

Key Points
Question
What are the differences in care and outcomes of patients with ST-segment elevation myocardial infarction among 3 vertical levels of hospitals in China?
Findings
In this cross-sectional study using data from the China Acute Myocardial Infarction Registry, which included 108 hospitals at the province, prefecture, and county levels, compared with patients in province-level hospitals, the rates of reperfusion therapy were lower among those in prefecture-level and county-level hospitals (69.4% vs 54.3% vs 45.8%). In-hospital mortality rates progressively increased among the 3 levels of hospitals, from 3.1% at the province level to 5.3% at the prefecture level to 10.2% at the county level.
Meaning
These findings suggest that more efforts should be made to address the gaps in care and outcomes of ST-segment elevation myocardial infarction for national quality improvement in China.
This cross-sectional study examines the variations in care and outcomes of patients with acute ST-segment elevation myocardial infarction (STEMI) at 3 different levels of hospitals—province, prefecture, and county—in China.
Abstract
Importance
The incidence of acute myocardial infarction has increased over the past decades in China, and management challenges include an unbalanced economy, disparate resources, and variable access to medical care across the nation.
Objective
To examine the variations in care and outcomes of patients with ST-segment elevation myocardial infarction among 3 levels of hospitals in the typical Chinese public hospital model.
Design, Setting, and Participants
This cross-sectional study used data from the China Acute Myocardial Infarction Registry to compare the differences in care and outcomes among patients at 108 hospitals from 31 provinces and municipalities throughout mainland China. Participants included patients with ST-segment elevation myocardial infarction directly admitted to hospitals between January 2013 and September 2014. Data analyses were performed from June 2015 to June 2019.
Exposures
Care in province-level, prefecture-level, or county-level hospitals in China.
Main Outcomes and Measures
The primary outcome was in-hospital mortality. Secondary outcomes included presentation, treatments, and major complications.
Results
A total of 12 695 patients (9593 men [75.6%]; median [interquartile range] age, 63 [54-72] years) were included; 3985 were at province-level hospitals, 6731 were at prefecture-level hospitals, and 1979 were at county-level hospitals. Compared with patients admitted to province-level hospitals, those admitted to prefecture-level and county-level hospitals were older (median [interquartile range] age, 61 [52-70] years vs 63 [54-72] years and 65 [57-75] years) and more likely to be women (815 women [20.5%] vs 1620 women [24.1%] and 667 women [33.7%]). Patients in prefecture-level and county-level hospitals were less likely to use ambulances compared with patients at province-level hospitals (11.6% [95% CI, 10.8%-12.4%] and 12.0% [95% CI, 10.6%-13.5%] vs 19.4% [95% CI, 18.1%-20.7%]; P < .001) and were less likely to experience early presentation, with onset-to-arrival times less than 12 hours for 75.3% (95% CI, 73.9%-76.6%) of patients at province-level hospitals, 70.8% (95% CI, 69.7%-71.9%) of patients at prefecture-level hospitals, and 69.8% (95% CI, 67.7%-71.8%) of patients at county-level hospitals (P < .001). The rates of reperfusion therapy were significantly lower in low-level hospitals (54.3% [95% CI, 53.1%-55.5%] for prefecture-level hospitals and 45.8% [95% CI, 43.6%-48.1%] for county-level hospitals) compared with province-level hospitals (69.4% [95% CI, 67.9%-70.8%]; P < .001). There was a progressively higher rate of in-hospital mortality at the 3 levels of hospitals: 3.1% (95% CI, 2.6%-3.7%) for province-level hospitals, 5.3% (95% CI, 4.8%-5.9%) for prefecture-level hospitals, and 10.2% (95% CI, 8.9%-11.7%) for county-level hospitals (P for trend < .001). After adjustment for patient characteristics, presentation, hospital facility, and treatments, the odds of death remained higher in prefecture-level (odds ratio, 1.39 [95% CI, 1.06-1.84]) and county-level (odds ratio, 1.43 [95% CI, 0.97-2.11]) hospitals compared with province-level hospitals (P for trend = .04).
Conclusions and Relevance
These findings suggest that there are significant variations in care and outcomes of patients among the 3 levels of hospitals in China. More efforts should be made to address the identified gaps, particularly in the prefecture-level and county-level hospitals. This work can inform national quality improvements efforts in China and in other developing countries.
Introduction
Ischemic heart disease is the leading cause of death in both developed and developing countries like China, largely due to acute coronary syndromes, particularly acute myocardial infarction (AMI).1 The mortality rate attributed to AMI remains variable across different regions worldwide.2,3,4 A decrease in deaths due to AMI has been seen in some countries, mainly because of the improvements in emergency medical services (EMSs), widespread adoption of early reperfusion therapy, and optimal medication usage in routine practice.5,6,7,8,9,10 On the other hand, the mortality rate associated with AMI is steady or even elevated in developing countries, which account for more than 80% of global deaths due to ischemic heart disease.2,3 The data on deaths in China demonstrated an upward trend by 5.6-fold in AMI-related deaths in both urban and rural populations from 1987 to 2014, with acceleration from 2006 onward and a more rapid increase in rural regions.11 A retrospective study12 also indicated that the in-hospital mortality rate for ST-segment elevation myocardial infarction (STEMI) in China had not changed within 10 years since 2001 despite rapid progresses in reperfusion therapy. China still faces challenges in providing optimal and equitable management strategies for all patients across the nation because of the broad geography and unbalanced economic development. In addition, disparate access to medical care may also lead to variations in AMI care provision, treatment patterns, and outcomes.
The major public medical system in China follows a traditional structure based on vertically administrative models of province, prefecture, and county in the order of decreasing size and level. The China AMI (CAMI) registry is a prospective, nationwide, multicenter, observational study for AMI care in these 3 levels of hospitals. The present cross-sectional study investigates the variations in care and outcomes of patients with STEMI among the 3 levels of hospitals in China.
Methods
Overview of CAMI Registry and Study Population
This study was approved by the institutional review board central committee at Fuwai Hospital. Written informed consent was obtained from eligible patients. This report follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.
The design of the CAMI registry was described previously.13 Briefly, 108 hospitals from 31 provinces and municipalities throughout mainland China have participated in the registry since January 2013 (eAppendix 1 in the Supplement). These hospitals included 31 province-level hospitals, 45 prefecture-level hospitals in their own provinces or municipalities, and 32 county-level hospitals in these selected prefectures, with broad coverage of geographical regions, including urban and rural areas. These hospitals are the largest or central hospitals in their administrative areas. Province-level hospitals are all university-affiliated academic hospitals located in capital city of each province, prefecture-level hospitals are in medium-sized cities, and county-level hospitals are in the smallest cities, usually with surrounding rural areas. Staffing ratios of cardiologists and cardiothoracic surgeons are in decreasing order from province to prefecture to county levels. In province-level, prefecture-level, and county-level hospitals, the median bed numbers in cardiology units are 122, 83, and 47, respectively; 100%, 96%, and 78% of hospitals, respectively, have a cardiac-coronary care unit (CCU); and 100%, 93%, and 44% of hospitals, respectively, have a catheterization laboratory.13 The vertical administrative relationship of the 3 levels of hospitals reflects the hierarchical performance of the current medical care system (eFigure 1 in the Supplement), thus making hospital-level comparisons appropriate.
Patients with a primary diagnosis of AMI including STEMI and non-STEMI admitted to participating hospitals within 7 days after the onset of ischemic symptoms were consecutively enrolled into the registry. The final diagnosis had to meet the third Universal Definition for Myocardial Infarction, including types 1, 2, 3, 4b, and 4c. Type 4a and type 5 AMIs were not eligible for the CAMI registry.14
Data Collection and Management
Comprehensive collection of data, including patient demographic factors, risk factors, medical history, prehospital medical contact, presentation, status at admission, vital signs, reperfusion therapy and reasons for it, medications, procedures, and events, was conducted. All information was collected using a standardized set of variables and predefined, standard, unified definitions, systematic data entry and transmission procedures, and rigorous data quality control. Data were collected, validated, and submitted through a secure, web-based electronic data capture system. Enrollment, data collection, and follow-up were all performed by trained physicians at each participating site in a real-time manner, to ensure data accuracy and reliability. Senior cardiologists were responsible for the data quality control. Periodic database checking was undertaken. Hospital sites underwent random on-site audits for the accuracy of diagnosis and variables based on medical records.
Variables in Care and Outcomes
The key variable in care for patients with STEMI was reperfusion therapy, including primary percutaneous coronary intervention (PCI) or fibrinolysis. We analyzed the percentage of patients undergoing reperfusion therapy among all patients and among the eligible patients who presented within 12 hours after symptom onset. Coronary angiography, stent implantation, elective PCI, coronary artery bypass grafting, intra-aortic balloon pump use, and medications, including traditional Chinese medicines, used during hospitalization were also assessed. The primary outcome was in-hospital mortality. Other outcomes included the complication rates of heart failure, cardiogenic shock, mechanical complications, severe arrhythmias, reinfarction, cerebrovascular accident or stroke, and nonintracranial hemorrhage bleedings (detailed definitions are shown in eAppendix 2 in the Supplement).
Statistical Analysis
Patient characteristics, medical contact, treatments, and the rates of in-hospital outcomes were compared among the 3 levels of hospitals. Continuous variables were expressed by mean (SD) or median (interquartile range) and were compared by analysis of variance or the Kruskal-Wallis H test as appropriate. Categorical variables were expressed as percentages with 95% CIs, and comparison was performed with the χ2 test. We also performed the Cochran-Armitage trend test for the rates of in-hospital outcomes among the 3 levels of hospitals. Multivariable logistic regression models were used to examine the differences in the odds of in-hospital outcomes among the 3 levels of hospitals by adjusting for confounding variables. Models 1 to 6 were fitted by adjusting for patient characteristics, medical contact, clinical status at admission, hospital facilities, reperfusion therapy, medications, and intra-aortic balloon pump use during hospitalization, as shown in eAppendix 2 in the Supplement. Odds ratios (ORs) and 95% CIs were calculated. In addition, linear trend tests were conducted for the ORs of death, heart failure, and cardiogenic shock among the 3 levels of hospitals. In-hospital mortality among the 3 levels of hospitals was also compared across 2 subgroups by onset-to-admission time of 12 hours or less vs longer than 12 hours and by receipt of reperfusion therapy or not. Multivariable logistic regression models were also used for the assessment of associated factors with in-hospital mortality. All the variables were missing in fewer than 10% of all cases, and multivariable outcomes analyses were based on the complete data. We also used multiple imputations for baseline variables to perform logistic regression to assess the outcomes as sensitivity analysis. A 2-tailed P < .05 was considered significant. Statistical analyses were performed using SAS statistical software (version 9.4 for Windows, SAS Institute) from June 2015 to June 2019.
Results
Patients in the Analysis
Of 19 334 patients with acute STEMI registered in the CAMI registry from January 1, 2013, through September 30, 2014, we excluded 5816 patients who transferred in, 821 patients who transferred out, and 2 patients with missing transfer data, to obtain the real prehospital information and to eliminate referral bias in comparison of care and outcomes among the 3 levels of hospitals. Thus, 12 695 patients (9593 men [75.6%]; median [interquartile range] age, 63 [54-72] years) with direct admission formed the core cohort for the care analysis, with 3985 patients in province-level hospitals, 6731 patients in prefecture-level hospitals, and 1979 patients in county-level hospitals (Figure 1). Moreover, 12 659 patients were included in the in-hospital outcomes analysis after further exclusion of 36 patients because of missing data on death.
Figure 1. Study Cohort Flow Diagram.

AMI indicates acute myocardial infarction; NSTEMI, non–ST-segment elevation myocardial infarction; and STEMI, ST-segment elevation myocardial infarction.
Baseline Characteristics, Medical Contact, and Presentation
Compared with patients admitted to province-level hospitals, the patients admitted to prefecture-level and county-level hospitals were older (median [interquartile range] age, 61 [52-70] years vs 63 [54-72] years and 65 [57-75] years) and more likely to be women (815 women [20.5%] vs 1620 women [24.1%] and 667 women [33.7%]), but less likely to have obesity, diabetes, dyslipidemia, previous PCI, and peripheral arterial disease and to be current smokers (Table 1). Compared with patients in province-level hospitals, those in prefecture-level and county-level hospitals were significantly less likely to arrive at the hospital within 12 hours from symptom onset (75.3% [95% CI, 73.9%-76.6%] vs 70.8% [95% CI, 69.7%-71.9%] vs 69.8% [95% CI, 67.7%-71.8%]; P < .001), and they had lower rates of ambulance transportation use (19.4% [95% CI, 18.1%-20.7%] vs 11.6% [95% CI, 10.8%-12.4%] vs 12.0% [95% CI, 10.6%-13.5%]; P < .001). Overall, 72.0% of patients (9147 of 12 695 patients) arrived at the hospital within 12 hours after symptom onset, and 14.1% of patients (141 of 12 440 patients) used ambulances. More patients in county-level hospitals presented with heart failure, cardiogenic shock, cardiac arrest, and Killip class III or IV heart failure (Table 1 and eTable 1 and eTable 2 in the Supplement).
Table 1. Baseline Characteristics of Patients With ST-Segment Elevation Myocardial Infarction Among the 3 Levels of Hospitals.
| Characteristics | Patients, No./total No. (%) | P valuea | |||
|---|---|---|---|---|---|
| Total (N = 12 695) | Province level (n = 3985) | Prefecture level (n = 6731) | County level (n = 1979) | ||
| Age, median (IQR), y | 63 (54-72) | 61 (52-70) | 63 (54-72) | 65 (57-75) | <.001 |
| ≥75 y | 2270/12 510 (18.1) | 591/3945 (15.0) | 1219/6619 (18.4) | 460/1946 (23.6) | <.001 |
| Male | 9593/12 695 (75.6) | 3170/3985 (79.5) | 5111/6731 (75.9) | 1312/1979 (66.3) | <.001 |
| Risk factors and medical history | |||||
| Body mass index, mean (SD)b | 24.5 (10.7) | 25.1 (15.6) | 24.3 (8.4) | 23.7 (3.4) | <.001 |
| Body mass index ≥25 | 4282/12 049 (35.5) | 1516/3763 (40.3) | 2154/6388 (33.7) | 612/1898 (32.2) | <.001 |
| Current smoker | 5601/12 401 (45.2) | 1968/3849 (51.1) | 2856/6606 (43.2) | 777/1946 (39.9) | <.001 |
| Hypertension | 6040/12 225 (49.4) | 1926/3781 (50.9) | 3187/6547 (48.7) | 927/1897 (48.9) | .08 |
| Diabetes history | 2267/11 958 (19.0) | 789/3687 (21.4) | 1200/6446 (18.6) | 278/1825 (15.2) | <.001 |
| Known dyslipidemia | 789/10 792 (7.3) | 335/3291 (10.2) | 356/6011 (5.9) | 98/1490 (6.6) | <.001 |
| Prior myocardial infarction | 792/11 673 (6.8) | 234/3397 (6.9) | 446/6406 (7.0) | 112/1870 (6.0) | .31 |
| Prior percutaneous coronary intervention | 558/12 074 (4.6) | 220/3579 (6.1) | 287/6581 (4.4) | 51/1914 (2.7) | <.001 |
| Prior heart failure | 193/11 845 (1.6) | 54/3435 (1.6) | 97/6518 (1.5) | 42/1892 (2.2) | .10 |
| Prior stroke | 1094/11 970 (9.1) | 299/3484 (8.6) | 610/6555 (9.3) | 185/1931 (9.6) | .37 |
| Peripheral artery disease | 54/11 898 (0.5) | 22/3460 (0.6) | 30/6525 (0.5) | 2/1913 (0.1) | .01 |
| Presentation | |||||
| Means of transport | |||||
| Self or family | 10 551/12 440 (84.8) | 3081/3856 (79.9) | 5768/6616 (87.2) | 1702/1968 (86.5) | <.001 |
| Ambulance | 1748/12 440 (14.1) | 747/3856 (19.4) | 765/6616 (11.6) | 236/1968 (12.0) | |
| In-hospital | 141/12 440 (1.1) | 28/3856 (0.7) | 83/6616 (1.3) | 30/1968 (1.5) | |
| Onset-to-arrival time | |||||
| <3 h | 3903/12 695 (30.7) | 1153/3985 (28.9) | 2092/6731 (31.1) | 658/1979 (33.2) | <.001 |
| 3-12 h | 5244/12 695 (41.3) | 1847/3985 (46.3) | 2674/6731 (39.7) | 723/1979 (36.5) | |
| 13-24 h | 1098/12 695 (8.6) | 323/3985 (8.1) | 584/6731 (8.7) | 191/1979 (9.7) | |
| 1-7 d | 2343/12 695 (18.5) | 634/3985 (15.9) | 1322/6731 (19.6) | 387/1979 (19.6) | |
| Uncertain | 107/12 695 (0.8) | 28/3985 (0.7) | 59/6731 (0.9) | 20/1979 (1.0) | |
| Anterior myocardial infarction | 6511/12 467 (52.2) | 2014/3876 (52.0) | 3437/6620 (51.9) | 1060/1971 (53.8) | .32 |
| Heart failure at admission | 1695/12 347 (13.7) | 468/3824 (12.2) | 878/6574 (13.4) | 349/1949 (17.9) | <.001 |
| Cardiogenic shock at admission | 482/12 396 (3.9) | 107/3852 (2.8) | 246/6587 (3.7) | 129/1957 (6.6) | <.001 |
| Cardiac arrest | 175/12 429 (1.4) | 50/3861 (1.3) | 83/6602 (1.3) | 42/1966 (2.1) | .02 |
| Systolic blood pressure, median (IQR), mm Hg | 128 (110-144) | 128 (111-143) | 127 (110-144) | 130 (110-147) | .39 |
| Heart rate, median (IQR), beats/min | 76 (65-87) | 76 (66-86) | 76 (65-87) | 76 (65-90) | .005 |
| Killip class III or IV heart failure | 955/12 419 (7.7) | 231/3856 (6.0) | 538/6596 (8.2) | 186/1967 (9.4) | <.001 |
Abbreviation: IQR, interquartile range.
P values indicate between-hospital comparisons of baseline characteristics for patients with ST-segment elevation myocardial infarction among 3 levels of hospitals.
Body mass index is calculated as weight in kilograms divided by height in meters squared.
Reperfusion Therapy, Procedures, and Medications
Rates of reperfusion therapy in province-level hospitals were significantly higher than those in prefecture-level and county-level hospitals among all patients (69.4% [95% CI, 67.9%-70.8%] vs 54.3% [95% CI, 53.1%-55.5%] vs 45.8% [95% CI, 43.6%-48.1%]; P < .001; the rate of perfusion therapy for all patients was 57.5% [7123 of 12 363 patients]) and among the eligible patients admitted within 12 hours after symptom onset (88.6% [95% CI, 87.3%-89.8%] vs 80.1% [95% CI, 78.8%-81.3%] vs 72.6% [95% CI, 70.0%-75.2%]; P < .001). Rates of primary PCI at province-level hospitals were significantly higher than rates at prefecture-level and county-level hospitals among all patients (65.7% [95% CI, 64.2%-67.2%] vs 42.2% [95% CI, 41.0%-43.4%] vs 20.2% [95% CI, 18.4%-22.1%]; P < .001) and among eligible patients admitted within 12 hours after symptom onset (83.8% [95% CI, 82.4%-85.2%] vs 61.5% [95% CI, 60.0%-63.0%] vs 31.6% [95% CI, 29.0%-34.4%]; P < .001) (Table 2 and eTable 3 and eTable 4 in the Supplement). The reasons for not receiving reperfusion therapy included patients or family members refusing because of concerns about reperfusion-related complications, patient’s finances, physician’s decision, and unclear diagnosis (predominantly in lower-level hospitals) (eFigure 2 in the Supplement). Of note, time delays from admission to care were seen in the 3 levels of hospitals; 15.4% (95% CI, 6.9%-28.1%) of patients at province-level hospitals, 31.0% (95% CI, 26.6%-35.6%) of patients at prefecture-level hospitals, and 36.5% (95% CI, 30.6%-42.9%) of patients at county-level hospitals met the door-to-needle time goal of 30 minutes or less, and 32.7% (95% CI, 28.9%-36.6%) of patients at province-level hospitals, 41.5% (95% CI, 38.6%-44.5%) of patients at prefecture-level hospitals, and 29.7% (95% CI, 22.5%-37.8%) of patients at county-level hospitals met the door-to-balloon time goal of 90 minutes or less (eFigure 3 in the Supplement).
Table 2. Treatments for Patients With ST-Segment Elevation Myocardial Infarction in China and Among the 3 Levels of Hospitals.
| Treatments | Patients, No./total No. (%) | P valuea | |||
|---|---|---|---|---|---|
| Total (N = 12 695) | Province level (n = 3985) | Prefecture level (n = 6731) | County level (n = 1979) | ||
| Reperfusion therapy | |||||
| Among all the patients | 7123/12 363 (57.5) | 2653/3824 (69.4) | 3576/6589 (54.3) | 894/1950 (45.8) | <.001 |
| Primary PCI | 5691/12 363 (46.0) | 2514/3824 (65.7) | 2783/6589 (42.2) | 394/1950 (20.2) | |
| Fibrinolysis | 1419/12 363 (11.5) | 137/3824 (3.6) | 782/6589 (11.9) | 500/1950 (26) | |
| Among the eligible patients admitted within 12 h from onset | 6533/7982 (81.8) | 2379/2685 (88.6) | 3302/4124 (80.1) | 852/1173 (72.6) | <.001 |
| Primary PCI | 5159/7982 (64.6) | 2251/2685 (83.8) | 2537/4124 (61.5) | 371/1173 (31.6) | |
| Fibrinolysis | 1363/7982 (17.1) | 126/2685 (5.0) | 756/4124 (18.3) | 481/1173 (41.0) | |
| Door-to-balloon time, median (IQR), min | 113 (77-204) | 123 (80-255) | 109 (74-175) | 124 (85-277) | .17 |
| Door-to needle time, median (IQR), min | 52 (29-100) | 91 (45-187) | 54 (28-94) | 45 (30-100) | .15 |
| Procedure | |||||
| Coronary angiography | 7722/12 695 (60.8) | 2995/3985 (75.2) | 4091/6731 (60.8) | 636/1979 (32.1) | <.001 |
| Stent implantation in primary PCI | 4799/5594 (85.8) | 2171/2492 (87.1) | 2283/2711 (84.2) | 345/391 (88.2) | .004 |
| Drug-eluting stent | 4287/4755 (90.1) | 1838/2155 (85.2) | 2116/2260 (93.6) | 333/340 (97.9) | <.001 |
| Elective PCI | 2853/12 289 (23.2) | 753/3772 (20.0) | 1800/6575 (27.4) | 300/1942 (15.4) | <.001 |
| Coronary artery bypass graft | 53/12 456 (0.4) | 30/3842 (0.8) | 20/6642 (0.3) | 3/1972 (0.2) | <.001 |
| Intra-aortic balloon pump use | 395/12 276 (3.2) | 164/3806 (4.3) | 221/6538 (3.4) | 10/1932 (0.5) | <.001 |
| Medication during hospitalization | |||||
| Aspirin | 12 056/12 406 (97.2) | 3758/3852 (97.6) | 6425/6607 (97.2) | 1873/1947 (96.2) | .02 |
| P2Y12-receptor inhibitor | 11 977/12 318 (97.2) | 3754/3821 (98.2) | 6411/6557 (97.8) | 1812/1940 (93.4) | <.001 |
| Statin | 11 311/11 609 (97.4) | 3539/3603 (98.2) | 6047/6179 (97.9) | 1725/1827 (94.4) | <.001 |
| β-blocker | 8623/12 283 (70.2) | 2695/3806 (70.8) | 4623/6541 (70.7) | 1305/1936 (67.4) | .01 |
| Angiotensin-converting enzyme inhibitor or angiotensin receptor blocker | 7265/12 269 (59.2) | 2267/3795 (59.7) | 3807/6537 (58.2) | 1191/1937 (61.5) | .03 |
| Heparin or fondaparinux | 11 091/12 137 (91.4) | 3310/3758 (88.1) | 6016/6459 (93.1) | 1765/1920 (91.9) | <.001 |
| Glucoprotein IIb or IIIa inhibitor | 4175/11 963 (34.9) | 1773/3731 (47.5) | 2018/6326 (31.9) | 384/1906 (20.1) | <.001 |
| Traditional Chinese medicine | 1994/12 231 (16.3) | 520/3785 (13.7) | 1138/6510 (17.5) | 336/1936 (17.4) | <.001 |
| Length of stay, median (IQR), d | 10 (7-13) | 8 (6-11) | 11 (7-14) | 10 (7-14) | .44 |
Abbreviations: IQR, interquartile range; PCI, percutaneous coronary intervention.
P values indicate between-hospital comparisons of treatments for patients with STEMI among 3 levels of hospitals.
Intra-aortic balloon pump was more frequently used in province-level and prefecture-level hospitals than in county-level hospitals (4.3% [95% CI, 3.7%-5.0%] vs 3.4% [95% CI, 3.0%-3.8%] vs 0.5% [95% CI, 0.2%-0.9%]; P < .001), despite higher rates of cardiogenic shock at presentation in county-level hospitals. We noted minor differences in medication use among 3 levels of hospitals. The usage rates for aspirin, P2Y12- receptor inhibitor, and statins during hospitalization were all high (>90%) (Table 2).
In-Hospital Outcomes
There was a significant and progressive trend for higher in-hospital mortality among 3 levels of hospitals: 3.1% (95% CI, 2.6%-3.7%) in province-level hospitals, 5.3% (95% CI, 4.8%-5.9%) in prefecture-level hospitals, and 10.2% (95% CI, 8.9%-11.7%) in county-level hospitals (P for trend < .001) (Figure 2). The disparity persisted in the subsets of reperfusion therapy and onset-to-arrival time less than 12 h or not (eTable 5 and eTable 6 in the Supplement). After adjustment for patient characteristics and presentation, the odds of death was still significantly higher in prefecture-level (adjusted OR, 1.47; 95% CI, 1.14-1.89) and county-level (adjusted OR, 2.48; 95% CI, 1.85-3.31) hospitals compared with province-level hospitals (P < .001). After further adjustment for hospital facility and treatments, the odds of death in the 2 lower levels of hospitals were attenuated but still higher than the odds in province-level hospitals (OR, 1.39 [95% CI, 1.06-1.84] for prefecture-level hospitals and 1.43 [95% CI, 0.97-2.11] for county-level hospitals; P for trend = .04). Similar results were obtained in sensitivity analysis of multiple imputation (adjusted OR, 1.55 [95% CI, 1.23-1.95] for prefecture-level hospitals and 1.87 [95% CI, 1.36-2.56] for county-level hospitals; P < .001) (Figure 3 and eTable 7 and eTable 8 in the Supplement). Receiving treatment at the 2 lower levels of hospitals was associated with in-hospital death, but the availability of a CCU and catheterization laboratory in the hospital were protective factors against in-hospital death (eTable 9 and eTable 10 in the Supplement). Similar variations were also seen in the odds of heart failure and cardiogenic shock (Figure 3 and eTable 7 and eTable 8 in the Supplement).
Figure 2. Incidence of In-Hospital Outcomes in Patients With ST-Segment Elevation Myocardial Infarction at the 3 Levels of Hospitals in China.
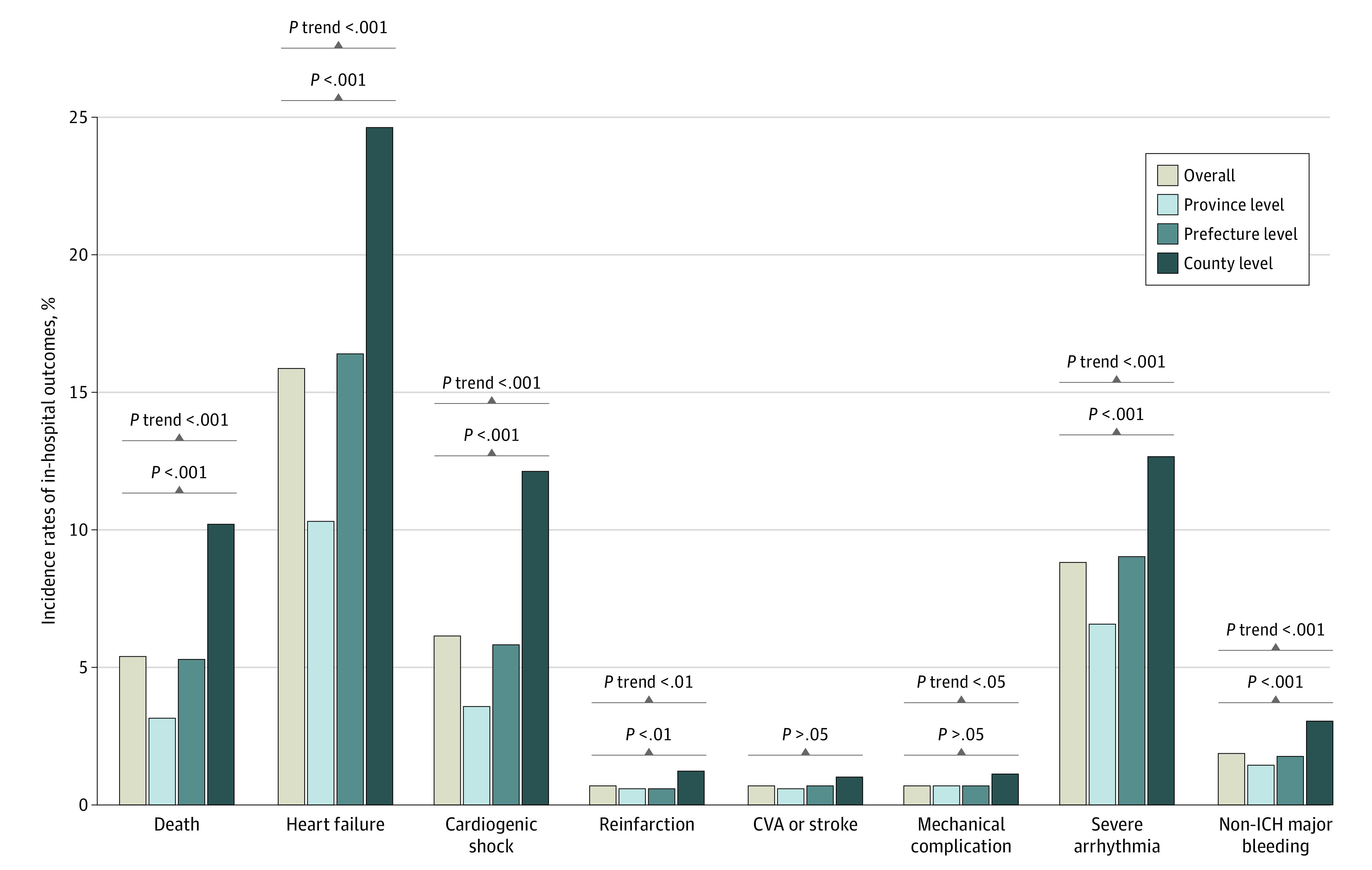
CVA indicates cerebrovascular accident; and ICH, intracranial hemorrhage.
Figure 3. Risk-Adjusted In-Hospital Outcomes Among Patients With ST-Segment Elevation Myocardial Infarction at the 3 Levels of Hospitals in China.

Adjustment variables include age, sex, hypertension, diabetes, prior myocardial infarction, prior heart failure, onset-to-arrival time, means of transport, anterior-wall infarction, systolic blood pressure at admission, heart rate at admission, cardiogenic shock at admission, heart failure at admission, cardiac arrest before or at admission, Killip class of heart failure, coronary care unit, coronary catheter laboratory availability, reperfusion therapy, aspirin, P2Y12- receptor inhibitor, statin, β-blocker, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker, and intra-aortic balloon pump use during hospitalization. OR indicates odds ratio.
Discussion
Gaps and variations in care and outcomes for patients with STEMI exist within and across countries in the world, particularly between developed and developing countries.1,3,15,16,17,18,19,20 The broad geography, unbalanced economy, and varying medical service capabilities across China make the disparities even greater. The present study has several important findings. First, the prehospital delay of patients with STEMI was common and prominent, with a low ambulance use rate of only 14.1% overall. Second, the rates of reperfusion therapy, especially primary PCI, were much lower in the prefecture-level and county-level hospitals compared with the province-level hospitals. The in-hospital delay of reperfusion therapy was also obvious, with only approximately one-third reaching the time goals. Third, there existed great disparity in the in-hospital mortality rates among the 3 levels of hospitals, with a rate of 10.2% in county-level hospitals, which is 3-fold higher than the 3.1% rate in province-level hospitals. Hospital facility and reperfusion therapy partly explained hospital-level variation in mortality. To our knowledge, this is the first national report on the hospital-level differences in medical care and outcomes for patients with STEMI in China, and it reveals the gaps and challenges that China is facing. These findings establish the fundamental current status in care and outcomes of STEMI and serve as a basis to guide efforts on quality improvement in STEMI care and allocation of resources.
We selected a diverse group of 3 levels of major public hospitals in all provinces and municipalities throughout mainland China, thus making the study representative of status in the ways to seek medical care, the performance of care with the facilities for reperfusion therapy, and the outcomes of AMI in China. The facilities for AMI care are unbalanced across the 3 levels of hospitals. This prospective national registry provided a unique opportunity to evaluate the differences in prehospital contact, treatment strategies and causes, and outcomes of patients among the 3 levels of hospitals.
The CAMI registry enrolled patients with AMI admitted within 7 days from symptom onset, which is unique and different from the criterion of admission within 24 or 72 hours of symptom onset used in acute coronary syndrome registries of other countries.21,22 We observed the long prehospital delay and inefficient systems for first medical contact. A high proportion of patients with STEMI went to the hospital late, with only 72.0% presenting to the hospital within 12 hours from symptom onset, whereas more than 90% of such patients present to the hospital within 12 hours from symptom onset in the US.23 Moreover, ambulance transportation was used for only 19.4% of patients in provincial cities, 11.6% of patients in prefectures, and 12.0% of patients in counties, whereas 60% to 70% of patients in the US, Canada, the UK, and Japan and 50% of patients in Singapore use ambulances.24,25,26,27,28,29 The possible reasons for this are thought to be mainly patients’ being unaware of their AMI and lack of information on EMSs’ performance. Furthermore, EMSs are still underdeveloped and inconvenient in China, especially in rural and remote areas. Socioeconomic status was associated with a number of prehospital clinical, access-related, and transport variables that are associated with outcomes for patients with STEMI.28
Another important finding showed that the rate of early reperfusion therapy was markedly low (57.5% of all patients), which is lower than the rates of 71% in Sweden and 77% in the UK, but similar to the rates of 56% in Brazil and 53.9% in India.1,16,21 Among eligible patients who arrived at the hospital within 12 hours of symptom onset, 88.6%, 80.1%, and 72.6% of patients received reperfusion therapy in province-level, prefecture-level, and county-level hospitals, respectively, whereas the corresponding rates in the US are 96%, 94%, and 83% in the top, median, and bottom performing hospitals, respectively.22 The reasons for not receiving reperfusion therapy among the eligible patients mainly included patient factors (eg, concern about the safety of reperfusion or affordability) and physician factors (eg, diagnostic dilemma and clinical experience). Moreover, primary PCI, which is regarded as a more effective strategy in reperfusion therapy for STEMI, was used for most patients receiving reperfusion in province-level hospitals, whereas it was used much less frequently in county-level hospitals.
The most important finding in our study revealed that significant variation in the in-hospital mortality rate was observed for patients with STEMI in China, with the highest rate of 10.2% in county-level hospitals and the lowest rate of 3.1% in province-level hospitals. The remarkable, nearly 3-fold difference in mortality rate persisted in the subsets of patients stratified by presentation delay and reperfusion therapy. The higher mortality rate in county-level hospitals was associated with patients being in more critical condition, lower use of reperfusion therapy, and lack of advanced hospital facilities, such as CCUs and catheterization laboratories. Moreover, the odds of in-hospital death remained higher even after adjustment for these factors, implying that other immeasurable factors, such as insufficient capabilities in clinical expertise, also likely contribute to the much higher mortality in lower level hospitals.
For addressing the current gaps in the care of patients with STEMI especially in low-level hospitals in China as in other developing countries, efforts should be focused on widespread access to timely reperfusion, which is a proven paradigm with the greatest potential to improve survival, especially in rural areas that have a very low density of hospitals and limited resources.30,31,32,33 Fibrinolytic therapy is still encouraged in low-level hospitals or remote areas where primary PCI is less feasible. The establishment and staffing of CCUs and catheterization laboratories to provide the basic facilities are essential for addressing the prominent gaps.34 Moreover, officers and administrators from both government and hospital aspects should make more efforts to optimize the processes of reperfusion therapy for reducing in-hospital time delay.35 Intensive training and technical support for physicians and interventional cardiologists in the low-level hospitals should be implemented as well. In addition, more efforts should be made to educate residents about awareness of and prompt response to ischemic symptoms, and convenient and efficient EMS transportation for shortening prehospital delay should be made available. The EMSs should be strengthened to develop regional medical combination networks, which can improve patient prognosis independently of health care setting or geographical locations. The EMS-based strategy of transporting patients to existing PCI-capable hospitals is less costly and more effective than hospital expansion options.23,25,36,37 These insights provide implications for China as well as other developing countries as a world opportunity to narrow gaps and variations in the care and outcomes of patients with AMI. We can reference the evidence-based approaches such as the Acute Coronary Treatment and Intervention Outcomes Network38 and the Accelerator Project39 and develop useful and more effective models suitable for China for further practice and quality improvement.
Limitations
This study has limitations that should be addressed. The CAMI registry did not include all hospitals and could not capture all the patients with STEMI. However, we uniquely included the 3 levels of hospitals instead of binary urban-rural or tertiary-secondary hospitals, which is in accordance with Chinese administrative and governmental models and objectively reflects routine practice and performance of AMI care in the Chinese medical system. The possibility of unmeasured confounding factors that can be present in any observational study exists. However, we tried to limit the effect of this by hierarchical multivariable models with adjustment for confounding factors. The study is not able to determine all of the factors associated with in-hospital mortality. However, our models are as comprehensive as the registry allowed and included the variables in multiple facets of presentation and care, consistent with or more extensive than other established registries. The CAMI registry enrolled patients admitted to the hospital but did not include outpatients. We analyzed the in-hospital mortality of patients with STEMI but could not assess out-of-hospital deaths.
Conclusions
This cross-sectional study shows that there are significant variations in STEMI presentation, treatment patterns, and in-hospital outcomes among the 3 levels of hospitals in China. Multipronged and systematic efforts for quality improvement with the aim of delivering equitable management across all national hospitals from time of admission through to discharge and beyond are essential in a developing country with large population, limited resources, and large variation.
eAppendix 1. Full List of Hospitals in the China AMI Registry
eAppendix 2. Definitions of In-Hospital Clinical Events
eTable 1. Baseline Characteristics With 95% Confidence Intervals of Patients With STEMI Among the Three-Level Hospitals
eTable 2. Multicomparisons in Baseline Characteristics of Patients With STEMI Among the Three-Level Hospitals in China
eTable 3. Reperfusion Therapy and Medications During Hospitalization With 95% Confidence Intervals Among the Three-Level Hospitals
eTable 4. Multicomparisons in Reperfusion Therapy and Medications During Hospitalization Among the Three-Level Hospitals in China
eTable 5. In-Hospital Mortality of STEMI Patients Stratified by Subsets in China and Among the Three-Level Hospitals
eTable 6. Multicomparison in In-Hospital Mortality Among the Three-Level Hospitals
eTable 7. Adjusted In-Hospital Major Outcomes Risk Analysis in STEMI Patients Among the Three-Level Hospitals Based on Complete Data
eTable 8. Adjusted In-Hospital Major Outcomes Risk Analysis in STEMI Patients Among the Three-Level Hospitals Based on Multiple Imputation Data
eTable 9. Associated Factors With In-Hospital Mortality of STEMI Patients in China
eTable 10. Associated Factors With In-Hospital Mortality of STEMI Patients in China Based on Multiple Imputation Data
eFigure 1. Chinese Vertical Governmental and Administrative Model and the Three-Level Hospitals in the CAMI Registry
eFigure 2. Reasons for No Reperfusion Therapy Among the Eligible STEMI Patients Admitted Within 12 Hours From Symptom Onset in China and Among the Three-Level Hospitals
eFigure 3. Percentage of Patients With Door-to-Balloon Time ≤90 min and Door-To-Needle Time ≤30 min in Patients Who Received Primary Percutaneous Coronary Intervention and Fibrinolysis Respectively in China and Among Three-Level Hospitals
References
- 1.Zhou M, Wang H, Zeng X, et al. . Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394(10204):1145-1158. doi: 10.1016/S0140-6736(19)30427-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rosselló X, Huo Y, Pocock S, et al. . Global geographical variations in ST-segment elevation myocardial infarction management and post-discharge mortality. Int J Cardiol. 2017;245:27-34. doi: 10.1016/j.ijcard.2017.07.039 [DOI] [PubMed] [Google Scholar]
- 3.Finegold JA, Asaria P, Francis DP. Mortality from ischaemic heart disease by country, region, and age: statistics from World Health Organisation and United Nations. Int J Cardiol. 2013;168(2):934-945. doi: 10.1016/j.ijcard.2012.10.046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chung SC, Sundström J, Gale CP, et al. ; Swedish Web-System for Enhancement and Development of Evidence-Based Care in Heart Disease Evaluated According to Recommended Therapies/Register of Information and Knowledge about Swedish Heart Intensive care Admissions; National Institute for Cardiovascular Outcomes Research/Myocardial Ischaemia National Audit Project; Cardiovascular Disease Research Using Linked Bespoke Studies and Electronic Health Records . Comparison of hospital variation in acute myocardial infarction care and outcome between Sweden and United Kingdom: population based cohort study using nationwide clinical registries. BMJ. 2015;351:h3913. doi: 10.1136/bmj.h3913 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362(23):2155-2165. doi: 10.1056/NEJMoa0908610 [DOI] [PubMed] [Google Scholar]
- 6.Rogers WJ, Frederick PD, Stoehr E, et al. . Trends in presenting characteristics and hospital mortality among patients with ST elevation and non-ST elevation myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am Heart J. 2008;156(6):1026-1034. doi: 10.1016/j.ahj.2008.07.030 [DOI] [PubMed] [Google Scholar]
- 7.Smolina K, Wright FL, Rayner M, Goldacre MJ. Determinants of the decline in mortality from acute myocardial infarction in England between 2002 and 2010: linked national database study. BMJ. 2012;344:d8059. doi: 10.1136/bmj.d8059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Laribi S, Aouba A, Resche-Rigon M, et al. . Trends in death attributed to myocardial infarction, heart failure and pulmonary embolism in Europe and Canada over the last decade. QJM. 2014;107(10):813-820. doi: 10.1093/qjmed/hcu083 [DOI] [PubMed] [Google Scholar]
- 9.Szummer K, Wallentin L, Lindhagen L, et al. . Improved outcomes in patients with ST-elevation myocardial infarction during the last 20 years are related to implementation of evidence-based treatments: experiences from the SWEDEHEART registry 1995-2014. Eur Heart J. 2017;38(41):3056-3065. doi: 10.1093/eurheartj/ehx515 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Reed GW, Rossi JE, Cannon CP. Acute myocardial infarction. Lancet. 2017;389(10065):197-210. doi: 10.1016/S0140-6736(16)30677-8 [DOI] [PubMed] [Google Scholar]
- 11.Chang J, Liu X, Sun Y. Mortality due to acute myocardial infarction in China from 1987 to 2014: secular trends and age-period-cohort effects. Int J Cardiol. 2017;227:229-238. doi: 10.1016/j.ijcard.2016.11.130 [DOI] [PubMed] [Google Scholar]
- 12.Li J, Li X, Wang Q, et al. ; China PEACE Collaborative Group . ST-segment elevation myocardial infarction in China from 2001 to 2011 (the China PEACE-Retrospective Acute Myocardial Infarction Study): a retrospective analysis of hospital data. Lancet. 2015;385(9966):441-451. doi: 10.1016/S0140-6736(14)60921-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Xu H, Li W, Yang J, et al. ; CAMI Registry study group . The China Acute Myocardial Infarction (CAMI) Registry: a national long-term registry-research-education integrated platform for exploring acute myocardial infarction in China. Am Heart J. 2016;175:193-201.e3. doi: 10.1016/j.ahj.2015.04.014 [DOI] [PubMed] [Google Scholar]
- 14.Thygesen K, Alpert JS, Jaffe AS, et al. ; Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction . Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020-2035. doi: 10.1161/CIR.0b013e31826e1058 [DOI] [PubMed] [Google Scholar]
- 15.Eagle KA, Goodman SG, Avezum A, Budaj A, Sullivan CM, López-Sendón J; GRACE Investigators . Practice variation and missed opportunities for reperfusion in ST-segment-elevation myocardial infarction: findings from the Global Registry of Acute Coronary Events (GRACE). Lancet. 2002;359(9304):373-377. doi: 10.1016/S0140-6736(02)07595-5 [DOI] [PubMed] [Google Scholar]
- 16.Kristensen SD, Laut KG, Fajadet J, et al. ; European Association for Percutaneous Cardiovascular Interventions . Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: current status in 37 ESC countries. Eur Heart J. 2014;35(29):1957-1970. doi: 10.1093/eurheartj/eht529 [DOI] [PubMed] [Google Scholar]
- 17.Cui Y, Hao K, Takahashi J, et al. . Age-specific trends in the incidence and in-hospital mortality of acute myocardial infarction over 30 years in Japan: report from the Miyagi AMI Registry Study. Circ J. 2017;81(4):520-528. doi: 10.1253/circj.CJ-16-0799 [DOI] [PubMed] [Google Scholar]
- 18.Schmidt M, Jacobsen JB, Lash TL, Bøtker HE, Sørensen HT. 25 Year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: a Danish nationwide cohort study. BMJ. 2012;344:e356. doi: 10.1136/bmj.e356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dégano IR, Salomaa V, Veronesi G, et al. ; Acute Myocardial Infarction Trends in Europe (AMITIE) Study Investigators . Twenty-five-year trends in myocardial infarction attack and mortality rates, and case-fatality, in six European populations. Heart. 2015;101(17):1413-1421. doi: 10.1136/heartjnl-2014-307310 [DOI] [PubMed] [Google Scholar]
- 20.Lee CH, Cheng CL, Yang YH, et al. . Trends in the incidence and management of acute myocardial infarction from 1999 to 2008: get with the guidelines performance measures in Taiwan. J Am Heart Assoc. 2014;3(4):e001066. doi: 10.1161/JAHA.114.001066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chung SC, Gedeborg R, Nicholas O, et al. . Acute myocardial infarction: a comparison of short-term survival in national outcome registries in Sweden and the UK. Lancet. 2014;383(9925):1305-1312. doi: 10.1016/S0140-6736(13)62070-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Peterson ED, Roe MT, Chen AY, et al. . The NCDR ACTION Registry-GWTG: transforming contemporary acute myocardial infarction clinical care. Heart. 2010;96(22):1798-1802. doi: 10.1136/hrt.2010.200261 [DOI] [PubMed] [Google Scholar]
- 23.Jollis JG, Al-Khalidi HR, Monk L, et al. ; Regional Approach to Cardiovascular Emergencies (RACE) Investigators . Expansion of a regional ST-segment-elevation myocardial infarction system to an entire state. Circulation. 2012;126(2):189-195. doi: 10.1161/CIRCULATIONAHA.111.068049 [DOI] [PubMed] [Google Scholar]
- 24.Boothroyd LJ, Lambert LJ, Segal E, et al. . Comparison of outcomes of ambulance users and nonusers in ST elevation myocardial infarction. Am J Cardiol. 2014;114(9):1289-1294. doi: 10.1016/j.amjcard.2014.07.060 [DOI] [PubMed] [Google Scholar]
- 25.Mathews R, Peterson ED, Li S, et al. . Use of emergency medical service transport among patients with ST-segment-elevation myocardial infarction: findings from the National Cardiovascular Data Registry Acute Coronary Treatment Intervention Outcomes Network Registry-Get With The Guidelines. Circulation. 2011;124(2):154-163. doi: 10.1161/CIRCULATIONAHA.110.002345 [DOI] [PubMed] [Google Scholar]
- 26.Ho AF, Loy EY, Pek PP, et al. . Emergency medical services utilization among patients with ST-segment elevation myocardial infarction: observations from the Singapore Myocardial Infarction Registry. Prehosp Emerg Care. 2016;20(4):454-461. doi: 10.3109/10903127.2015.1128032 [DOI] [PubMed] [Google Scholar]
- 27.Quinn T, Johnsen S, Gale CP, et al. ; Myocardial Ischaemia National Audit Project (MINAP) Steering Group . Effects of prehospital 12-lead ECG on processes of care and mortality in acute coronary syndrome: a linked cohort study from the Myocardial Ischaemia National Audit Project. Heart. 2014;100(12):944-950. doi: 10.1136/heartjnl-2013-304599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Agarwal S, Garg A, Parashar A, Jaber WA, Menon V. Outcomes and resource utilization in ST-elevation myocardial infarction in the United States: evidence for socioeconomic disparities. J Am Heart Assoc. 2014;3(6):e001057. doi: 10.1161/JAHA.114.001057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Takii T, Yasuda S, Takahashi J, et al. ; MIYAGI-AMI Study Investigators . Trends in acute myocardial infarction incidence and mortality over 30 years in Japan: report from the MIYAGI-AMI Registry Study. Circ J. 2010;74(1):93-100. doi: 10.1253/circj.CJ-09-0619 [DOI] [PubMed] [Google Scholar]
- 30.Wu Y, Li S, Patel A, et al. ; CPACS-3 Investigators . Effect of a quality of care improvement initiative in patients with acute coronary syndrome in resource-constrained hospitals in China: a randomized clinical trial. JAMA Cardiol. 2019;4(5):418-427. doi: 10.1001/jamacardio.2019.0897 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.[No authors listed.] STEMI in India. Eur Heart J. 2016;37(31):2449-2453. doi: 10.1093/eurheartj/ehw279 [DOI] [PubMed] [Google Scholar]
- 32.Baena CP, Chowdhury R, Schio NA, et al. . Ischaemic heart disease deaths in Brazil: current trends, regional disparities and future projections. Heart. 2013;99(18):1359-1364. doi: 10.1136/heartjnl-2013-303617 [DOI] [PubMed] [Google Scholar]
- 33.N’Guetta R, Yao H, Ekou A, et al. . Prevalence and characteristics of acute coronary syndromes in a sub-Saharan Africa population [in French]. Ann Cardiol Angeiol (Paris). 2016;65(2):59-63. [DOI] [PubMed] [Google Scholar]
- 34.Kirtane AJ, Stone GW. STEMI care in China: a world opportunity. Lancet. 2015;385(9966):400-401. doi: 10.1016/S0140-6736(14)61033-3 [DOI] [PubMed] [Google Scholar]
- 35.Song L, Yan H, Zhao H, et al. . Improvement in door-to-balloon times in patients with ST-elevation myocardial infarction at a large urban teaching hospital in China. Int J Cardiol. 2011;153(1):81-82. doi: 10.1016/j.ijcard.2011.08.068 [DOI] [PubMed] [Google Scholar]
- 36.Yan JC, Yan Y, Wang CP, Xu LJ, Liang Y. A new cooperative approach for ST-elevation myocardial infarction patients to receive timely and effective percutaneous coronary reperfusion in China. J Geriatr Cardiol. 2016;13(7):602-607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Concannon TW, Kent DM, Normand SL, et al. . Comparative effectiveness of ST-segment-elevation myocardial infarction regionalization strategies. Circ Cardiovasc Qual Outcomes. 2010;3(5):506-513. doi: 10.1161/CIRCOUTCOMES.109.908541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Peterson ED, Roe MT, Rumsfeld JS, et al. . A call to ACTION (Acute Coronary Treatment and Intervention Outcomes Network): a national effort to promote timely clinical feedback and support continuous quality improvement for acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2009;2(5):491-499. doi: 10.1161/CIRCOUTCOMES.108.847145 [DOI] [PubMed] [Google Scholar]
- 39.Jollis JG, Al-Khalidi HR, Roettig ML, et al. . Impact of regionalization of ST-segment-elevation myocardial infarction care on treatment times and outcomes for emergency medical services-transported patients presenting to hospitals with percutaneous coronary intervention: mission—Lifeline Accelerator-2. Circulation. 2018;137(4):376-387. doi: 10.1161/CIRCULATIONAHA.117.032446 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix 1. Full List of Hospitals in the China AMI Registry
eAppendix 2. Definitions of In-Hospital Clinical Events
eTable 1. Baseline Characteristics With 95% Confidence Intervals of Patients With STEMI Among the Three-Level Hospitals
eTable 2. Multicomparisons in Baseline Characteristics of Patients With STEMI Among the Three-Level Hospitals in China
eTable 3. Reperfusion Therapy and Medications During Hospitalization With 95% Confidence Intervals Among the Three-Level Hospitals
eTable 4. Multicomparisons in Reperfusion Therapy and Medications During Hospitalization Among the Three-Level Hospitals in China
eTable 5. In-Hospital Mortality of STEMI Patients Stratified by Subsets in China and Among the Three-Level Hospitals
eTable 6. Multicomparison in In-Hospital Mortality Among the Three-Level Hospitals
eTable 7. Adjusted In-Hospital Major Outcomes Risk Analysis in STEMI Patients Among the Three-Level Hospitals Based on Complete Data
eTable 8. Adjusted In-Hospital Major Outcomes Risk Analysis in STEMI Patients Among the Three-Level Hospitals Based on Multiple Imputation Data
eTable 9. Associated Factors With In-Hospital Mortality of STEMI Patients in China
eTable 10. Associated Factors With In-Hospital Mortality of STEMI Patients in China Based on Multiple Imputation Data
eFigure 1. Chinese Vertical Governmental and Administrative Model and the Three-Level Hospitals in the CAMI Registry
eFigure 2. Reasons for No Reperfusion Therapy Among the Eligible STEMI Patients Admitted Within 12 Hours From Symptom Onset in China and Among the Three-Level Hospitals
eFigure 3. Percentage of Patients With Door-to-Balloon Time ≤90 min and Door-To-Needle Time ≤30 min in Patients Who Received Primary Percutaneous Coronary Intervention and Fibrinolysis Respectively in China and Among Three-Level Hospitals