

Abstract
Aim and objective
The present report aims to present a case of delayed eruption of permanent maxillary central incisors in an 11-year-old male child due to the presence of two supernumerary teeth in anterior maxilla.
Case description
In this case, clinical and radiographic assessment revealed the presence of two supernumerary teeth palatal to unerupted maxillary permanent central incisors. These teeth were removed surgically under local anesthesia and were diagnosed as supplemental incisor, and the other appeared like tuberculate with dens invaginatus.
Conclusion
The permanent incisors erupted spontaneously within 6 months follow-up after extraction of the two supernumerary teeth without any orthodontic interception.
How to cite this article
Alsweed AA, Al-sughier Z. Surgical Management of Unerupted Permanent Maxillary Central Incisors Due to Presence of Two Supernumerary Teeth. Int J Clin Pediatr Dent 2020;13(4):421–424.
Keywords: Delayed eruption, Maxillary incisor, Supernumerary teeth
Introduction
The eruption of permanent maxillary central incisors teeth can be considered delayed when contralateral incisor has erupted more than 6 months previously, or eruption of lower incisors has occurred more than 1 year before and the upper incisors remain unerupted or the eruption sequence deviates significantly from the normal, as lateral incisors erupt ahead of central incisors.1 Delayed eruption of maxillary permanent incisor teeth usually occurs in the early mixed dentition and is often observed at age of 7–9 years.2 In the literature, there are many causes of delayed eruption of permanent maxillary incisors such as supernumerary teeth, dilacerated incisors after trauma to primary incisors, pathological obstructions in the incisor path of eruption, prolonged retention of primary incisors that become ankylosed, mucosal barrier in the eruptive path, tooth agenesis, abnormal morphology, association with particular syndromes, and inadequate space in the dental arch.3 The presence of supernumerary teeth is the most common cause of delayed eruption of maxillary permanent incisors, and their early diagnosis through clinical and radiographic examinations is essential.4 In the dental literature, it has been reported that the prevalence of supernumerary teeth in general population ranges from 0.1 to 3.8%.5 Supernumerary teeth can be categorized according to their position in the dental arch as mesiodens, paramolar, and distomolar or according to their shape as conical, tuberculate, supplemental molariform, and odontome.6 In the anterior maxilla, supplemental maxillary incisors are the least common type than conical or tuberculate supernumerary teeth. Besides, among the supplemental incisors, the central incisors are the least common one.7 There are many complications that might occur as a result of the presence of supernumerary teeth such as delayed eruption, diastema, crowding, spacing, impaction, malposition of the adjacent tooth bud, and rotation of the adjacent tooth.8 Therefore, avoidance of such complications is best achieved through early detection and management.
The present report aims to present a case of delayed eruption of permanent maxillary central incisors in a child due to the presence of two supernumerary teeth in anterior maxilla.
Case Description
An 11-year-old boy presented to the pediatric dental clinic of Qassim University, Saudi Arabia, complaining from delayed eruption of his upper anterior teeth. The patient appeared healthy, and his medical and family histories were nonrelevant. There was no dental history of past trauma to primary incisor teeth. Intraoral examination revealed good oral health, class I occlusion, all permanent teeth were erupted except the upper central incisors, incisal edge of one supernumerary tooth was evident palatally to unerupted upper right central incisor, and a labial palpable bulge was found in the unerupted incisors area (Fig. 1). An orthopantogram and periapical radiograph showed almost complete maturation of the incisors’ root and presence of two dense opaque masses palatal to the unerupted maxillary permanent central incisors that were provisionally diagnosed as supernumerary teeth (Figs 2 and 3).
Fig. 1.

Intraoral view showing the missing permanent central incisors, partially erupted supernumerary tooth in left maxillary permanent incisor position, bugle above the incisor area
Fig. 2.
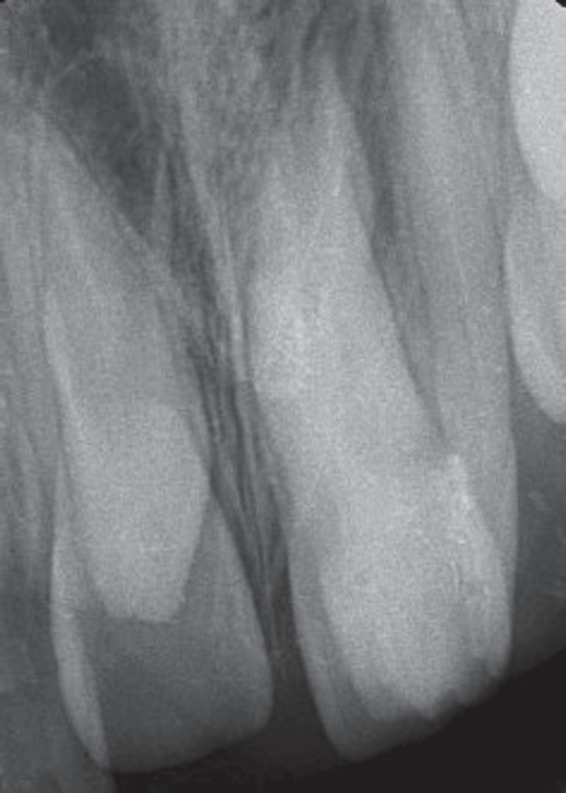
Periapical radiograph shows two supernumerary teeth above two impacted maxillary permanent central incisors
Fig. 3.

Panoramic radiograph showing the impacted maxillary permanent central incisors with two supernumerary teeth
Immediate surgical extraction of the supernumerary teeth was planned, as initial treatment to promote spontaneous eruption of the maxillary permanent central incisors, patient and his parent were notified, and explained the need of this procedure with written informed consent obtained from the child's parent. Under local anesthesia, a full-thickness mucoperiosteal flap was raised, and the supernumerary teeth were extracted without exposure of the unerupted incisors (Figs 4 and 5). Hemostasis was achieved, and the flap was repositioned (Fig. 6). Gross examination of the removed supernumerary teeth revealed that one resembled central incisor and was diagnosed as supplemental, while the other one had unusual crown and root morphology (multiple cusps in the crown, incomplete root development, deep pit on the palatal surface, greater buccopalatal dimension, and dilated root) and appeared like tuberculate supernumerary with dens invaginatus (Fig. 7). After a period of 6 months, clinical and radiographic examination showed that upper permanent incisors erupted on its own without any intervention (Figs 8 and 9). One-year follow-up showed advanced eruption progression of the upper permanent maxillary incisors (Figs 10 and 11).
Fig. 4.

Photograph shows the impacted supernumerary tooth after raising the buccal and palatal flap
Fig. 5.

Surgical site after extraction of erupted supernumerary teeth
Fig. 6.

Sutures in place
Fig. 7.

Extracted supernumerary teeth
Fig. 8.

Clinical photograph showing erupting maxillary central incisors after 6 months of the operation
Fig. 9.

Periapical radiograph 6 months postoperative showing the erupting two permeant maxillary central incisors
Fig. 10.

Clinical photograph showing erupting maxillary central incisors after 1 year of the operation
Fig. 11.

Periapical radiograph 1 year postoperatively showing the eruption of two permanent maxillary central incisors
Discussion
There is a considerable amount of literature on the management of unerupted maxillary incisors. Becker has recommended treatment order as space opening to encourage normal eruption process followed by surgical removal of obstruction and exposure of the unerupted tooth and finally orthodontic traction and alignment.9 There is controversy regarding the appropriate time for mesiodens removal. Mason et al. suggested that earlier removal of obstruction before maturity of adjacent incisor tooth increases the opportunity of spontaneous eruption, they observed spontaneous eruption of 72% of immature incisors have been occurred after early extraction of associated obstruction, while 63% of mature ones required further operation.10 On the other hand, Alacam and Bani advised late treatment after maturity of adjacent incisor to avoid damage to tooth apical area.11
The recent guidelines recommended the basics for the management of unerupted maxillary incisors is to get rid of the obstruction that might interfere with eruption and to provide enough space in the dental arch; other contributing factors include age of patient, medical history, compliance for treatment, etiology, and location of the delayed erupted incisor.12 Leyland et al., in a retrospective study, found that 49 to 91% of permanent maxillary incisors have been erupted spontaneously within 18 months after supernumerary tooth removal alone provided that there is adequate space available.13
According to the National clinical guidelines of Faculty of Dental Surgery, Royal College of Surgeons of England (FDSRCS), there are two approaches of treatment based on the child's age.12 A child under 9 years of age with an open apex permanent maxillary incisor has to be monitored for spontaneous eruption during 9–12 months after the extraction of supernumerary tooth, before starting any other intervention. While in a child older than 9 years of age with closed apex permanent maxillary incisor, it is feasible to expose the impacted incisors surgically and to extrude it orthodontically.
In this case report, the child was 11 years old while his maxillary incisors were in stage 4 of CVEK classification of root development (the root length of the tooth is almost finished however, its apex still widely open).14 Clinically, one of the extracted supernumerary teeth was diagnosed as supplemental central incisor because it showed similarity to incisor tooth, whereas the other supernumerary one revealed unusual morphological variation in both the crown and the root with appearance such as tuberculate supernumerary with dens invaginatus. Further, after the procedure, the child and his father insisted to take the extracted supernumerary teeth with them, so we lost the ability to subject the extracted tooth to additional investigation like radiographic assessment, microcomputed tomography analysis, and/or tooth sectioning to confirm diagnosis of this supernumerary tooth.
In the present case, as there was sufficient available space and the bulge of unerupted incisors was palpable, we decided to remove the supernumerary teeth and monitor their spontaneous eruption on recall visits. The permanent incisors erupted spontaneously within 6 months follow-up without any orthodontic interception.
Conclusion
The permanent incisors erupted spontaneously within 6 months follow-up after extraction of the two supernumerary teeth without any orthodontic interception.
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Yaqoob O, O'Neill J, Gregg T, et al. Management of unerupted maxillary incisors. Royal College of Surgeons England Publication; 2010. [Google Scholar]
- 2.Shaw WC, O'Brien KD, Richmond S, et al. Quality control in orthodontics: risk/benefit considerations. Br Dent J. 1991;170(1):33–37. doi: 10.1038/sj.bdj.4807399. DOI: [DOI] [PubMed] [Google Scholar]
- 3.Huber KL, Suri L, Taneja P. Eruption disturbances of the maxillary incisors: a literature review. J Clin Pediatr Dent. 2008;32(3):221–230. doi: 10.17796/jcpd.32.3.m175g328l100x745. DOI: [DOI] [PubMed] [Google Scholar]
- 4.Bishara SE. Treatment of unerupted incisors. Am J Orthod. 1971;59(5):443–447. doi: 10.1016/0002-9416(71)90080-7. DOI: [DOI] [PubMed] [Google Scholar]
- 5.Demiriz L, Durmuslar MC, Misir AF. Prevalence and characteristics of supernumerary teeth: a survey on 7348 people. J Int Soc Prevent Communit Dent. 2015;5:39–43. doi: 10.4103/2231-0762.156151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mitchell L. Supernumerary teeth. Dent Update. 1989;16(2):65–69. [PubMed] [Google Scholar]
- 7.Nuvvula S, Pavuluri C, Mohapatra A, et al. Atypical presentation of bilateral supplemental maxillary central incisors with unusual talon cusp. J Indian Soc Pedod Prev Dent. 2011;29(2):149–154. doi: 10.4103/0970-4388.84689. DOI: [DOI] [PubMed] [Google Scholar]
- 8.Kim Y, Jeong T, Kim J, et al. Effects of mesiodens on adjacent permanent teeth: a retrospective study in Korean children based on cone-beam computed tomography. Int J Paediatr Dent. 2018;28(2):161–169. doi: 10.1111/ipd.12317. DOI: [DOI] [PubMed] [Google Scholar]
- 9.Becker A. Early treatment for impacted maxillary central incisors. Am J Orthod Dentofacial Orthop. 2002;121(6):586–587. doi: 10.1067/mod.2002.124171. DOI: [DOI] [PubMed] [Google Scholar]
- 10.Mason C, Azam N, Holt RD, et al. A retrospective study of unerupted maxillary incisors associated with supernumerary teeth. Br J Oral Maxillofac Surg. 2000;38(1):62–65. doi: 10.1054/bjom.1999.0210. DOI: [DOI] [PubMed] [Google Scholar]
- 11.Alacam A, Bani M. Mesiodens as a risk factor in treatment of trauma cases. Dent Traumatol. 2009;25(2):25–31. doi: 10.1111/j.1600-9657.2008.00734.x. DOI: [DOI] [PubMed] [Google Scholar]
- 12.Seehra J, Yaqoob O, Patel S, et al. National clinical guidelines for the management of unerupted maxillary incisors in children. Br Dent J. 2018;224(10):779–785. doi: 10.1038/sj.bdj.2018.361. DOI: [DOI] [PubMed] [Google Scholar]
- 13.Leyland L, Batra P, Wong F, et al. A retrospective evaluation of the eruption of impacted permanent incisors after extraction of supernumerary teeth. J Clin Paediatr Dent. 2006;30(3):225–231. doi: 10.17796/jcpd.30.3.60p6533732v56827. DOI: [DOI] [PubMed] [Google Scholar]
- 14.Cvek M, Lundberg M. Histological appearance of pulps after exposure by a crown fractures, partial pulpotomy, and clinical diagnosis of healing. J Endod. 1983;9(1):8–11. doi: 10.1016/S0099-2399(83)80005-3. DOI: [DOI] [PubMed] [Google Scholar]