

Abstract
Sinus of Valsalva aneurysm (SOVA) is an unusual cardiac anomaly that is potentially fatal with rupture. It is often asymptomatic but has various presentations. We describe a case of a 67-year-old male who presented with atypical chest pain. Transthoracic echocardiogram and cardiac computed tomography scan confirmed a large SOVA complicated by thrombus formation and compression of the left atrium and left ventricular outflow tract. The patient successfully underwent a Bentall procedure—surgical aortic aneurysm repair with mechanical aortic valve conduit. We discuss several clinical decision-making branch points to highlight the complexity of managing this condition. Even in asymptomatic or minimally symptomatic patients with SOVA, surgery may be indicated if the aneurysm meets the criteria for size or has thrombus formation or compressive effects.
Keywords: sinus of Valsalva aneurysm, SOVA, cardiac anomaly
INTRODUCTION
Sinus of Valsalva aneurysm (SOVA) is a rare condition that is often asymptomatic but has various presentations, including rupture that could be fatal.1,2 We hereby present a case of a large unruptured SOVA complicated by thrombus formation and compression of the left atrium and left ventricular outflow tract, highlighting the importance of prompt diagnosis and the condition's associated diagnostic challenges.
CASE PRESENTATION
A 67-year-old man with a history of hypertension but no history of cigarette smoking, connective tissue disease, or chest trauma presented after a single episode of chest pain. Ten years prior to presentation, he had a diagnostic coronary angiogram that showed nonobstructive coronary artery disease. On presentation, he denied dyspnea, orthopnea, palpitations, syncope, or lower extremity edema. A basic laboratory work-up and cardiopulmonary examination were both unremarkable, and a 12-lead electrocardiogram (ECG) did not show any notable changes. Transthoracic echocardiogram (TTE) showed normal left ventricular function with no regional wall motion abnormalities. However, the aortic root was significantly enlarged at the sinus of Valsalva, measuring 5.3 cm. On close examination, the noncoronary cusp of the aortic valve appeared aneurysmal, representing a SOVA (Figure 1 A). Computer tomography (CT) of the thorax with ECG gating was obtained for further evaluation, and the sinus of Valsalva measured 5.6 cm on the coronal plane on CT. A circumferential area of low density was also visualized around the noncoronary cusp, suggestive of a thrombus or a previous thrombosed dissection (Figure 1 B). Cardiothoracic surgery was consulted to evaluate for surgical management. As part of the preoperative evaluation, coronary angiogram was deferred given the high risk of thrombus embolization; however, a coronary CT angiogram was performed and showed 50% to 60% focal stenosis of the left anterior descending artery (LAD) mid segment. The noncoronary sinus aneurysm of the aortic valve with a large thrombus was seen again. The aneurysm exerted mass effect on the anterior wall of the left atrium and led to narrowing of the left ventricular outflow tract; however, this was not apparent on the transthoracic or transesophageal echocardiograms on 2-dimensional images, and there were no hemodynamically significant Doppler effects.
Figure 1.
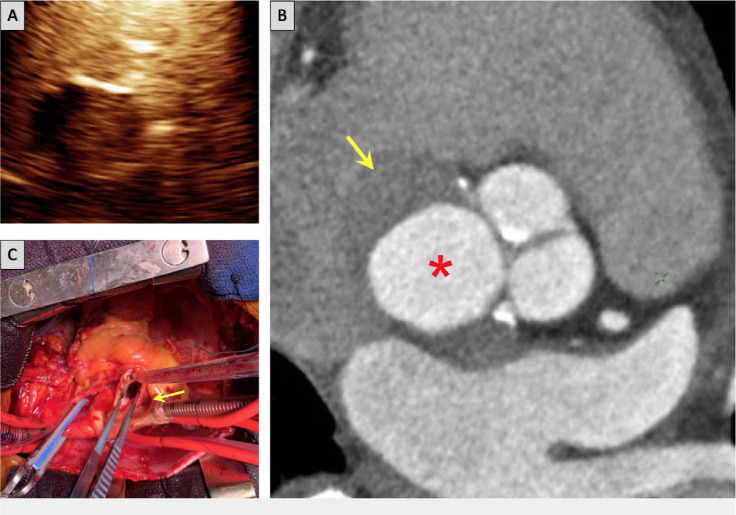
(A) Transthoracic echocardiogram shows a filling defect within the noncoronary cusp after administration of ultrasound contrast, suggestive of a thrombus. (B) Computed tomography coronary angiogram shows aneurysmal noncoronary sinus (*indicates dilated noncoronary cusp aneurysm, arrow indicates thrombus). (C) Intraoperative image shows aortic root at the level of sinus of Valsalva and the noncoronary cusp aneurysm (arrow).
Since the thrombus was likely chronic in nature and there was concern for a paradoxical increase in thromboembolism risk, anticoagulation was not started. The patient eventually underwent surgical aortic aneurysm repair with a single left internal mammary artery-LAD bypass and mechanical aortic valve conduit. Intraoperatively, a tear was seen posteriorly through the intervalvular fibrosa onto the roof of the left atrium, suggesting prior dissection. The patient tolerated surgery without complications and was discharged on warfarin. He was doing well on follow-up and had no chest pain. It was difficult to conclude whether or not his prior chest pain on initial presentation was related to the SOVA, but we could not find any other clear explanation. Nevertheless, it did ultimately expose the SOVA and was no longer present after the surgery.
DISCUSSION
Aneurysm of the sinus of Valsalva is so rare that a review of 8,138 autopsies found it in only 0.09% of participants.1 SOVA can be congenital or acquired, and etiologies for the latter include infections such as bacterial endocarditis, syphilis, tuberculosis, trauma, connective tissue diseases, vasculitis, and chronic changes of atherosclerosis.1 Although our patient did not report a history of trauma, the finding of a separation between the left ventricle and the medial wall of the SOVA points to trauma as the potential etiology.
Unruptured SOVA is generally asymptomatic. Between 30% and 50% of patients present with progressive dyspnea secondary to aortic regurgitation. They may also present with arrhythmia since atrial fibrillation and complete heart block have been reported. A review of 177 patients with unruptured SOVA showed that 14% were asymptomatic, 56% had dyspnea, 46% had chest pain, 18% had palpitations, and 57% had murmur on exam.1 In this case, the SOVA was compressing the left atrium and left ventricular outflow tract, which possibly resulted in chest pain.
While invasive aortogram has historically been the gold standard for diagnosing SOVA, noninvasive imaging modalities are increasingly being used.1,3 In fact, compared to surgical findings, TTE was found to be 93.9% sensitive and 99.9% specific in diagnosing SOVA.4 Computed tomography adds additional value when evaluating patients with SOVA, particularly if aortocardiac shunts are present. In this case, cardiac CT allowed for evaluation of coronary anatomy as well. Cardiac magnetic resonance imaging has also been used to evaluate SOVA and surrounding anatomy in great detail. Of note, a particular diagnostic consideration in this case was the use of CT angiography rather than conventional angiography to evaluate coronary anatomy due to the high embolic risk with catheter manipulation. There have been reported cases of mural thrombi or calcifications causing blockage of the coronary artery ostium.2
Thrombus formation in the aorta is uncommon due to high blood flow velocity. A SOVA is a potential site of thrombus formation because it causes turbulent blood flow and stasis.5 Optimal treatment for sinus of Valsalva thrombus remains poorly defined since most guidance is via case reports with surgery as the main treatment.6–8 However, there are reports of successful treatment with anticoagulation alone.9 For instance, in a case report of thrombus formation in a left coronary cusp SOVA, the patient was treated with 4 months of anticoagulation.8 In our case, the decision was made not to start the patient on anticoagulation because of the chronicity of the thrombus, potential risk of clot destabilization, and immediate plan for surgery within days.8
There is limited data on managing patients with SOVA. Surgical correction of unruptured SOVA has been used for definitive treatment with the goal of preventing rupture.8 In a review of 19 cases in which patients presented with chest pain attributed to unruptured SOVA that interfered with coronary flow, 9 were treated surgically. Among the 10 patients not treated surgically, 5 experienced fatal myocardial infarction. None of them had a thrombus in the SOVA.8 In one case of SOVA in the right coronary cusp complicated by atherothrombosis, surgical repair was performed with patch placement over an intimal tear to prevent rupture. A review of 15 cases of patients with ascending aorta thrombus found that 27% who were treated with anticoagulation alone suffered recurrent embolism.5 It was for that reason that surgical repair was considered the appropriate course of action for our patient. For ruptured SOVA, immediate surgery is the treatment of choice.10
Percutaneous closure of a ruptured SOVA with a patch has also been reported. In a review of SOVA cases in which 20 and 15 patients were treated surgically and percutaneously, respectively, there was no statistically significant difference in success rate, mortality, or New York Heart Association class on postoperative evaluation.10 Of note, none of the patients in those cases also had thrombus formation in the SOVA.
CONCLUSION
SOVA is a rare aortic abnormality that can potentially be acquired through inflammation, trauma, or connective tissue disease. TTE is the most common method for initial diagnosis. The aneurysm creates an environment of blood stasis and hence a nidus for thrombus formation. Coronary angiogram should be avoided in these patients given the risk of embolism with catheter manipulation. Surgical repair remains the standard of care for unruptured SOVA.
Footnotes
Conflict of Interest Disclosure:
The authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
REFERENCES
- 1.Bricker AO, Avutu B, Mohammed TL, et al. Valsalva sinus aneurysms: Findings at CT and MR imaging. RadioGraphics. 2010 Jan;30(1):99–110. doi: 10.1148/rg.301095719. [DOI] [PubMed] [Google Scholar]
- 2.Zhang J, Liu Y, Liu L, Deng Y. An extracardiac unruptured right sinus of valsalva aneurysm complicated with atherothrombosis. Echo Res Pract. 2016 Mar; doi: 10.1530/ERP-15-0028. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bamford P, Collins N. Severe Dilatation of Coronary Artery Ostium Complicating Sinus of Valsalva Aneurysm: Differential Diagnosis and Review of the Literature. Case Rep Cardiol. 2017 Apr 13; doi: 10.1155/2017/8694652. doi. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cheng TO, Yang, Xie M, et al. Echocardiographic diagnosis of sinus of Valsalva aneurysm: a 17-year (1995–2012) experience of 212 surgically treated patients from one single medical center in China. Int J Cardiol. 2014 Apr 15;173(1):33–9. doi: 10.1016/j.ijcard.2014.02.003. [DOI] [PubMed] [Google Scholar]
- 5.Abubakar H, Ahmed A, Subahi A, Yassin A. Thrombus in the Right Coronary Sinus of Valsalva Originating from the Left Atrial Appendage Causing Embolic Inferior Wall Myocardial Infarction. J Investig Med High Impact Case Rep. 2018 Jan-Dec;6:2324709618792023. doi: 10.1177/2324709618792023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Eguchi K, Ohtaki E, Misu K, et al. Acute myocardial infarction caused by embolism of thrombus in the right coronary sinus of Valsalva: a case report and review of the literature. J Am Soc Echocardiogr. 2004 Feb;17(2):173–7. doi: 10.1016/j.echo.2003.10.002. [DOI] [PubMed] [Google Scholar]
- 7.Choi JB, Choi SH, Kim NH, Jeong JW. Floating thrombus in the proximal aortic arch. Texas Heart Inst J. 2004;31(4):432–434. [PMC free article] [PubMed] [Google Scholar]
- 8.Lijol A, Parodi E, Passerone GC, Scarano F, Caruso D, Iannetti M. Unruptured Aneurysm of the Left Sinus of Valsalva Causing Coronary Insufficiency. Texas Heart Inst J. 2002;29(1):40–44. [PMC free article] [PubMed] [Google Scholar]
- 9.Nakata A, Yoshizawa H, Hirota S, Takazakura E. Sinus of Valsalva thrombosis causing renal infarction. Intern Med. 2006 Feb;45(15):909–12. doi: 10.2169/internalmedicine.45.1634. [DOI] [PubMed] [Google Scholar]
- 10.Liu S, Xu X, Ding X, Guanzhong L, Zhao Z, Qin Y. Comparison of immediate results and mid-term follow-up of surgical and percutaneous closure of ruptured sinus of Valsalva aneurysm. J Cardiol. 2014 Mar;63(3):239–43. doi: 10.1016/j.jjcc.2013.08.011. [DOI] [PubMed] [Google Scholar]