

Introduction
Several studies have reported successful atrial fibrillation (AF) ablation with the help of intracardiac echocardiography (ICE) using different techniques in patients with dextrocardia with situs inversus (1-3). However, ICE may not always be available, as that observed in the present study. We successfully performed AF and atrial flutter (Afl) ablation in our patient using a 180° mirror image and performed catheter manipulations in the opposite manner as that of usual maneuvers. To the best our knowledge, this is the first report that presents both AF and Afl ablations in the same session in a patient with dextrocardia with situs inversus.
Case Report
A 50-year-old man with dextrocardia with situs inversus was admitted for symptomatic, drug-refractory paroxysmal AF attacks that were persistent for 2.5 years (Fig. 1). After obtaining written informed consent, the patient was transferred to the catheter laboratory for AF ablation. At the beginning of the procedure, we changed the setting of the angiographic system (Artis zee, Siemens, Healthineers, Muenchen, Germany) and achieved a 180° mirror image. Thereafter, we inserted a 6-F decapolar catheter (St. Jude Medical) into the coronary sinus (CS) via the right internal jugular vein. We made a single transseptal (TS) puncture from the right femoral vein using a TS needle (BRK-1™, St. Jude Medical) through a 8.5-F TS sheath (SL0, St. Jude Medical). We performed the TS puncture in the opposite manner as that of usual catheter maneuvers in the same orientation as the normal fluoroscopic images. We directed the whole system medially and posteriorly by pointing the needle tip to the 10–11 o’clock position at the patient’s leg in the anteroposterior view (a usual TS puncture requires a needle orientation at the 4–5 o’clock direction) (4). The interatrial septum was punctured by advancing the needle in the left anterior oblique view. Additionally, the TS sheath was replaced with a 12-F steerable sheath (FlexCath Advance, Medtronic Inc.) over the wire.
Figure 1.

(a) Chest X-ray and (b) computed tomography images of the patient with dextrocardia with situs inversus
A second-generation 28-mm cryoballoon (CB) catheter (Arctic Front©, Medtronic CryoCath LP, Kirkland, Canada) was inserted into the left atrium (LA) and a spiral catheter (Achieve Advance™ mapping catheter 20 mm, Medtronic) was used both to maneuver the CB into the pulmonary vein (PV) and to record the PV signals. After entering the targeted PV with the spiral catheter, the balloon was inflated in the LA and directed to the PV ostium. An intravenous contrast material was injected through the central lumen of the balloon to confirm the complete closure of the PV ostium. A 180-s freeze cycle was performed for each vein (Fig. 2). If PV isolation was not achieved within 60 s after freezing, then the cycle was applied for additional 120 s. The diaphragmatic contraction was manually monitored for all the PVs using intermittent fluoroscopic imaging by pacing with another 6-F decapolar catheter (St. Jude Medical) placed in the superior vena cava and right subclavian vein. Electrical isolation of the anatomical right inferior PV required additional application of the freezing cycle, whereas the other veins were isolated with a single freezing cycle. Finally, all the PVs were isolated.
Figure 2.

(a) The mirror image of X-ray fluoroscopy in the left oblique projection. Achieve and cryoballoon catheters were placed in the anatomical RSPV; (b) intracardiac and surface electrography recordings obtained during PV isolation
RSPV - right superior pulmonary vein
Another instance of tachycardia was recorded during pacing from the CS to analyze the entrance block. The entrainment maneuvers revealed that it was a typical cavotricuspid isthmus (CTI)–dependent Afl. Linear ablation was performed in the CTI using an irrigated-type catheter (TactiCath™, St. Jude Medical) with the help of a three-dimensional system (EnSite Precision™ Cardiac Mapping System, St. Jude Medical) (Fig. 3). After ablation, the presence of a bidirectional block was demonstrated in the CTI. Again, we used a 180° mirror image for CTI ablation and performed catheter manipulations in the opposite manner as that of usual maneuvers.
Figure 3.
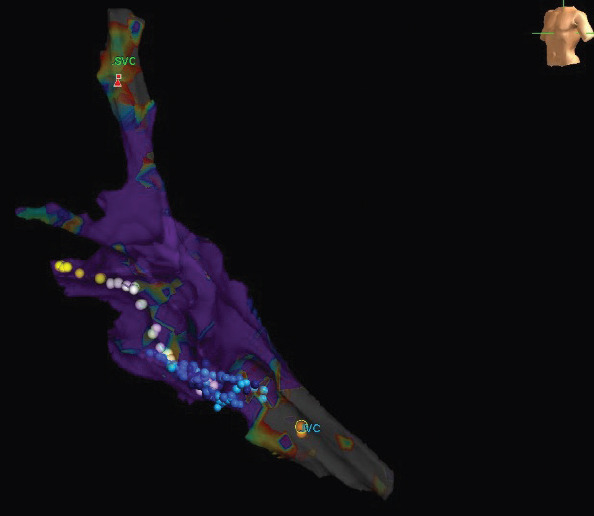
Three-dimensional electroanatomic view from the left anterior oblique projection. Blue dots indicate the linear ablation line in the cavotricuspid isthmus, yellow dots indicate the His region, and white dots indicate the tricuspid annulus
The total fluoroscopic time and total procedural time were longer in our patient because both AF ablation and CTI ablation were involved (48 and 150 min, respectively). No complications were recorded during or after the procedure. At the 6-month follow-up, the patient demonstrated a sinus rhythm without any antiarrhythmic drugs.
Discussion
The present study describes the case of a patient with dextrocardia with situs inversus who was scheduled to undergo AF and Afl ablations in the same procedure. Importantly, we used the mirror image of X-ray fluoroscopy and performed catheter manipulations in the opposite manner as that of usual maneuvers for both the ablations.
The frequency of dextrocardia with situs inversus has been reported to be 1–2 cases in 20,000 people of the general population (5). The orientation of fluoroscopic image may be confusing in patients with dextrocardia. Previous studies have reported cases of successful PV isolation with CB or radiofrequency ablation in patients with dextrocardia with situs inversus (1-3, 6). In these cases, ICE was used to assist TS puncture and PV isolation. The use of ICE, particularly in patients with a complex anatomy, facilitates the procedure and reduces the risk of complications (1-3). Three-dimensional mapping systems in combination with ICE have also been employed to assist PV isolation (1-3, 6).
The mirror image approach provides the same orientation as the normal one. However, it should be kept in mind that catheter manipulations should be performed in the opposite direction. Miyauchi et al. (2) have described a case of hot balloon ablation in a patient with paroxysmal AF with complete situs inversus with the help of a mirror image; they performed the procedure under the guidance of ICE. However, ICE may not always be available. The use of a 180° mirror image facilitates orientation in patients with dextrocardia with situs inversus.
Conclusion
In conclusion, the present study demonstrated that AF and Afl ablations can be safely performed by obtaining a mirror image without using ICE. However, if available, ICE would be an appropriate approach to guide the procedure in patients with dextrocardia with situs inversus. More importantly, the catheter manipulations must be performed in the opposite manner as that of the normal maneuvers.
Footnotes
Informed consent: The patient gave written informed consent for the scientific use of the images.
References
- 1.Yoshiga Y, Shimizu A, Ueyama T, Ono M, Fumimoto T, Ishiguchi H, et al. Successful cryoballoon pulmonary vein isolation in a patient with situs inversus and dextrocardia. J Arrhythm. 2016;32:493–5. doi: 10.1016/j.joa.2016.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Miyauchi S, Nakano Y, Ikeuchi Y, Okamura S, Okubo Y, Hironobe N, et al. HotBalloon ablation of atrial fibrillation in patients with dextrocardia and situs inversus by “mirror image”approach. J Arrhythm. 2019;35:855–7. doi: 10.1002/joa3.12240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Meulet J, Trim G, Hunt B, Lim KT, James A, Henry A, et al. Radiofrequency Pulmonary Vein Isolation in a Patient with Dextrocardia With Situs Inversus Totalis. Heart Lung Circ. 2017;26:e33–6. doi: 10.1016/j.hlc.2016.10.003. [DOI] [PubMed] [Google Scholar]
- 4.Manolis AS. Transseptal Access to the Left Atrium:Tips and Tricks to Keep it Safe Derived from Single Operator Experience and Review of the Literature. Curr Cardiol Rev. 2017;13:305–18. doi: 10.2174/1573403X13666170927122036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Maldjian PD. Diagnostic imaging approach to dextrocardia:self-assessment module. AJR Am J Roentgenol. 2007;188(6 Suppl):S35–8. doi: 10.2214/AJR.07.0192. [DOI] [PubMed] [Google Scholar]
- 6.Gromyko GA, Mihaylichenko SU, Novichkov SA, Mangutov DA, Kranin DL, Krukov EV. Pulmonary Vein Isolation for Treatment of Paroxysmal Atrial Fibrillation on Patient with Situs Inversus Totalis. J Atr Fibrillation. 2017;10:1609. doi: 10.4022/jafib.1609. [DOI] [PMC free article] [PubMed] [Google Scholar]