

Abstract
The purpose of the STAR 2019 Working Group was to build on findings from the initial STAR report to further clarify the expectations, limitations, perceptions, and utility of alloimmune assays that are currently in use or in development for risk assessment in the setting of organ transplantation. The goal was to determine the precision and clinical feasibility/utility of such assays in evaluating both memory and primary alloimmune risks. The process included a critical review of biologically driven, state‐of‐the‐art, clinical diagnostics literature by experts in the field and an open public forum in a face‐to‐face meeting to promote broader engagement of the American Society of Transplantation and American Society of Histocompatibility and Immunogenetics membership. This report summarizes the literature review and the workshop discussions. Specifically, it highlights (1) available assays to evaluate the attributes of HLA antibodies and their utility both as clinical diagnostics and as research tools to evaluate the effector mechanisms driving rejection; (2) potential assays to assess the presence of alloimmune T and B cell memory; and (3) progress in the development of HLA molecular mismatch computational scores as a potential prognostic biomarker for primary alloimmunity and its application in research trial design.
Keywords: alloantibody, antigen biology, clinical research/practice, histocompatibility, lymphocyte biology, major histocompatibility complex (MHC), rejection: antibody‐mediated (ABMR)
Short abstract
This meeting report from an AST‐ASHI expert workgroup provides recommendations on the utility and “clinical‐grade” qualification of assays and biomarkers to evaluate alloimmune risk.
Abbreviations
- AMR
antibody‐mediated rejection
- ASC
antibody‐secreting cell
- ASHI
American Society of Histocompatibility and Immunogenetics
- AST
American Society of Transplantation
- CLIA
Clinical Laboratory Improvement Act
- CMS
Centers for Medicare and Medicaid Services
- Tfh
T follicular helper cells
- CV
coefficient of variance
- DSA
donor‐specific antibody
- EMS
electrostatic mismatch score
- FDA
US Food and Drug Administration
- LN
lymph node
- MFI
mean fluorescence intensity
- mMM
molecular mismatch
- PIRCHE‐II
predicted indirectly recognizable HLA epitopes presented by recipient HLA‐class II antigens
- PRT
panel reactive T cell
- RCT
randomized controlled trial
- SAB
single antigen bead
1. INTRODUCTION
The ability to personalize management for a given transplant recipient and thereby optimize their long‐term outcome remains a critical unmet need. Indeed, the majority of variance in the choice of induction or maintenance therapy is based on center‐specific practices rather than on the traditional risk factors offered in practice guidelines. 1 , 2 By comparison, other medical fields are realizing major advances in the development of diagnostic, prognostic, and predictive biomarkers enabling individualized therapeutic and monitoring strategies while avoiding futile treatments with their associated toxicities.
In 2017, the STAR Working Group was launched by the American Society of Transplantation (AST) and American Society for Histocompatibility and Immunogenetics (ASHI) to address these unmet needs by evaluating (1) the prognostic utility of laboratory assays to precisely characterize an individual's alloimmune risk and (2) the predictive utility of laboratory assays to guide therapeutic decisions for the individual before transplant.
The STAR 2017 report 3 highlighted the marked variability among centers for defining and assigning a level of alloimmune risk for a given donor/recipient pair. In part this is due to the misuse, and lack, of standardized terminology, and the varying interpretation of clinical assays without rigorous proof of the claims being asserted. STAR provided a primer to bring clarity and accuracy to alloimmune risk definitions and terminology. The STAR 2017 report also created a framework and identified the need for every donor/recipient pair to be assigned 2 independent risk assessments: 1 for alloimmune memory and 1 for primary alloimmunity. This framework is intended to serve as a basis for precision therapeutic strategies.
The STAR 2019 Working Group's goal was to further expand on the expectations, limitations, perceptions, and actual utility of available alloimmune assays that are currently in use or in development to precisely evaluate alloimmune risk. Along with critically reviewing biologically driven, state‐of‐the‐art, clinical diagnostics literature by experts in the field, the STAR 2019 workshop was open for public participation, to allow broader engagement of the AST and ASHI membership. High‐level summary and recommendations is presented in Figure 1. To facilitate discussion on the clinical utility of current assays, this report provides a primer on the requirements set forth by Clinical Laboratory Improvement Act (CLIA), College of American Pathologists, and the US Food and Drug Administration (FDA) for qualification as a “clinical‐grade” assay or biomarkers.
Figure 1.
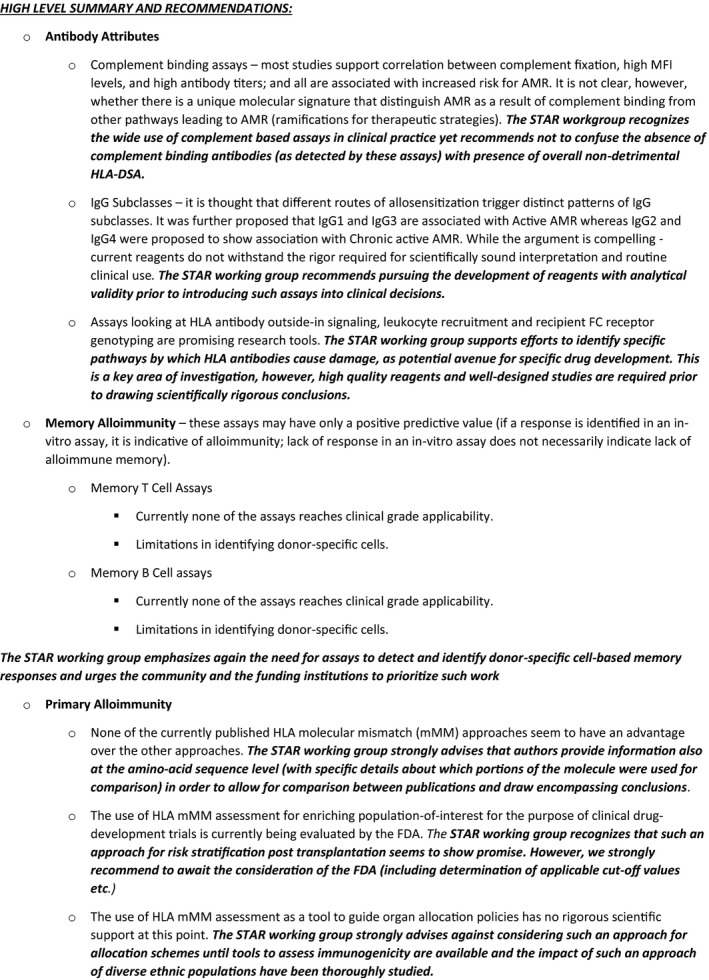
High level summary and recommendations: provide a brief review of assays and approaches to assess immunogenicity, their limitations, and recommendations regarding their use
2. ANALYTICAL VALIDITY, CLINICAL VALIDITY, AND CLINICAL UTILITY OF LABORATORY ASSAYS
In the United States, to ensure accurate and reliable test results, only laboratories accredited by a CLIA‐approved program, such as Collage of American Pathologists, ASHI, etc., can perform tests using patients’ samples to support clinical decision making. All assays must demonstrate analytical validity, performance characteristics, as it pertains to the use of the assay in the laboratory's own environment (see 42 CFR 493.1253(b) 2 ; establishment of performance specifications). The analytical validation must document accuracy, precision, and analytical sensitivity (reproducibility, coefficient of variance [CV], reportable ranges, reference interval values, and analytical specificity). Calibration and control procedures must be determined, and the laboratory must be enrolled in external proficiency testing programs. Even for an unmodified, FDA‐cleared or approved test system, a laboratory must (1) demonstrate that it can obtain performance specifications comparable to those established by the manufacturer for accuracy and precision and (2) verify that the manufacturer's reference intervals (normal values) are appropriate for the laboratory's patient population before reporting results using that test (Table 1).
Table 1.
Evaluation of laboratory assays—path for clinical utility
| Purpose/expectations | Information provided | Regulated by |
|---|---|---|
| Analytical validity | ||
| Demonstrates the accuracy, precision, and reproducibility of the test in a clinical laboratory setting | How well does the test measure what it claims to measure | CMS/CLIA mandate |
| Clinical validity | ||
| Demonstrates the effectiveness of the test—ie correlation between the test result and the pathophysiology of the disease—for diagnostic/prognostic/predictive accuracy | How relevant is the test measurement to the clinical condition? | FDA mandate |
| Clinical utility | ||
| Demonstrates that the test result performs around the clinical decision point (SD and %CV that can change patient treatment) | Is the test result relevant to the clinical decision making (eg treatment). Can it lead to clinical decision that improves patient outcome | Often determined after the assay is in clinical use |
| Statistical significance ≠ clinical significance | ||
Abbreviations: CLIA, Clinical Laboratory Improvement Act; CMS, Centers for Medicare and Medicaid Services; CV, coefficient of variance; FDA, US Food and Drug Administration.
It is important to appreciate that an assay with pristine analytical validity does not imply association between the test result and a clinical outcome. Thus, clinical validity of an assay should be proved beyond the analytical validity. For example, serum samples of patients undergoing dialysis do not have the same characteristics as samples from healthy controls. Similarly, sera from patients with high breadth and strength of HLA antibodies are likely to exhibit different properties compared with individuals with no or low levels of HLA antibodies. 4 It should be noted that the antibody‐assay manufacturers do not have easy access to relevant patient populations’ material and thus are limited in their ability to evaluate assay performance in a clinical setting. As a result, our field only recently came to appreciate the limitations of inhibitory/interfering substances (“prozone”) and of bead saturation. 5 See the call for immediate action in this regard (Figure 2).
Figure 2.
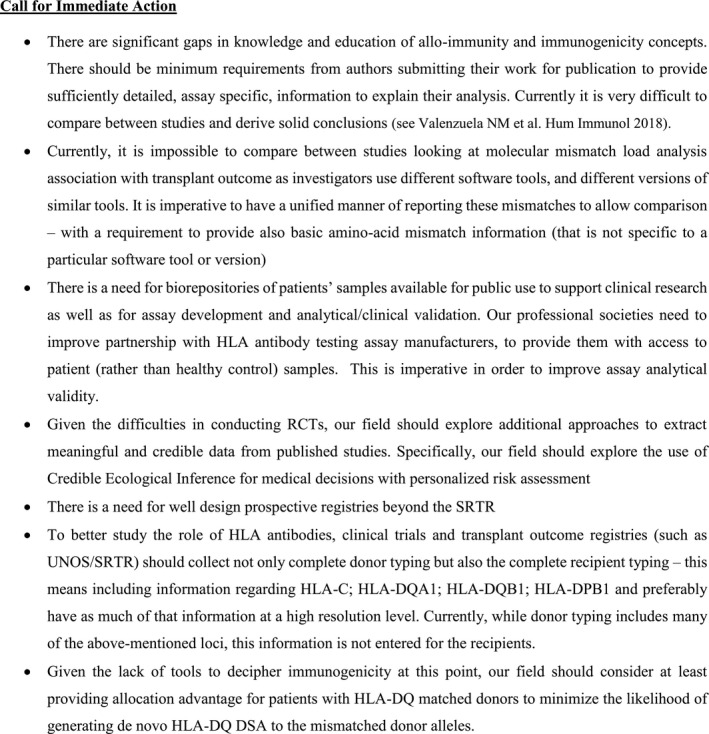
Call for immediate action: highlights area where progress can be achieved within the near future, or where action is required in order to drive progress
The clinical utility of an assay requires evidence of an improved, measurable, clinical outcome that is directly related to the use of the test; that is, the test should add significant value to patient care. This takes into consideration how the assay is interpreted and how results are reported (positive/negative vs continuous scale) and applied. Unfortunately, while proper evaluation of an assay's clinical utility requires prospective randomized controlled trials (RCTs), to date new assays in the field of transplantation report prospective/retrospective observational correlations, at best. In the absence of RCTs, evaluation of clinical utility is inferred based on systematic reviews and/or meta‐analytic approaches.
A systematic review collects, critically appraises, and summarizes the empirical evidence that fits a prespecified eligibility criterion. Meta‐analysis is a statistical approach that assigns a point estimate (of an unknown “common truth”) from individual studies and pools results of multiple studies based on a weighted average. Most often, the random‐effects model is used to express heterogeneity across disparate studies. A key benefit of this approach is the accumulation of information to reach higher statistical power. The end result, however, is an estimate of a mean parameter across population‐of‐studies rather than a population of patients. 6 , 7 This is especially true in publications assessing HLA antibodies as different studies use different testing methods and criteria to define the presence or absence of those antibodies.
A significant limitation of both systematic reviews and meta‐analysis is “publication bias.” 8 , 9 , 10 It is well established that most manuscripts accepted for publication report on research that shows a significant result, usually in favor of a new treatment/test. “Negative result” submissions are rarely published. Thus, a literature search is fundamentally biased as it is unlikely to identify publications with negative results. Many studies have identification problems arising from imperfections in the internal and external validity of the study, which cannot be fixed by the use of meta‐analysis. It was therefore reported that the relevance of systematic reviews and meta‐analysis to personalized patient care is not evident and cannot replace well‐designed prospective clinical trials. 11 See the call for immediate action in this regard (Figure 2).
It is through this lens that the STAR 2019 workshop considered the potential state‐of‐the‐art assays for pretransplant risk assessment, highlighting need for scrutiny before full implementation into clinical decision‐making schemes.
3. ATTRIBUTES OF HLA ANTIBODIES
Although HLA donor‐specific antibody (DSA) has shown association with AMR and poor allograft outcome, 12 this correlation is far from being absolute. Factors that may contribute to this observation involve the slow learning curve of accurately interpreting single antigen bead (SAB) assay results. Even if a strict cutoff value is enforced, which is a questionable practice given the relatively high %CV in mean fluorescence intensity (MFI) read‐out (>25% even when stringent standardization was applied), 13 additional factors such as lack of appreciation of potential inhibition, bead saturation, and “shared epitope phenomena” as mentioned by the STAR 2017 report 3 can lead to incorrect conclusions regarding antibody detection. Finally, different attributes of HLA antibodies may lead to, or at least are associated with, different transplant outcomes. Thus, new approaches are being explored to optimize risk stratification (Table 2).
Table 2.
HLA IgG antibody attributes
| Assay | Expected utility | Pros | Cons | Research tool | Analytic validity | Clinical validity | Clinical utility |
|---|---|---|---|---|---|---|---|
| HLA‐SAB with complement fixation attribute | Risk stratification of patients at high risk to develop AMR (similar to the CDC‐XM with added specificity); currently used both pre‐ and posttransplant | Overcome (at least in part) the “prozone” effect; improves quantification of antibody strength over pure MFI values (especially if inhibition is not treated); correlated with positive XM and inreased risk of AMR | Currently, does not provide information beyond high antibody titer; different assays target different steps of the complement cascade; may send false sense of “low‐risk” if negative but does not correlate with level of activation of memory responses; poor intra‐assay negative and positive controls; in vitro complement binding does not always equal in vivo complement binding | ✓ | ✓ | Inferred | N/D |
| HLA antibody IgG subclass | Determination of Ig subclass may distinguish between different antibody activation pathways; currently suggested for posttransplant use | Identification of effector function pathways can guide development of new immunosuppressive regimens and lead to improved intervention | Poor quality of reagents; crossreactivity of reagents; lack of relevant controls; different affinity of secondary antibody and potentially differences in levels of flourescence; inability to compare between different subclasses quantitatively | ✓ | N/D | N/D | N/D |
| HLA antibody and outside in signaling | Use of the mTOR signaling axis as a diagnostic tool for AMR after DSA binding to the HLA epitope and mTOR pathway activation | Identification of pathogenic pathways can guide development of new immunosuppressive regimens and lead to improved intervention | Lack of analytically validated reagents | ✓ | N/D | N/D | N/D |
| Analysis of DSA subclass and recipient Fc receptor genotype | Risk stratification of AMR episodes based on specific antibody attributes for leukocyte recruitment and activation in the microcirculation | Identification of pathogenic pathways can guide development of new immunosuppressive regimens and lead to improved intervention | Lack of analytically validated reagents | ✓ | N/D | N/D | N/D |
Inferred*—given the multitude of work published associating positive results in complement binding assays and poor graft outcome, the clinical validity may be inferred despite the cons described.
Abbreviations: AMR, antibody‐mediated rejection; CDC‐XM, complement‐dependent cytotoxic crossmatch; MFI, mean fluorescence intensity; N/D, not demonstrated; SAB, single antigen bead.
3.1. Complement fixation assays
Lessons from the CDC crossmatch assay, the “gold standard,” indicated that complement activation is associated with the most severe forms of antibody‐mediated rejection (AMR)—hyperacute and accelerated rejections. 14 Thus, the increased sensitivity of the solid‐phase–based Luminex assays was proposed as a means to differentially attribute risk levels to antibodies that activate complement in vitro vs those that do not. 15 , 16 , 17 Assays developed to look at different components of the complement cascade (C1q, C3d, C4d) indeed appear to reveal a correlation between this attribute and greater likelihood to develop AMR and a higher incidence of graft loss, 18 , 19 , 20 including in a systematic review and meta‐analysis. 21 However, in AMR with DSAs that in vitro do not exhibit complement fixation, 40% have been reported to exhibit C4d+ histology in vivo. 22 Most of the data reveal a strong association between in vitro complement fixation and high MFI levels/antibody titers. 4 , 23 , 24 , 25 This is further complicated by the fact that antibody titer can change dynamically, which will affect the complement assay results, such that a low titer complement fixing DSA at a particular time point will be C1q– and then increase its titer to become C1q+ in a consecutive test. 4 , 5 , 26 , 27 Although a distinct molecular signature for AMR appears to occur in the context of in vitro complement‐fixing antibodies, 28 it is not clear whether this correlation is due to the titer and/or polyclonality of the circulating antibody rather than the relative ability of each subclass to fix complement. 22 , 28 , 29 , 30 , 31
Gaps requiring further research:
Need to distinguish whether in vitro complement binding in solid‐phase assays is simply a marker of higher titer/enhanced functional capacity of DSAs, or if it provides additional information of an in vivo mechanism of physiological complement activation. This may have implications in associating such qualities with different types of AMR.
Need for biochemical analysis of antibody attributes associated with function (e.g., comparing class I vs class II antibodies, sialyation status of DSA, 32 and the relationship with the time of detection in a process). This may guide interpretation of assay results and choice of therapeutic management.
3.2. HLA antibody subclass
Cell‐based and solid‐phase assays testing for HLA antibodies traditionally identify antibodies of the IgG isotype. However, these assays do not distinguish between stronger complement‐fixing IgG1 and IgG3 subclasses from the lesser complement‐fixing IgG2 and IgG4, given that the detection reagent is specific for all Fcγ. Different routes of allosensitization trigger distinct patterns of IgG subclasses directed against HLA. 33 , 34 , 35 Preliminary studies of HLA antibody subclasses suggest that IgG2 and IgG4 do not constitute a large proportion of HLA DSAs. Rather, HLA IgG1 and IgG3 are the predominant subclasses associated with graft rejection and graft loss. 36 , 37 , 38 , 39 , 40 Although preformed IgG3 DSAs may be associated with risk of acute rejection, DSAs of the IgG2 and IgG4 subclasses are not associated with absence of rejection (i.e., these subclasses are not demonstrably benign). 36 , 41 This may be due to the fact that IgG4 arises from repeated antigen stimulation such as is seen in allergy or chronic infection and that the γ2 and γ4 genes are further downstream on the germline and often only produced after sequential switching from other γ immunoglobulins. 28 , 42 , 43 , 44 , 45 Importantly, current reagents to determine IgG subclasses in the context of HLA‐SAB assays have cross‐reactivity/lack of specificity. 46 Moreover, all studies to date attempting to define the IgG subclass of HLA antibodies have conceded that 10%‐20% of total IgG‐positive HLA antibodies could not be classified by any of the 4 IgG subclass‐specific reagents. 36 Other technical limitations include difficulties in directly comparing concentrations of the individual IgG subclasses, different affinities of reagents, and the relative abundance of each subclass. 34 , 47 , 48 Finally, virtually all patients present with a mixture of HLA DSA subclasses. All of these aforementioned issues make it difficult to draw robust conclusions regarding mechanisms of injury related to a given subclass of DSA and their individual impact on transplant outcome.
Gaps requiring further research:
Development of analytically validated reagents to study different strengths/titers of IgG antibody subclass in the context of commercially available HLA antibody testing platforms.
Longitudinal analyses of HLA antibody subclasses are needed, given that this is a dynamic and responsive biological system.
The mechanisms of graft injury by different subclasses are unknown and need to be confirmed in experimental transplant models and in situ in allografts. This is required for assessing treatment strategies aimed at manipulating IgG subclass diversity.
3.3. HLA antibody and outside‐in signaling
Crosslinking of HLA molecules is a universal function of HLA class I and II antibodies irrespective of subclass. Crosslinking triggers outside‐in signal transduction and endothelial cell survival, proliferation, and migration, as evidenced by in vitro and in vivo models. 49 , 50 , 51 , 52 , 53 , 54 The mechanisms have been studied and described to include the Src/FAK/Rho pathways. 55 , 56 More recently, signaling downstream of HLA crosslinking has also been demonstrated in parenchymal epithelial cells. 52 It has been shown that the capacity for HLA antibodies to induce outside‐in signaling is dependent on the level of HLA antigen expression on graft cells and on HLA antibody titer and affinity/avidity. Experimental evidence highlights signaling pathways in vascular cells downstream of HLA class II molecules. 51 , 57 The mTOR signaling axis that is activated by HLA class I and class II antibodies represents a potential diagnostic criterion for AMR and a therapeutic target to reduce endothelial cell activation during AMR. However, the relative role that outside‐in signaling pathways play in determining patient outcomes remains to be studied in vivo.
Gaps requiring further research:
There is a need to determine which qualitative aspects of HLA‐DSA (IgG subclasses, titer, and specificities) are most relevant to the in vivo function (i.e., leukocyte recruitment, cell survival, cell proliferation amd migration, complement activation) and the pathology caused.
Correlation of signaling pathways identified in experimental models with the wealth of information arising from transcriptomic characterization of human transplant biopsies undergoing rejection.
Determining whether the outside‐in signaling pathways are also inducted following recognition by an Fc receptor–positive cell remains unknown.
3.4. Leukocyte recruitment, microcirculation inflammation, and recipient Fc receptor genotype
A hallmark of AMR across all solid organ transplants is the presence of intracapillary inflammatory cells in the allograft. 28 Interactions between endothelial‐bound HLA IgG antibodies and myeloid and NK cell FcγRs can facilitate tethering and adhesion of leukocytes. Endothelial cells exposed to HLA antibodies produce cytokines and growth factors that can signal in an autocrine and paracrine manner and promote inflammation. 58 , 59 Data from in vitro experimental assays indicate that FCGR2A polymorphisms on monocytes govern interactions with distinct HLA IgG subclasses. 60 Similarly, the FcγRIIIA V158 high‐affinity allele (CD16a) expressed on NK cells could enhance the ability of anti‐HLA DSA to trigger inflammation in the microcirculation, resulting in adverse allograft outcomes. 28 , 61
Gaps requiring further research:
Studies are needed to understand the mechanistic role of intravascular leukocytes in antibody‐mediated acute and chronic graft injury and the interplay between HLA DSA titer, subclass, activated complement split products, Fc receptor polymorphism, and mechanisms of graft injury by microcirculation inflammation.
Larger prospective studies are needed to assess the effect of signal transduction inhibitors and other mediators of antibody‐FcγR signaling pathways in active and chronic AMR and define the impact of FcγR polymorphisms on leukocyte recruitment and long‐term graft outcomes.
4. ALLO‐SPECIFIC B AND T CELL IMMUNE MEMORY
Although HLA antibodies in the circulation pose best known apparent and immediate risk to the allograft, many patients may harbor adaptive memory T and B cell responses that, at the time of clinical consideration, are not apparent. STAR 2017 identified the lack of available assays to robustly detect B and T cell memory that have the potential to rapidly mount allo‐specific responses as a significant gap. Here we provide a more in‐depth summary of available assays.
4.1. B cells
Current assays to determine prior sensitization to HLA antigen measure preformed circulating HLA antibodies (IgG). This reflects antibody production by long‐lived plasma cells in the bone marrow and/or ongoing generation of short‐lived plasma cells. Yet, humoral sensitization that resulted in the generation of memory B cells that are capable of mounting an amnestic response early posttransplant remain undetected. 62 , 63 , 64 When driven into recall responses, the majority of memory B cells rapidly convert into antibody‐secreting cells (ASCs) and produce highly specific HLA antibodies, leading to acute AMR. 64 Prior sensitizing events resulting in HLA antibody generation may have occurred decades before transplant assessment, and as such, the breadth and strength of antibodies detected in the circulation may not reflect the breadth and depth of plasma cells or memory B cells that had been generated at the time of antigen exposure. In addition, loss of plasma cells or memory B cells may independently occur over time. 65 , 66 Finally, there is a qualitative difference in affinity between memory B cells that tend to have lower B cell receptor affinity compared with antibodies produced by plasma cells (Table 3). 67
Table 3.
Memory B cell assays
| Assay | Expected utility | Pros | Cons | Research tool | Analytic validity | Clinical validity | Clinical utility |
|---|---|---|---|---|---|---|---|
| Quantifying the frequency of HLA‐binding memory B cells by flow‐cytometry | Quantification of memory B cells for specific HLA targets (ie, anti‐donor) | Relatively rapid assay | Requires a wide range of reagents, either as HLA tetramers of single‐HLA coated beads in a multiplex format; limited sensitivity when frequency of HLA‐specific memory B cells is low; assay does not provide information about antibody‐secreting capacity of the memory B cells; potential nonspecific binding similar to the SAB‐antibody detection assay, and may require extraction from biopsies | ✓ | N/D | N/D | N/D |
| In vitro differentiation of memory B cells into ASCs; assessment of anti‐HLA IgG in culture supernatant | Evaluating the functional importance of memory B cells and secreted antibodies in determining graft outcome | Once B memory B cells matured into ASC in culture—simple detection of secreted HLA Abs by SAB assay | Requires 6‐10 d in‐vitro culture; assumes all ASC secrete the same amount of HLA Abs; low sensitivity for low frequency memory B cells. Potentially require extraction from biopsies | ✓ | N/D | N/D | N/D |
| In vitro differentiation of memory B cells into ASCs; assessment of HLA‐specific ASCs by ELISPOT or fluorospot assay | Evaluating the functional importance of memory B cells in determining graft outcome | Enumerate HLA‐specific memory B cells capable to differentiate into ASC | Requires 6‐10 d culture; need a complete repertoire of HLA Class I and Class II molecules for the ELISPOT assay; expensive and labor intensive. Potentially require extraction from biopsies | ✓ | N/D | N/D | N/D |
Abbreviations: ASC, antibody secreting cell; N/D, not demonstrated.
Reliable means to detect the presence of allo‐specific memory B cells before transplant many have the potential to transform our ability to risk‐stratify patients and individualize immunosuppression and monitoring protocols, and several assays are under investigation. Flow cytometry–based assays using single HLA antigen–coated beads or multimers for detecting antigen‐specific B cells are conceptually straightforward and can be rapidly performed. However, there are significant technical challenges preventing the rapid application of these assay for use in the clinic, including the lack of a broad array of HLA multimers, challenges in defining the conditions that allow for the specific identification of low‐frequency donor‐specific B cells, preventing nonspecific binding to the HLA multimers or HLA‐coated beads, and addressing the potential issue of B cell polyreactivity. Importantly, these assays have not been shown to be able to reliably and specifically quantify the frequency of memory HLA‐reactive B cells in humans. 64 , 68 , 69 , 70 , 71 , 72
Other studies have attempted to differentiate memory B cells into ASCs in vitro, followed by quantification of the resulting ASCs in an IgG ELISpot assay, or measurement of donor‐specific antibodies in the culture supernatant as surrogate measures of the frequency of memory B cells. With these assays, it is important to remember that the HLA antibody concentration in the culture supernatant may not necessarily correspond to the frequency of the in vitro differentiated memory B cell, as it is possible that each plasma cell secretes different amounts of HLA antibody. In addition, such assays require 6‐10 days of culture of the memory B cells for inducing in vitro differentiation, making these assays less practical when clinical results are required in a short time frame. On the other hand, potential recipients of a living‐donor transplant may benefit from such detailed quantification of memory B cell frequency. The use of an in vitro memory B cell ELISpot assay to inform risk of AMR was recently evaluated in kidney transplant recipients. 69 , 73 Multivariate analysis showed that pretransplant and posttransplant DSAs and frequency of donor reactive memory B cell were independent predictors of AMR. To this point, 21 of 29 patients with chronic AMR were DSA negative at the time of AMR diagnosis but had detectable donor reactive memory B cells. 69 These data suggest that monitoring donor‐reactive memory B cells may be a useful complement to DSA quantification in order to accurately predict or diagnose AMR after kidney transplant.
Gaps requiring further research:
Development of rapid, reliable, and clinically feasible assays to determine the frequency of anti‐HLA memory B cells (need to determine whether this can this be achieved using peripheral blood or requires sampling of certain niches)
Design studies to assess predictive value of circulating anti‐donor HLA memory B cell frequencies and transplant outcome
4.2. T cells
Seminal studies showed that the frequencies of donor‐specific IFNγ‐secreting memory T cells measured via ELISpot correlated with risk of rejection in both nonhuman primates (NHPs) 74 , 75 and human renal, but not heart, studies. 76 , 77 However, this approach has yet to be translated into clinical use in part due to the technical difficulty of standardizing this assay and the time needed to generate results (6‐24 hours). The panel‐reactive T cell (PRT) assay is more feasible currently in that it measures memory T cell alloreactivity against a panel of target cells expressing distinct HLA molecules, thus allowing the test to be run before the identification of a donor. 78 Still, recent studies suggest that IFNγ secretion may identify only a small subset of antigen‐specific T cells, 79 and these assays largely measure direct antigen recognition of native HLA molecules that may be less predictive of pathologic immune responses relative to measures of indirect recognition by HLA antigens processed and presented by recipient APCs. 80 , 81 These limitations thus present challenges for the clinical implementation of these assays as measures of pretransplant donor reactivity (Table 4).
Table 4.
Memory T cell assays
| Assay | Expected utility | Pros | Cons | Research tool | Analytic validity | Clinical validity | Clinical utility |
|---|---|---|---|---|---|---|---|
| Quantifying frequency of DONOR‐HLA‐specific, IFNγ‐secreting memory T cells | Assess the functional importance of memory T cells in determining graft outcomes | Quantification of memory T cells that are specific for donor antigens | Requires 6‐24 h and is technically difficult; quantification is based on a single read‐out (IFNγ production); measures only direct presentation | ✓ | N/D | N/D | N/D |
| Panel reactive T cell (PRT) Assay—quantifying frequency of any HLA specific IFNγ‐secreting memory T cells | Risk stratification to “high” vs “low”. If panel is large enough—may determine broad specificities | Quantification of memory T cells that are specific for HLA antigens in general | Requires 6‐24 h and is technically difficult; quantification is based on a single read‐out (IFNγ production); measures only direct presentation | ✓ | N/D | N/D | N/D |
| Measurement of bulk memory T cell immunophenotypic signature | Risk stratification to “high” vs “low” | Simple cell surface flow cytometric assay that could easily be performed by a clinical lab | Does not measure donor‐reactive memory T cells. Not specific even for HLA targets | ✓ | N/D | N/D | N/D |
| Follicular helper T cells—TfH | Monitoring of newly developed memory T cells leading to generation of donor‐specific B cells and antibody responses | Quantification of memory T cells that are specific for donor antigens | Circulating Tfh may not reflect the full spectrum of Tfh responses; may require use of LN fine needle aspirates | ✓ | N/D | N/D | N/D |
| Flow cytometric analysis using peptide:HLA tetramer technology | May be the most useful assay for capturing both quantity and quality of memory T cell risk profile | Provide quantification as well as specificity | Requires knowledge of the specific peptide targets commonly found in alloreactivity (may be overcome with the use of CLIP?) | ✓ | N/D | N/D | N/D |
Abbreviation: N/D, not demonstrated.
In parallel, several groups have taken the alternate approach of attempting to define immunophenotypes of bulk (non–donor‐specific) memory T cell populations to assess a given patient's overall “memory T cell risk” for rejection. For example, 2 recent studies identified a memory T cell signature that was associated with risk of acute rejection in kidney recipients treated by costimulation blockade using belatacept. 82 , 83 Studies showed that patients who went on to reject their grafts exhibited a higher frequency of CD8+CD28+TEM than those who were stable on belatacept. A potentially related population of CD57+PD‐1lo cells was also found to correlate with risk of belatacept‐resistant rejection. 84 Similar to the PRT assay, the use of bulk memory T cell immunophenotypic signatures to stratify patient risk will not provide information on donor‐specific memory T cell compartment.
Follicular helper T cells (Tfh) are of particular interest for monitoring newly developed memory T cells, as these cells provide critical signals for the generation of donor‐specific B cell and antibody responses. 85 Recent studies in human renal transplant recipients have confirmed that circulating Tfh are generated and detectable in patients who develop DSAs. 86 However, they may not reflect the full magnitude of the Tfh response that exists in the draining lymph nodes (LNs). 79 Fine needle aspirates can detect LN Tfh via cytokine‐independent activation‐induced marker (AIM) assay. 79 While fine needle aspirate assays on patient lymph nodes presents a major logistical challenge, the AIM assay for Tfh measurement has shown some utility in the blood. 79
Gaps requiring further research:
Develop a rapid, reliable, and clinically feasible assay to determine whether anti‐HLA memory T cells exist, their frequencies, and whether they recognize donor antigens via the direct or the indirect pathway.
Expand tools to study Tfh (potentially with emphasis on fine needle aspirates).
Design studies to assess potential correlation between circulating anti‐HLA memory T cells and transplant outcome.
5. PRIMARY (NAÏVE OR DE NOVO) ALLO‐IMMUNE RESPONSE
5.1. HLA molecular mismatch and immunogenicity
HLA immunogenicity is a consequence of reactivity at both the cellular (T cell alloreactivity) and the humoral (B cell alloreactivity) levels, as these immune responses are interdependent and intrinsically linked. 87 , 88 Advances in the science of B/T cell receptor interaction with their target ligands (i.e., epitopes) led to the development of computational modeling approaches to predict potential T cell immunizing epitopes in the context of cancer therapy, vaccine development, etc. and specifically for the field of transplantation—surmizing donor HLA allo‐epitopes recognized by recipient B/T cells.
The principal hypothesis underpinning this theoretical approach to predicting the risk of development of primary alloimmunity is that HLA allorecognition by recipient B/T cells is more likely the more ‘different’ the donor HLA compared with recipient HLA molecules. 89 Thus, current computational algorithms aim to quantify a measure of “dissimilarity” between donor and recipient HLA—the HLA Molecular Mismatch (mMM) Score. The most common approaches include HLA Matchmaker, Electrostatic Mismatch Score (EMS), 90 , 91 , 92 , 93 PIRCHE®, 94 and a simple count of amino acid mismatches. A comparison between the different methods is presented in Table 5. To date, correlations have been demonstrated by all of these computational approaches with differences at the sequence level. 89 , 91
Table 5.
Moleulcar mismatch calculation approaches
| Assay | Description |
|---|---|
| HLA matchmaker | This is the first theoretical algorithm to emphasize that HLA antibodies recognize only a portion of an antigen, corresponding to the contact area between them (epitope/complementary‐determining region [CDR] structure). HLA Matchmaker, developed by Rene Duquesnoy, uses donor/recipient amino acid sequences to determine continuous and discontinuous “eplets” that are likely part of the area recognized by an antibody's CDR. HLAMatchmaker focuses only on polymorphic regions and provides information regarding “verified” and “non‐verified” epitopes. All mismatched eplets are assigned the same value for a sum of eplet mismatch load. Multiple versions of the software are available, either on Duquesnoy's website (free of charge) or as part of different SAB analysis software—with differences between the versions, not easily identified or reported by the users. While the software declares “verified” from “non‐verified” “epitopes”—it is not clear what “verification” means. Most of these “epitopes” were not tested, nor confirmed, by absorption elution experiments. Additionally, the standard Matchmaker approaches relates to both recipient alleles as a single entity, and to both donor alleles as a singel allo‐entity (this is not a physiologic representation of how HLA antigens are expressed on a cell surface) |
| Electrostatic Mismatch Score (EMS) | This approach measured the physiochemical properties and the unique surface electrostatic value of the different amino acids forming the HLA molecule. It therefore provides a measure of variance between physiochemical properties of donor and recipient alleles beyond the pure number, or mismatch load comparison. The EMS software was developed by Vasilis Kosmoliaptsis and has 2 versions. EMS‐2D is available for download free of charge. EMS‐3D was developed recently |
| Predicted Indirectly ReCognizable HLA Epitopes presented by recipient HLA‐Class II antigens = PIRCHE‐II | PIRCHE ® approach adds the complexity of processes associated with indirect presentation to recipient T cells. PIRCHE‐II uses algorithms to predict which peptides derived from donor HLA antigens can be presented in the context of recipient HLA‐DR molecules. Given that T cell help is required to activate B cell responses, this approach may provide information beyond the previously described approaches. The algorithm in its current format does not consider the role of HLA‐DQαβ, DPαβ, and DRβ3/4/5 in antigen presentation. It also uses a relatively low stringency to define “presentable” peptides and thus may lack sufficient specificity. PIRCHE® is available as a commercial software |
| Amino acid sequence comparison | Donor and recipient HLA alleles are converted into the corresponding amino acid sequences and the number of mismatches are enumerated. Similar to eplet analysis, this approach does not assign potential values regarding immunogenicity of different amino acid mismatches. However, it does not make a priori assumptions regarding which areas of the molecule may be more relevant for antibody recognition. Compared with all other approaches, this is the simplest approach with the least potential bias in analysis |
There is a body of evidence in support of the utility of HLA mMM score as a basis for primary alloimmunity risk stratification. Wiebe et al 95 demonstrated that in a naive kidney transplant cohort, the sum of the HLA‐DR or ‐DQ mMM scores for the DR and DQ loci (regardless if determined by eplet MM, amino acid MM, or electrostatic MM) is an independent correlate of de novo DSA to HLA‐DR or ‐DQ. 91 Notably, HLA eplet mMM evaluation of each individual HLA‐DR/DQ mismatched molecule is better associated with de novo DSA development against that unique mismatch compared with approaches that sum all HLA mMM scores at a given HLA locus. 96 In this study, patients could be assigned to a low, intermediate, or high primary alloimmune risk category using HLA mMM thresholds derived for all HLA‐DRβ1/3/4/5 and HLA‐DQα1/β1 molecules. Finally, in 3 independent cohorts, the DR or DQ HLA mMM score correlated with the level of calcineurin inhibitor–based immunosuppression required to control primary alloimmunity. 97 , 98 Based on this body of work, the FDA Center for Drug Evaluation and Research agreed to evaluate the potential role of HLA‐DR/DQ eplet mMM score as a strategy for enrichment or risk stratification in phase 2 and 3 kidney transplant clinical drug development trials and as a prognostic biomarker for de novo DSA, graft rejection, and graft failure. 99 Whether eplet mMM or single molecule HLA‐DR or ‐DQ eplet mMM scores can be used to guide risk stratification for personalized immunosuppression requires proof through prospective clinical trials, because different investigators report different risk thresholds. 100 , 101 , 102 , 103
Although a strong correlation exists between increased mMM and de novo DSA, some of the patients do develop de novo DSA despite having a low HLA mMM score. 101 , 103 This emphasizes that certain mMM may have a higher immunogenic impact compared with other mMM and that not all mMM should be assigned the same immunogenic value. An approach to investigate immunogenicity was recently published by Tambur et al. 101 Without clear understanding of the immunogenic value of each mismatch, mMM evaluation is far from being optimized for consideration in allocation schemes and may be premature for use other than design/enrichment of clinical trials.
Gaps requiring further research:
Currently, there are multiple approaches to calculate mMM. Approaches need to be optimized and algorithms should be standardized such that they can be locked before implementation in clinical practice.
Thresholds for risk categories need to be established and the impact of other factors on these thresholds need to be accounted for (e.g., recipient age, race, etc.). Formal evaluation, in prospective clinical trials, should be performed before clinical grade recommendations can be made.
Tools to prospectively determine donor/recipient HLA specific immunogenicity beyond the mismatch load (given that DSA can be developed in some patients with low HLA mMM score) should be developed. This is essential before considering evaluation and implementation of immunogenicity analysis as a guide to organ allocation schemes.
5.2. Genetic modifiers of alloimmunity
Genome‐wide studies have focused on gene polymorphisms in both recipient and donor and their association with transplant outcome (for a review, see ref. 104). Multiple single nucleotide polymorphisms (SNPs) have been identified in association with allograft renal function 105 although disputed on further study. 106 Donor polymorphisms have also been identified associated with allograft survival. 107 , 108 There have also been associations with protection against allograft loss and NF‐κB1. 109 A more comprehensive review of these associations is presented by Dorr et al 104 and Hernandez‐Fuentes et al. 110
Despite a large body of published data, there is a lack of concordance across genetically varied transplant populations and with differences in disease phenotype definition such as serum creatinine or specific pathological diagnoses whose criteria change periodically. 111 , 112 Similarly, the effect of individual gene variants is generally relatively small, and it is likely that few are obligatory for the outcome to occur. 113 Complexity is further compounded by the potential genetic interaction of donor and recipient factors and additional studies are required. An approach of “loss of function compatibility” 114 is suggested by the international consortium iGeneTRAiN, the International Genetics and Translational Research in Transplantation Network.
SNPs have been identified not only in immune response genes but also in other genes associated with drug metabolism. 115 Studies primarily focused on CNI metabolism hypothesize that achieving specific immunosuppression target level quickly may be associated with improved transplant outcomes, although this has not been proved definitively. 116 , 117 Similarly, there have been SNP associations with IMPDH and RNA metabolism affecting mycophenolate levels 118 and associated with acute rejection 119 or associated with harmful toxicities such leukopenia and anemia, 120 which are dose limiting. Recent meta‐analysis of pharmacogenomics markers suggests a positive impact in transplant management. 121 However, until definitive prospective trial data indicate that proper early dosing minimizes adverse events, further adoption of such markers is unlikely to have a clinical impact.
In summary, the study of genetic variation influencing the quality of the alloimmune response is likely to expand significantly in the coming years as the cost of genome‐wide studies decrease and technologies become more accessible. This will be driven by the potential benefit of validated SNPs for either susceptibility/risk biomarker or predictive biomarker as a guide for more precise prescription of immunosuppressive load to avoid harmful side effects of either overimmunosuppression or underimmunosuppression.
Gaps requiring further research:
Prospective clinical trials are needed to validate the impact of potential immunoregulatory SNPs on modulating the immune response before they can be adopted as routine susceptibility/risk biomarkers.
Prospective clinical trials are needed to determine the impact of polymorphism‐directed drug dosing, and dosing equations exist that can be used. 122 , 123
6. ROADMAP AND FUTURE DIRECTIONS
While the goal of the STAR 2019 working group was to provide an up‐to‐date, high stringency, critique of transplant‐related assays used to inform laboratory and nonlaboratory clinicians, it was not meant to discourage them from pursuing best standards of care for their patients. The STAR working group believes that it is imperative for clinicians to have in‐depth understanding of both the value and limitations of the assays in order to be better informed as to how to use the results clinically, in the current time. The need to pause and reexplore the value and wisdom of current practices is the hallmark of improving patient care. The ability to use current knowledge to reevaluate and, if needed, criticize some of the older highly cited works, can provide valuable insights. Only by doing so will our field come together to navigate toward faster future innovations.
We are currently at an intersection between rapid offering of new assays (and better understanding on how to use and interpret currently available ones) and the slow accumulation of prospective transplant outcome data (with the need to have 5‐10 years of follow‐up). Intense efforts by the Transplant Therapeutic Consortium and Paris Transplant Group are seeking to shorten this time through the development of validated surrogate composite endpoints for clinical trials (e.g., iBOX). 124 , 125 However, in the interim at this critical juncture, it may require some “out of the box” thinking on how to best use our existing resources. More collaborative efforts and less aversion to retrospective analysis, where samples were collected prospectively in a systematic fashion, should be considered. The past decade had seen many National Institutes of Health–sponsored Clinical Trials in Organ Transplantation, where samples were collected both for testing and biobanked for future use. HLA‐related testing were performed for some of these studies, using best practices for that time, but as recommended by STAR 2017, HLA typing should be performed at a high resolution for both donor and recipient, and antibody testing should use measures to overcome limitations of the SAB assays (e.g., removal of inhibition, etc.), in order to more accurately interpret the data. Further, we now appreciate the need for adjudication of some of the SAB testing rather than using an arbitrary MFI value for a threshold in all cases. Until such efforts take place, the STAR 2019 provide the following recommendation as an immediate call for action (summarized in Figure 2).
6.1. Plans for STAR 2021
Planning for STAR 2021 will commence in early 2020. In response to feedback from the transplant community we plan to add a couple of topics, specifically looking at tests evaluating role of non‐HLA antibodies, and tests in support of assigning HLA antibody strength (to aid pretransplant desensitization decision‐making and treatment efficacy monitoring, including treatment of AMR posttransplant). As before, STAR 2021 working groups will reevaluate categories that were discussed in this report to provide progress if available. Special emphasis will be given to organs beyond kidneys (with the hope that sufficient literature will be available by that time). We encourage those who are interested in actively being involved with the STAR process to contact the corresponding author.
DISCLOSURE
The authors of this manuscript have no conflicts of interest to disclose as described by the American Journal of Transplantation.
FUNDING
This study was sponsored by the National Institute of Allergy and Infectious Diseases, American Society of Histocompatibility and Immunogenetics, American Society of Transplantation, and Paul Terasaki Research Fund.
ACKNOWLEDGMENTS
The authors thank the American Scoeity of Transplantation for logistical assistance.
Tambur AR, Campbell P, Chong AS, et al. Sensitization in transplantation: Assessment of risk (STAR) 2019 Working Group Meeting Report. Am J Transplant. 2020;20:2652–2668. 10.1111/ajt.15937
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
REFERENCES
- 1. Axelrod DA, Naik AS, Schnitzler MA, et al. National variation in use of immunosuppression for kidney transplantation: a call for evidence‐based regimen selection. Am J Transplant. 2016;16(8):2453‐2462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Dharnidharka VR, Naik AS, Axelrod DA, et al. Center practice drives variation in choice of US kidney transplant induction therapy: a retrospective analysis of contemporary practice. Transpl Int. 2018;31(2):198‐211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Tambur AR, Campbell P, Claas FH, et al. Sensitization in transplantation: assessment of risk (STAR) 2017 working group meeting report. Am J Transplant. 2018;18(7):1604‐1614. [DOI] [PubMed] [Google Scholar]
- 4. Tambur AR, Herrera ND, Haarberg KMK, et al. Assessing antibody strength: comparison of MFI, C1q, and titer information. Am J Transplant. 2015;15(9):2421‐2430. [DOI] [PubMed] [Google Scholar]
- 5. Tambur AR, Wiebe C. HLA diagnostics: evaluating DSA strength by titration. Transplantation. 2018;102(1S Suppl 1):S23‐S30. [DOI] [PubMed] [Google Scholar]
- 6. Manski CF. Patient Care Under Uncertainty. Princeton, NJ: Princeton University Press; 2019. [Google Scholar]
- 7. Manski CF. Credible ecological inferences for medical decisions with personalized risk assessment. Quant Econ. 2018;9(20):541‐569. [Google Scholar]
- 8. Dickersin K, Chalmers I. Recognizing, investigating and dealing with incomplete and biased reporting of clinical research: from Francis Bacon to the WHO. J R Soc Med. 2011;104(12):532‐538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kicinski M, Springate DA, Kontopantelis E. Publication bias in meta‐analyses from the Cochrane Database of Systematic Reviews. Stat Med. 2015;34(20):2781‐2793. [DOI] [PubMed] [Google Scholar]
- 10. Luijendijk HJ, Koolman X. The incentive to publish negative studies: how beta‐blockers and depression got stuck in the publication cycle. J Clin Epidemiol. 2012;65(5):488‐492. [DOI] [PubMed] [Google Scholar]
- 11. Manski CF. Reasonable patient care under uncertainty. Health Econ. 2018;27(10):1397‐1421. [DOI] [PubMed] [Google Scholar]
- 12. Valenzuela NM, Reed EF. Antibodies in transplantation: the effects of HLA and non‐HLA antibody binding and mechanisms of injury. Methods Mol Biol. 2013;1034:41‐70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Reed EF, Rao P, Zhang Z, et al. Comprehensive assessment and standardization of solid phase multiplex‐bead arrays for the detection of antibodies to HLA. Am J Transplant. 2013;13(7):1859‐1870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Tait BD. Detection of HLA antibodies in organ transplant recipients ‐ triumphs and challenges of the solid phase bead assay. Front Immunol. 2016;7:570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Viglietti D, Loupy A, Vernerey D, et al. Value of donor‐specific anti‐HLA antibody monitoring and characterization for risk stratification of kidney allograft loss. J Am Soc Nephrol. 2017;28(2):702‐715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Valenzuela NM, McNamara JT, Reed EF. Antibody‐mediated graft injury: complement‐dependent and complement‐independent mechanisms. Curr Opin Organ Transplant. 2014;19(1):33‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Chin C, Chen GE, Sequeria F, et al. Clinical usefulness of a novel C1q assay to detect immunoglobulin G antibodies capable of fixing complement in sensitized pediatric heart transplant patients. J Heart Lung Transplant. 2011;30(2):158‐163. [DOI] [PubMed] [Google Scholar]
- 18. Sicard A, Ducreux S, Rabeyrin M, et al. Detection of C3d‐binding donor‐specific anti‐HLA antibodies at diagnosis of humoral rejection predicts renal graft loss. J Am Soc Nephrol. 2015;26(2):457‐467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Takeda A, Otsuka Y, Horike K, et al. Significance of C4d deposition in antibody‐mediated rejection. Clin Transplant. 2012;26(Suppl 24):43‐48. [DOI] [PubMed] [Google Scholar]
- 20. Loupy A, Lefaucheur C, Vernerey D, et al. Complement‐binding anti‐HLA antibodies and kidney‐allograft survival. N Engl J Med. 2013;369(13):1215‐1226. [DOI] [PubMed] [Google Scholar]
- 21. Bouquegneau A, Loheac C, Aubert O, et al. Complement‐activating donor‐specific anti‐HLA antibodies and solid organ transplant survival: a systematic review and meta‐analysis. PLoS Medicine. 2018;15(5):e1002572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Wiebe C, Gareau AJ, Pochinco D, et al. Evaluation of C1q status and titer of de novo donor‐specific antibodies as predictors of allograft survival. Am J Transplant. 2017;17(3):703‐711. [DOI] [PubMed] [Google Scholar]
- 23. Yell M, Muth BL, Kaufman DB, Djamali A, Ellis TM. C1q binding activity of de novo donor‐specific HLA antibodies in renal transplant recipients with and without antibody‐mediated rejection. Transplantation. 2015;99(6):1151‐1155. [DOI] [PubMed] [Google Scholar]
- 24. Zachary AA, Lucas DP, Detrick B, Leffell MS. Naturally occurring interference in Luminex assays for HLA‐specific antibodies: characteristics and resolution. Hum Immunol. 2009;70(7):496‐501. [DOI] [PubMed] [Google Scholar]
- 25. Diebolder CA, Beurskens FJ, de Jong RN, et al. Complement is activated by IgG hexamers assembled at the cell surface. Science. 2014;343(6176):1260‐1263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Guidicelli G, Anies G, Bachelet T, et al. The complement interference phenomenon as a cause for sharp fluctuations of serum anti‐HLA antibody strength in kidney transplant patients. Transpl Immunol. 2013;29(1–4):17‐21. [DOI] [PubMed] [Google Scholar]
- 27. Comoli P, Cioni M, Tagliamacco A, et al. Acquisition of C3d‐binding activity by de novo donor‐specific HLA antibodies correlates with graft loss in nonsensitized pediatric kidney recipients. Am J Transplant. 2016;16(7):2106‐2116. [DOI] [PubMed] [Google Scholar]
- 28. Lefaucheur C, Viglietti D, Hidalgo LG, et al. Complement‐activating anti‐HLA antibodies in kidney transplantation: allograft gene expression profiling and response to treatment. J Am Soc Nephrol. 2018;29(2):620‐635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Lan JH, Tinckam K. Clinical utility of complement dependent assays in kidney transplantation. Transplantation. 2018;102(1S Suppl 1):S14‐S22. [DOI] [PubMed] [Google Scholar]
- 30. Claisse G, Absi L, Cognasse F, Alamartine E, Mariat C, Maillard N. Relationship between Mean fluorescence intensity and C1q/C3d‐fixing capacities of anti‐HLA antibodies. Hum Immunol. 2017;78(4):336‐341. [DOI] [PubMed] [Google Scholar]
- 31. Honger G, Amico P, Arnold ML, Spriewald BM, Schaub S. Effects of weak/non‐complement‐binding HLA antibodies on C1q‐binding. HLA. 2017;90(2):88‐94. [DOI] [PubMed] [Google Scholar]
- 32. Barba T, Harb J, Ducreux S, et al. Highly variable sialylation status of donor‐specific antibodies does not impact humoral rejection outcomes. Front Immunol. 2019;10:513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Vidarsson G, Dekkers G, Rispens T. IgG subclasses and allotypes: from structure to effector functions. Front Immunol. 2014;5:520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Lowe D, Higgins R, Zehnder D, Briggs DC. Significant IgG subclass heterogeneity in HLA‐specific antibodies: implications for pathogenicity, prognosis, and the rejection response. Hum Immunol. 2013;74(5):666‐672. [DOI] [PubMed] [Google Scholar]
- 35. Ponsirenas RVG, Cazarote HB, Araújo SDA, et al. Anti‐HLA donor‐specific IgG subclasses and C1q‐binding evolution in posttransplant monitoring. Transplant Direct. 2018;4(9):e385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Lefaucheur C, Viglietti D, Bentlejewski C, et al. IgG donor‐specific anti‐human HLA antibody subclasses and kidney allograft antibody‐mediated injury. J Am Soc Nephrol. 2016;27(1):293‐304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Arnold ML, Ntokou IS, Doxiadis II, Spriewald BM, Boletis JN, Iniotaki AG. Donor‐specific HLA antibodies: evaluating the risk for graft loss in renal transplant recipients with isotype switch from complement fixing IgG1/IgG3 to noncomplement fixing IgG2/IgG4 anti‐HLA alloantibodies. Transpl Int. 2014;27(3):253‐261. [DOI] [PubMed] [Google Scholar]
- 38. Gao ZH, McAlister VC, Wright JR Jr, McAlister CC, Peltekian K, MacDonald AS. Immunoglobulin‐G subclass antidonor reactivity in transplant recipients. Liver Transpl. 2004;10(8):1055‐1059. [DOI] [PubMed] [Google Scholar]
- 39. Khovanova N, Daga S, Shaikhina T, et al. Subclass analysis of donor HLA‐specific IgG in antibody‐incompatible renal transplantation reveals a significant association of IgG4 with rejection and graft failure. Transpl Int. 2015;28(12):1405‐1415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Kaneku H, O'Leary JG, Taniguchi M, Susskind BM, Terasaki PI, Klintmalm GB. Donor‐specific human leukocyte antigen antibodies of the immunoglobulin G3 subclass are associated with chronic rejection and graft loss after liver transplantation. Liver Transpl. 2012;18(8):984‐992. [DOI] [PubMed] [Google Scholar]
- 41. Jackson AM, Kanaparthi S, Burrell BE, et al. IgG4 donor‐specific HLA antibody profile is associated with subclinical rejection in stable pediatric liver recipients. Am J Transplant. 2020;20:513‐524. [DOI] [PubMed] [Google Scholar]
- 42. Berkowska MA, Driessen GJA, Bikos V, et al. Human memory B cells originate from three distinct germinal center‐dependent and ‐independent maturation pathways. Blood. 2011;118(8):2150‐2158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Ottesen EA, Skvaril F, Tripathy SP, Poindexter RW, Hussain R. Prominence of IgG4 in the IgG antibody response to human filariasis. J Immunol. 1985;134(4):2707‐2712. [PubMed] [Google Scholar]
- 44. Jackson KJ, Wang Y, Collins AM. Human immunoglobulin classes and subclasses show variability in VDJ gene mutation levels. Immunol Cell Biol. 2014;92(8):729‐733. [DOI] [PubMed] [Google Scholar]
- 45. van Zelm MC. B cells take their time: sequential IgG class switching over the course of an immune response? Immunol Cell Biol. 2014;92(8):645‐646. [DOI] [PubMed] [Google Scholar]
- 46. Cicciarelli JC, Lemp NA, Chang Y, et al. Renal transplant patients biopsied for cause and tested for C4d, DSA, and IgG subclasses and C1q: which humoral markers improve diagnosis and outcomes? J Immunol Res. 2017;2017:1652931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Pinelli DGM, Joong A, Thrush P, Tambur A. Temporal variability of IgG subclasses. Am J Transplant. 2017;17(Suppl 3):A130. [Google Scholar]
- 48. Warner PGI, Youngs DA, Zimring J. Next generation HLA antibody reagents. Hum Immunol. 2017;78:16.27743878 [Google Scholar]
- 49. Valenzuela NM, Trinh KR, Mulder A, Morrison SL, Reed EF. Monocyte recruitment by HLA IgG‐activated endothelium: the relationship between IgG subclass and FcgammaRIIa polymorphisms. Am J Transplant. 2015;15(6):1502‐1518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Jindra PT, Hsueh A, Hong L, et al. Anti‐MHC class I antibody activation of proliferation and survival signaling in murine cardiac allografts. J Immunol. 2008;180(4):2214‐2224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Jin YP, Valenzuela NM, Zhang X, Rozengurt E, Reed EF. HLA class II‐triggered signaling cascades cause endothelial cell proliferation and migration: relevance to antibody‐mediated transplant rejection. J Immunol. 2018;200(7):2372‐2390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Egelkamp J, Chichelnitskiy E, Kuhne JF, et al. Back signaling of HLA class I molecules and T/NK cell receptor ligands in epithelial cells reflects the rejection‐specific microenvironment in renal allograft biopsies. Am J Transplant. 2019;19(10):2692‐2704. [DOI] [PubMed] [Google Scholar]
- 53. Li F, Wei J, Valenzuela NM, et al. Phosphorylated S6 kinase and S6 ribosomal protein are diagnostic markers of antibody‐mediated rejection in heart allografts. J Heart Lung Transplant. 2015;34(4):580‐587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Lion J, Burbach M, Cross A, et al. Endothelial cell amplification of regulatory T cells is differentially modified by immunosuppressors and intravenous immunoglobulin. Front Immunol. 2017;8:1761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Salehi S, Sosa RA, Jin Y‐P, et al. Outside‐in HLA class I signaling regulates ICAM‐1 clustering and endothelial cell‐monocyte interactions via mTOR in transplant antibody‐mediated rejection. Am J Transplant. 2018;18(5):1096‐1109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Valenzuela NM, Mulder A, Reed EF. HLA class I antibodies trigger increased adherence of monocytes to endothelial cells by eliciting an increase in endothelial P‐selectin and depending on subclass, by engaging FcgammaRs. J Immunol. 2013;190(12):6635‐6650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Lion J, Taflin C, Cross AR, et al. HLA class II antibody activation of endothelial cells promotes Th17 and disrupts regulatory T lymphocyte expansion. Am J Transplant. 2016;16(5):1408‐1420. [DOI] [PubMed] [Google Scholar]
- 58. Sablik KA, Litjens NHR, Klepper M, Betjes MGH. Increased CD16 expression on NK cells is indicative of antibody‐dependent cell‐mediated cytotoxicity in chronic‐active antibody‐mediated rejection. Transpl Immunol. 2019;54:52‐58. [DOI] [PubMed] [Google Scholar]
- 59. Yazdani S, Callemeyn J, Gazut S, et al. Natural killer cell infiltration is discriminative for antibody‐mediated rejection and predicts outcome after kidney transplantation. Kidney Int. 2019;95(1):188‐198. [DOI] [PubMed] [Google Scholar]
- 60. Arnold ML, Fuernrohr BG, Weiss KM, Harre U, Wiesener MS, Spriewald BM. Association of a coding polymorphism in Fc gamma receptor 2A and graft survival in re‐transplant candidates. Hum Immunol. 2015;76(10):759‐764. [DOI] [PubMed] [Google Scholar]
- 61. Arnold ML, Kainz A, Hidalgo LG, et al. Functional Fc gamma receptor gene polymorphisms and donor‐specific antibody‐triggered microcirculation inflammation. Am J Transplant. 2018;18(9):2261‐2273. [DOI] [PubMed] [Google Scholar]
- 62. Crotty S, Aubert RD, Glidewell J, Ahmed R. Tracking human antigen‐specific memory B cells: a sensitive and generalized ELISPOT system. J Immunol Methods. 2004;286(1–2):111‐122. [DOI] [PubMed] [Google Scholar]
- 63. Crotty S, Ahmed R. Immunological memory in humans. Semin Immunol. 2004;16(3):197‐203. [DOI] [PubMed] [Google Scholar]
- 64. Lúcia M, Luque S, Crespo E, et al. Preformed circulating HLA‐specific memory B cells predict high risk of humoral rejection in kidney transplantation. Kidney Int. 2015;88(4):874‐887. [DOI] [PubMed] [Google Scholar]
- 65. Halliley J, Tipton C, Liesveld J, et al. Long‐lived plasma cells are contained within the CD19(‐)CD38(hi)CD138(+) subset in human bone marrow. Immunity. 2015;43(1):132‐145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Pape KA, Taylor JJ, Maul RW, Gearhart PJ, Jenkins MK. Different B cell populations mediate early and late memory during an endogenous immune response. Science. 2011;331(6021):1203‐1207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Weisel FJ, Zuccarino‐Catania GV, Chikina M, Shlomchik MJ. A temporal switch in the germinal center determines differential output of memory B and plasma cells. Immunity. 2016;44(1):116‐130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Luque S, Lúcia M, Melilli E, et al. Value of monitoring circulating donor‐reactive memory B cells to characterize antibody‐mediated rejection after kidney transplantation. Am J Transplant. 2019;19(2):368‐380. [DOI] [PubMed] [Google Scholar]
- 69. Luque S, Lucia M, Crespo E, Jarque M, Grinyo JM, Bestard O. A multicolour HLA‐specific B‐cell FluoroSpot assay to functionally track circulating HLA‐specific memory B cells. J Immunol Methods. 2018;462:23‐33. [DOI] [PubMed] [Google Scholar]
- 70. Snanoudj R, Claas FH, Heidt S, Legendre C, Chatenoud L, Candon S. Restricted specificity of peripheral alloreactive memory B cells in HLA‐sensitized patients awaiting a kidney transplant. Kidney Int. 2015;87(6):1230‐1240. [DOI] [PubMed] [Google Scholar]
- 71. Karahan GE, de Vaal YJ, Roelen DL, Buchli R, Claas FH, Heidt S. Quantification of HLA class II‐specific memory B cells in HLA‐sensitized individuals. Hum Immunol. 2015;76(2–3):129‐136. [DOI] [PubMed] [Google Scholar]
- 72. Lucas DP, Leffell MS, Zachary AA. Tetramer staining for the detection of HLA‐specific B cells. Methods Mol Biol. 2013;1034:313‐318. [DOI] [PubMed] [Google Scholar]
- 73. Karahan GE, de Vaal YJH, Krop J, et al. A Memory B Cell crossmatch assay for quantification of donor‐specific memory B cells in the peripheral blood of HLA‐immunized individuals. Am J Transplant. 2017;17(10):2617‐2626. [DOI] [PubMed] [Google Scholar]
- 74. Nadazdin O, Boskovic S, Murakami T, et al. Host alloreactive memory T cells influence tolerance to kidney allografts in nonhuman primates. Sci Transl Med. 2011;3(86):86ra51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Yamada Y, Boskovic S, Aoyama A, et al. Overcoming memory T‐cell responses for induction of delayed tolerance in nonhuman primates. Am J Transplant. 2012;12(2):330‐340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. Heeger PS, Greenspan NS, Kuhlenschmidt S, et al. Pretransplant frequency of donor‐specific, IFNgamma‐producing lymphocytes is a manifestation of immunologic memory and correlates with the risk of posttransplant rejection episodes. J Immunol. 1999;163(4):2267‐2275. [PubMed] [Google Scholar]
- 77. Starling RC, Stehlik J, Baran DA, et al. Multicenter analysis of immune biomarkers and heart transplant outcomes: results of the clinical trials in organ transplantation‐05 study. Am J Transplant. 2016;16(1):121‐136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Poggio ED, Clemente M, Hricik DE, Heeger PS. Panel of reactive T cells as a measurement of primed cellular alloimmunity in kidney transplant candidates. J Am Soc Nephrol. 2006;17(2):564‐572. [DOI] [PubMed] [Google Scholar]
- 79. Dan JM, Lindestam Arlehamn CS, Weiskopf D, et al. A cytokine‐independent approach to identify antigen‐specific human germinal center T follicular helper cells and rare antigen‐specific CD4+ T cells in blood. J Immunol. 2016;197(3):983‐993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Buhler L, Illigens BM, Nadazdin O, et al. Persistence of indirect but not direct T cell xenoresponses in baboon recipients of pig cell and organ transplants. Am J Transplant. 2016;16(6):1917‐1922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Marino J, Paster J, Benichou G. Allorecognition by T lymphocytes and allograft rejection. Front Immunol. 2016;7:582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Cortes‐Cerisuelo M, Laurie SJ, Mathews DV, et al. Increased pretransplant frequency of CD28+ CD4+ TEM predicts belatacept‐resistant rejection in human renal transplant recipients. Am J Transplant. 2017;17(9):2350‐2362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Mathews DV, Wakwe WC, Kim SC, et al. Belatacept‐resistant rejection is associated with CD28+ memory CD8 T cells. Am J Transplant. 2017;17(9):2285‐2299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Espinosa J, Herr F, Tharp G, et al. CD57 CD4 T cells underlie belatacept‐resistant allograft rejection. Am J Transplant. 2016;16:1102‐1112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Crotty S. Follicular helper CD4 T cells (TFH). Annu Rev Immunol. 2011;29:621‐663. [DOI] [PubMed] [Google Scholar]
- 86. Cano‐Romero FL, Laguna Goya R, Utrero‐Rico A, et al. Longitudinal profile of circulating T follicular helper lymphocytes parallels anti‐HLA sensitization in renal transplant recipients. Am J Transplant. 2019;19(1):89‐97. [DOI] [PubMed] [Google Scholar]
- 87. Koutsakos M, Nguyen THO, Kedzierska K. With a little help from T follicular helper friends: humoral immunity to influenza vaccination. J Immunol. 2019;202(2):360‐367. [DOI] [PubMed] [Google Scholar]
- 88. Petersone L, Edner NM, Ovcinnikovs V, et al. T cell/B cell collaboration and autoimmunity: an intimate relationship. Front Immunol. 2018;9:1941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Copley HC, Elango M, Kosmoliaptsis V. Assessment of human leukocyte antigen immunogenicity: current methods, challenges and opportunities. Curr Opin Organ Transplant. 2018;23(4):477‐485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Duquesnoy RJ. Clinical usefulness of HLAMatchmaker in HLA epitope matching for organ transplantation. Curr Opin Immunol. 2008;20(5):594‐601. [DOI] [PubMed] [Google Scholar]
- 91. Wiebe C, Kosmoliaptsis V, Pochinco D, Taylor CJ, Nickerson P. A comparison of HLA molecular mismatch methods to determine HLA immunogenicity. Transplantation. 2018;102(8):1338‐1343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Kosmoliaptsis V, Mallon DH, Chen Y, Bolton EM, Bradley JA, Taylor CJ. Alloantibody responses after renal transplant failure can be better predicted by donor‐recipient HLA amino acid sequence and physicochemical disparities than conventional HLA matching. Am J Transplant. 2016;16(7):2139‐2147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Mallon DH, Kling C, Robb M, et al. Predicting humoral alloimmunity from differences in donor and recipient HLA surface electrostatic potential. J Immunol. 2018;201(12):3780‐3792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Geneugelijk K, Niemann M, Drylewicz J, et al. PIRCHE‐II is related to graft failure after kidney transplantation. Front Immunol. 2018;9:321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Wiebe C, Pochinco D, Blydt‐Hansen TD, et al. Class II HLA epitope matching‐A strategy to minimize de novo donor‐specific antibody development and improve outcomes. Am J Transplant. 2013;13(12):3114‐3122. [DOI] [PubMed] [Google Scholar]
- 96. Wiebe C, Kosmoliaptsis V, Pochinco D, et al. HLA‐DR/DQ molecular mismatch: a prognostic biomarker for primary alloimmunity. Am J Transplant. 2019;19(6):1708‐1719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Wiebe C, Nevins TE, Robiner WN, Thomas W, Matas AJ, Nickerson PW. The synergistic effect of class II HLA epitope‐mismatch and nonadherence on acute rejection and graft survival. Am J Transplant. 2015;15(8):2197‐2202. [DOI] [PubMed] [Google Scholar]
- 98. Wiebe C, Rush DN, Nevins TE, et al. Class II eplet mismatch modulates tacrolimus trough levels required to prevent donor‐specific antibody development. J Am Soc Nephrol. 2017;28(11):3353‐3362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Nickerson P FDA LOI Decision Letter. https://www.fda.gov/media/119432/download.
- 100. Tambur AR. HLA‐epitope matching or eplet risk stratification: the devil is in the details. Front Immunol. 2018;9:2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Tambur AR, McDowell H, Hod‐Dvorai R, Abundis MAC, Pinelli DF. The quest to decipher HLA immunogenicity: telling friend from foe. Am J Transplant. 2019;19(10):2910‐2925. [DOI] [PubMed] [Google Scholar]
- 102. Tambur AR, Claas FH. Toward HLA epitope matching in clinical transplantation. Am J Transplant. 2013;13(12):3059‐3060. [DOI] [PubMed] [Google Scholar]
- 103. Tambur AR, Rosati J, Roitberg S, Glotz D, Friedewald JJ, Leventhal JR. Epitope analysis of HLA‐DQ antigens: what does the antibody see? Transplantation. 2014;98(2):157‐166. [DOI] [PubMed] [Google Scholar]
- 104. Dorr CR, Oetting WS, Jacobson PA, Israni AK. Genetics of acute rejection after kidney transplantation. Transpl Int. 2018;31(3):263‐277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105. O'Brien RP, Phelan PJ, Conroy J, et al. A genome‐wide association study of recipient genotype and medium‐term kidney allograft function. Clin Transplant. 2013;27(3):379‐387. [DOI] [PubMed] [Google Scholar]
- 106. Pihlstrøm HK, Mjøen G, Mucha S, et al. Single nucleotide polymorphisms and long‐term clinical outcome in renal transplant patients: a validation study. Am J Transplant. 2017;17(2):528‐533. [DOI] [PubMed] [Google Scholar]
- 107. Freedman BI, Julian BA, Pastan SO, et al. Apolipoprotein L1 gene variants in deceased organ donors are associated with renal allograft failure. Am J Transplant. 2015;15(6):1615‐1622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108. Michielsen LA, van Zuilen AD, Kardol‐Hoefnagel T, Verhaar MC, Otten HG. Association between promoter polymorphisms in CD46 and CD59 in kidney donors and transplant outcome. Front Immunol. 2018;9:972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Vu D, Tellez‐Corrales E, Shah T, Hutchinson I, Min DI. Influence of cyclooxygenase‐2 (COX‐2) gene promoter‐1195 and allograft inflammatory factor‐1 (AIF‐1) polymorphisms on allograft outcome in Hispanic kidney transplant recipients. Hum Immunol. 2013;74(10):1386‐1391. [DOI] [PubMed] [Google Scholar]
- 110. Hernandez‐Fuentes M, Stapleton CP, Cavalleri GL, Conlon P, Weale ME, Lord GM. The genetic determinants of renal allograft rejection. Am J Transplant. 2018;18(8):2100‐2101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Reindl‐Schwaighofer R, Heinzel A, Kainz A, et al. Contribution of non‐HLA incompatibility between donor and recipient to kidney allograft survival: genome‐wide analysis in a prospective cohort. Lancet. 2019;393(10174):910‐917. [DOI] [PubMed] [Google Scholar]
- 112. Mesnard L, Muthukumar T, Burbach M, et al. Exome sequencing and prediction of long‐term kidney allograft function. PLoS Comput Biol. 2016;12(9):e1005088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Stapleton CP, Conlon PJ, Phelan PJ. Using omics to explore complications of kidney transplantation. Transpl Int. 2018;31(3):251‐262. [DOI] [PubMed] [Google Scholar]
- 114. International Genetics & Translational Research in Transplantation Network (iGeneTRAiN) . Design and implementation of the International Genetics and Translational Research in Transplantation Network. Transplantation. 2015;99(11):2401‐2412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Israni A, Leduc R, Holmes J, et al. Single‐nucleotide polymorphisms, acute rejection, and severity of tubulitis in kidney transplantation, accounting for center‐to‐center variation. Transplantation. 2010;90(12):1401‐1408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116. Barry A, Levine M. A systematic review of the effect of CYP3A5 genotype on the apparent oral clearance of tacrolimus in renal transplant recipients. Ther Drug Monit. 2010;32(6):708‐714. [DOI] [PubMed] [Google Scholar]
- 117. Oetting WS, Wu B, Schladt DP, et al. Genome‐wide association study identifies the common variants in CYP3A4 and CYP3A5 responsible for variation in tacrolimus trough concentration in Caucasian kidney transplant recipients. Pharmacogenomics J. 2018;18(3):501‐505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Kuypers DR, Naesens M, Vermeire S, Vanrenterghem Y. The impact of uridine diphosphate‐glucuronosyltransferase 1A9 (UGT1A9) gene promoter region single‐nucleotide polymorphisms T‐275A and C‐2152T on early mycophenolic acid dose‐interval exposure in de novo renal allograft recipients. Clin Pharmacol Ther. 2005;78(4):351‐361. [DOI] [PubMed] [Google Scholar]
- 119. Wang J, Yang JW, Zeevi A, et al. IMPDH1 gene polymorphisms and association with acute rejection in renal transplant patients. Clin Pharmacol Ther. 2008;83(5):711‐717. [DOI] [PubMed] [Google Scholar]
- 120. Jacobson PA, Schladt D, Oetting WS, et al. Genetic determinants of mycophenolate‐related anemia and leukopenia after transplantation. Transplantation. 2011;91(3):309‐316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121. Rojas L, Neumann I, Herrero MJ, et al. Effect of CYP3A5*3 on kidney transplant recipients treated with tacrolimus: a systematic review and meta‐analysis of observational studies. Pharmacogenomics J. 2014;15:38. [DOI] [PubMed] [Google Scholar]
- 122. Birdwell KA, Decker B, Barbarino JM, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for CYP3A5 genotype and tacrolimus dosing. Clin Pharmacol Ther. 2015;98(1):19‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Sanghavi K, Brundage RC, Miller MB, et al. Genotype‐guided tacrolimus dosing in African‐American kidney transplant recipients. Pharmacogenomics J. 2017;17(1):61‐68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124. Loupy A, Aubert O, Orandi BJ, et al. Prediction system for risk of allograft loss in patients receiving kidney transplants: international derivation and validation study. BMJ. 2019;366:l4923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125. Stegall MD, Troy Somerville K, Everly MJ, et al. The importance of drug safety and tolerability in the development of new immunosuppressive therapy for transplant recipients: the Transplant Therapeutics Consortium's position statement. Am J Transplant. 2019;19(3):625‐632. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.