

Abstract
Job-related stress had adverse effects on both patients and community nurses. To evaluate stress, an effective and reliable instrument was needed. The aim of this study was to develop a short-form Chinese Community Nurse Stress Scale and examine its psychometric properties.
A cross-sectional study was conducted. A total of 969 community nurses were selected from 56 community centers/stations in Sichuan Province. The socio-demographic data and job stress assessed by the Chinese Community Nurse Stress Scale (CNSS) were collected. After randomly splitting the sample into group 1 and group 2, exploratory and confirmatory factor analysis were carried out to shorten the scale and test its reliability and construct validity.
There were no significant differences in socio-demographic variables between group 1 (n = 488) and group 2 (n = 481). During exploratory factor analysis, 4 factors were selected, including management and interpersonal relationships (8 items), patient care (7 items), environment and resources of work (6 items), and career promotion (4 items), which explained 62.66% of all variance. Cronbachs α coefficient of the short-form CNSS was 0.94, and the cross-sample validity test supported the best fit model for this 25-item CNSS.
The results in this study supported that the 25-item CNSS had a good reliability and validity when it was administrated to Chinese community nurses.
Keywords: confirmatory factor analysis, exploratory factor analysis, job-related stress, psychometric properties
1. Introduction
Primary health care services are recognized as important resources addressing the aging and chronic disease, which are the main health problems in China and all over the world.[1–4] In 2009, the Chinese government launched a series of health system reforms to strengthen the primary health care services, and community health services played a central role in these reforms.[5,6] Community health care is defined as the provision of essential, wide-ranging health care services in the community for people from all socioeconomic groups and geographic regions.[7,8] At the end of 2018, there were 34,997 community health care centers/stations and 582 thousand of community health care providers nationwide in China.[9] Among all community health service providers, community nurses, who are responsible for chronic disease prevention, rehabilitation, health education, medication administration, family planning guidance and immunization, present the largest proportion.[8,10,11] However, some evidence has indicated that community nurses have insufficient capabilities for the various health care needs of patients, due to the shortage of nursing staff and inadequate professional skill training for community health service providers.[9,12,13] The gap between the health care demands and the abilities and knowledge of community nurses has led to job-related stress,[14] which is the main health problem among community nursing staff.
Job-related stress occurs when a persons knowledge and ability cannot match the demands and pressure of his or her job.[14] For nurses, job-related stress is defined as the physical and emotional reactions resulting from the interactions between nurses and the occupational environment where the work demands exceeded their capabilities and resources in the environment.[15] Previous studies has found that job-related stress in nurses was a multidimensional phenomenon that is affected by various factors, such as the characteristics of nurses,[16] the nature of nursing care,[14,17,18] interpersonal relationships,[19,20] opportunities for professional promotion,[21] and organizational management.[14,20,22] For community nurses, the organizational structure and the institutional atmosphere may play more important roles in job-related stress.[21] It is clear that job-related stress has adverse effects on both nurses and health care services. For example, high job-related stress can reduce the quality of work life of health professions, increase hostility, aggression and turnover, and notably reduce productivity.[23] Moreover, high job-related stress in nurses is found to reduce nursing care quality.[24] Therefore, it was imperative to assess job-related stress in community nurses so that interventions can be performed.
To efficiently evaluate Chinese nurses job-related stress, some researchers have developed specific instruments. Li and Liu [25] produced the first Chinese Nurse Stress (CNS) scale in 2000 to evaluate job-related stress of nurses. It was a 35-item tool based on the Nurse Stress Scale [26] and the Source of Stress Inventory,[27] showing a good reliability in Chinese sample (Cronbachs α = 0.98).[10,28] This scale includes 5 dimensions: nursing profession and work issues (7 items), workload and time allocation (5 items), environment and resources (3 items), patient care (eleven items), management and interpersonal problems (9 items). And the response options for each item range from 0 (never) to 3 (always). The CNS has long been a widely used instrument to assess job-related stress in various nursing groups in China. Lu et al,[28] used the CNS to evaluate job-related stress in emergency department nurses to explore the relationship between stress and coping strategies of nurses. Qin et al,[15] identified the stressors of nurses in hospitals through the CNS. Luan et al, [29] used the CNS to describe the job-related stress of senior and head nurses. Although the CNS has a good reliability and wide use, there are limited studies focusing on the validity of this instrument. In 2005, Zhao and Fang [30] first examined the construct validity of the CNS by exploratory factor analysis. Afterwards, Wang and Meng [31] produced a new 38-item version of the Chinese Nurse Stress scale in 2007. This new version also had 5 dimensions, including nature and environment of work, personal relationships, the attitudes of patients and their relatives, professional skills, and status and career development. Despite the wide use of the CNS, it was only suitable for nurses in hospitals. For community nurses, the role, nature of work and occupational environment differed greatly from those of nurses in hospitals. Hence, a specific tool for job-related stress among community nurses was developed by Guo, Liu, and Li [10] in 2005 based on the original vision of the CNS. In this Chinese Community Nurse Stress Scale (CNSS), 40 items were divided into 5 dimensions: profession and duty of nursing (7 items), workload and time allocation (6 items), environment and resources of work (6 items), patient care issues (11 items), management and interpersonal relationship (10 items). Respondents rate items using a 4-point Likert scale (1-never to 4-always). A previous study suggested that the CNSS had a good internal consistency reliability (Cronbach’α) estimate of 0.98.[10]
Although the need and utility of the CNS and the CNSS were confirmed, both tools remained underutilized, which may result from time constraints due to too many items.[32,33] It is important to develop a user-friendly and time-saving instrument to assess job-related stress in community nurses. Hence, the aims of this study were to construct a short-form of the Chinese Community Nurse Stress Scale and evaluate its psychometric properties via exploratory and confirmatory factor analysis.
2. Methods
2.1. Study Design
We conducted a cross-sectional study to revise the Chinese Community Nurses Stress Scale and to test the reliability and validity of its short form.
2.2. Samples and Settings
This study was performed in 4 regions: the provincial capital, and the central, southern and northeastern regions of Sichuan Province in China. In total, there were 928 community health centers in Sichuan Province. We randomly selected 56 of these centers, 18 were located in the provincial capital, 11 were located in the central region, 13 were located in the southern region and 14 were located in the northeastern region. Participants were recruited using the cluster sampling method in the selected centers. The eligibility criteria included nurses who
-
1.
were currently employed in the centers/stations,
-
2.
have worked for at least 6 months, and
-
3.
agreed to take part in this study.
This study was approved by the Ethics Committee of Sichuan University. The research assistants explained the study to participants before obtaining consent. The data were only used for research purposes.
2.3. Data Collection
First, researchers explained the purpose and procedure of the study to participants and invited them to take part in this study. After signing the informed consent, each participant was given a sealed envelope with the Community Nurses Stress Scale and a socio-demographic questionnaire. The participants completed the questionnaire in a quiet and private room. The completed questionnaires were collected in sealed envelopes by 2 research assistants and stored in a locked room.
2.4. Measures
We used a self-designed social-demographic questionnaire and the Chinese Community Nurse Stress Scale as the instruments in this study.
The socio-demographic questionnaire assessed the participants age, gender, education level, marital status, geographic area, employment type (there is a unique employment status called “bianzhi” in the Chinese medical system, in which someone could be hired permanently and stably; in this study, we used “temporary” and “permanent” to distinguish the employment type), profession title, income, work shift, community nursing train, duration of nursing and duration of community nursing.
The Chinese Community Nurse Stress Scale was a 40-item instrument developed by Guo, Liu, and Li [10] based on the original version of the Chinese Nurse Stress scale.[25] It consists of 5 dimensions: profession and duty of nursing, workload and time allocation, environment and resources of work, patient care issues, management and interpersonal relationship. The response options for each item ranges from 1 (never) to 4 (always), and the total scores range from 40 to 160, with higher scores indicating more serious stress. The internal consistency reliability of Cronbachs α coefficient was 0.96.
2.5. Data analysis
Data were randomly split into a calibration group (G1) and a validation group (G2). Appropriate methods were used to describe the variables in the 2 groups. The chi-square test and Fisher exact test were performed to compare demographic characteristics between G1 and G2. Item analysis was carried out in G1 to remove ambiguous items. Principal component analysis with orthogonal rotation was performed in the exploratory factor analysis in G1 to examine the construct validity of the 40-item CNSS. Then, we performed a confirmatory factor analysis to select the best fit model. The root mean square error of approximation (RMSEA), the goodness-of-fit index (GFI), the adjusted goodness-of-fit index (AGFI), the comparative fit index (CFI), and the Akaike Information Criterion (AIC) were used to evaluate the goodness-of-fit. For an acceptable fit, the RMSEA should be <0.08, and the GFI, AGFI, and CFI should be >0.90. All analyses were performed using Amos 24 and SPSS 24 (SPSS Inc., Chicago, IL).
3. Results
3.1. Socio-demographic characteristics of the participants
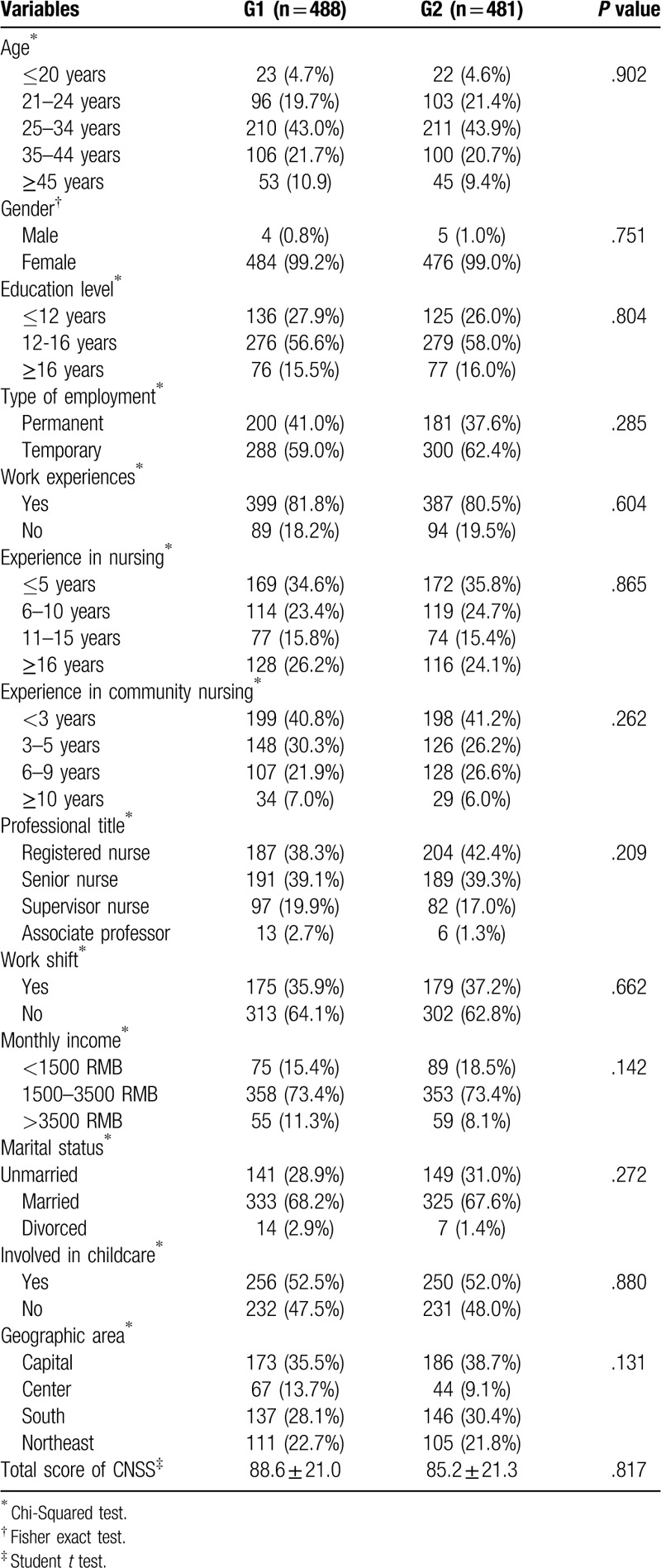
A total of 969 community nurses took part in this study, and they were randomly split into G1 (n = 488) and G2 (n = 481). Table 1 shows the detailed socio-demographic characteristics of the participants in the 2 groups. In both groups, young community nurses accounted for over 60 percent of all participants. Of all participants, 71.1% in G1 and 68.4% in G2 had worked as community nurses less than 5 years. More than 99% of the participants in both groups were females. In total, 18.2% and 19.5% community nurses in G1 and G2, respectively, received no specific community health care training. Most participants in both groups had a monthly income of 1500 to 3500 RMB. Over 50% of the participants in G1 and G2 involved childcare. There were no significant differences in the socio-demographic characteristics or the CNSS scores of the 2 groups.
Table 1.
Socio-demographic data of calibration group (G1) and validation group (G2).
3.2. Item analysis
The item analysis showed that the item-remainder correlation ranged from 0.37 to 0.71, indicating that no item had a low correlation (<0.30). Therefore, all 40 items were included in the next step of the analysis.
3.3. Determining the number of factors
Exploratory factor analysis was used to examine the structure of the 40-item CNSS. The result of the Kaiser–Meyer–Olkin test was 0.94 (>0.70), suggesting a sufficient sample size. Bartlett test of sphericity indicated that the correlation matrix was not singular or identical (χ2 = 11,656.47, P < .001). Therefore, the 40-item CNSS was factorable.
The factors were selected with eigenvalues above 1, combined with the results of the scree plot (Fig. 1). Principal component analysis with orthogonal rotation was performed to delete items with a factor loading below 0.4 or items that had similar factor loadings in 2 factors at the same time. To keep the structure stable, a stepwise method was used to select factors and items according to the suggestions of Wu.[34] Finally, 4 factors remained and explained 62.66% of all variance: each factor explained 39.62%, 10.81%, 6.65%, and 5.59% of the variance (Table 2). Based on the abovementioned criteria, 15 items were deleted, and 25 items remained.
Figure 1.
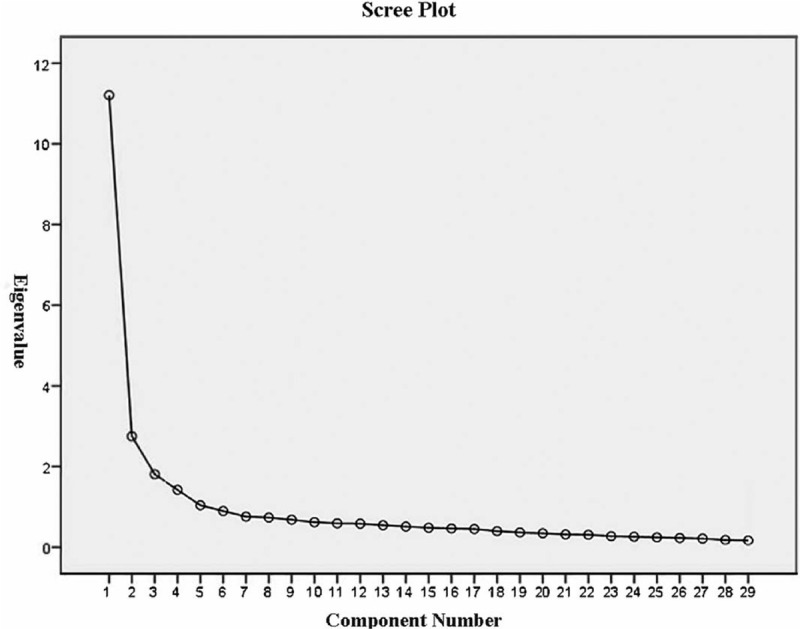
The result of scree plot.
Table 2.
Total variance explained by the 4 extracted factors from the Chinese Community Nurse Stress Scale.

3.4. Factor labeling
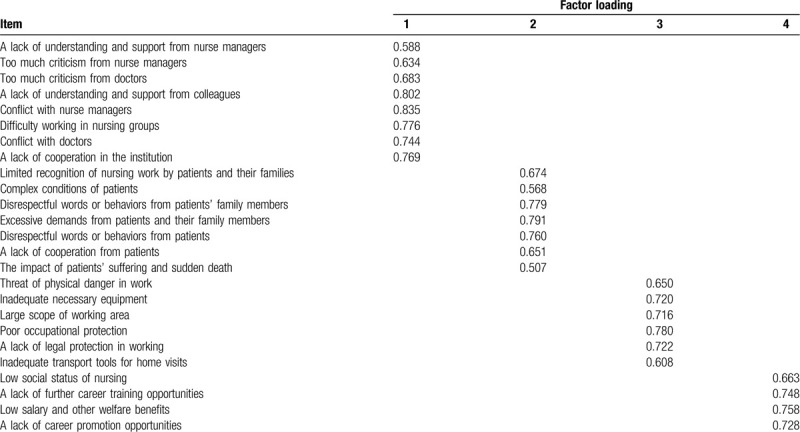
Factor 1 had 8 items with factor loadings ranging from 0.588 to 0.835. The 8 items involved organizational management and interpersonal relationships in the workplace, including the lack of understanding and support from nurse managers, too much criticism from nurse managers, too much criticism from doctors, a lack of understanding and support from colleagues, conflict with nurse managers, difficulty working in nursing groups, conflict with doctors, and a lack of cooperation in the institution. Thus, factor 1 was named management and interpersonal relationship. Factor 2 had 7 items with the factor loadings from 0.507 to 0.791, which pertained to nursing care issues about health care receipts, including limited recognition of nursing work by patients and their families, complex conditions of patients, disrespectful words or behaviors from patients family members, excessive demands from patients and their family members, disrespectful words or behaviors from patients, a lack of cooperation from patients, the impact of patients’ suffering and sudden death. Thus, this factor was named patient care. Factor 3 had 6 items with factor loadings ranging from 0.608 to 0.780, which were related to the environment of the workplace. Factor 3 included threat of physical danger in work, inadequate necessary equipment, large scope of working area, poor occupational protection, a lack of legal protection in working, and inadequate transport tools for home visits. Therefore, this factor was named environment and resources of work. Factor 4 had 4 items with factor loadings ranging from 0.663 to 0.758, which were involved in career promotion. Factor 4 included low social status of nursing, a lack of further career training opportunities, low salary and other welfare benefits, and a lack of career promotion opportunities. Therefore, the last factor was named career promotion. (Table 3)
Table 3.
Principle component analysis of the 25-item CNSS.
3.5. Examinations of the validity of the 25-item CNSS
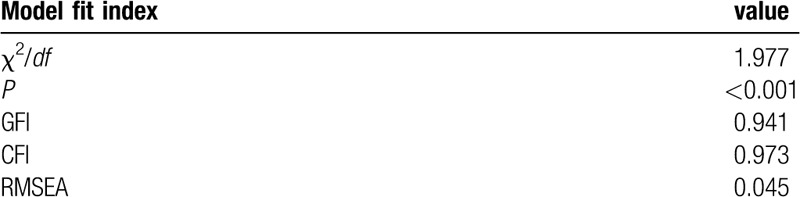
A first order confirmatory factor analysis based on structural equation modeling was performed to validate the 4-factor structure of the 25-item CNSS using the data of G2 (Fig. 2). The results of the goodness-of-fit indexes are displayed in Table 4 and as follows: GFI = 0.941 > 0.90, AGFI = 0.902 > 0.90, CFI = 0.973 > 0.90, RMSEA = 0.045 < 0.08, AIC = 645.431 and χ2/df = 1.977. These indexes indicated the good fit of this model. Regarding the internal consistency reliability of the 25-item CNSS, Cronbachs α coefficient was 0.938. The internal consistency reliability (Cronbachs α coefficient) of factors 1, 2, 3, and 4 was 0.894, 0.876, 0.890, and 0.843, respectively. The last step was to examine the cross-sample validity of the CNSS. Cross-sample validity refers to the ability of an instrument to keep its factor structure stable across different samples.[35] To test the cross-sample validity, data from G1 were used in the model produced by the confirmatory factor analysis above. The fit indexes were as follows: GFI = 0.930 > 0.90, AGFI = 0.884 < 0.90, CFI = 0.962 > 0.90, RMSEA = 0.053 < 0.08, AIC = 719.324, and χ2/df = 2.354. Therefore, the results suggested that the 25-item CNSS had good cross-sample validity.
Figure 2.

Examinations of the validity of the 25-item CNSS.
Table 4.
The goodness-of-fit index of the 25-item CNSS (construct validity).
4. Discussion
In this study, we developed a short-form CNSS based on the original version of the scale by a multiple analytic approach. The results confirmed the reliability and validity of the 25-item CNSS for evaluating Chinese community nurses job-related stress.
In this study, no item was removed during the item analysis, indicating that the items of the original CNSS developed by Guo [10] were closely related to job-related stress. A total of 15 items were removed during the exploratory factor analysis approach because these items failed to theoretically match the 4-factor structure of the CNSS. Finally, the short-form CNSS consisted of 25 items and 4 dimensions, including management and interpersonal relationships, patient care, environment and resources of work, and career promotion. This result was similar to those of previous studies that identified the stressors of nurses. In 1980, Marshall described 9 elements that may be job-related stressors among nurses: nature of nursing, workload, impact of death and dying, uncertainty, high responsibility, role conflicts, interpersonal relationships, the interface of home and work, and the expectations of the role of nurses among patients.[21] Subsequently, Cooper [36] divided these elements into 6 factors: work environment, role stress, interpersonal relationship, career promotion, organization of work and the home/work interface. The final model of the short-form CNSS in this study was similar to the framework of Coopers theory, except for the lack of home/work interface factors. Because Chinese community nurses experience less night shift and weekend work that allows more spare time for family interactions.
However, the results reported herein differed greatly from previous studies conducted in China. The first revised version of the 38-item CNS was introduced by Zhao and Fang.[30] This version of the CNS had 7 dimensions: nature of nursing, workload, time allocation, environment and resource of work, patient care, interpersonal relationship with patients and their family members, management and interpersonal relationship with colleagues. Wang and Meng [31] made further efforts to modify the CNS by developing a 38-item scale with 5 dimensions: environment and nature of work, management and interpersonal relationship with colleagues, attitudes of patients and their family members, profession skills, social status, and career promotion. The 2 scales mainly used in hospital nurses. It was inconsistent with this study, in which professional skills was excluded. The reason may be different roles and clinical skill requirement between hospital and community nurses. For nurses in hospitals, great responsibility for the health and lives of patients, making quick and difficult decisions, low decision authority, and skill discretion were the characteristics brought by the roles and nursing tasks of nurses in hospitals,[14,37,38] leading to job-related stress. However, among community nurses, the organization structure, and culture were the main source of job-related stress rather than nursing tasks.[21,39] Therefore, the final model of the CNSS in this study had no dimensions related to clinical practice skills. And the dimension of management and interpersonal relationship took the largest proportion of all variance of community nurse stress in this study, which confirmed the previous results.[21,39]
Moreover, the final model of the 4-factor CNSS with 25 items presented a good fit, supporting the construct validity of the new 25-item CNSS. The Cronbachs alpha coefficient for the 25-item CNSS was 0.94, similar to that of the 40-item CNSS (0.96) in a previous study.[10] In addition, the composite reliabilities of all factors were over 0.80, suggesting that the new tool has a good reliability.[40]
4.1. Study limitations
There were some limitations in this study. First, although our participants were selected randomly from Sichuan Province, the development of economic and primary health care services vary across different provinces in China, thus limiting the generalizability of our sample. Secondly, the questionnaire was a self-reported instrument, and the respondents emotional status and degree of cooperation may affect the results, although investigators conducted detailed explanations.
5. Conclusion
It is important to assess the job-related stress of community nurses. In this study, we refined the CNSS and examined the psychometric properties of the 25-item CNSS. The findings in our study supported the use of a short-form CNSS with good reliability and construct validity to evaluate the job-related stress of community nurses. More researches are needed to further test the reliability and validity of the 25-item CNSS.
Acknowledgments
Thanks for Prof. Liu Guanjian for the statistics analysis consulting.
Author contributions
The manuscript has been read and approved by all authors. The authors are alone responsible for the content and writing of the paper. All authors contributed toward data analysis, drafting and revising the paper and agreed to be accountable for all aspects of the work.
Conceptualization: Wei Zhu, Hongxia Guo, Jiping Li.
Data curation: Wei Zhu.
Formal analysis: Wei Zhu.
Investigation: Wei Zhu, Hongxia Guo.
Methodology: Wei Zhu, Hongixa Guo, Jiping Li.
Supervision: Jiping Li.
Writing – original draft: Wei Zhu.
Writing – review & editing: Wei Zhu, Hongxia Guo, Jiping Li.
Footnotes
Abbreviations: AGFI = adjusted goodness-of-fit index, AIC = Akaike Information Criterion, CFI = comparative fit index, CNS = Chinese Nurse Stress, CNSS = Chinese Community Nurse Stress Scale, GFI = goodness-of-fit index, RMSEA = root mean square error of approximation.
How to cite this article: Zhu W, Guo H, Li J. Psychometric properties of the short-form Chinese Community Nurses Stress Scale: a cross-sectional study. Medicine. 2020;99:32(e21607).
HG and JL contributed equally to this work.
This study was funded by Chinese Medical Board (11-085).
The authors declared no conflicts of interests in this study.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Fernández-Ballesteros R, Robine JM, Walker A, et al. Active aging: a global goal. Curr Gerontol Geriatr Res 2013;2013:1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Volkert J, Schulz H, H?rter M, et al. The prevalence of mental disorders in older people in Western countries – a meta-analysis. Ageing Res Rev 2013;12:339–53. [DOI] [PubMed] [Google Scholar]
- [3].Chen Z, Yu J, Song Y, et al. Aging Beijing: challenges and strategies of health care for the elderly. Ageing Res Rev iews 2010;9: 9 Suppl 1: S2–5. [DOI] [PubMed] [Google Scholar]
- [4].Lancet T. China's major health challenge: control of chronic diseases. Lancet 2011;378:457. [DOI] [PubMed] [Google Scholar]
- [5].Chen Z. Launch of the health-care reform plan in China. Lancet 2009;373:1322–4. [DOI] [PubMed] [Google Scholar]
- [6].Li L, Zhang Z, Sun Z, et al. Relationships between actual and desired workplace characteristics and job satisfaction for community health workers in China: a cross-sectional study. BMC Family Practice 2014;15:1–1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Smolowitz J, Speakman E, Wojnar D, et al. Role of the registered nurse in primary health care: meeting health care needs in the 21st century. Nurs Outlook 2015;63:130–6. [DOI] [PubMed] [Google Scholar]
- [8].Weiguang M, Xiandong M, Yi W, et al. Roles and activities of community nurses in China: a descriptive study. J Nurs Manag 2019;27:433–41. [DOI] [PubMed] [Google Scholar]
- [9].Statistical Communique on the Development of Chinese Health Program in 2018. National Health Commission of the People's Republic of China 2019. http://www.nhc.gov.cn/guihuaxxs/s10748/201905/9b8d52727cf346049de8acce25ffcbd0.shtml. Accessed May 22, 2019. [Google Scholar]
- [10].Hongxia G, Chunping N, Changqing L, et al. Perceived job stress among community nurses: a multi-center cross-sectional study. Int J NursPract 2019;25:e12703. [DOI] [PubMed] [Google Scholar]
- [11].Grumbach K, Bodenheimer T. Can health care teams improve primary care practice? JAMA 2004;291:1246–51. [DOI] [PubMed] [Google Scholar]
- [12].Nowrouzi B, Lightfoot N, Lariviere M, et al. Occupational stress management and Burnout interventions in nursing and their implications for healthy work environments: a literature review. Workplace Health Saf 2015;63:308–15. [DOI] [PubMed] [Google Scholar]
- [13].Wei ZS, Dong Y, Xiaozhi Lin MM, et al. Community health service capacity in China: a survey in three municipalities. J Eval Clin Pract 2013;19:167–72. [DOI] [PubMed] [Google Scholar]
- [14].Ilic IM, Arandjelovic M, Jovanovic JM, et al. Relationships of work-related psychosocial risks, stress, individual factors and burnout - questionnaire survey among emergency physicians and nurses. Medycyna Pracy 2017;68:167. [DOI] [PubMed] [Google Scholar]
- [15].Qin Z, Zhong X, Ma J, et al. Stressors affecting nurses in China. Contemp Nurse 2016;52:447–53. [DOI] [PubMed] [Google Scholar]
- [16].Zeller JM, Levin PF. Mindfulness interventions to reduce stress among nursing personnel: an occupational health perspective. Workplace Health Saf 2013;61:86–90. [DOI] [PubMed] [Google Scholar]
- [17].Sehlen S, Vordermark D, Schafer C, et al. Job stress and job satisfaction of physicians, radiographers, nurses and physicists working in radiotherapy: a multicenter analysis by the DEGRO Quality of Life Work Group. Radiat Oncol 2009;4:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Grunfeld E, Zitzelsberger L, Coristine M, et al. Job stress and job satisfaction of cancer care workers. Psychooncology 2010;14:61–9. [DOI] [PubMed] [Google Scholar]
- [19].Ploeg VD. Acute and chronic job stressors among ambulance personnel: predictors of health symptoms. Occup Environ Med 2003;60: Suppl 1: i40–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Kim HJ. Work stress and job satisfaction of community mental health nurses in South Korea: a qualitative content analysis. J Korean Acad Psychiatr Mental Health Nurs 2013;22:295–306. [Google Scholar]
- [21].Sveinsdóttir H, Biering P, Ramel A. Occupational stress, job satisfaction, and working environment among Icelandic nurses: A cross-sectional questionnaire survey. Int J Nurs Stud 2006;43:875–89. [DOI] [PubMed] [Google Scholar]
- [22].Naiqiang Q, Hao Z, Lihua F, et al. Analysis on work stress and occupational Burnout among community health service staff in Harbin. Med Soc 2013;26:87–9. [Google Scholar]
- [23].Mosadeghrad AM, Ferlie E, Rosenberg D. A study of relationship between job stress, quality of working life and turnover intention among hospital employees. Health Serv Manage Res 2011;24:170–81. [DOI] [PubMed] [Google Scholar]
- [24].Tarnowmordi WO, Hau C, Warden A, et al. Hospital mortality in relation to staff workload: a 4-year study in an adult intensive-care unit. Lancet 2000;356:185–9. [DOI] [PubMed] [Google Scholar]
- [25].Xiaomei L, Yanjun L. Job stressors and Burnout among staff nurses. Chinese Journal of Nursing 2000;35:645. [Google Scholar]
- [26].Graytoft P, Anderson JG. Stress among hospital nursing staff: its causes and effects. Social Science & Medicine 1981;15:639–47. [DOI] [PubMed] [Google Scholar]
- [27].Wheeler H, Riding R. Occupational stress in general nurses and midwives. Br J Nurs 1994;3:527–34. [DOI] [PubMed] [Google Scholar]
- [28].Lu DM, Ning S, Su H, et al. Occupational stress and coping strategies among emergency department nurses of China. Arch Psychiatr Nurs 2015;29:208–12. [DOI] [PubMed] [Google Scholar]
- [29].Luan X, Wang P, Hou W, et al. Job stress and burnout: a comparative study of senior and head nurses in China. Nurs Health Sci 2017;19:163–9. [DOI] [PubMed] [Google Scholar]
- [30].Ran Z, Xiaoyi F. Nurses’ stress and type-A behavior: characteristics and its relationship with mental health. Chin J Clin Psychol 2005;13:153–5. [Google Scholar]
- [31].Shu W, Xianzhang M. Primary modification of Chinese nurse job stressors questionnaire. Chin J Clin Psychol 2007;15:129–31. [Google Scholar]
- [32].Senin T, Franz M, Deuschle M, et al. QLiS-SF: development of a short form of the quality of life in schizophrenia questionnaire. BMC Psychiatry 2017;17:149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Micklewright D, St Clair Gibson A, Gladwell V, et al. Development and validity of the Rating-of-Fatigue Scale. Sports Med 2017;47:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Minglong W. Questionnaire Statistical Practice-Application of SPSS. 1st edn2011;Chongqing: Chongiqng University Press, 267–272. [Google Scholar]
- [35].Wang L, Chang Y, Chou H, et al. Psychometric properties of the short form of the health practices questionnaire–II Chinese version. J Obstetr Gynecol Neonat Nurs 2019;48:205–15. [DOI] [PubMed] [Google Scholar]
- [36].Cooper CL. Theories of organizational stress. Administrative Science Quarterly 2000; 45:640. [Google Scholar]
- [37].Mcgrath A, Reid NG, Boore J. Occupational stress in nursing. Int J Nurs Stud 2003;40:555–65. [DOI] [PubMed] [Google Scholar]
- [38].Adriaenssens J, De Gucht V, Der Doef MV, et al. Exploring the burden of emergency care: predictors of stress-health outcomes in emergency nurses. J Adv Nurs 2011;67:1317–28. [DOI] [PubMed] [Google Scholar]
- [39].Snelgrove Occupational stress and job satisfaction: a comparative study of health visitors, district nurses and community psychiatric nurses. J Nurs Manag 1998;6:8. [DOI] [PubMed] [Google Scholar]
- [40].Ferketich SL. Internal consistency estimates of reliability. Res Nurs Health 1990;13:437–40. [DOI] [PubMed] [Google Scholar]