

Abstract
Background:
Once a device for telecommunication, now a powerful device bringing the whole world in one's palm, smartphones are increasingly becoming a common commodity among the medical students. Smartphones foster social interaction and facilitate multitasking and learning, but they also have some adverse effects. Young people, especially students, who are always inquisitive towards new technology, are likely to be affected by both these positive and negative impacts.
Objective:
To assess smartphone use and its association with the quality of life (QOL) of medical students.
Materials and Method:
A cross-sectional study was conducted among the undergraduate medical students of Government Medical College (GMC), Haldwani. All the students enrolled in MBBS course in GMC, Haldwani, who gave consent for participation and were present on the day of questionnaire administration, were included in the study. Smartphone addiction scale (SAS-SV), and WHO-BREF questionnaires for QOL were used for assessing smartphone use, and QOL of the medical students, respectively.
Results:
A total of 395 medical students were included in the study; out of them, 42% considered themselves addicted to the smartphone. According to SAS-SV, smartphone addiction was found among 43.8% medical students. It was seen that the junior-most and senior-most batches were significantly less addicted to the smartphone (p-value < 0.001). Male students were more addicted (OR = 1.45, CI = 0.962–2.174) to the smartphone as compared to females. The QOL of the students was significantly affected by smartphone use in all domains assessed (p-value ranging from < 0.001 to 0.002).
Conclusions:
Smartphone addiction is high among medical students and it has a significant negative impact on their QOL.
Keywords: Addiction, mobile phone, quality of life, smartphone, undergraduate medical students
Introduction
One of the greatest utility commodities of the modern age is the smartphone. Apart from the features of conventional phone, a smartphone is distinguished by the sophisticated hardware, software, internet and multimedia functionality. It has grown to be an essential and indispensable part of our daily life.
Telecom Regulatory Authority of India puts the number of wireless telephone users at 1183 million (89.55% of the population) as on 31 October 2019 with a monthly growth rate of 0.82%.[1] According to the Global Mobile Market Report, 2019, smartphone penetration in India is 345.916 million (25.3%).[2] This growth is a part of “Digital India” initiative – a campaign launched by the Government of India to ensure the availability of government's services electronically through the use of smartphone via the internet to every citizen of India.[3] The 'Digital India' initiative has made access to smartphones and the internet cheaper and widely available to everyone.
Smartphones foster social interaction and facilitate multitasking while at the same time impairing learning among youngsters.[4,5,6,7] Some of the other adverse effects of excessive use of smartphones are stress, depression, sleep deprivation, decreased academic performance, reduced available cognitive capacity, and dissatisfaction with life.[8,9,10,11] It may also be a potential means of transmitting microorganisms in healthcare settings.[12] Young people, especially students, who are always inquisitive towards new technology, are likely to be affected by both these positive and negative impacts.
Excessive smartphone use may lead to a series of changes in the QOL of an individual.[13] QOL is a subjective and multifaceted concept and implies satisfaction in physical, emotional, psycho-social, and spiritual needs. WHO defined quality of life (QOL) as “individuals' perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”.[14] As seen from various studies, the impact of smartphone usage whether positive or negative has a role in molding the QOL of an individual.[15,16,17] Physicians are likely to overlook smartphone addiction symptoms and group them under common diseases. Hence, the physicians need to be aware about the symptoms and how it affects the life of individuals. In this study, we intend to find out the relationship between the use of the smartphone and the QOL of the medical students, which has not been sufficiently studied so far.
Materials and Methods
Study design
A cross-sectional study.
Study settings
The study was conducted in Government Medical College (GMC), Haldwani, district Nainital, which is a tertiary level institute in Kumaun Division of Uttarakhand (India).
Sample size
All the students enrolled in the undergraduate medical course at GMC, Haldwani at the time of the study and who gave consent for participation, were included in the study.
Study population
The study was initiated after obtaining ethical approval from the Institutional Ethical Committee. GMC, Haldwani has an annual intake of 100 medical students in the Bachelor of Medicine and Bachelor of Surgery (MBBS) course. The MBBS course is spread over 5 years and 6 months (including 1-year internship period) and is divided into four professionals/phases: first professional (1 year), second professional (1 year 6 months), third professional part-I (1 year), third professional part-II (1 year), followed by 1 year of internship program. Therefore, at any given point of time, a maximum of 500 students are enrolled for the course in the institute. All the students enrolled in the MBBS course during the study period formed the part of study population.
Inclusion criteria
Medical students who were present on the day of filling the questionnaire and gave written consent were included in the study.
Exclusion criteria
Students who did not own a smartphone were excluded from the study. Also, questionnaires that were more than 20% incomplete were excluded from the final analysis.
Study tools
The following tools were utilized in this study:
Smartphone Addiction Scale (SAS) – SV was a validated scale, containing 10 questions with 6-point Likert scale was used to assess smartphone addiction. The cut-off used was 31 and 33 for male and female respondents respectively. The items on the scale have Cronbach's alpha of 0.911.[18]
WHO QoL – BREF consisting of 26 questions divided into 4 domains was used to assess the QOL. The mean score of questions within each domain was used to calculate the domain score, and scores of each domain were transformed into a scale ranging from 0 to 100.[14] The cut-off score for QOL was taken as 60, where higher scores indicate better or satisfied QOL and scores less than 60 indicates poor or unsatisfied QOL.[19]
Data collection
The students were approached unannounced in the lecture halls at the end of the lecture; after taking prior permission from the concerned faculties. The time of administration of the questionnaire was adjusted in a manner so that the students were not delayed for the next class - this was done to reduce apprehension and hurriedness in filling the form. The students were made to sit at an appropriate distance to prevent them from discussing among themselves. The aim and objectives of the study were explained and the students who were not interested in participating were allowed to leave. The questionnaires were given to the participants to fill them. The participants were requested to fill, and sign the consent form attached at the bottom of the front page of every questionnaire; it was torn-off from the main questionnaire by the participants themselves and collected separately, to maintain anonymity. The questionnaire took around 10 minutes to complete.
Data analysis
The data obtained was entered in MS Excel and descriptive analysis has been presented in appropriate figures, numbers/frequencies and percentages. The data were analyzed using Epi Info version 7.2.2.16. The p value of < 0.05 was considered to be statistically significant. Box-and-whisker plot is used to depict the distribution of scores of the various domains of QOL.
Results
Out of the total students enrolled, 414 participated in the study. After excluding 19 incomplete forms, 395 questionnaires were included in the final analysis. Out of the 395 study participants, 154 (39.0%) were male and 241 (61.0%) female. Majority of them were hostellers (94.7%) and the rest were day-scholars. The participant's age ranged from 17-28 years with the mean (SD) age of 20.94 (1.8) years. The educational status of the parents showed that 80.75% of the fathers and 62.12% of the mothers were either graduate or had a higher qualification. The majority of the mothers were reported to be homemakers (78.16%). Only 5.35% of the fathers were reported to have retired from their work [Table 1]. Among all the study participants, 42% felt that they were addicted to their smartphone use, which was similar to the overall smartphone addiction prevalence (43.8%) as estimated by the SAS-SV questionnaire [Table 2].
Table 1.
General characteristics of medical students in the study
| Sl. No | Characteristics (N=395) | Frequency | Percentage (%) | |
|---|---|---|---|---|
| 1 | Batch | 2018-19 | 79 | 20.00 |
| 2017-18 | 84 | 21.30 | ||
| 2016-17 | 84 | 21.30 | ||
| 2015-16 | 88 | 22.30 | ||
| 2014-15 | 60 | 15.20 | ||
| 2 | Gender | Male | 154 | 39.00 |
| Female | 241 | 61.00 | ||
| 3 | Age (years) | 17-20 | 163 | 41.30 |
| 21-24 | 219 | 55.40 | ||
| 25-28 | 13 | 3.30 | ||
| 4 | Residence | Hosteller | 374 | 94.70 |
| Day scholar | 21 | 5.30 | ||
| 5 | Fathers’ education (n=374) | 0-10 | 14 | 3.74 |
| 11-12 | 58 | 15.51 | ||
| Graduate and above | 302 | 80.75 | ||
| 6 | Fathers’ occupation (n=374) | Govt. sector | 245 | 65.51 |
| Private sector | 109 | 29.14 | ||
| Retired | 20 | 5.35 | ||
| 7 | Mothers’ education (n=367) | 0-10 | 56 | 15.26 |
| 11-12 | 83 | 22.62 | ||
| Graduate and above | 228 | 62.12 | ||
| 8 | Mothers’ occupation (n=380) | Working | 83 | 21.84 |
| Housewife | 297 | 78.16 | ||
Table 2.
Smartphone addiction according to social characteristics and self-reported addiction
| Characteristics | Smartphone addiction, N=395 (%) | P* | OR* (95% CI*) | ||
|---|---|---|---|---|---|
| Present | Absent | ||||
| Batch | 2018-19 | 22 (27.8) | 57 (25.7) | <0.001 | 1 |
| 2017-18 | 39 (46.4) | 45 (53.6) | 2.24 (1.17-4.31) | ||
| 2016-17 | 40 (47.6) | 44 (52.4) | 2.35 (1.23-4.52) | ||
| 2015-16 | 54 (61.4) | 34 (38.6) | 4.11 (2.14-7.90) | ||
| 2014-15 | 18 (30.0) | 42 (70.0) | 1.11 (0.53-2.33) | ||
| Gender | Female | 97 (40.2) | 144 (59.8) | 0.076 | 1 |
| Male | 76 (49.4) | 78 (50.6) | 1.45 (0.96-2.17) | ||
| Age (years) | 17-20 | 61 (37.4) | 102 (62.6) | 0.043 | 1 |
| 21-24 | 108 (49.3) | 111 (50.7) | 1.63 (1.08-2.46) | ||
| 25-28 | 4 (30.8) | 9 (69.2) | 0.74 (0.22-2.52) | ||
| Self-reported addiction | Not addicted | 57 (24.9) | 172 (75.1) | <0.001 | 1 |
| Addicted | 116 (69.9) | 50 (30.1) | 7.00 (4.48-10.94) | ||
*P<0.05. CI: Confidence interval; OR: Odds ratio
Batch-wise analysis of smartphone addiction among medical students, revealed that 46.4%, 47.6% and 61.4% of the batches 2017-18, 2016-17, 2015-16 students, respectively, were addicted to smartphone, which was significantly higher than the students of junior-most batch, 2018-19 (27.8%) and senior-most batch, 2014-15 (30.0%) (p-value < 0.001). Smartphone addiction was also found to be more common in the males (OR = 1.45, CI = 0.962–2.174) though not statistically significant (p-value 0.076), and the study participants belonging to age group 21-24 years (OR = 1.63, CI = 1.08-2.46) [Table 2].
The sociodemographic characteristics of the study participants along with their scores of QOL are shown in Table 3. Figure 1 depicts a box-and-whisker plot with median scores for the QOL of different domains. More than half of the students' scores in psychological and environmental domain were found to be non-satisfactory. Among those who showed non-satisfactory levels in the domains under study, a significant difference between physical health, mental health, social well-being, and environmental surrounding of the students with smartphone addiction was found (p-value ranging from < 0.001 to 0.002) [Table 4]. The mean scores of each domain of QOL for students is shown in Figure 2.
Table 3.
Distribution of scores of quality of life with batch and demographic characteristics
| Characteristics | Physical health range | Psychological health range | Social relationship range | Environment range | |
|---|---|---|---|---|---|
| Batch | 2018-19 | (31-88) | (13-94) | (6-69) | (31-100) |
| 2017-18 | (31-100) | (31-94) | (25-69) | (25-100) | |
| 2016-17 | (19-100) | (31-88) | (0-69) | (19-88) | |
| 2015-16 | (13-94) | (132-94) | (19-69) | (31-94) | |
| 2014-15 | (19-94) | (25-94) | (25-69) | (31-100) | |
| Gender | Male | (31-100) | (13-94) | (0-69) | (31-100) |
| Female | (13-94) | (19-94) | (25-69) | (19-88) | |
| Age (years) | 17-20 | (19-100) | (13-94) | (6-69) | (25-100) |
| 21-24 | (13-94) | (13-94) | (19-69) | (25-100) | |
| 25-28 | (44-100) | (44-81) | (0-69) | (50-88) | |
Figure 1.
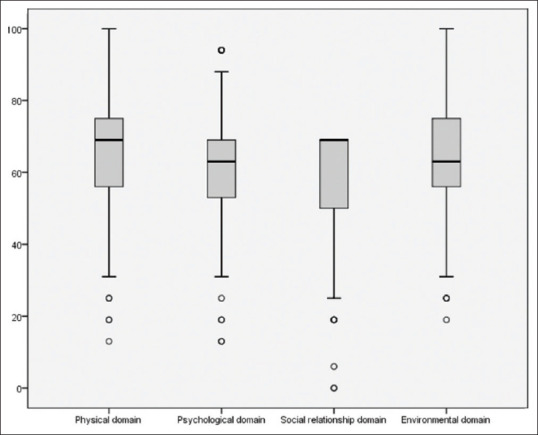
Box-and-whisker plot depicting the distribution of scores of QOL domains
Table 4.
Association between smartphone addiction and quality of life of medical students
| Characteristics | Smartphone addiction, N=395 (%) | P | ||
|---|---|---|---|---|
| Absent (n=222) | Present (n=173) | |||
| Physical domain | Not satisfied | 87 (47.54) | 96 (52.45) | 0.002 |
| Satisfied | 135 (63.68) | 77 (36.32) | ||
| Psychological domain | Not satisfied | 69 (40.35) | 102 (59.65) | <0.001 |
| Satisfied | 153 (68.30) | 71 (31.70) | ||
| Social domain | Not satisfied | 86 (47.00) | 97 (53.00) | <0.001 |
| Satisfied | 136 (64.15) | 76 (35.85) | ||
| Environmental domain | Not satisfied | 101 (49.0) | 105 (51.0) | 0.003 |
| Satisfied | 121 (64.0) | 68 (36.0) | ||
Figure 2.

Distribution of scores of QOL domains with the batches of medical students
Discussion
In the age of advancing technology, a smartphone is one of the indispensable entities in everyday life. Smartphones are not only used for communication but also used for browsing the internet for information, entertainment, and numerous other activities. Nonetheless, with the introduction of new technology both comfort and problems are inherited. In the present study, we report the prevalence of smartphone addiction and the relationship between smartphone addiction and QOL of undergraduate medical students and interns at a Government Medical College.
There has been a considerable reduction in the cost of smartphones in recent years,[20] which make the smartphone an affordable commodity, thereby leading to indiscriminate use. Smartphone addiction was found to be present in 43.8% of the participants in our study. Similar findings are reported in the studies conducted by Basu et al.[21] in North India and by Alhazmi et al.[22] in Saudi Arabia. The prevalence was recorded to be much higher by Sethuraman AR et al. (85%) in a medical college in Andaman and Nicobar Islands.[23] But, smartphone addiction was reported to be lesser by Chen et al.[24] in China and Ammati et al.[25] in South India. The reasons for higher smartphone addiction in Andaman and Nicobar Islands may include that Andaman and Nicobar Islands is a geographically secluded area from mainland India with limited avenues for other kinds of social interactions or recreational activities especially for students from mainland India. Also, place-specific cultural or individual factors may influence smartphone addiction levels – all of which are not known/have been studied. The lower prevalence in China and South India may be explained by more cohesive social structures in these regions which might limit smartphone use and its addiction.
About 70% of the study participants who self-reported that smartphone addiction, was actually addicted to smartphone use according to SAS-SV questionnaire. Thus, the majority of the study participants were aware of their over-use of smartphones in our study. Karki et al. have also observed self-acknowledgement as a predictor of smartphone addiction.[23] We corroborate their finding and state that there is high degree of awareness of being addicted to smartphone use among excessive mobile phone users.
Most of the studies conducted in different parts of the globe have suggested that females are more addicted to smartphones as compared to males.[15,26,27,28] Some of the reasons cited were, women regard interpersonal interaction (development and maintenance of relationship) and quick communication more highly, which is fulfilled through various social media platforms.[26] In contrary, studies conducted by Basu and Ghosh among Indian medical students found more male students addicted to the smartphone than females.[21,29] In the present study, we too report smartphone addiction to be significantly higher among male students. Findings similar to our study have also been reported by Hassan and Hassan[30] and Karki et al.[31] in other South-east Asian countries. The variance in the above findings may be attributed to the disparity in the participants' psycho-social and cultural environments based on different parts of the world. It has been observed that female students are often more inclined towards the academic achievement (which is also reflected in the examination results) in India.[32,33]
The study participants included in our study consisted of five different batches undergoing medical education and training. Smartphone addiction was observed to be significantly high among the students of batch 2017-18 and least among the first year (2018-19) and those among the senior-most batch (2014-15). This could be ascribed to three things, firstly, the first-year students may not yet have totally internalized the identity and lifestyles as medical student and thus may be different from their senior batches, also because of the tough and totally different nature of studies during MBBS course (compared to school), they might still be getting accustomed to it which may limit the use of a smartphone. Students belonging to senior batches may get accustomed to the curriculum hence might be giving more time to leisure activities and social networking through smartphones. It might also be due to a negative outlook among senior batches due to a tough curriculum with limited opportunities for personal hobby development and the constant pressure of examinations and fear of failure. Students of the senior-most batch may get less time due to their duties in the hospital and also, they might be preparing for the upcoming exams, thereby reducing their time spent with the smartphones.
The present study showed a significant association between non-satisfactory feelings in different domains of QOL and smartphone addiction among the study participants. The most important domain affected by smartphone addiction is the psychological domain, where only 31% of the addicted individuals were found to be satisfied with their mental status. Some of the reasons behind the unsatisfactory feeling towards the mental domain may be because smartphone addiction leads to sleep interference and is often accompanied with substance and behavioral abuses, and other comorbidities such as stress, anxiety, and depression.[34] Also, studies have shown that addiction to smartphone tends to make one's life stressful and lonely and unsatisfactory relationship.[16,35] Youth tends to follow and idolize celebrities via social media and other online or offline platform and compare themselves with the latter and even concluded that their life is meaningless and are even embarrassed of their physical appearances.[36] The attitude of comparing and competing, fear of missing out, along with other factors mentioned earlier may be some of the reasons for unsatisfactory psychological level shown by the smartphone addicts.
Individuals glued to their smartphones tend to be sedentary and often socialize only with their virtual friends rather than the actual person next to him/her thereby limiting their inter-personal relationships and the opportunity for leisure activities away from the smartphone. Most of the smartphone addicts were not satisfied with the support they obtain from their friends nor were they satisfied with themselves or their daily activities.
Limitations
As it is a cross-sectional study, we cannot establish any temporal relationship between QOL and smartphone addiction; since the study was conducted in a single medical college in Uttarakhand, caution must be exercised while generalizing the findings from the study. The current study did not differentiate between smartphone use for educational and other purposes.
Conclusion
The present study shows that smartphone addiction is present among medical students, especially so among males. We also report that smartphone addiction has a significant negative association with QOL among medical students and is inversely related. Therefore, students should be counselled regarding the judicious use and negative effects arising from the excessive use of a smartphone. We also recommend more studies to generate more data on this issue from other colleges, the community at large, and also, for testing/evaluation of potential interventions to deal with this issue.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Telecom Regulatory Authority of India. Available from: https://wwwtraigovin/release-publication/reports/telecom-subscriptions-reports .
- 2.Global Mobile Market Report. Available from: https://newzoocom/insights/rankings/top-50-countries-by-smartphone-penetration-and-users/
- 3.Digital India. Available from: http://digitalindiagovin/
- 4.Rotondi V, Stanca L, Tomasuolo M. Connecting alone: Smartphone use, quality of social interactions and well-being? J Econ Psychol. 2017;63:17–26. doi: 10.1016/j.joep. 2017.09.001. [Google Scholar]
- 5.Gladden D. The effects of smartphones on social lives: How they affect our social interactions and attitudes2018 OTS Master's Level Projects & Papers 586. Available from: https://digitalcommonsoduedu/ots_masters_projects/586 .
- 6.Carrillo R, Subrahmanyam K. Mobile phone multitasking and learning. Available from: https://wwwsemanticscholarorg/paper/Mobile-Phone-Multitasking-and- Learning-Carrillo-Subrahmanyam/587 c01633ea2458f5e509fffcead32c008fedf66#citing-papers . doi: 104018/978-1-4666-8239-9ch007.
- 7.Chen Q, Yan Z. Does multitasking with mobile phones affect learning?? A review. Comput Hum Behav. 2016;54:34–42. doi: 10.1016/j.chb. 2015.07.047. [Google Scholar]
- 8.Wallace P. Internet addiction disorder and youth. EMBO Rep. 2014:15. doi: 10.1002/embr.201338222. doi: 101002/embr201338222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Samaha M, Hawi NS. Relationships among smartphone addiction, stress, academic performance, and satisfaction with life. Comput Hum Behav. 2016;57:321–5. [Google Scholar]
- 10.Tao S, Wu X, Zhang S, Tong S, Hao J, Tao F. Association of alcohol use with problematic mobile phone use and depressive symptoms among college students in Anhui, China. J Public Health. 2017;25:103–12. [Google Scholar]
- 11.Ward AF, Duke K, Gneezy A, Bos MW. Brain drain: The mere presence of one's own smartphone reduces available cognitive capacity. J Assoc Consum Res. 2017;2:140–54. [Google Scholar]
- 12.Bisht M, Kumar M, Solanki HK, Kaur T, Umesh, Rawat V. Microbial contamination of mobile phones of health care providers at a teaching hospital in a Hilly North Indian State. Ind J Comm Fam Med. 2018;4:34–9. [Google Scholar]
- 13.Baek S-S, Cho J-Y. The effects of college students' life stress, depression, and smartphone addiction on their quality of life. J Korean AcadIndus Technol Soc. 2017;18:248–56. [Google Scholar]
- 14.WHOQOL: Measuring Quality of Life. Available from: https://wwwwhoint/healthinfo/survey/whoqol-qualityoflife/en/
- 15.Shahrestanaki E, Maajani K, Safarpour M, Ghahremanlou HH, Tiyuri A, Sahebkar M. The relationship between smartphone addiction and quality of life among students at Tehran University of medical sciences. Addicta: Turk J Addict. 2020;7:61–6. [Google Scholar]
- 16.Safa DeMajeed S. Smartphone addiction, loneliness, interpersonal relationship and quality of life in adolescents and adults. EurJ Res Soc Sci. 2020;8:23–9. [Google Scholar]
- 17.Mascia ML, Agus M, Penna MP. Emotional intelligence, self-regulation, smartphone addiction: Which relationship with student well-being and quality of life?? Front Psychol. 2020;11:375. doi: 10.3389/fpsyg.2020.00375. doi: 10.3389/fpsyg. 2020.00. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kwon M, Kim D-J, Cho H, Yang S. The smartphone addiction scale: Development and validation of a short version for adolescents? PLoS One. 2013;8:e83558. doi: 10.1371/journal.pone.0083558. doi: 10.1371/journal.pone. 0083558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Silva PA, Soares SM, Santos JF, Silva LB. Cut-off point for WHOQOL-bref as a measure of quality of life of older adults. Rev Saude Publica. 2014;48:390–7. doi: 10.1590/S0034-8910.2014048004912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dholakia K. A study in price drops of popular smartphones. Available from: https://wwwmedianamacom/2015/02/223-a-study-in-price-drops- of-popular-smartphones-ankur-p-agarwal-pricebaba/
- 21.Basu S, Garg S, Singh MM, Kohli C. Addiction-like behavior associated with mobile phone usage among medical students in Delhi. Indian J Psychol Med. 2018;40:446–51. doi: 10.4103/IJPSYM.IJPSYM_59_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Alhazmi AA, Alzahrani SH, Baig M, Salawati EM, Alkatheri A. Prevalence and factors associated with smartphone addiction among medical students at King Abdulaziz University, Jeddah. Pak J Med Sci. 2018;34:984–8. doi: 10.12669/pjms.344.15294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sethuraman AR, Rao S, Charlette L, Thatkar PV, Vincent V. Smartphone addiction among medical college students in the Andaman and Nicobar Islands. Int J Community Med Public Health. 2018;5:4273–7. [Google Scholar]
- 24.Chen B, Liu F, Ding S, Ying X, Wang L, Wen Y. Gender differences in factors associated with smartphone addiction: Across-sectional study among medical college students. BMC Psychiatry. 2017;17:341. doi: 10.1186/s12888-017-1503-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ammati R, Kakunje A, Karkal R, Nafisa D, Kini G, Chandrashekaran P. Smartphone addiction among students of medical university in South India: A cross-sectional study. Ann Int Med Den Res. 2018;4:PY01–4. [Google Scholar]
- 26.Lee KE, Kim SH, Ha TY, Yoo YM, Han JJ, Jung JH, et al. Dependency on smartphone use and its association with anxiety in Korea. Public Health Rep. 2016;131:411–9. doi: 10.1177/003335491613100307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Igarashi T, Takai J, Yoshida T. Gender differences in social network development via mobile phone text messages: A longitudinal study. J Soc Pers Relat. 2005;22:691–713. [Google Scholar]
- 28.Andone I, Błaszkiewicz K, Eibes M, Trendafilov B, Montag C, Markowetz A. How age and gender affect smartphone usage Proceedings of the 2016. ACM International Joint Conference on Pervasive and Ubiquitous Computing Adjunct – UbiComp. 2016 doi: 101145/29682192971451. [Google Scholar]
- 29.Ghosh S, Chatterjee S. Assessment of internet addiction among undergraduate medical students: Across-sectional study in a medical college of Kolkata. J ClinDiagn Res. 2018;12:VC05–9. [Google Scholar]
- 30.Hassan N, Hassan T. Female students get more marks as compared to male students: Astatistical study? J Bus Fin Aff. 2016;5:226. doi: 10.4172/2167-0234.1000. [Google Scholar]
- 31.Karki S, Singh JP, Paudel G, Khatiwada S, Timilsina S. How addicted are newly admitted undergraduate medical students to smartphones.: A cross-sectional study from Chitwan medical college, Nepal? BMC Psychiatry. 2020;20:95. doi: 10.1186/s12888-020-02507-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.CBSE announces Class 12 results. Two UP girls top the exams. Available from: https://economictimes.indiatimes.com/industry/services/education/cbse-class-12-result/articleshow/69141465.cms?from=mdr .
- 33.NEET 2018 Result Statistics. Available from: https://medicinecareers360com/articles/neet-2018-result-statistics .
- 34.De-Sola Gutiérrez J, Rodríguez de Fonseca F, Rubio G. Cell-phone addiction: Areview. Front Psychiatry. 2016;7:175. doi: 10.3389/fpsyt.2016.00175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cunningham S. The hidden stress of cell phones. Available from: https://wwwuchealthorg/today/the-hidden-stress-of-cell-phones/
- 36.Mannino B. Ideal to real body image survey. Available from: https://wwwaolcom/article/2014/02/24/loveyourselfie/20836450/