

Abstract
Objectives:
To analyze the influence of Baduanjin exercise on blood pressure in patients with essential hypertension.
Methods:
Randomized controlled trials were identified in Chinese and English databases to study the impact of Baduanjin exercise on essential hypertension. Qualified trials were selected and methodologic quality was critically evaluated. Two reviewers selected studies independently of each other.
Results:
Twelve trials were included. There was a significant difference between the Baduanjin exercise intervention and control groups with regard to the change in systolic blood pressure (SBP) [SMD = − 1.80, 95% CI (− 2.86, − 0.73), P = .0009] and diastolic blood pressure (DBP) [SMD = −0.22, 95% CI (−2.00, −0.57), P = .0004]. Taking into account the subgroup analyses, the combined results showed that Baduanjin plus Antihypertensive drugs significantly reduced both SBP and DBP over a period > 12 weeks in all studies.
Conclusions:
Compared with control interventions, Baduanjin exercise seems to be an effective physical exercise in treating essential hypertension. Different training durations can lead to different effects.
Keywords: Baduanjin exercise, essential hypertension, meta-analysis, mind–body exercise
1. Introduction
With the rapid development of society, people's diet structure and living habits have undergone great changes. Increased intake of high-protein and high-fat food, irregular rest and reduced exercise have led to a sharp increase in the number of patients with hypertension.[1,2] Hypertension is a clinical syndrome characterized by increased systemic arterial pressure. The syndrome remains a major threat to public health.[3] One in four adults worldwide is suffering from high blood pressure, and this ratio is expected to rise to 29% by 2025.[4] The prevalence of hypertension is 37.3% in developed countries and 22.9% in developing countries. Among the population with hypertension, more than 90% suffer from essential hypertension, which makes this hypertension type a major global chronic non-communicable disease without a secondary cause.[5] As an important aspect of hypertension care, lifestyle management of patients with hypertension, including self-management, physical activity, and medical nutrition treatment, has attracted increasing attention.[6] Physical activity is an important part of hypertension management planning and plays a specific role in the management of blood pressure and prevention of hypertension complications in patients with essential hypertension.[7] The European Society of Hypertension (ESH) suggests that patients with essential hypertension should increase their physical activity to increase flexibility, muscle strength and balance.[6]
Baduanjin exercise is favored as a kind of physical and mental therapy. Badunjin exercise originated from ancient martial arts in oriental culture and has been widely used for centuries.[8] In modern times, it is used as a form of movement to improve body consciousness and balance.[9] This is because Baduanjin exercise is considered a pleasurable activity that combines meditation with gentle movements.[10] A growing body of research has shown that Baduanjin exercise strengthens the joints of the limbs, modulates the pressure receptors in the aortic arch and carotid sinus, and plays a role in lowering blood pressure and expanding coronary arteries.[11–13]
Research has shown that[14] traditional Chinese exercise can effectively reduce SBP and DBP in patients, thereby improving symptoms in patients with cardiovascular disease. Some studies have shown that Baduanjin exercise as an alternative treatment for cardiovascular patients can improve the health of cardiovascular patients and reduce the occurrence of cardiovascular risk factors.[15] However, some studies have shown that Baduanjin exercise is not enough to improve and reduce blood pressure in patients with essential hypertension. In view of the differences in the current studies, it is necessary to comprehensively, objectively and systematically evaluate the effect of the Baduanjin exercise on blood pressure control in patients with essential hypertension.
Therefore, we conducted a systematic review of this topic to evaluate the effects of Baduanjin exercise on blood pressure in patients with essential hypertension and determine whether different intervention durations have different effects on patients with essential hypertension.
2. Methods
2.1. Research strategy
We searched the PubMed, Cochrane Library, Embase, CNKI, VIP, and Wanfang databases for studies published before February 2020. The search terms were blood pressure, hypertension, hypertensive, primary hypertension, essential hypertension, Baduanjin exercise, and randomized controlled trials (RCTs). Two independent reviewers selected and screened all results and, in cases where they disagreed, a third reviewer was asked for advice. The review applied the PRISMA statement guidelines for reporting systematic reviews and meta-analyses.[16]
2.2. Eligibility criteria
The inclusion criteria for this systematic review were as follows:
-
1)
randomized controlled trial (RCT) design related to the therapeutic effect of Baduanjin exercise;
-
2)
human subjects were recruited;
-
3)
Baduanjin exercise was included as the main intervention in the experimental group and was compared to a non-active control condition; and
-
4)
at least one blood pressure parameter was reported, and data including the mean and standard deviation of each group at baseline and post-intervention, along with the number of participants in each group, were obtainable.
The criteria for exclusion were as follows:
-
1)
duplicate publications;
-
2)
nonintervention designs (such as case-control studies, cohort studies cross-sectional studies, case reports and experiences, theory research, and reviews); and
-
3)
non-clinical tests and animal experiments.
2.3. Data extraction
Two review authors independently screened the literature using the predetermined inclusion criteria and extracted data from the trials. The following information was extracted: participant characteristics, intervention and outcome data, adverse effects, and methodological quality. We resolved any disagreements about the extracted data from the included studies by consensus and consulted a third review author if disagreements persisted.
2.4. Risk of bias assessment
The risk of study bias was assessed using the Cochrane Handbook for Systematic Reviews. The risk of bias was evaluated with regard to the following aspects: generating random sequences, allocation of hidden methods, application of the blinding method, incomplete results, selective reporting of results, and other bias. Funnel diagrams were used to detect publication bias.
2.5. Statistical analysis
2.5.1. Extracting and merging of data
The Cochrane Collaboration's Review Manager 5.3 software was used to extract the relevant dichotomous or continuous data from the literature for analysis. Risk ratios (RRs) were calculated for dichotomous data, whereas the mean differences (MDs) and standard deviations (SDs) were calculated for continuous variables. The corresponding 95% confidence intervals (CI) and forest plots were used in both cases. In our meta-analysis, we used SD values when the data were in the same unit. When they were in different units, we performed a conversion. The chi-squared and I2 (inconsistency) tests were used to detect heterogeneity. A P value < .10 or I2 > 50% indicated that there was significant heterogeneity. The fixed-effect model was used when P > .10 and I2 < 50%, and the random-effect model was used when P < .10 or I2 ≥ 50%.
2.5.2. Data conversion
The final values of systolic blood pressure (SBP) and diastolic blood pressure (DBP) were used as indicators to evaluate the efficacy of Baduanjin exercise in the intervention group and the control group. When SBP or DBP were not explicitly reported in the study, we calculated the mean value and SD of SBP and DBP with the following formulas:
1) If the number of samples (n) and the standard error (SE) were known, the SD was calculated as:
SD = SE × √n
2) Estimates of SD were calculated if the number of samples (n), mean, and 95% CI[17,18] were known: “a” and “b” are the upper and lower confidence limits, respectively:
SD = a − mean /1.96 √n
SD = mean − b /1.96 √n
3. Results
3.1. Study selection
A total of 116 study reports were screened, 62 of which were excluded because they were duplicate publications. After reading the titles and abstracts, an additional 11 articles were excluded, and 43 articles were retained. Among them, 31 articles did not meet the inclusion criteria, 16 studies were improperly compared, and for 15 studies, we could not extract the data. Finally, 12 RCTs with a total of 961 participants were included. The PRISMA flow diagram is shown in Figure 1.
Figure 1.
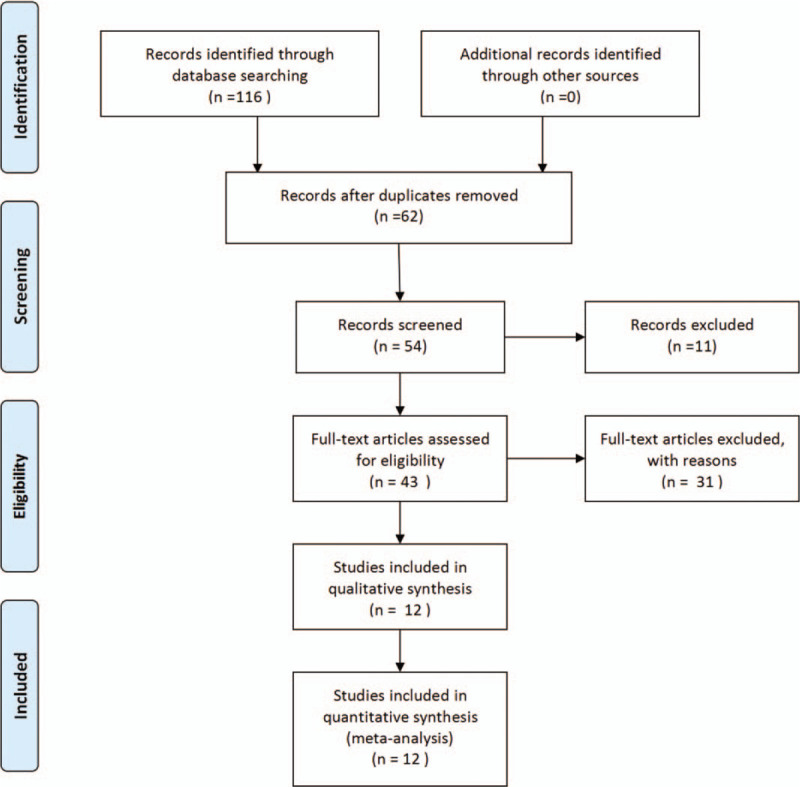
Study selection procedure according to the PRISMA statement.
3.2. Study characteristics
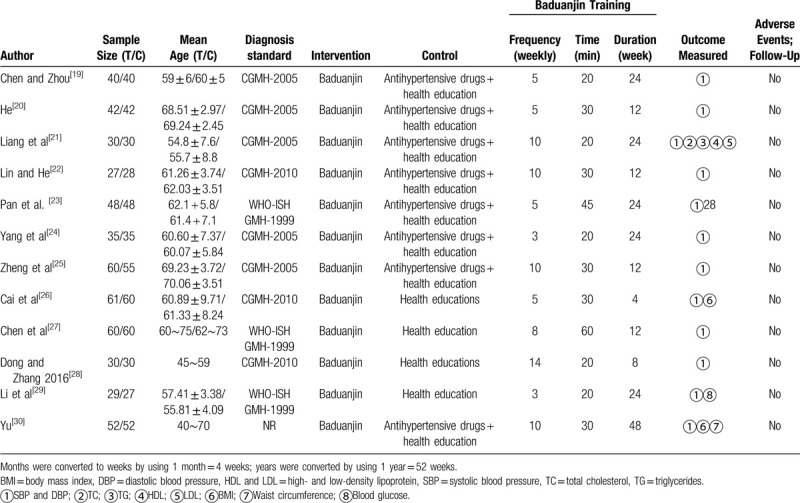
The principal study characteristics are summarized in Table 1. Twelve studies were published between 2012 and 2019. A total of 961 participants were included. The number of participants in the individual studies ranged from 27 to 61. Seven of the included trials were single-center studies. The included studies were from the same country. The duration of the intervention varied from 4 to 48 weeks. All participants had essential hypertension.
Table 1.
Randomized controlled trials included in the systematic review on the effects of Baduanjin on hypertension.
3.3. Quality assessment
Figures 2 and 3 provide an overview of the risk of bias for the included studies based on the tools provided by the Cochrane Manual. All included studies used a double-blind approach and reported dropouts. Most trials reported allocation concealment and random allocation but did not mention the specific method used. Eight studies[19,20,24–29] reported automatic generation of random sequences by a computer, while 2 studies[24,28] reported that they divided participants into an experimental group and a control group by using random number tables. Selective reporting was unbiased but without any description to evaluate the existence of other biases. All the included trials reported whether adverse events occurred.
Figure 2.
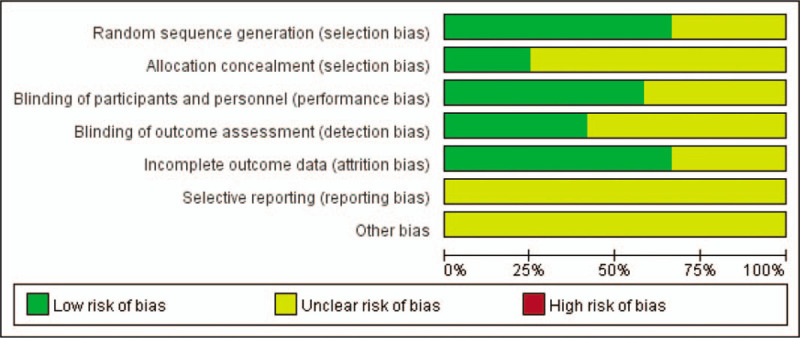
Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.
Figure 3.
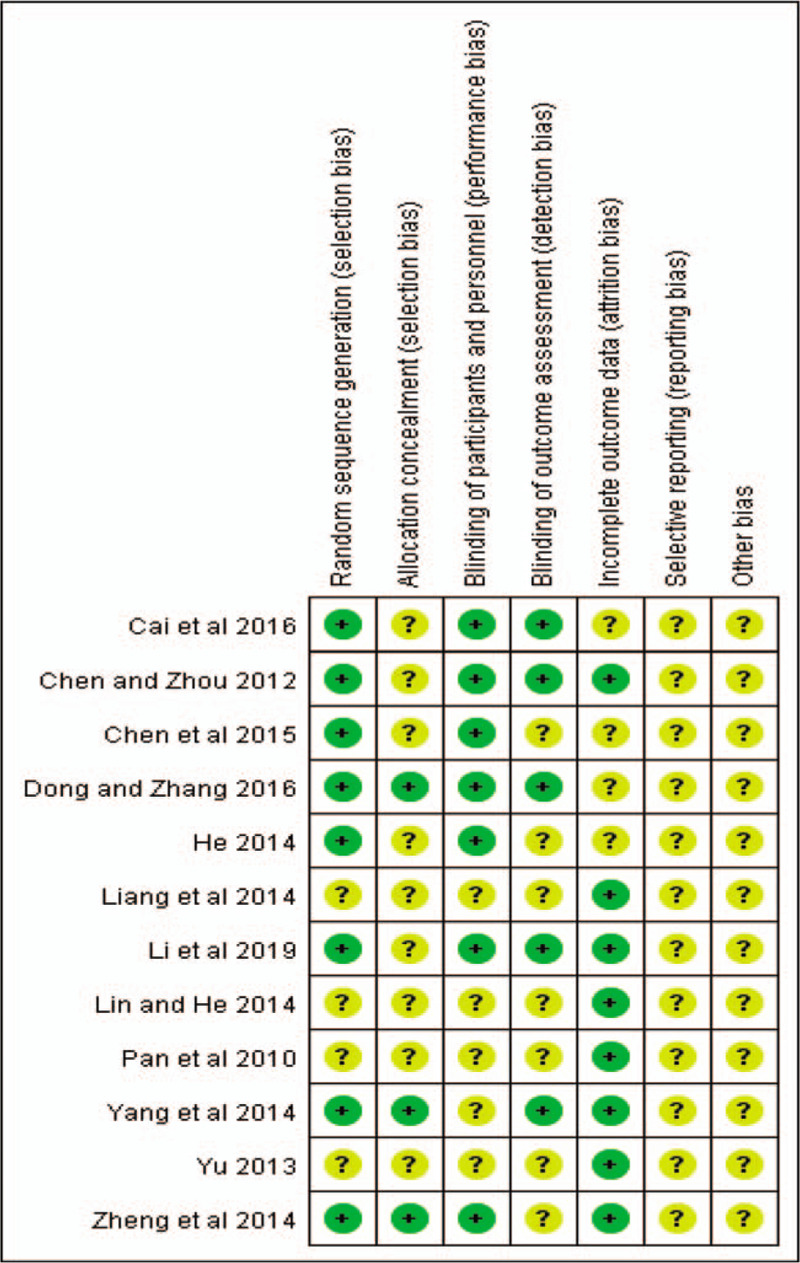
Risk of bias summary: review authors’ judgments about each risk of bias item for each included study.
3.4. Study results
3.4.1. SBP
Figure 4 shows the forest plots of the SBP analysis. We divided the intervention groups according to different Baduanjin intervention methods. Seven included trials,[19–25] which included 560 participants, compared the SBP in patients with hypertension receiving “Baduanjin plus Antihypertensive drugs versus Antihypertensive drugs”. The combined result was statistically significant (SMD = −0.77, 95% CI (−1.16, −0.38), P = .0001), and Baduanjin plus Antihypertensive drugs had a positive effect on SBP in patients with essential hypertension compared to that in the control group. Five included trials,[26–30] which included 401 participants, compared the SBP in patients with hypertension receiving “Baduanjin versus Health educations” There was significant heterogeneity in SBP between the essential hypertension patients who participated in the Baduanjin intervention ant the patients in the control group (I2 = 95%, P < .00001). There was a significant difference in SBP between the essential hypertension patients who received a Baduanjin intervention and the control group (SMD = −1.80, 95% CI (−2.86, −0.73), P = .0009).
Figure 4.
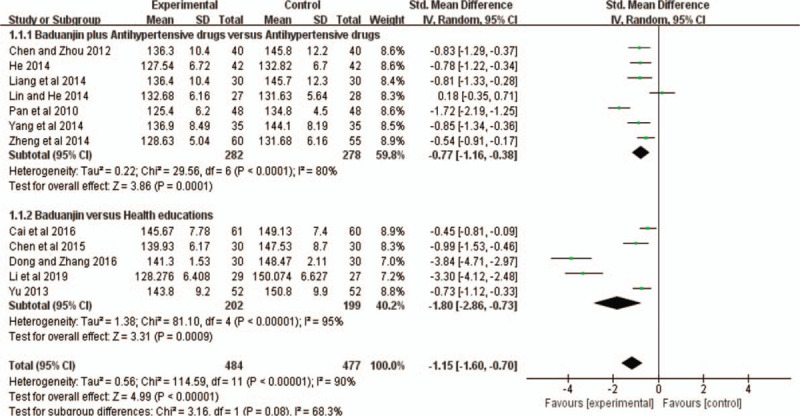
Forest plot of the comparison of the mean systolic blood pressure in twelve randomized control trials on the effect of Baduanjin exercise on essential hypertension.
3.4.2. SBP Subgroup results
First, we divided the intervention group according to the different Baduanjin plus Antihypertensive drugs training durations. The subgroup analysis was performed according to different durations of Baduanjin plus Antihypertensive drugs intervention: ≤12 weeks and > 12 weeks. For the interventions with a duration ≤12 weeks,[20,22,25] the combined results of the three studies showed that Baduanjin plus Antihypertensive drugs did significantly reduce SBP (WMD = −2.65, 95% CI (−4.11, −1.19), P = .0004), with high heterogeneity (I2 = 78%, P = .01) (Fig. 5). In the intervention duration >12 weeks group,[19,21,23,24] the combined results of the four studies also showed that Baduanjin plus Antihypertensive drugs did significantly reduce SBP (WMD = −8.99, 95% CI (−10.68, −7.30), P < .00001), with low heterogeneity (I2 = 0%, P = .80) (Fig. 5).
Figure 5.
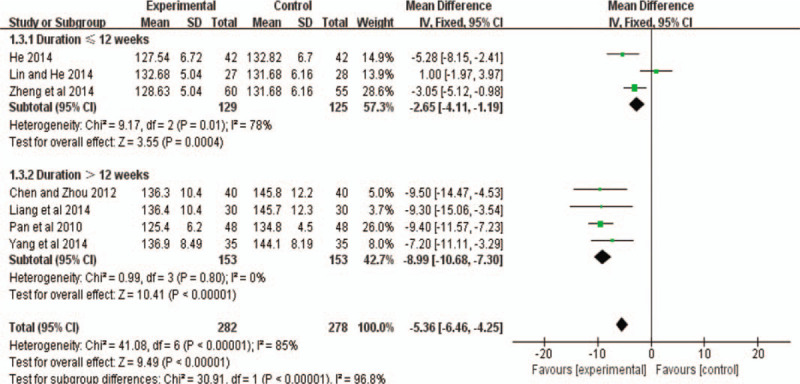
Forest plot of the comparison between Baduanjin exercise and the control group for the outcome SBP. The subgroup analysis was performed based on different intervention durations: ≤12 weeks and >12 weeks.
3.4.3. DBP
In terms of reducing DBP, there was a significant difference between the Baduanjin exercise and the control group (SMD = − 0.22, 95% CI (−2.00, −0.57), P = .0004) (Fig. 6). There was substantial heterogeneity among the included studies (I2 = 90%, P < .00001).
Figure 6.
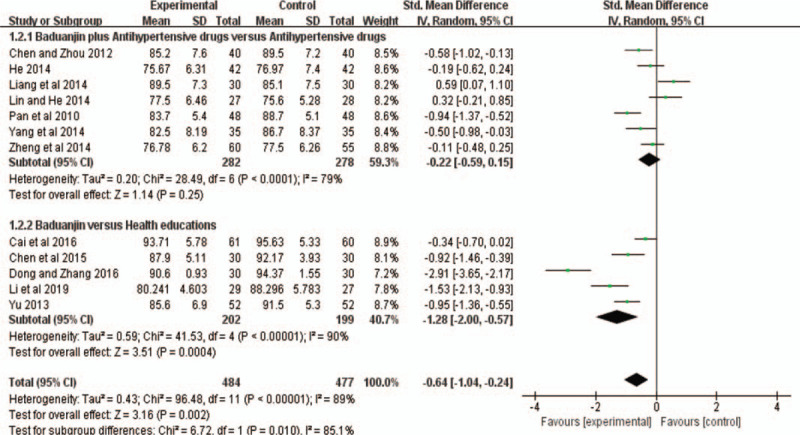
Forest plot of the comparison of the mean diastolic blood pressure in twelve randomized control trials on the effect of Baduanjin exercise on essential hypertension.
3.4.4. DBP Subgroup results
The subgroup analysis was performed according to different durations of Baduanjin plus Antihypertensive drugs intervention: ≤12 weeks and >12 weeks. For the interventions with a duration ≤12 weeks,[20,22,25] the combined results of the three studies showed that Baduanjin plus Antihypertensive drugs did not significantly reduce DBP (WMD = − 0.13, 95% CI (−1.66, −1.40), P = .87), with low heterogeneity (I2 = 31%, P = .23) (Fig. 7). During the intervention durations >12 weeks,[19,21,23,24] the combined results of the four studies showed that Baduanjin plus Antihypertensive drugs did significantly reduce DBP (WMD = −3.21, 95% CI (−4.67, −1.75), P < .0001), with high heterogeneity (I2 = 85%, P = .0002) (Fig. 7).
Figure 7.
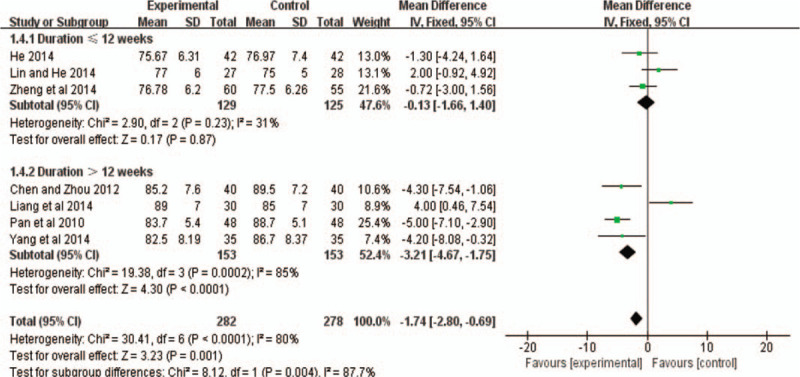
Forest plot of the comparison between Baduanjin exercise and the control group for the outcome DBP. The subgroup analysis was performed based on different intervention durations: ≤12 weeks and >12 weeks.
3.5. Publication bias
The publication bias of the 12 RCTs was evaluated with a funnel plot. Figure 8 shows that the publication bias across the studies was small.
Figure 8.
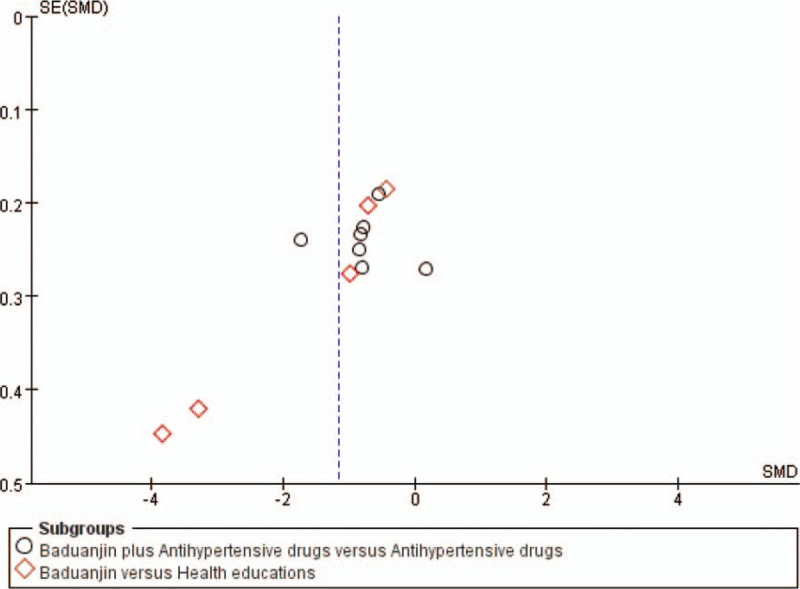
Funnel plot of thirteen randomized control trials on the effect of Baduanjin exercise on essential hypertension.
4. Discussion
Baduanjin exercise originated from eastern traditional culture, and its development has absorbed traditional philosophy, the theory of Yin and Yang, the theory of the 5 elements, the theory of meridians and other traditional Chinese theories.[31] Baduanjin exercise originated in ancient times and is widely used. As a kind of low-intensity aerobic exercise, it is increasingly popular in terms of health.[32] Previous studies have revealed that practicing Baduanjin exercise can increase the central excitability of breath and aspiration, increase the excited focus spread to the parasympathetic nerve, increase parasympathetic excitability, increase peripheral small pulse relaxation, remove spasms, reduce blood flow resistance, and decrease blood pressure.[33,34] Baduanjin exercise has the coordinated effect of regulating the heart, body and breath, which produces a relaxation effect, reduces hyperactivity of the sympathetic nervous system, corrects the imbalance of the nervous system, and improves symptoms of hyperactivity of the sympathetic nervous system, such as dizziness and neck tension.[35,36] However, previous clinical research conclusions have been inconsistent. Meanwhile, in previous systematic reviews, the possible impact of different Baduanjin exercise training durations has not been evaluated. Through quantitative synthesis, we found that Baduanjin exercise, as a physical exercise, seems to be effective in controlling blood pressure in patients with essential hypertension and suggest that different training durations lead to different therapeutic effects.
4.1. Summary of the main results
Combined with our research results, we found that Baduanjin exercise is effective in treating essential hypertension. This systematic review and meta-analysis showed that the SBP and DBP effects in the Baduanjin exercise intervention group were stronger than those of the control group. There was heterogeneity in the reduction of SBP and DBP, but significant differences in the effects were observed. In the subgroup analysis of SBP, the results showed that there was a significant decrease in SBP with Baduanjin plus Antihypertensive drugs for ≤12 weeks or >12 weeks.
There was a significant difference in the DBP reduction between those who Baduanjin exercise and the control group (with intervention duration ≤12 weeks or >12 weeks). However, Baduanjin plus Antihypertensive drugs did not significantly reduce DBP and the studies had high heterogeneity. Baduanjin exercise has many different durations, so it can be used in many combinations to make mental, psychological and even physiological changes to the human body. Our research is the first to notice that different training durations of Baduanjin exercise intervention may lead to different effects. We analyzed subgroups of different Baduanjin exercise training durations. The results showed that Baduanjin plus Antihypertensive drugs had effectiveness in reducing SBP or DBP, after a duration of >12 weeks. However, when the duration was ≤12 weeks, Baduanjin plus Antihypertensive drugs had no effect on reducing DBP.
Studies have shown that the cerebral cortex is in a “relaxed” state when practising Baduanjin exercise, which is a state of protective inhibition that can reduce the excitability of the sympathetic nervous system, leading to a decrease in norepinephrine and epinephrine, which, in turn, can decrease vasoconstrictive enzyme activity.[37,38] With Baduanjin exercise, the tissue is stimulated to release histamine, irritants and other substances, which relaxes the blood vessels and reduces blood pressure.[39] During the practice of Baduanjin exercise, the muscles are always in a relaxed state, which reduces the peripheral resistance of the blood vessels and eventually leads to a reduction in blood pressure.[40] One study proved that Baduanjin exercise promoted health, prevented disease, and had a superior effect on arterial stiffness and static/dynamic balance.[41,42] Some studies have shown that Baduanjin exercise can enhance the use of active neural networks by regulating physical and psychological methods.[43,44]
4.2. Limitations
This study has several limitations. First, in some cases, we had to calculate and transform data, rather than these being provided directly. Second, the study distribution between the 12 RCTs was included, which may affect the meta-analysis results. The results of the included studies showed significant differences, which may be due to inconsistent exercise intensity. We performed a sensitivity analysis of the included RCTs and found that 2 studies may be a source of most of the heterogeneity. In both studies, the quality of life scale was used as a measurement index, which may have an impact on the comprehensive measurement results. In addition, language and publication biases limited our study. Finally, this review only included randomized controlled trials. In the future, there is a need for a greater diversity of research, such as cooperation between multiple centers, more rigorous clinical reports, and prospective studies.
4.3. Clinical implications
We summarize the current status of the research on the effect of Baduanjin exercise in patients with essential hypertension and provide data to support future clinical trials of essential hypertension. Although this study shows that Baduanjin exercise can effectively control blood pressure levels in patients with essential hypertension, due to the low quality of these research methods and the observed clinical heterogeneity, the current evidence and potential findings should be interpreted carefully. In future research, more attention should be paid to the influence of different Baduanjin exercise intensities and measurement methods in studies of patients with essential hypertension. In conclusion, this study found that Baduanjin exercise can be used to help control blood pressure levels.
5. Conclusion
Compared with control interventions, Baduanjin exercise seemed to be an effective physical exercise intervention in patients with essential hypertension. Different training durations led to different effects. More RCTs with rigorous study designs are needed to determine the efficacy of Baduanjin exercise in the treatment of essential hypertension and to apply Baduanjin exercise in healthy lifestyle interventions to prevent or treat essential hypertension and other related chronic diseases.
Acknowledgments
The authors thank Professor Huaien Bu for providing important information.
Author contributions
Conceptualization: Yuanyuan Guan, Yang Hao, Yun Guan, Hongwu Wang.
Data curation: Yuanyuan Guan, Yang Hao.
Formal analysis: Yuanyuan Guan, Yang Hao.
Investigation: Yang Hao, Yun Guan.
Methodology: Yuanyuan Guan, Yang Hao, Yun Guan, Hongwu Wang.
Project administration: Hongwu Wang.
Software: Yuanyuan Guan.
Supervision: Hongwu Wang.
Writing – original draft: Yuanyuan Guan.
Writing – review & editing: Yuanyuan Guan.
Footnotes
Abbreviations: BMI = body mass index, CI = confidence interval, CNKI = China National Knowledge Infrastructure, DBP = diastolic blood pressure, ESH = European Society of Hypertension, HDL = high-density lipoprotein, LDL = low-density lipoprotein, MD = mean difference, PRISMA = preferred reporting items systematic reviews and meta-analyses, PubMed = National Library of Medicine, RCT = randomized controlled trial, RR = risk ratio, SBP = systolic blood pressure, SD = standard deviation, SE = standard error, TC = total cholesterol, TG = triglycerides, VIP = VIP Database for Chinese Technical Periodicals, WMD = weighted mean difference.
How to cite this article: Guan Y, Hao Y, Guan Y, Wang H. Effects of baduanjin exercise on essential hypertension: a meta-analysis of randomized controlled trials. Medicine. 2020;99:32(e21577).
This project was supported by the National Key Research and Development Program of China (approval No.: 2017YFC1703305) and the Basic Research on Health Identification of Traditional Chinese Medicine in Tianjin Colleges and Universities “Innovation Team Training Plan” (approval No.: TD13−5049) during the 13th five-year plan period.
The authors have no conflicts of interest to disclose.
All the data in this paper support the results of this study.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Zhang X, Huang L, Peng X, et al. Association of handgrip strength with hypertension among middle-aged and elderly people in Southern China: a cross-sectional study. Clin Exp Hypert (New York, NY: 1993) 2020;42:190–6. [DOI] [PubMed] [Google Scholar]
- [2].Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC Guidelines for themanagement of arterial hypertension The Task Force for the management ofarterial hypertension of the European Society ofHypertension (ESH) and of the European Society of Cardiology (ESC). J Hypert 2013;31:1281–357. [DOI] [PubMed] [Google Scholar]
- [3].Bath A, Irfan FB, Aggarwal S, et al. National trends and outcomes of essential hypertension on emergency departments in USA. J Am Coll Cardiol 2019;73:1890–1890.30999991 [Google Scholar]
- [4].Mansia G, De Backer G, Dominiczak A, et al. 2007 ESH-ESC Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Press 2007;16:135–232. [DOI] [PubMed] [Google Scholar]
- [5].Lauche R, Peng W, Ferguson C, et al. Efficacy of Tai Chi and qigong for the prevention of stroke and stroke risk factors: a systematic review with meta-analysis. Medicine (Baltimore) 2017;96:e8517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 2018;39:3021–104. [DOI] [PubMed] [Google Scholar]
- [7].Poggio R, Melendi SE, Beratarrechea A, et al. Cluster randomized trial for hypertension control: effect on lifestyles and body weight. Am J Prev Med 2019;57:438–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Zou LY, Pan ZJ, Yeung A, et al. A review study on the beneficial effects of Baduanjin. J Altern Complement Med 2018;24:324–35. [DOI] [PubMed] [Google Scholar]
- [9].Chen TT, Yue GH, Tian Y, et al. Baduanjin mind-body intervention improves the executive control function. Front Psychol 2016;7:2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].An T, He ZC, Zhang XQ, et al. Baduanjin exerts anti-diabetic and anti-depression effects by regulating the expression of mRNA, lncRNA, and circRNA. Chin Med 2019;14:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Li ZM, Cao Y, Tao SX. The rehabilitative effects of baduanjin qigong in chronic kidney disease (1-3 Stage). Basic Clin Pharmacol Toxicol 2019;124:36–7. [Google Scholar]
- [12].Xie Y, Guo F, Lu YY, et al. A 12-week Baduanjin Qigong exercise improves symptoms of ankylosing spondylitis: a randomized controlled trial. Complement Ther Clin Pract 2019;36:113–9. [DOI] [PubMed] [Google Scholar]
- [13].Li JY, Yu F, Huang N, et al. Effect of Baduanjin exercise on patients with chronic heart failure: protocol for a systematic review and meta-analysis. BMJ Open 2019;9:e028771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Yu M, Li S, Li S, et al. Baduanjin exercise for patients with ischemic heart failure on phase-II cardiac rehabilitation (BEAR trial): study protocol for a prospective randomized controlled trial. Trials 2018;19:381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Xiao X, Wang J, Gu Y, et al. Effect of community based practice of Baduanjin on self-efficacy of adults with cardiovascular diseases. Plos One 2018;13:e0200246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg (London, England) 2010;8:336–41. [DOI] [PubMed] [Google Scholar]
- [17].Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 2005;5:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Wan X, Wang W, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014;14:135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Chen H, Zhou Y. Effects of Baduanjin on blood pressure and serum high-sensitivity C-reactive protein in patients with essential hypertension. Chin J Rehab Med 2012;27:178–9. [Google Scholar]
- [20].He X. Rehabilitation efficacy of Baduanjin exercise in elderly patients with hypertension. J Cardiovasc Rehab Med 2015;24:252–4. [Google Scholar]
- [21].Liang Y, Liao S, Han C, et al. Effects of baduanjin exercise intervention on blood pressure and blood lipid in patients with essential hypertension. Henan Chin Med 2014;34:2380–1. [Google Scholar]
- [22].Fang L, He Q. Observation on the curative effect of Baduanjin exercise on the elderly with grade 1 hypertension. Chin J Geriatr 2014;12:25–6. [Google Scholar]
- [23].Pan H, Feng Y. Clinical observation of baduanjin exercise on the rehabilitation treatment of grade 1 hypertension in the elderly. J Nanjing Inst Phys Educa (Natural Science Edition) 2010;9:4–6. [Google Scholar]
- [24].Yang Hui. Effect of Baduanjin on quality of life and autonomic nervous response in patients with hypertension. Hebei United University 2014;44:609. [Google Scholar]
- [25].Zheng L, Chen Q, et al. Effects of Baduanjin exercise on vascular endothelial function in elderly patients with grade 1 hypertension. Chin J Rehab Med 2014;29:223–7. [Google Scholar]
- [26].Cai Y, Shang Y, Ma L, et al. Intervention study on the health education of middle-aged and elderly people in the community by Baduanjin combined with health education. Chong Med J 2016;45:795–6. [Google Scholar]
- [27].Chen Y, Liu R, He R. Effect of Baduanjin on sleep quality in elderly patients with hypertension. Hunan J Trad Chin Med 2015;31: 52-53+82. [Google Scholar]
- [28].Dong C, Zhang Y. Antihypertensive Baduanjin” in blood pressure control of middle-aged patients with grade I essential hypertension. J Nurs Chinese People's Liber Army 2016;33:32–5. [Google Scholar]
- [29].Li W, Wu Z, Jing C, et al. Effects of Baduanjin on blood glucose and blood pressure in patients with prediabetes accompanied by mild hypertension. N Chin Med 2019;51:291–4. [Google Scholar]
- [30].Yu H. Clinical observation on 104 patients with hypertension and obesity treated by baduanjin exercise therapy. Chin Clin 2013;41:47–8. [Google Scholar]
- [31].Koh TC. Baduanjin -- an ancient Chinese exercise. Am J Chin Med 1982;10:14–21. [DOI] [PubMed] [Google Scholar]
- [32].Zou LY, Sasaki JE. A systematic review and meta-analysis of baduanjin for health benefits. Res Q Exer Sport 2017;88:A62–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Liu SJ, Ren Z, Wang L, et al. Mind− Body (Baduanjin) exercise prescription for chronic obstructive pulmonary disease: a systematic review with meta-analysis. Int J Environ Res Public Health 2018;15: [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Fan B, Song W, Zhang J, et al. The efficacy of mind-body (Baduanjin) exercise on self-reported sleep quality and quality of life in elderly subjects with sleep disturbances: a randomized controlled trial. Sleep Breath = Schlaf & Atmung 2020;24:695–701. [DOI] [PubMed] [Google Scholar]
- [35].Li HN, Ge D, Liu SW, et al. Baduanjin exercise for low back pain: a systematic review and meta-analysis. Complement Ther Med 2019;43:109–16. [DOI] [PubMed] [Google Scholar]
- [36].Xiao CM, Zhuang YC, Kang Y. Effect of health Qigong baduanjin on fall prevention in individuals with parkinson's disease. J Am Geriatr Soc 2016;64:E227–8. [DOI] [PubMed] [Google Scholar]
- [37].Zheng G, Chen B, Fang Q, et al. Baduanjin exercise intervention for community adults at risk of ischamic stroke: A randomized controlled trial. Sci Rep 2019;9:1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Zhao Y. The impact of qigong baduanjin on cognitive function & mental state in patients with type 2 diabetes. Med Sci Sports Exer 2019;51:554–5. [Google Scholar]
- [39].Lan C, Chou SW, Chen SY, et al. The aerobic capacity and ventilatory efficiency during exercise in Qigong and Tai Chi Chuan practitioners. Am J Chin Med 2004;32:141–50. [DOI] [PubMed] [Google Scholar]
- [40].Ryu H, Lee HS, Shin YS, et al. Acute effect of qigong training on stress hormonal levels in man. Am J Chin Med 1996;24:193–8. [DOI] [PubMed] [Google Scholar]
- [41].Zou L, Wang C, Chen X, et al. Baduanjin exercise for stroke rehabilitation: a systematic review with meta-analysis of randomized controlled trials. Int J Environ Res Public Health 2018;15: [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Xiao C, Zhuang Y, Kang Y. Effect of health qigong baduanjin on fall prevention in individuals with Parkinson's disease. J Am Geriatr Soc 2016;64:e227–8. [DOI] [PubMed] [Google Scholar]
- [43].Zhang HL, Zhu MX, Song Y, et al. Baduanjin exercise improved premenstrual syndrome symptoms in Macau women. J Tradit Chin Med 2014;34:460–4. [DOI] [PubMed] [Google Scholar]
- [44].Zou L, Yeung A, Quan X, et al. Mindfulness-Based Baduanjin exercise for depression and anxiety in people with physical or mental illnesses: a systematic review and meta-analysis. Int J Environ Res Public Health 2018;15: [DOI] [PMC free article] [PubMed] [Google Scholar]