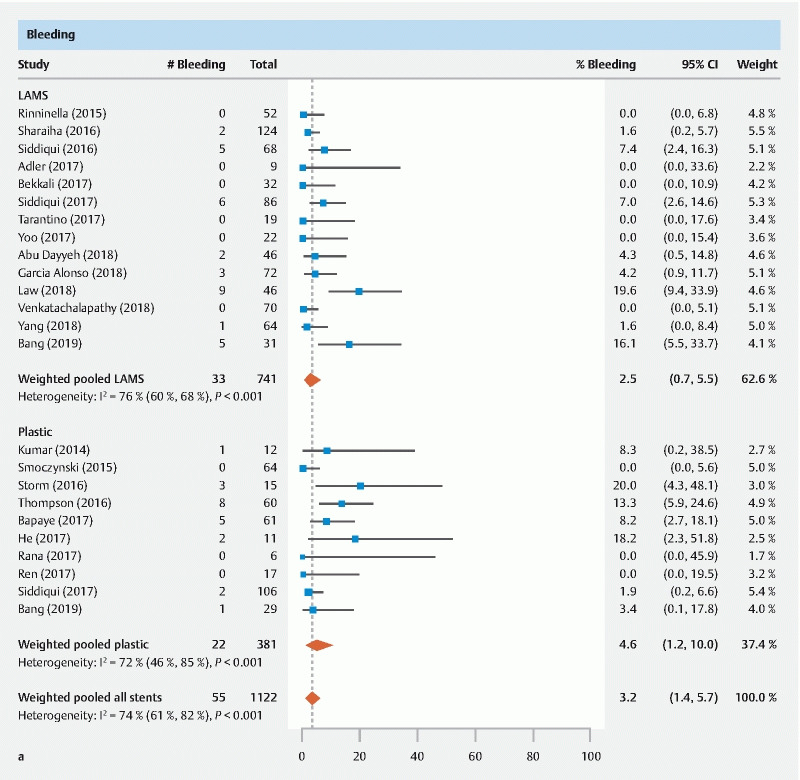
Analysis of safety outcomes. Outcomes for a bleeding.
Perforation
Varying definitions of perforation were used across studies. Two studies defined it as perforation of the WON wall/capsule only; one study defined it as pneumoperitoneum on imaging with associated peritoneal signs; eight studies did not define it in the methods section but described it in varying ways in the results; nine studies did not define it; and 11 studies did not collect and/or record it ( Supplementary Table 7 ).
Among 16 publications including 832 patients with analyzable perforation data, perforation rates were the same for the LAMS group vs. DPPS group (0.5 % vs. 1.1 % respectively; P = 0.35) ( Table 2 , Fig. 2b ).
Fig. 2 .
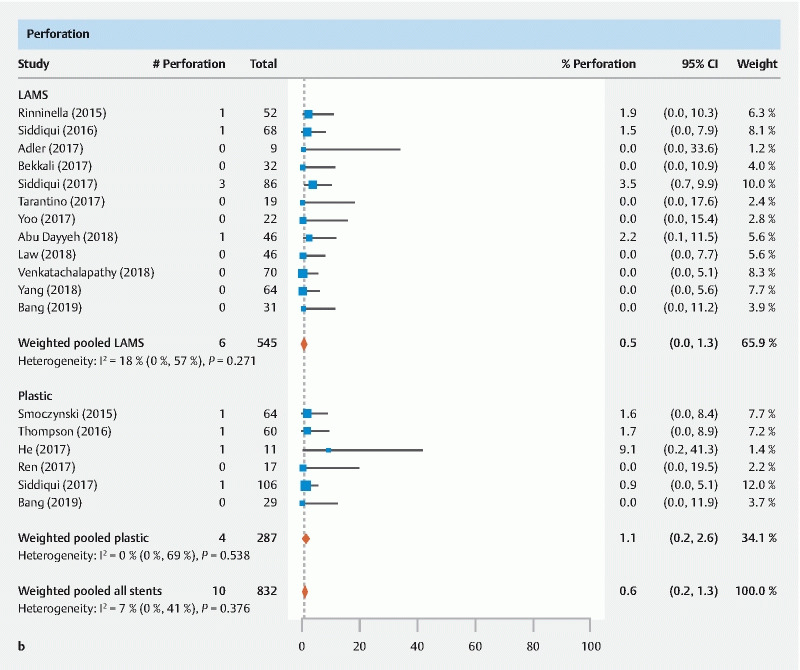
Analysis of safety outcomes. Outcomes for b perforation.
Stent migration
Stent migration was defined as migration within the WON or outside the WON in 2 studies; as involving retrieval from the WON cavity or the enteral lumen in 1 study; as other definitions in seven studies. In five studies, stent migration was defined in the results section of the publication, not in the methods; in eight studies it was not defined; and in seven studies it was not collected and/or recorded ( Supplementary Table 8 ).
Among 17 studies including 1,106 patients with analyzable stent migration data, stent migration occurred at similar rates in the LAMS group vs. DPPS group (5.9 % vs. 6.8 % respectively; P = 0.79) ( Table 2 , Fig. 2c ).
Fig. 2 .
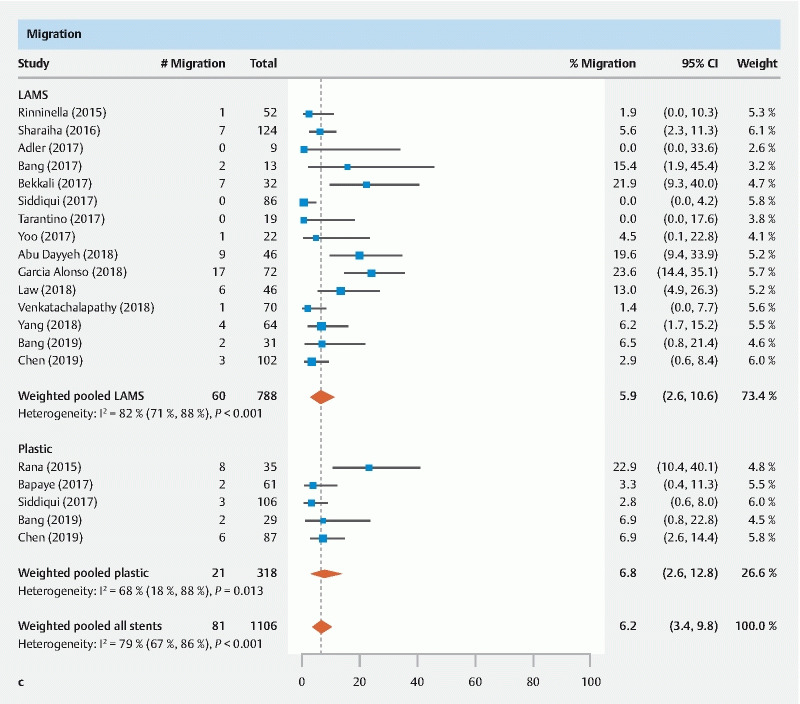
Analysis of safety outcomes. Outcomes for c stent migration.
Stent occlusion
Among 14 studies including 969 patients with analyzable stent occlusion data, stent occlusion occurred at insignificantly different rates in the LAMS group vs. DPPS group (3.8 % vs. 5.2 % respectively; P = 0.78) ( Table 2 , Fig. 2d ).
Fig. 2 .
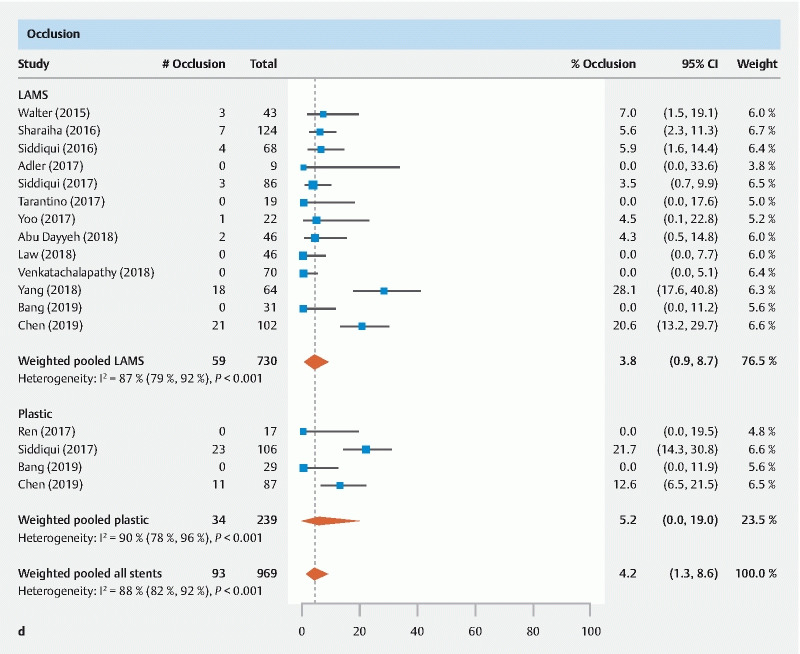
Analysis of safety outcomes. Outcomes for d stent occlusion.
Efficacy outcomes
Resolution of WON
Overall, six different definitions of WON resolution were used throughout the studies, and six studies did not provide a definition ( Supplementary Table 9 ). Twenty-four studies included symptom resolution in the definition, and the majority of studies used a radiologic measure to define resolution.
Among 28 studies including 1,441 patients with analyzable data on WON resolution, WON resolution rates were similar for LAMS vs. DPPS (87.4 % vs. 87.5 % respectively, P = 0.99) ( Table 2 , Fig. 3a ).
Fig. 3.
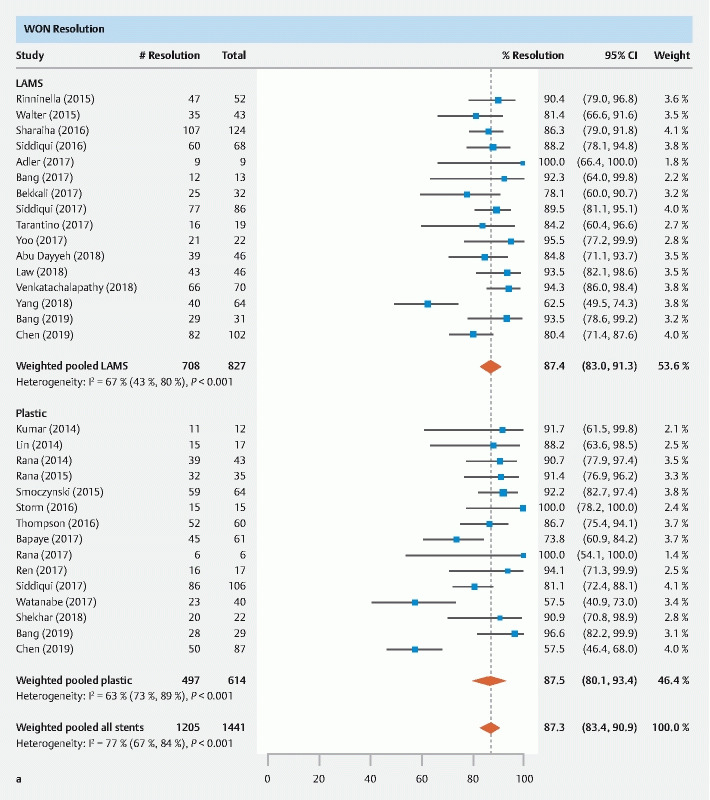
Analysis of efficacy outcomes. Outcomes for a resolution of WON.
Total number of procedures to achieve resolution
Seven publications with 306 patients reported the total number of endoscopic procedures needed to achieve WON resolution. This number was similar between the specific LAMS vs. DPPS (2.09 vs. 1.88 procedures respectively; P = 0.72) ( Table 2 , Fig. 3b ).
Fig. 3.
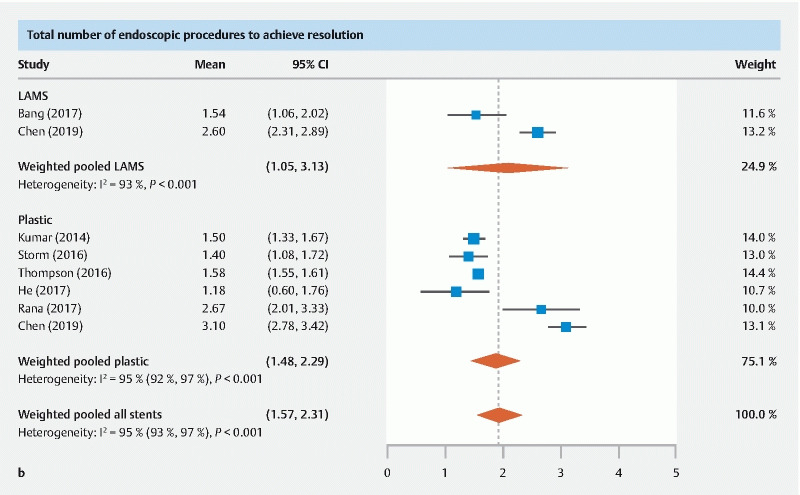
Analysis of efficacy outcomes. Outcomes for b total number of endoscopic procedures to achieve resolution.
Subanalysis including EUS- and non-EUS-guided cases
Expanding the analysis to include non-EUS-guided cases led to two statistically significant changes in the LAMS vs. DPPS comparisons. Estimated bleeding rate in the DPPS group increased and was significantly higher than the bleeding rate for LAMS (9.0 % vs. 2.5 % respectively, P = 0.009) ( Supplementary Table 10 ). Similarly, the estimated perforation rate for DPPS increased and was significantly higher than the rate for LAMS (2.6 % vs. 0.5 % respectively, P = 0.005). LAMS and DPPS had similar performance for all other safety and efficacy endpoints in the sub-analysis.
Sensitivity analysis of concomitant use of DPPS with LAMS
Five studies (223 patients) 14 27 28 29 30 included in the analysis noted concomitant use of DPPS together with LAMS. One study placed DPPS to help anchor the LAMS 29 (information obtained via correspondence with the author in the case of one study 29 ); one study placed DPPS to reduce the risk of stent occlusion in 4 of 9 patients 27 ; and three studies utilized concomitant DPPS at the discretion of the endoscopist, but did not indicate the number of patients in which it was used 14 28 30 . When removing these 5 studies with concomitant DPPS and LAMS use from safety and efficacy analyses, conclusions did not change ( Table 3 ).
Table 3. Sensitivity analysis of studies that had no concomitant use of DPPS with LAMS.
| Outcome | LAMS with DPPS use (1) Studies = 5 |
LAMS no DPPS use (2) Studies = 12 |
P
value
1 vs 2 |
DPPS (3) Studies = 26 |
P
value
2 vs 3 |
|||
| N | % | N | % | N | % | |||
| Safety Outcomes | ||||||||
| Bleeding | 223 | 3.0 % | 518 | 2.2 % | 0.78 | 381 | 4.6 % | 0.35 |
| Perforation | 151 | 0.0 % | 394 | 0.9 % | 0.064 | 287 | 1.1 % | 0.82 |
| Stent migration | 223 | 12.3 % | 565 | 3.7 % | 0.046 | 318 | 6.8 % | 0.29 |
| Stent occlusion | 119 | 3.8 % | 611 | 3.7 % | 0.99 | 239 | 5.2 % | 0.76 |
| Efficacy Outcomes 1 | ||||||||
| Resolution of WON | 151 | 86.4 % | 676 | 88.0 % | 0.85 | 614 | 87.5 % | 0.88 |
CI, confidence interval; LAMS, lumen-apposing metal stents, DPPS, double-pigtail plastic stents; WON, walled-off necrosis.
Number of procedures not reported for the five studies of LAMS with concomitant DPPS use.
Publication bias
There was no significant publication bias (p > 0.10) for LAMS studies ( Supplementary Table 11 ); however, the Begg and Mazumdar test was significant (p ≤ 0.10) for perforation. The Egger test showed a lack of symmetry of the funnel plots ( Supplementary Fig. 1a–f ) only for migration and resolutions for DPPS.
Discussion
Management of WON has evolved from open surgical interventions to minimally invasive strategies that routinely involve endoscopic drainage. Despite increased use of endoscopic drainage of WON, the ideal endoscopic technique, including stent choice remains unclear. LAMS have been increasingly utilized for endoscopic WON management, have several theoretical advantages over DPPS and were a suggested option for endoscopic WON management in a 2020 clinical practice update 31 for management of pancreatic necrosis. Larger caliber LAMS may allow for subsequent easy access to the WON cavity for inspection and necrosectomy without the need for stent removal/exchange nor dilation of the cyst-enterostomy tract. In addition, the larger diameter of indwelling LAMS allows spontaneous drainage of solid debris. However, enthusiasm for the intuitive advantages of LAMS has been mitigated by recent reports of high bleeding rates noted with LAMS. The majority of relevant published studies are single-arm retrospective cohort studies. By grading the quality of evidence and following established guidelines, we aimed to conduct a high-quality systematic review and meta-analysis to carefully evaluate the safety and efficacy of LAMS and to provide a basis for comparison to DPPS for the management of WON.
In this study, we found that LAMS was associated with similar rates of bleeding compared to DPPS for WON. Bleeding associated with endoscopic drainage of WON may occur either from the cyst-enterostomy tract, from vessels within the cavity, or remote from the cyst-enterostomy stent. While in theory, placement of a large diameter LAMS may reduce the risk of bleeding from the tract by tamponading superficial vessels in the GI wall, collapse of the WON cavity may lead to increased risk of erosion of the back wall of the cavity against the edge of the LAMS compared to softer and rounded DPPS 9 . Coaxial placement of a DPPS within a LAMS did not reduce the rate of bleeding (3.0 %) compared to LAMS placement alone (2.2 %, P = 0.78).
There were similar rates of perforation with LAMS compared to DPPS. This rate was significantly higher for DPPS when studies with and without EUS were included. The covering membrane of LAMS along with its high mechanical lumen-apposing force instinctively may seal perforation or defects from the cyst-enterostomy tract compared with DPPS which have no lateral covering or support.
Despite the larger caliber design of LAMS, stent migration and stent occlusion were noted to be similar with LAMS and DPPS. AE rates as a function of indwelling time of the stent could not be evaluated with this analysis due to insufficient detail in published data. In the only RCT included in this analysis, interim assessment of overall stent-related AE rate was noted to be higher for LAMS (8 events, 25.8 %) than for DPPS (0 events), all of which were observed at ≥ 3 weeks post-procedure. After the safety board mandated a CT scan at 3 weeks post-LAMS-insertion with stent removal upon detection of WON resolution, stent-related AE rates were similar (6.5 % vs 6.9 % respectively, P = 0.999) 32 . The authors reported four LAMS-related bleeding events (3 prior to and 1 after the protocol amendment) and an episode of massive bleeding during stent retrieval of a buried LAMS prior to the protocol amendment; therefore, we included 5 bleeding episodes for the LAMS cohort.
Our study also provides important information regarding current practices associated with stent placement for drainage of WON. For example, the majority of studies reported concomitant therapy with endoscopic necrosectomy and nasocystic drains; most studies of AXIOS TM used both 10 and 15 mm AXIOS TM stents and about half used the electrocautery-tipped Hot AXIOS TM ; and 13 out of 30 studies reported the rate of infected WON prior to the index procedure. Infected WON collections almost always require necrosectomy to improve treatment success rates and may sometimes require multiple interventions to achieve clinical success. Given the high rates of concomitant therapy of nasocystic drainage with endoscopic necrosectomy, this study evaluates WON resolution after a single procedure, and provides an important assessment of the efficacy of the stents to effectuate disease resolution on their own without subsequent intervention.
Our evaluation of the notable lack of uniformity in outcome definitions and consistency in outcome reporting across studies also provides an important appraisal of the current state of the research in this disease area. Definitions of WON resolution, perforation, stent migration, and stent occlusion differed among studies, and in several cases, no definitions were provided. Although authors are attempting to better define study outcomes 33 , there remains wide variation in the interpretation of each event. For example, perforation could imply puncture of the WON wall or of another organ; it could also indicate fault of the operator (procedure-related) or fault of the stent, but clear and precise definitions are lacking and should be clarified in future studies. Other authors have noted that the relatively large variations in reported complication rates in these studies may be partially attributable to the different definitions of complications or in the length of follow-up 17 . The definition of WON resolution, which not only differed between studies but also in terms of the timeframe in which resolution was assessed, ranged from ≤ 4 weeks 28 in some studies to > 1 year in others 34 . In addition, WON size reporting was not standardized, with some studies reporting the length of the longest axis of the WON, and other studies not specifying the dimension being reported. The lack of reporting standards across these studies highlights the need for uniformity in outcome definition and reporting in this treatment area.
This meta-analysis is the largest study to date assessing the safety and efficacy of the LAMS under study compared with DPPS for treatment of WON. Other strengths of the present study include the large sample size of studies from diverse regions of the world. In addition to the outcome definition and reporting problems noted above, our study had other limitations. The majority of the studies included in this meta-analysis were single cohort retrospective studies with few comparative studies and only one RCT. To provide data on WON only 35 , several studies had to be excluded due to the reporting of WON and pseudocyst outcomes together 11 36 37 . Data were collected by expert endoscopists at large tertiary referral centers; however, a small 2019 study 38 reported successful use of LAMS to treat WON in a community hospital. We could not control for differences in endoscopic methods (e. g., cyclic irrigation technique, multiple transluminal gateway technique, etc.), nor populations that were unique or with comorbidities 39 40 . Data on number of plastic stents used; average stent indwell time; timing of bleeding (periprocedural, early or late postprocedural, puncture-related); estimated amount of solid vs. liquid necrosis that might influence stent choice; presence of disconnected pancreatic duct/parenchyma or paracolic gutter extension that might influence WON resolution; and proton pump inhibitor use could not be analyzed because they were incompletely reported or not reported among studies. Reporting of these items could improve future meta-analyses by allowing estimates of time to WON resolution, and by identifying patient populations at higher risk of delayed WON resolution or increased adverse events. Cost-effectiveness was outside the scope of this analysis. Although one prospective study did not demonstrate a benefit in treatment outcomes of LAMS for WON 32 , a large, multicenter RCT is needed to better determine if LAMS with frequent WON assessments improve WON treatment outcomes compared to DPPS.
Conclusions
In this systematic review and meta-analysis of 30 studies with 1,524 patients with WON, we found that compared to DPPS with EUS guidance, LAMS was associated with similar rates of bleeding, perforation, stent migration, stent occlusion and WON resolution. Further study is needed to determine the efficacy and safety of LAMS in patient subgroups and mid/long-term outcomes are needed. Additionally, given the inconsistency in outcome definitions and reporting, improved research standards should be implemented across studies, providing specific, clear, and uniform outcome definitions and clarify the manner and location of AEs. Careful monitoring of WON resolution may be important to reduce the risk of adverse events.
Acknowledgement
The data, analytic methods, and study materials for this study may be made available to other researchers in accordance with the Boston Scientific Data Sharing Policy ( http://www.bostonscientific.com/en-US/data-sharing-requests.html ).
Footnotes
Competing interests Dr. Chandrasekhara is on the Advisory Board of Interpace Diagnostics and is a shareholder in Nevakar Corporation. Dr. Barthet received a research grant from Boston Scientific Corporation. Dr. Devière has received grants from Boston Scientific Corporation, Cook Endoscopy, and Olympus, and is a shareholder in Endotools. Dr. Easler is a consultant for Boston Scientific Corporation. Dr. Peetermans, Mr. McMullen, Ms. Gjata, and Dr. Gourlay are full – time employees of Boston Scientific Corporation. Dr. Abu Dayyeh received a research grant and consultation fee from Boston Scientific Corporation, research support from Medtronic, and education/lecture fees from Olympus.
Supplementary material :
References
- 1.Peery A F, Crockett S D, Murphy C C et al. Burden and cost of gastrointestinal, liver, and pancreatic diseases in the United States: update 2018. Gastroenterology. 2019;156:254–2.72E13. doi: 10.1053/j.gastro.2018.08.063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yadav D, Lowenfels A B. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013;144:1252–1261. doi: 10.1053/j.gastro.2013.01.068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Banks P A, Bollen T L, Dervenis C et al. Classification of acute pancreatitis – 2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62:102–111. doi: 10.1136/gutjnl-2012-302779. [DOI] [PubMed] [Google Scholar]
- 4.Aparna D, Kumar S, Kamalkumar S. Mortality and morbidity in necrotizing pancreatitis managed on principles of step-up approach: 7 years experience from a single surgical unit. World J Gastrointest Surg. 2017;9:200–208. doi: 10.4240/wjgs.v9.i10.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ashley S W, Perez A, Pierce E A.Necrotizing pancreatitis: contemporary analysis of 99 consecutive cases Ann Surg 2001234572–579.; discussion 579-580 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schmid S W, Uhl W, Friess H et al. The role of infection in acute pancreatitis. Gut. 1999;45:311–316. doi: 10.1136/gut.45.2.311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Petrov M S, Shanbhag S, Chakraborty M et al. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology. 2010;139:813–820. doi: 10.1053/j.gastro.2010.06.010. [DOI] [PubMed] [Google Scholar]
- 8.Muthusamy V R, Chandrasekhara V, Acosta R D et al. The role of endoscopy in the diagnosis and treatment of inflammatory pancreatic fluid collections. Gastrointestinal endoscopy. 2016;83:481–488. doi: 10.1016/j.gie.2015.11.027. [DOI] [PubMed] [Google Scholar]
- 9.Bang J Y, Hasan M, Navaneethan U et al. Lumen–apposing metal stents (LAMS) for pancreatic fluid collection (PFC) drainage: may not be business as usual. Gut. 2017;66:2054–2056. doi: 10.1136/gutjnl-2016-312812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tarantino I, Ligresti D, Tuzzolino F et al. Clinical impact of EUS treatment of walled–off pancreatic necrosis with dedicated devices. Endosc Int Open. 2017;5:E784–E791. doi: 10.1055/s-0043-112494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Brimhall B, Han S, Tatman P D et al. Increased incidence of pseudoaneurysm bleeding with lumen–apposing metal stents compared to double pigtail plastic stents in patients with peripancreatic fluid collections. Clin Gastroenterol Hepatol. 2018 doi: 10.1016/j.cgh.2018.02.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sahar N, Kozarek R, Kanji Z S et al. Do lumen-apposing metal stents (LAMS) improve treatment outcomes of walled-off pancreatic necrosis over plastic stents using dual-modality drainage? Endosc Int Open. 2017;5:E1052–E1059. doi: 10.1055/s-0043-111794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zhu H, Lin H, Jin Z et al. Re-evaluation of the role of lumen-apposing metal stents (LAMS) for pancreatic fluid collection drainage. Gut. 2017;66:2192. doi: 10.1136/gutjnl-2017-313949. [DOI] [PubMed] [Google Scholar]
- 14.Garcia-Alonso F J, Sanchez-Ocana R, Penas-Herrero I et al. Cumulative risks of stent migration and gastrointestinal bleeding in patients with lumen–apposing metal stents. Endoscopy. 2018;50:386–395. doi: 10.1055/a-0581-9040. [DOI] [PubMed] [Google Scholar]
- 15.Zeissig S, Sulk S, Brueckner S et al. Severe bleeding is a rare event in patients receiving lumen-apposing metal stents for the drainage of pancreatic fluid collections. Gut. 2019;68:945–946. doi: 10.1136/gutjnl-2018-316581. [DOI] [PubMed] [Google Scholar]
- 16.Mussetto A, Fugazza A, Fuccio L et al. Current uses and outcomes of lumen-apposing metal stents. Annals of gastroenterology. 2018;31:535. doi: 10.20524/aog.2018.0287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.DeSimone M L, Asombang A W, Berzin T M. Lumen apposing metal stents for pancreatic fluid collections: Recognition and management of complications. World J Gastrointest Endosc. 2017;9:456–463. doi: 10.4253/wjge.v9.i9.456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bazerbachi F, Sawas T, Vargas E J et al. Metal stents versus plastic stents for the management of pancreatic walled-off necrosis: a systematic review and meta-analysis. Gastrointest Endosc. 2018;87:30–4.2E16. doi: 10.1016/j.gie.2017.08.025. [DOI] [PubMed] [Google Scholar]
- 19.Abu Dayyeh B K, Mukewar S, Majumder S et al. Large-caliber metal stents versus plastic stents for the management of pancreatic walled-off necrosis. Gastrointest Endosc. 2018;87:141–149. doi: 10.1016/j.gie.2017.04.032. [DOI] [PubMed] [Google Scholar]
- 20.Moher D, Liberati A, Tetzlaff J et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Haffar S, Bazerbachi F, Prokop L et al. Frequency and prognosis of acute pancreatitis associated with fulminant or non-fulminant acute hepatitis A: A systematic review. Pancreatology. 2017;17:166–175. doi: 10.1016/j.pan.2017.02.008. [DOI] [PubMed] [Google Scholar]
- 22.Bazerbachi F, Leise M D, Watt K D et al. Systematic review of mixed cryoglobulinemia associated with hepatitis E virus infection: association or causation? Gastroenterol Rep (Oxf) 2017;5:178–184. doi: 10.1093/gastro/gox021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Murad M H, Sultan S, Haffar S et al. Methodological quality and synthesis of case series and case reports. BMJ Evid Based Med. 2018;23:60–63. doi: 10.1136/bmjebm-2017-110853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Higgins J P, Thompson S G, Deeks J J et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Begg C B, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994:1088–1101. [PubMed] [Google Scholar]
- 26.Egger M, Smith G D, Schneider M et al. Bias in meta–analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Adler D G, Taylor L J, Hasan R et al. A retrospective study evaluating endoscopic ultrasound-guided drainage of pancreatic fluid collections using a novel lumen–apposing metal stent on an electrocautery enhanced delivery system. Endosc Ultrasound. 2017;6:389–393. doi: 10.4103/eus.eus_4_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bekkali N LH, Nayar M K, Leeds J S et al. A comparison of outcomes between a lumen-apposing metal stent with electrocautery-enhanced delivery system and a bi-flanged metal stent for drainage of walled-off pancreatic necrosis. Endosc Int Open. 2017;5:E1189–E1196. doi: 10.1055/s-0043-120831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Law S T, De La Serna Higuera C, Simón P G et al. Comparison of clinical efficacies and safeties of lumen-apposing metal stent and conventional-type metal stent-assisted EUS-guided pancreatic wall-off necrosis drainage: a real-life experience in a tertiary hospital. Surg Endosc. 2018;32:2448–2453. doi: 10.1007/s00464-017-5946-6. [DOI] [PubMed] [Google Scholar]
- 30.Yang D, Perbtani Y B, Mramba L K et al. Safety and rate of delayed adverse events with lumen-apposing metal stents (LAMS) for pancreatic fluid collections: a multicenter study. Endosc Int Open. 2018;6:E1267–E1275. doi: 10.1055/a-0732-502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Baron T H, DiMaio C J, Wang A Y et al. American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis. Gastroenterology. 2020;158:67–75. doi: 10.1053/j.gastro.2019.07.064. [DOI] [PubMed] [Google Scholar]
- 32.Bang J Y, Navaneethan U, Hasan M K et al. Non-superiority of lumen-apposing metal stents over plastic stents for drainage of walled-off necrosis in a randomised trial. Gut. 2019;68:1200–1209. doi: 10.1136/gutjnl-2017-315335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lakhtakia S, Basha J, Talukdar R et al. Endoscopic “step-up approach” using a dedicated biflanged metal stent reduces the need for direct necrosectomy in walled-off necrosis (with videos) Gastrointest Endosc. 2017;85:1243–1252. doi: 10.1016/j.gie.2016.10.037. [DOI] [PubMed] [Google Scholar]
- 34.He W H, Zhu Y, Liu P et al. The outcomes of initial endoscopic transluminal drainage are superior to percutaneous drainage for patients with infected pancreatic necrosis: a prospective cohort study. Surg Endosc. 2017;31:3004–3013. doi: 10.1007/s00464-016-5324-9. [DOI] [PubMed] [Google Scholar]
- 35.Tenner S, Baillie J, DeWitt J et al. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol. 2013;108:1400–1416. doi: 10.1038/ajg.2013.218. [DOI] [PubMed] [Google Scholar]
- 36.Lang G D, Fritz C, Bhat T et al. EUS-guided drainage of peripancreatic fluid collections with lumen-apposing metal stents and plastic double-pigtail stents: comparison of efficacy and adverse event rates. Gastrointest Endosc. 2018;87:150–157. doi: 10.1016/j.gie.2017.06.029. [DOI] [PubMed] [Google Scholar]
- 37.Consiglieri C F, Gornals J B, Busquets J et al. Fluoroscopy-assisted vs fluoroless endoscopic ultrasound-guided transmural drainage of pancreatic fluid collections: A comparative study. Gastroenterol Hepatol. 2018;41:12–21. doi: 10.1016/j.gastrohep.2017.07.008. [DOI] [PubMed] [Google Scholar]
- 38.Garg R, Chaar A, Szpunar S. Efficacy and safety of lumen-apposing stents for management of pancreatic fluid collections in a community hospital setting. Clinical Endoscopy. 2020;53:480–486. doi: 10.5946/ce.2019.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Storm A C, Thompson C C. Safety of direct endoscopic necrosectomy in patients with gastric varices. World J Gastrointest Endosc. 2016;8:402–408. doi: 10.4253/wjge.v8.i10.402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rana S S, Kumar A, Lal A et al. Safety and efficacy of angioembolisation followed by endoscopic ultrasound guided transmural drainage for pancreatic fluid collections associated with arterial pseudoaneurysm. Pancreatology. 2017;17:658–662. doi: 10.1016/j.pan.2017.08.002. [DOI] [PubMed] [Google Scholar]
- 41.Kumar N, Conwell D L, Thompson C C. Direct endoscopic necrosectomy versus step-up approach for walled-off pancreatic necrosis: comparison of clinical outcome and health care utilization. Pancreas. 2014;43:1334–1339. doi: 10.1097/MPA.0000000000000213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Lin H, Zhan X B, Sun S Y et al. Stent selection for endoscopic ultrasound–guided drainage of pancreatic fluid collections: a multicenter study in china. Gastroenterol Res Pract. 2014;2014:193562. doi: 10.1155/2014/193562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Rana S S, Bhasin D K, Sharma R K et al. Do the morphological features of walled off pancreatic necrosis on endoscopic ultrasound determine the outcome of endoscopic transmural drainage? Endosc Ultrasound. 2014;3:118–122. doi: 10.4103/2303-9027.131039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Rana S S, Bhasin D K, Sharma R et al. Factors determining recurrence of fluid collections following migration of intended long term transmural stents in patients with walled off pancreatic necrosis and disconnected pancreatic duct syndrome. Endosc Ultrasound. 2015;4:208–212. doi: 10.4103/2303-9027.162999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Rinninella E, Kunda R, Dollhopf M et al. EUS-guided drainage of pancreatic fluid collections using a novel lumen-apposing metal stent on an electrocautery-enhanced delivery system: a large retrospective study (with video) Gastrointest Endosc. 2015;82:1039–1046. doi: 10.1016/j.gie.2015.04.006. [DOI] [PubMed] [Google Scholar]
- 46.Smoczyński M, Jagielski M, Jabłońska A et al. Endoscopic necrosectomy under fluoroscopic guidance – a single center experience. Wideochir Inne Tech Maloinwazyjne. 2015;10:237–243. doi: 10.5114/wiitm.2015.52058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Walter D, Will U, Sanchez-Yague A et al. A novel lumen-apposing metal stent for endoscopic ultrasound-guided drainage of pancreatic fluid collections: a prospective cohort study. Endoscopy. 2015;47:63–67. doi: 10.1055/s-0034-1378113. [DOI] [PubMed] [Google Scholar]
- 48.Sharaiha R Z, Tyberg A, Khashab M A et al. Endoscopic therapy with lumen-apposing metal stents is safe and effective for patients with pancreatic walled-off necrosis. Clin Gastroenterol Hepatol. 2016;14:1797–1803. doi: 10.1016/j.cgh.2016.05.011. [DOI] [PubMed] [Google Scholar]
- 49.Siddiqui A A, Adler D G, Nieto J et al. EUS-guided drainage of peripancreatic fluid collections and necrosis by using a novel lumen-apposing stent: a large retrospective, multicenter U.S. experience (with videos) Gastrointest Endosc. 2016;83:699–707. doi: 10.1016/j.gie.2015.10.020. [DOI] [PubMed] [Google Scholar]
- 50.Thompson C C, Kumar N, Slattery J et al. A standardized method for endoscopic necrosectomy improves complication and mortality rates. Pancreatology. 2016;16:66–72. doi: 10.1016/j.pan.2015.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bang J Y, Hasan M K, Navaneethan U et al. Lumen-apposing metal stents for drainage of pancreatic fluid collections: When and for whom? Dig Endosc. 2017;29:83–90. doi: 10.1111/den.12681. [DOI] [PubMed] [Google Scholar]
- 52.Bapaye A, Dubale N A, Sheth K A et al. Endoscopic ultrasonography-guided transmural drainage of walled-off pancreatic necrosis: Comparison between a specially designed fully covered bi-flanged metal stent and multiple plastic stents. Dig Endosc. 2017;29:104–110. doi: 10.1111/den.12704. [DOI] [PubMed] [Google Scholar]
- 53.Ren Y C, Chen S M, Cai X B et al. Endoscopic ultrasonography-guided drainage combined with trans-duodenoscope cyclic irrigation technique for walled-off pancreatic necrosis. Dig Liver Dis. 2017;49:38–44. doi: 10.1016/j.dld.2016.08.120. [DOI] [PubMed] [Google Scholar]
- 54.Siddiqui A A, Kowalski T E, Loren D E et al. Fully covered self-expanding metal stents versus lumen-apposing fully covered self-expanding metal stent versus plastic stents for endoscopic drainage of pancreatic walled-off necrosis: clinical outcomes and success. Gastrointest Endosc. 2017;85:758–765. doi: 10.1016/j.gie.2016.08.014. [DOI] [PubMed] [Google Scholar]
- 55.Watanabe Y, Mikata R, Yasui S et al. Short- and long-term results of endoscopic ultrasound-guided transmural drainage for pancreatic pseudocysts and walled-off necrosis. World J Gastroenterol. 2017;23:7110–7118. doi: 10.3748/wjg.v23.i39.7110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Yoo J, Yan L, Hasan R et al. Feasibility, safety, and outcomes of a single-step endoscopic ultrasonography-guided drainage of pancreatic fluid collections without fluoroscopy using a novel electrocautery-enhanced lumen-apposing, self-expanding metal stent. Endosc Ultrasound. 2017;6:131–135. doi: 10.4103/2303-9027.204814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Shekhar C, Maher B, Forde C et al. Endoscopic ultrasound-guided pancreatic fluid collectionsʼ transmural drainage outcomes in 100 consecutive cases of pseudocysts and walled off necrosis: a single-centre experience from the United Kingdom. Scand J Gastroenterol. 2017 doi: 10.1080/00365521.2017.1398346. [DOI] [PubMed] [Google Scholar]
- 58.Venkatachalapathy S V, Bekkali N, Pereira S et al. Multicenter experience from the UK and Ireland of use of lumen-apposing metal stent for transluminal drainage of pancreatic fluid collections. Endosc Int Open. 2018;6:E259–E265. doi: 10.1055/s-0043-125362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Chen Y-I, Yang J, Friedland S et al. Lumen apposing metal stents are superior to plastic stents in pancreatic walled-off necrosis: a large international multicenter study. Endosc Int Open. 2019;7:E347–E354. doi: 10.1055/a-0828-7630. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.