

Abstract
Introduction:
Tricortical iliac bone is the gold standard as an autograft for the reconstruction of the anterior column in tuberculosis (TB) of the thoracic spine. However, the quantity of graft needed is significant. It creates a considerable defect in the pelvic bone, causing graft site complications, including pain, pelvic instability, fractured ilium, herniated muscle, or abdominal contents. To prevent these donor site morbidities, ribs that were removed during the versatile approach were used for anterior reconstruction. The aim of this study was to assess the clinical and radiological results of the reconstruction of the anterior column of the spine with the help of an excised rib during the versatile approach.
Subjects and Methods:
This retrospective study was undertaken at a tertiary care center with a study duration of 14 years. Between January 2004 and December 2016, 52 patients with thoracic Koch's spine had anterior column reconstructed with multiple rib grafts. A single surgeon performed all operations. Indications for the surgery in these patients were the presence of neurologic deficit (49 patients) and vertebral column instability (3 patients). The preoperative kyphosis angle and visual analog scale (VAS) score were compared with postoperative values using a paired t-test.
Results:
All patients underwent a minimum follow-up of 18 months and were evaluated clinicoradiologically. Good bony fusion with neurological recovery was achieved in all cases. The VAS score for back pain improved significantly postsurgery. There was one case of graft buckling treated conservatively.
Discussion:
Appropriate anterior reconstruction forms the cornerstone of successful surgical management of spinal TB. The “Versatile approach” used offers anterior and posterior access in the lateral position. In these patients, we obviated the need for iliac crest graft using multiple segments of the rib for anterior column reconstruction. This meticulous rib grafting technique gives good functional outcome in terms of solid bony fusion.
Conclusion:
Meticulous rib grafting technique gives 360° bony fusion and good functional outcome in surgery for thoracic spinal TB. It has the advantage of avoiding the complications associated with a tricortical iliac crest graft.
Keywords: Anterior column reconstruction, fusion, rib graft, thoracic spine, tuberculosis
Introduction
The first modern case of the spine tuberculosis (TB) was described in 1779 by Pott[1] and hence the name Pott's spine. The spine is the most common site for the development of skeletal TB and accounts for 50% of cases. What makes spinal TB alarming is the risk of neurological deficits, which may vary from 10% to 43%.[2] Any part of the spine can be affected; however, the thoracic spine and the dorsolumbar junction are the most commonly affected region.[3]
Indications for the surgery in the thoracic spine TB include the neurological deficit, instability, and failure of conservative management. Approaches for surgery include anterior, posterior, or combined.[4,5,6,7,8] Thoracic spine surgery with the anterior approach for TB, leaves a large void which is filled with bone grafts or cage or bone substitutes for obtaining solid fusion. Tricortical iliac bone is the gold standard as an autograft for the reconstruction of this defect. However, the quantity of graft needed is significant, and it creates a considerable defect in the pelvic bone. This may cause graft site complications, including pain at the donor site, pelvic instability,[9] fractured ilium,[10] herniated muscle, or abdominal contents.[11] To prevent these donor site morbidities, ribs that were removed during the versatile approach (combined anterior plus posterior approach in lateral position) for the thoracic spine TB were used for the purpose of anterior reconstruction. This study aims to assess the clinical and radiological results of the reconstruction of the anterior column of the spine with the help of the excised rib during the versatile approach for TB of the dorsal spine.
Subjects and Methods
This retrospective study was undertaken at a tertiary care center with a study duration of 12 years. Between January 2004 and December 2016, 52 patients with thoracic spine TB had anterior column reconstructed with multiple rib grafts. Thirty males and 22 females with ages ranging from 18 to 61 years were included in the study, with 27.34 years being the average age of patients. All patients were operated by a single surgeon. The presence of neurologic deficit (49 patients) and vertebral column instability (3 patients) were the indications for the surgery in this study. The unstable vertebral column was defined as complete loss of >1 vertebral body with localized kyphosis of >30°, with or without coronal/sagittal plane translation.
All patients with Frankel Grade C or D were treated by the “middle path regime” which was popularized by Tuli. Early surgical intervention was planned for patients with neurological grade Frankel Grade A or B.
Demographic details which included the patient's age, gender, diagnosis, levels of vertebrae involved, number of levels fused, preoperative and postoperative kyphosis angles (K angle), correction loss at follow-up, preoperative and postoperative neurological status (Frankel Grading), preoperative and postoperative pain as assessed by the visual analog scale (VAS) score, and postoperative complications were noted in a case record form.
Statistical analysis
Descriptive statistics, including the means and standard deviations, were calculated for variables using SPSS software 17.0 (SPSS Inc., Chicago, IL, USA). The preoperative K angle and VAS score were compared with postoperative values using a paired t-test.
Surgical procedure
Versatile approach[3] (combined anterior plus posterior approach in lateral position) was used to expose the lesion. This approach has been described for the first time by the lead author of this paper. Patients were positioned on the left lateral side. Thoracotomy done through the right side usually directly leads to the lesion as pus tends to track along the path of least resistance. The vena cava on the right side offers less resistance as compared to the aorta on the left, which has thick muscular walls. Furthermore, a left lateral approach allows easier passage of sublaminar wires by a right-handed surgeon. A semilunar incision was made in the right paramedian region. Skin, subcutaneous tissue, deep fascia, and trapezius muscle were cut along the skin incision. The rhomboids were incised toward the midline. The outer surface of the rib cage was exposed by retracting the scapula and attached muscle anteriorly. The rib, which corresponds to the collapsed vertebral level, was excised [Figure 1]. The anterior surface of the vertebral body was reached using the extrapleural or transpleural approach. A chest spreader was used to increase the space; the lung was retracted on a mop with a Deaver retractor. Anterior necrotic tissue was debrided. Posterior exposure of the spinous process, laminae, transverse processes, and facet joints was performed by separating the erector spinae muscle bilaterally. Posterior instrumentation was done at this stage in the form of the Hartshill loop rectangle with sublaminar wire. Strut grafting was performed using appropriate size rib after making slots in proximal and distal regions of the healthy bone [Figure 2]. An additional Onlay graft (part of the excised rib) was placed between the vertebral body and the anterior longitudinal ligament to span the diseased area. Posterior bony reconstruction (fusion) was then performed using bivalved rib grafts to bridge the laminectomy defect.
Figure 1.
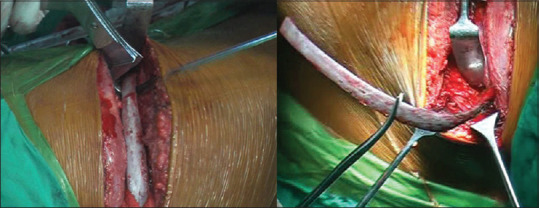
Excision of a large segment of the rib during the versatile approach
Figure 2.
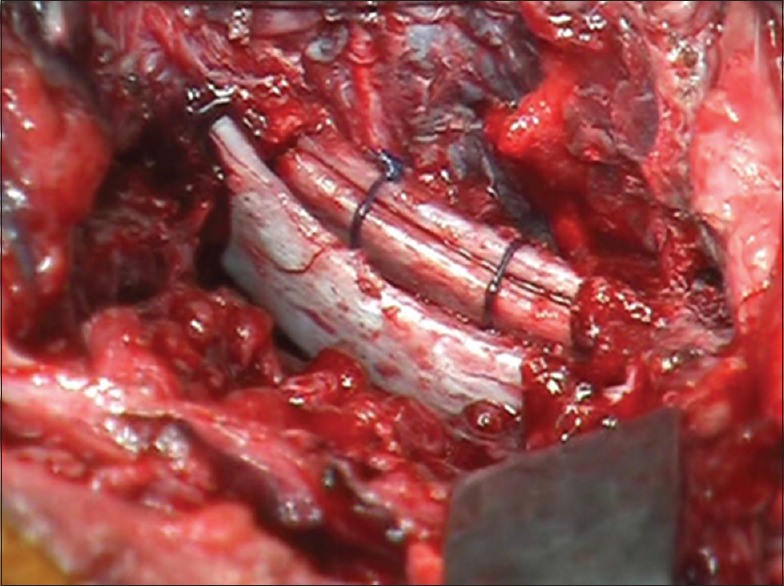
Reconstruction of the anterior column with multiple rib grafts
Intraoperative samples from all patients were sent for culture and drug sensitivity. Anti-tubercular therapy (ATT) was administered for 18 months as per the sensitivity report. In cases of drug-resistant TB, ATT was administered for 2 years. Since TB is essentially a medical disease, the surgical intervention did not change in the case of multidrug-resistant TB. The only change in treatment was appropriate drugs as per the sensitivity report for a longer duration.
Radiographic evaluation
Preoperatively, patients were evaluated radiologically by X-ray and magnetic resonance imaging. Radiographs included standing anteroposterior (AP) and lateral views of the thoracolumbar spine. Supine radiographs were acquired in patients with no ambulatory power in their lower limbs or those with imminent paralysis. AP and lateral radiographs of the thoracolumbar spine were performed postoperatively and during follow-up at 3, 6, 12, and 24 months. K angle was calculated by drawing lines from the upper to the lower border of the first normal vertebra above and below the diseased area, respectively. Computed tomography scan was performed 1 year postoperatively in patients in whom fusion could not be assessed on X-ray.
Results
All 52 patients underwent a minimum follow-up of 18 months, with a mean follow-up of 57.23 ± 24.36 months (range, 18–153 months). During the presentation, the mean value of preoperative kyphosis was 25.02° ± 8.47° (range, 8°–49°). The average number of the vertebral bodies involved was 3.12 ± 0.36 (range, 2–4), with D5–6 being the most common involved level [Table 1].
Table 1.
Results
| Mean (range) | P | ||
|---|---|---|---|
| Preoperative | Postoperative | ||
| Number of vertebral bodies involved | 3.12±0.36 (2-4) | ||
| Total levels fixed | 5.7±1.01 (4-9) | ||
| K-angle | 25.02±8.47 (8-49) | 9.17±4.17 (1-23) | <0.001 |
| VAS score | 7.02±0.9 (5-9) | 1.57±0.59 (1-3) | <0.01 |
VAS – Visual Analogue Scale
No laminectomy was needed for forty patients. Laminectomy was indicated only in those patients where there was posterior compression. Ten patients required single-level laminectomy, wheras two patients needed two-level laminectomy. The total levels fixed were 5.70 ± 1.01 (range, 4–9). The mean immediate postoperative K angle was 9.17° ± 4.17° (range, 1°–23°). Improvements in K angle were statistically significant (P < 0.001). Pain improved from an average VAS score of 7.02 ± 0.97 (range, 5–9) preoperatively to 1.57 ± 0.59 (range, 1–3) at the final follow-up. Improvements were statistically significant (P < 0.01). Fusion was achieved in all cases.
Five patients did not have any preoperative neurological deficits. Postoperatively their neurological status was unchanged. All five patients with Frankel Grade D recovered completely. Of 24 patients with Frankel Grade C, 15 patients recovered completely, and nine patients recovered to Grade D. Of 18 patients with Frankel Grades A and B, 12 patients recovered completely, ifivepatients recovered to Grade D, and one patient remained paraplegic. No patient deteriorated following surgery [Table 2].
Table 2.
Pre- and post-operative neurological status of patients
| Number of patients | |||
|---|---|---|---|
| Preoperative Frankel stage | Postoperative Frankel stage | ||
| E (5) | E (5) | ||
| D (5) | E (5) | ||
| C (24) | E (15) | D (9) | |
| A and B (18) | E (12) | D (5) | A (1) |
Three patients had superficial wound infection, of which two healed by daily cleaning and dressing while the other required secondary suturing. One patient developed buckling of the anterior rib graft, with the reappearance of kyphosis [Figure 3]. However, because this patient recovered neurologically from Frankel Grade D to Grade A and had a negligible cosmetic deformity, revision surgery was not opted for. The patient was mobilized with a Thoraco-Lumbo-Sacral Orthosis and ultimately, bony fusion was achieved.
Figure 3.

Buckling of the graft with consolidation in mild kyphosis
Discussion
Spinal TB is essentially a medical disease and ATT has a central role in the recovery and response of patients. In many patients, in the absence of neurologic deficit, instability, and deformity, only ATT has been shown to be effective even in the presence of a paravertebral abscess.[2] Indications for surgical intervention have not changed significantly since the “middle path regimen” was originally described by Tuli in 1975.[12,13]
The authors would like to emphasize that “sound anterior reconstruction” forms the cornerstone of successful surgical management of spinal TB. After debridement of the necrotic material, the anterior fusion is performed by bone graft (iliac or rib), metal cage, and bone graft substitutes. However, bone graft substitutes are expensive and carry the risk of infection. Iliac crest bone graft is the gold standard for anterior reconstruction as it provides adequate strength plus gives a scaffolding for bony ingrowth. However, it leaves behind a defect in iliac crest leading to donor site morbidities. Many studies have shown that the iliac crest graft harvest is not risk-free, with an overall complication rate ranging from 9.4% to 49%.[14] The major complications include long-term disabling pain,[9] fractured ilium,[10] herniation of the muscle or abdominal contents at the harvest site,[11] deep wound infection, and incisional hernia. Minor ones include superficial infections, seromas, and hematomas. Elderly, obese, and those with poor muscle tone are patients at increased risk of these complications.
In our study, to obviate these complications associated with iliac crest graft, we used only rib grafts for the anterior reconstruction. The surgical approach used was the versatile approach, which offers anterior and posterior access in the lateral position. This approach has the additional advantage of direct visualization of the anterior defect. After removal of the anterior necrotic tissue and posterior fixation, the anterior void can be seen directly. Further debridement may be performed until the healthy bone is visible at both proximal and distal ends. To ensure that the graft snugly fits into the anterior column and to provide a large surface area for the union, before fitting the graft a slot is prepared in the proximal and distal bone. However, the slot must be prepared using small and sharp instruments, with extreme care, because the bone is usually soft due to tuberculous abscesses. Since the use of a single piece of the rib would not be sufficient to support the entire anterior column, as many pieces of the rib as possible have to be used. In the versatile approach, while approaching the collapsed vertebral body, knowingly a large segment of the rib corresponding to that collapsed body was excised. This segment was divided into multiple pieces depending on the length of the anterior defect to be reconstructed. Small hole was drilled in these pieces and they were tied together with a nonabsorbable suture material to make a bony strut with a large surface area. This increased the overall stability of the graft. An additional rib graft segment was placed anteriorly as an Onlay graft if the space permitted. Bivalved rib segment was placed posteriorly to fuse affected bony segments or to bridge the laminectomy defects.
Meticulous rib grafting technique, as described in this article, gave 360° bony fusion with a good functional outcome while avoiding complications associated with a tricortical iliac crest graft.
One of the limitations of this study is its retrospective nature and relatively small sample size. A prospective study with a control group where iliac crest autograft is used for the comparison is needed to further validate our findings.
Conclusion
Meticulous rib grafting technique gives 360° bony fusion and good functional outcome in surgery for thoracic spinal TB. It has the advantage of avoiding the complications associated with a tricortical iliac crest graft. Thus, we conclude that the use of rib grafts in anterior column reconstruction of the spine obviates the need for iliac crest grafts and gives good clinical outcomes.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Pott P, Earle J. The Chirurgical Works of Percivall Pott J Johnson. 1808 [Google Scholar]
- 2.Tuli SM. Tuberculosis of the Skeletal System. 3rd ed. New Delhi: Jaypee Brothers Medical Publishers Ltd; 2004. Tuberculous osteomyelitis; pp. 174–83. [Google Scholar]
- 3.Srivastava SK, Aggarwal RA, Bhosale SK, Roy K, Nemade PS. The versatile approach: A novel single incision combined with anterior and posterior approaches for decompression and instrumented fusion to treat tuberculosis of the thoracic spine. Asian Spine J. 2017;11:294–304. doi: 10.4184/asj.2017.11.2.294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hodgson AR, Stock FE. Anterior spine fusion for the treatment of tuberculosis of the spine: The operative findings and results of treatment in the first 100 cases. Bone Joint J Surg. 1960;42:295–310. [Google Scholar]
- 5.Upadhyay SS, Saji MJ, Yau AC. Duration of anti-tuberculosis chemotherapy in conjunction with radical surgery in the management of spinal tuberculosis. Spine. 1996;21:1898–903. doi: 10.1097/00007632-199608150-00014. [DOI] [PubMed] [Google Scholar]
- 6.Zhang HQ, Lin MZ, Shen KY, Ge L, Li JS, Tang MX, et al. Surgical management for multilevel noncontiguous thoracic spinal tuberculosis by single-stage posterior transforaminal thoracic debridement, limited decompression, interbody fusion, and posterior instrumentation (modified TTIF) Arch Orthop Trauma Surg. 2012;132:751–7. doi: 10.1007/s00402-012-1473-z. [DOI] [PubMed] [Google Scholar]
- 7.Louw JA. Spinal tuberculosis with neurological deficit. Treatment with anterior vascularised rib grafts, posterior osteotomies and fusion. J Bone Joint Surg Br. 1990;72:686–93. doi: 10.1302/0301-620X.72B4.2380228. [DOI] [PubMed] [Google Scholar]
- 8.Moon MS, Woo YK, Lee KS, Ha KY, Kim SS, Sun DH. Posterior instrumentation and anterior inter-body fusion for tuberculous kyphosis of dorsal and lumbar spines. Spine (Phila Pa 1976) 1995;20:1910–6. doi: 10.1097/00007632-199509000-00013. [DOI] [PubMed] [Google Scholar]
- 9.Chan K, Resnick D, Pathria M, Jacobson J. Pelvic instability after bone graft harvesting from posterior iliac crest: Report of nine patients. Skeletal Radiol. 2001;30:278–81. doi: 10.1007/s002560100344. [DOI] [PubMed] [Google Scholar]
- 10.Porchet F, Jaques B. Unusual complications at iliac crest bone graft donor site: Experience with two cases. Neurosurgery. 1996;39:856–9. doi: 10.1097/00006123-199610000-00043. [DOI] [PubMed] [Google Scholar]
- 11.Hamad MM, Majeed SA. Incisional hernia through iliac crest defects. A report of three cases with a review of the literature. Arch Orthop Trauma Surg. 1989;108:383–5. doi: 10.1007/BF00932452. [DOI] [PubMed] [Google Scholar]
- 12.Tuli SM. Results of treatment of spinal tuberculosis by “middle-path” regime. J Bone Joint Surg Br. 1975;57:13–23. [PubMed] [Google Scholar]
- 13.Rajasekaran S, Kanna RM, Shetty AP. Pathophysiology and treatment of spinal tuberculosis. JBJS Rev. 2014:2. doi: 10.2106/JBJS.RVW.M.00130. pii: 01874474-201409000-00004. [DOI] [PubMed] [Google Scholar]
- 14.Banwart JC, Asher MA, Hassanein RS. Iliac crest bone graft harvest donor site morbidity. A statistical evaluation. Spine (Phila Pa 1976) 1995;20:1055–60. doi: 10.1097/00007632-199505000-00012. [DOI] [PubMed] [Google Scholar]