

ABSTRACT
Background and Objectives:
One of the important steps toward achieving a successful fixed partial denture treatment is the fabrication of interim restorations with good marginal adaptation. Poor marginal adaptation of the interim restorations will allow ingress of fluids and microorganisms between the restorations and may lead to caries and pulpitis. The objective of this study was to evaluate and compare the marginal accuracy of interim restorations made from two polymethyl methacrylate (PMMA) and two bis-acryl materials.
Materials and Methods:
An in vitro method was used to replicate a clinical procedure in which the interim crown was made using a direct technique. A maxillary first molar typodont tooth was prepared to receive a full cast crown restoration having 1 mm chamfer and a taper of 5°, and then the prepared artificial tooth was cast into a cobalt chromium metal die. Wax patterns were prepared on the metal die using type 2 inlay wax for full metal crowns. The impression of the die along with the wax pattern was made with a putty-type polyvinyl siloxane, and this impression was used as a mold for making interim restorations. Two PMMA and two bis-acryl provisional crown materials were distributed as follows: Group A: Unifast Trad (GC Dental), Group B: DPI self-cure tooth molding material, Group C: Structur 2 QM (VOCO), and Group D: Cool Temp Natural (Coltene/Whaledent). A total of 60 interim restorations from all the four materials were fabricated (15 interim restorations from each material). The marginal discrepancy of the interim restoration was determined by measuring the space between the margin of the interim restoration and the finish line of the metal die at four vertical reference lines previously marked at the midpoint of the metal die finish line at the buccal, palatal, mesial, and distal surfaces of the die. The marginal gaps were visualized at ×45 magnification using a stereomicroscope and interpreted using ProgRes image capture software.
Results:
The mean marginal discrepancy calculated in PMMA materials was 269 µm for DPI and 205 µm for Unifast Trad, and the mean marginal gap for the bis-acryl material was 171 µm for Cool Temp and 140 µm for Structur 2 QM.
Interpretation and Conclusion:
Comparison of marginal accuracy showed that bis-acryl provisional crown material showed better marginal accuracy than PMMA provisional crown material. Among the materials tested, Structur 2 QM showed the best marginal accuracy, and the least marginal accuracy was shown by DPI.
KEYWORDS: Bis-acryl, interim restoration, marginal integrity, polymethyl methacrylate
INTRODUCTION
Restoration of broken down teeth by means of a crown to maintain form, function, and aesthetics has been the preferred choice of treatment for patients. Advances in material science and better understanding of mechanical and biological factors of tooth preparation and fixed prosthodontics have become the standard of care for restoration of broken down tooth with a crown or replacement of single or multiple missing teeth with a fixed partial denture.
The steps in the treatment of fixed partial denture involve both clinical and laboratory phases. After the biomechanical preparation of the tooth, an indirect fabrication of the definitive prosthesis takes place in a well-equipped laboratory. This may need 1 or 2 weeks considering the various steps involved. During this period, the prepared tooth structure in the oral cavity is vulnerable to pulpal trauma due to exposed dentinal tubules during the tooth preparation, risk of fracture due to weakened tooth structure, migration of the tooth, and functional and aesthetic concerns. As a solution to all these problems, provisional crowns are used as an important component of fixed prosthodontic restoration. Provisional crowns are also known as the temporary restorations or interim restoration.
A provisional restoration is a fixed or removable prosthesis, fabricated to enhance aesthetics, stabilization, and/or function for a limited period, after which it is to be replaced by a definite prosthesis as per the Glossary of Prosthodontic Terms-9.[1]
Until the definitive restoration is ready, the provisional crowns serve the function of providing stabilization of occlusal relationships, protection to dentin-pulpal system, and address the aesthetic and functional concerns.
The success of provisional restoration is largely dependent on its marginal accuracy. Unless the temporary restoration has a well-adapted and well-contoured margin, it may be difficult to achieve this goal. Obtaining the best possible marginal adaptation of provisional restoration effectively prevents plaque accumulation and insulates the pulp from thermal, bacterial, and chemical abuse. Pronounced marginal discrepancy can result in the development of pulpal sensitivity, gingival recession, and tissue inflammation.[2]
Provisional restorations can be fabricated either using prefabricated shells or it can be custom-made. The methods for fabrication of custom-made provisional prosthesis may be categorized as (1) direct, (2) indirect, and (3) combination of direct and indirect.[3] In the literature, it is found that the custom-made techniques are the preferred method for the fabrication of provisional restoration to have better marginal accuracy. Among these techniques, the direct technique is preferred by most of the clinicians because of ease of fabrication and shortened chairside time, despite superior performance of indirect technique.[4] Over a period, a large number of materials have been used for the fabrication of provisional restorations. The oldest and the most commonly used materials are the acrylic resins. The marginal accuracy varies with the different materials and different commercial brands. The purpose of this in vitro study was to evaluate and compare the marginal accuracy of provisional crowns fabricated from different commercially available acrylic resin materials using a direct technique.
MATERIALS AND METHODS
This study to measure and compare the marginal accuracy of interim crown restorations made from self-cure composite and autopolymerizing acrylic resin was conducted in the Department of Prosthodontic Crown and Bridge and Department of Oral Pathology, Sree Anjaneya Institute of Dental Sciences, Calicut, Kerala, India. One artificial typodont maxillary first molar was mounted on a dental stone base. The mounted maxillary first molar was prepared for full cast crown, using the standard principles of tooth preparation with 1 mm chamfer finish line and 5° taper using a standard airotor dental handpiece and diamond burs. A metal die was cast from the prepared typodont tooth and mounted in autopolymerizing acrylic resin in the shape of a cylinder, 20 mm in diameter and 15 mm high [Figure 1]. The base portion was then lubricated with petroleum jelly and mounted in a dental stone block that was furnished with a metal box (3 × 3 × 2.5), and a close-fitting metal top (3.5 × 3.5 × 4.5) was used to replicate an impression tray. Then, petroleum jelly was applied uniformly on the mounted metal die and a wax pattern for full metal crown was prepared using type 2 inlay wax [Figure 2A]. Putty impression material was loaded on the metal top and placed over the metal die–metal box assembly along the indexing. Once the impression material had set completely, the clamp was released and the impression removed. The wax pattern lodged in the putty impression was carefully taken out. The impression was then inspected for any defects and completeness. It acted as a mold for making the provisional restoration [Figure 2B]. The temporization materials chosen for the study were as follows: Group A: Unifast Trad (GC Dental, Japan), Group B: Self-cure tooth molding material (DPI, India), Group C: Structur 2 QM (VOCO, Germany), Group D: Cool Temp Natural (Coltene/Whaledent, Switzerland). The temporization materials were manipulated according to manufacturer’s instructions and loaded in the prepared mold. Care was taken to make sure that the mold was completely seated on the metal die setup with the indexing as reference. The temporary restoration and metal die were placed in water bath at 37°C, till the polymerization was complete. After the polymerization was complete, the gingival margin of the interim restoration was trimmed with fine bur at low speed under ×3.5 magnification, and no further finishing and no further polishing procedures were carried out on the interim restoration. All the interim crowns fabricated were thoroughly checked for voids, cracks, deficiencies, and acceptable marginal finish. From each of the materials chosen for the study, 15 interim crowns were made following the same aforementioned procedure, and a total of 60 interim crowns were fabricated for the four temporization materials used in the study. All the interim crowns were marked with a dot of different colors, just above the crown margin, coinciding with the indexing on the metal die (mesial: red, distal: blue, buccal: black, and lingual: no color), and the samples from different materials were stored in separate labeled container. All the samples were stored in water at room temperature for 24h before being tested. For measuring the marginal accuracy, the provisional restorations were individually secured on the metal die with the help of a spring-loaded holding device [Figure 3]. The marginal discrepancy of the interim restorations was determined by visualizing and measuring the gap between the margin of the interim restorations and the finish line of the metal die. For each interim restoration, measurements were made at four vertical reference points 1 mm below the finish line at four different points to represent buccal, lingual, mesial, and distal surfaces of the die. The marginal accuracy was measured using stereomicroscope at ×45 magnification. A specially designed spring-loaded holding device was used to measure and replace the provisional crowns precisely on master die. Photographs of each side were taken after calibrating microscope at ×45 and using the camera mounted to the microscope [Figure 4]. Measurements were made at vertical reference lines marked at midpoint on each side (mesial, distal, buccal, and palatal) of metal die finish line and were interpreted using ProgRes image capture software. The marginal gap observed for all the 60 samples were recorded and statistically analyzed using descriptive statistics, one-way analysis of variance (ANOVA), Scheffe post hoc test, and independent sample t test.
Figure 1.

The finished and polished casting mounted in acrylic block
Figure 2.

(A) Wax pattern on the metal die (B) Putty index prepared from the wax pattern
Figure 3.

Spring-loaded holding device for securing crown on metal die
Figure 4.
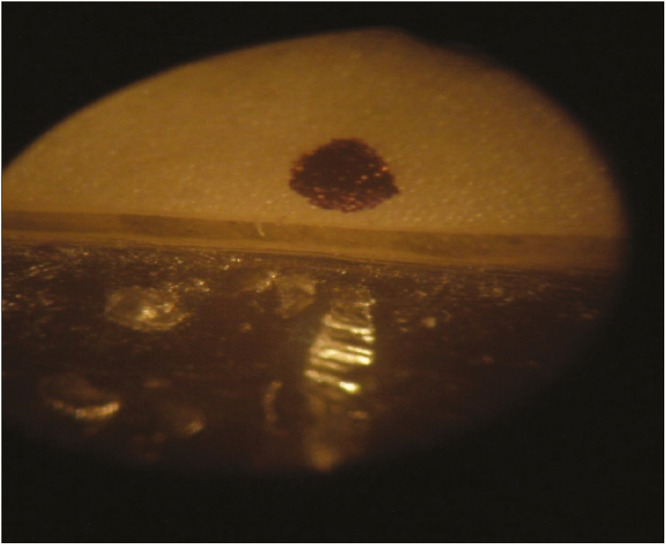
Marginal gap as seen under stereomicroscope (mesial surface of Unifast Trad specimen)
OBSERVATION AND RESULTS
Table 1, using the one-way ANOVA descriptive, shows the mean, standard deviation, maximum, and minimum values (in millimeter) of marginal discrepancies of two PMMA (DPI and Unifast Trad) and two bis-acrylic (Cool Temp and Structur 2 QM) provisional crown materials evaluated using stereomicroscope.
Table 1.
One-way analysis of variance descriptives showing the mean, standard deviation, maximum, and minimum values for all four materials tested
| One-way analysis of variance descriptives | Total | ||||
|---|---|---|---|---|---|
| N | Mean | Std. deviation | Minimum | Maximum | |
| DPI | 15 | 0.269940 | 0.0149159 | 0.2489 | 0.3039 |
| Unifast Trad | 15 | 0.205983 | 0.0075632 | 0.1867 | 0.2183 |
| Cool Temp | 15 | 0.171672 | 0.0141767 | 0.1452 | 0.1876 |
| Structur 2 QM | 15 | 0.140478 | 0.0118904 | 0.1228 | 0.1579 |
| Total | 60 | 0.197018 | 0.0499604 | 0.1228 | 0.3039 |
Among the four provisional crown materials tested, the maximum marginal accuracy was shown by Structur 2 QM (mean, 0.140478 mm with SD of 0.0118904 mm), followed by Cool Temp (mean, 0.171672 with SD of 0.0141767) then Unifast Trad (mean, 0.205983 mm with SD of 0.0075632), and the minimum marginal accuracy by DPI (mean, 0.269940 mm with SD of 0.0149159 mm).
Scheffe post hoc test revealed that DPI had highest marginal gap, followed by Unifast Trad and Cool Temp, and Structur 2 QM had the best marginal accuracy [Table 2].
Table 2.
Scheffe post hoc test
| Total Scheffe test | |||||
|---|---|---|---|---|---|
| Materials | N | Subset for alpha = 0.05 | |||
| 1 | 2 | 3 | 4 | ||
| Structur 2 QM | 15 | 0.140478 | |||
| Cool Temp | 15 | 0.171672 | |||
| Unifast Trad | 15 | 0.205983 | |||
| DPI | 15 | 0.269940 | |||
Table 3 shows the intergroup comparison between the two groups (PMMA and bis-acrylic provisional crown materials) by application of the t test for equality. A highly significant difference was found (P = 0.000) when compared for the marginal discrepancy with a mean difference 0.081887. Between the two groups of provisional crown material bis-acrylic material was found to have better marginal accuracy than PMMA material.
Table 3.
Comparison between the two groups polymethyl methacrylate and bis-acrylic) provisional restorative materials by application of the t test for equality
| Group statistics | ||||||
|---|---|---|---|---|---|---|
| Groups | N | Mean | Std. deviation | Std. error of mean | ||
| Total | Acrylic | 30 | 0.237962 | 0.0345384 | 0.0063058 | |
| Bis-acrylic | 30 | 0.156075 | 0.0204187 | 0.0037279 | ||
| Independent test | ||||||
| t test for equality | ||||||
| t | df | Sig (2-tailed) | Mean difference | |||
| Total | Equal variances | 11.179 | 58 | 0.000 | 0.081887 | |
P < 0.05
Comparison shows highly significant value
Graph 1 depicts the mean marginal gap between two groups (PMMA and bis-acrylic provisional crown materials).
Graph 1.
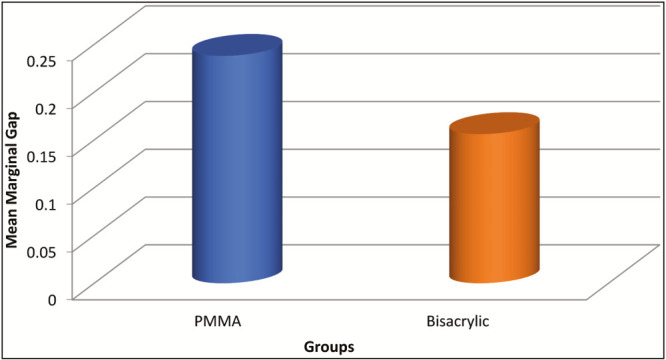
Mean marginal gap between two groups (polymethyl methacrylate and bis-acrylic) provisional restorative materials
DISCUSSION
Provisional crowns are essential for the maintenance of periodontal health and also help in guided tissue healing of the surrounding gingival tissues.[4] Provisional restorations can also be used as an important tool to provide an insight into the final outcome and limitations of the treatment to the patient.[5] In the past, provisional restorations were mostly considered from the functional aspect, but in recent years, the increased aesthetic demand has led to evolution of an array of provisional restorative materials with superior color stability, a more precise fit along with improved mechanical properties. Commercially, there are three types of provisional restorative materials available. These are ethyl methacrylates, methyl methacrylates, and bis-acryl resin composites. Ethyl methacrylates have poor aesthetics and wear resistance, and thus methyl methacrylates and bis-acryl resin composite materials are preferred for the fabrication of provisional restorations.[5] Among all requirements of provisional restorative materials, marginal accuracy is of most importance because poor marginal adaptation allows ingress of fluids and microorganisms into the gap and may predispose the tooth to caries or pulpitis. In addition, poor marginal adaptation of provisional crowns will cause mechanical irritation to surrounding tissues and increase plaque accumulation with subsequent periodontal problems, especially when the margins of restorations are placed subgingivally.[6] Direct technique of provisional crown fabrication is usually preferred for single- to four-unit fixed partial denture provisional restorations.[7] The major concern for direct technique is exothermic heat that is generated during polymerization. There are several means of protecting the prepared tooth from thermal insult due to exothermic heat generated during polymerization. A thin layer of insulating material such as lubricant can be applied on the prepared tooth, this not only protects pulp and gingiva but also facilitates the removable of a set resin.[8] In this study, the residual polymerization of the specimens were carried out at 37°C in water bath in an incubator. As suggested by Koumjian and Holmes,[9] all the specimens were stored in water for 24h as they showed that water absorption compensated for polymerization shrinkage in PMMA materials, whereas they produced no change in bis-acryl provisional materials. In this study, the artificial maxillary right first molar was prepared for complete crown restoration with 1 mm chamfer finish line and approximately 5° of taper. The prepared tooth was casted in cobalt–chromium alloy to get a metal die. The advantage of using metal die of prepared tooth for the fabrication of specimens and measurements was to prevent damage of margins of master die by repeated seating of specimens and to standardize the tooth size.[10] The mean marginal gap obtained for PMMA materials was 269 µm for DPI and 205 µm for Unifast Trad, and the mean marginal gap for the bis-acryl material was 171 µm for Cool Temp and 140 µm for Structur 2 QM. According to McLean and von Fraunhofer,[11] the range of values of clinically acceptable marginal gap starts from 50 μm and reaches out to approximately 120 μm. According to Crispin et al.,[12] studies have reported 30 μm to be clinically acceptable gap discrepancy.
The marginal accuracy obtained for the bis-acryl material was significantly higher than the PMMA materials. The volumetric polymerization shrinkage for PMMA is 6% when compared with 1% to 2% for composite materials.[2] Polymerization shrinkage also depends on the molecular weight of the monomer. The larger the molecular weight of the monomer before polymerization, the lower the shrinkage strain due to the lower proportion of the monomer to be reacted for a given volume. For that reason, PMMA-based materials are expected to have higher shrinkage strain than bis-acryl materials.[13] Bis-acryl materials are provided as a cartridge-based dispensing system, which may contribute to the superior marginal accuracy because of a more accurately proportioned and consistent mix. The polymerization reaction is exothermic, which causes additional contraction when the restoration cools, and the temperature rise in PMMA is reported to be higher than that in bis-acryl material, thus resulting in greater marginal contraction in relation to PMMA materials.[14] The marginal accuracy obtained for the Unifast Trad was better than that for DPI.
Manufacturer-recommended polymer:monomer ratio of Unifast Trad is 1g/0.5 mL and that of DPI is 1.3g/1 mL. Nejatidanesh et al.[6] stated that a greater volume of monomer will result in higher polymerization shrinkage due to the higher proportion of the monomer available to react for a given volume.
The marginal accuracy obtained for the Structur 2 QM was better than that for the Cool Temp. This difference may be attributed to the matrix composition, filler content, and size of the filler used in the materials.
All the four provisional restorative materials used in the study showed clinically acceptable levels of marginal gap. Of the four materials tested on PMMA material, DPI showed the least marginal accuracy, and on bis-acryl material, Structur 2 QM showed the best marginal accuracy.
CONCLUSION
On the basis of the analysis of the results obtained and limitations of the study, the following conclusions were drawn:
Comparison between bis-acryl group and the PMMA group showed highly significantly results with bis-acryl group showing better marginal accuracy than PMMA group.
Among the materials tested, Structur 2 QM showed the best marginal accuracy, followed by Cool Temp, then Unifast Trad (GC dental), and the least marginal accuracy was shown by DPI.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.The glossary of prosthodontic terms. J Prosthet Dent. 2017;117:e1–e105. doi: 10.1016/j.prosdent.2016.12.001. [DOI] [PubMed] [Google Scholar]
- 2.Burns DR, Beck DA, Nelson SK Committee on Research in Fixed Prosthodontics of the Academy of Fixed Prosthodontics. A review of selected dental literature on contemporary provisional fixed prosthodontic treatment: report of the committee on research in fixed prosthodontics of the academy of fixed prosthodontics. J Prosthet Dent. 2003;90:474–97. doi: 10.1016/s0022-3913(03)00259-2. [DOI] [PubMed] [Google Scholar]
- 3.Vahidi F. The provisional restoration. Dent Clin North Am. 1987;31:363–81. [PubMed] [Google Scholar]
- 4.Federick DR. The provisional fixed partial denture. J Prosthet Dent. 1975;34:520–6. doi: 10.1016/0022-3913(75)90039-6. [DOI] [PubMed] [Google Scholar]
- 5.Yap AU, Mah MK, Lye CP, Loh PL. Influence of dietary simulating solvents on the hardness of provisional restorative materials. Dent Mater. 2004;20:370–6. doi: 10.1016/j.dental.2003.06.001. [DOI] [PubMed] [Google Scholar]
- 6.Nejatidanesh F, Lotfi HR, Savabi O. Marginal accuracy of interim restorations fabricated from four interim autopolymerizing resins. J Prosthet Dent. 2006;95:364–7. doi: 10.1016/j.prosdent.2006.02.030. [DOI] [PubMed] [Google Scholar]
- 7.Kopp FR. Esthetic principles for full crown restorations. Part II: provisionalization. J Esthet Dent. 1993;5:258–64. doi: 10.1111/j.1708-8240.1993.tb00790.x. [DOI] [PubMed] [Google Scholar]
- 8.Moulding MB, Teplitsky PE. Intrapulpal temperature during direct fabrication of provisional restorations. Int J Prosthodont. 1990;3:299–304. [PubMed] [Google Scholar]
- 9.Koumjian JH, Holmes JB. Marginal accuracy of provisional restorative materials. J Prosthet Dent. 1990;63:639–42. doi: 10.1016/0022-3913(90)90320-c. [DOI] [PubMed] [Google Scholar]
- 10.Lang R, Rosentritt M, Behr M, Handel G. Fracture resistance of PMMA and resin matrix composite-based interim FPD materials. Int J Prosthodont. 2003;16:381–4. [PubMed] [Google Scholar]
- 11.McLean JW, von Fraunhofer JA. The estimation of cement film thickness by an in vivo technique. Br Dent J. 1971;131:107–11. doi: 10.1038/sj.bdj.4802708. [DOI] [PubMed] [Google Scholar]
- 12.Crispin BJ, Watson JF, Caputo AA. The marginal accuracy of treatment restorations: a comparative analysis. J Prosthet Dent. 1980;44:283–90. doi: 10.1016/0022-3913(80)90012-8. [DOI] [PubMed] [Google Scholar]
- 13.Kim SH, Watts DC. Exotherm behavior of the polymer-based provisional crown and fixed partial denture materials. Dent Mater. 2004;20:383–7. doi: 10.1016/j.dental.2003.11.001. [DOI] [PubMed] [Google Scholar]
- 14.Rosenstiel SF, Land MF, Fujimoto J. Contemporary fixed prosthodontics. 3rd ed. St. Louis, MO: Mosby; 2000. pp. 391–4. [Google Scholar]