

ABSTRACT
Early childhood caries is an aggressive type of caries leading to early loss of crown structure. Retention of post and core is important in restoring teeth where there is compromised coronal structure. This case report describes the use of root stumps of primary teeth as a post and core for primary teeth.
KEYWORDS: Post and core, primary teeth, root stumps
INTRODUCTION
Early childhood caries is a rapidly progressing type of caries with loss of crown structure in an early part of child’s life. This can lead to aesthetic, psychological, and speech defects.[1] Dental treatment aims to restore the lost tooth structure as well as to maintain functional integrity of oral and maxillofacial region and prevent developing psychological stress.[2] With the lack of cognitive development in children at their early childhood, treating them is a challenge for pediatric dentists.
Loss of crown structure demands the clinician to extract support from the remaining tooth structure, at times only root stumps to recreate coronal part of the tooth. To define as an ideal post and core in primary teeth, it should be resorbable and should provide an adequate retention and resistance without causing radicular fracture and secondary infection.
Extension of post in the primary root canal is vital in determining the retention and fracture resistance of the post. In primary teeth to prevent obstruction to erupting or developing permanent teeth, they are restricted to the coronal third of the root approximately 3–4 mm. To increase the resistance and retention of post, it should be placed more apically in the middle third of the root. Numerous methods and techniques were adopted to create coronal structures with a different post and core systems.[3,4,5,6] Most of these systems are non-resorbable and hence cannot be pushed apically, leading to poor resistance and retention. Therefore, the search for a material that can resorb at a similar rate to the primary tooth was investigated. This has led to the introduction of biomimetic materials in clinical practice.
The use of extracted teeth as the post and core is not a new concept but has been advocated in permanent teeth. Lack of availability of extracting primary anterior teeth restricts them to use it as a post and core. This article presents and explains the use of root stumps of primary tooth as a post and core.
CASE REPORT
A 3-year-old definitely negative behavior female child reported to the department of pediatric and preventive dentistry with a chief complaint of pain and fractured right primary maxillary central incisors. Her medical history was not significant and dental history revealed that discoloration of maxillary incisor was seen a few years ago, and chipping of the tooth has occurred progressively, leading to loss of complete coronal structure. Intraoral examinations revealed that right maxillary central incisor is caries extending up to the cervical third with an exposure of the pulp chamber, restored and pulp therapy done 54, dental caries in 51, 61, 62, and 64. Orthopantomogram confirmed the clinical findings and presence of permanent teeth. Pulpectomy followed by intra-radicular biological post and core with crown was planned for 52; restoration of 51, 61, 62, and 64; and stainless-steel crown for 54.
Extracted root stump is placed in a sodium hypochlorite 3% solution in a day for dissolution of organic structure [Figure 1]. The surface layer is removed using an ultrasonic scalar and washed thoroughly with saline and hydrogen peroxide. This removes any remnants of organic structure as well as conditions the root stump. It is disinfected and sterilized at 121°C at 15 lbs pressure for 15min.[7] This is stored in saline mixed with hypochlorite till donor is available.
Figure 1.

Extracted root stump of primary maxillary molar to prepare post
Pulpectomy for 51 was performed and zinc oxide eugenol was used as obturating materials. A thinner mix of zinc oxide initially is used to coat the canal walls. A thick mix of zinc oxide eugenol is condensed in the canal with a help of cylindrical condenser. About 6 mm of cement is removed from the coronal end of the root on the same day. Cotton is placed in the root canal space and appointment is given after 1 day for post and core preparation. This time interval allows the cement to set and form a hard base.
In this case, biological post was prepared from the palatal root of human primary maxillary first molar. For the second time, the post is sterilized at 130°C for 5min before checking for fit. On the basis of the prediction of the root canal shape of the restored teeth, it is cut buccolingually (if it is conical) or mesiodistally (if it is ribbon shaped) with a metal disc. It is then washed with saline and checked for fit [Figure 2]. After minor adjustments and checking for mild resistance, intraoral periapical radiograph is taken to check for fit, which appears as mild radiopacity as it is demineralized.[8,9] It is cemented with glass ionomer cement with the post at least 3–4 mm above the cervical line and clearance of at least 1–2 mm from the opposing teeth should be maintained [Figures 3 and 4]. The coronal part of the post is restored with a thin layer of glass ionomer cement later on with a composite by sandwich technique. Composite crown built up is performed with a pedo jacket crown [Figure 5].
Figure 2.
Prepared post prepared according to the root canal shape
Figure 3.

Intraoperative clinical photograph
Figure 4.
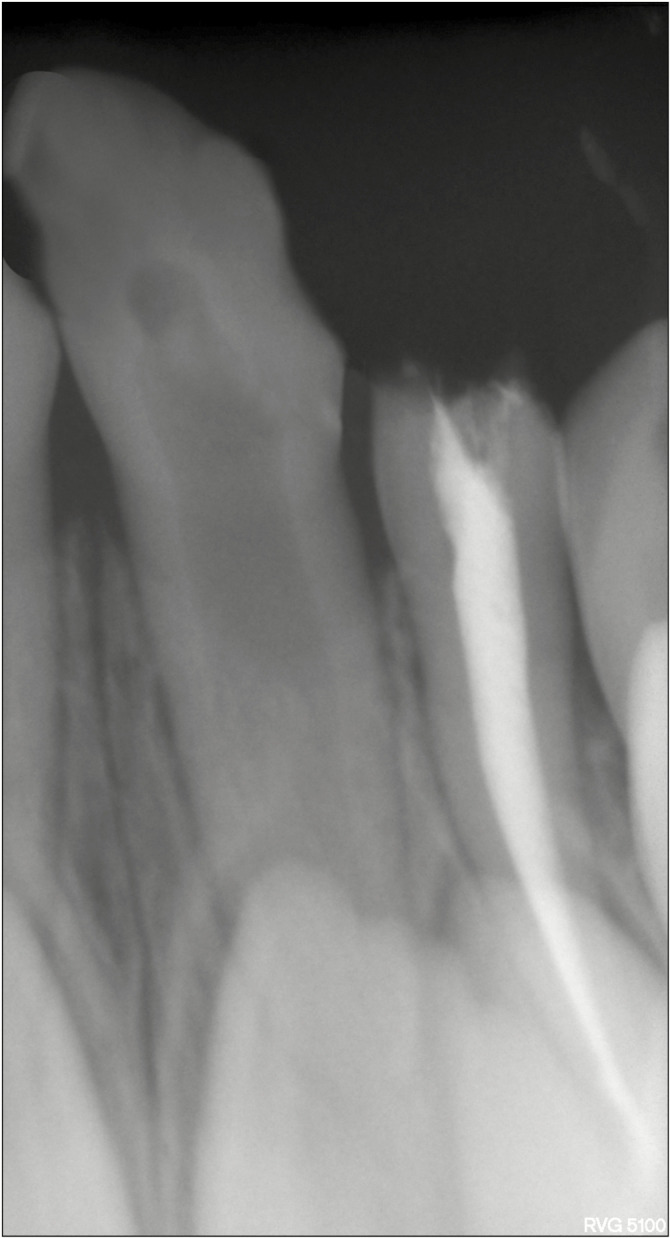
Radiograph with root post inserted in 52
Figure 5.

Postoperative clinical photograph after cementation of crown
DISCUSSION
Rehabilitation of an endodontically treated primary tooth similar to natural teeth is still a great challenge for clinicians. Posts made from different materials, such as fiberglass, screw post carbon fiber, metal, and ceramic, were investigated for intracanal retention, resistance, and stability of coronal structure.[10,11,12,13] The high failure rate of post and core in primary teeth is attributed to absence of tooth structure, poor adhesion of bonding agent to primary teeth, and poor cooperative ability of the child. Recent advances aimed at increasing the bond strength or adhesive strength of the post and core, thereby reducing the post length or short post. These are turning out to be expensive and technique sensitive and also require the expertise of the operator.[14]
Biological post is prepared from permanent anterior teeth. Many case reports have been published in permanent teeth only. Extracted primary teeth could be used as a post and core in primary teeth. The availability of primary teeth is less, added to that the bioavailability of primary anterior teeth is still scarce. Hence, we put forward the use of root stumps of any primary teeth. With the mere availability of root stumps in primary teeth comparatively, these can be inexpensive, less technique sensitive, resorbing properties similar to the natural teeth, and provide good adhesion. Elasticity of a post is comparable to that of root dentin, thereby acting as a shock absorber and limiting the stress transmitted to the dentinal walls. By the presence of similar bonding structures, monoblock effect is created by luting cement.[15] As these posts are reabsorbable, these can be extended to the middle and apical third of the root, thereby increasing retention and resistance of the post considerably.
Hence, it is a simpler, easier, and inexpensive technique for treating severely damaged teeth.
CONCLUSION
The use of root stumps as the post and core is easy to fabricate and inexpensive. To evaluate retention, resistance of these posts, and long-term success, further studies have to be performed.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century–the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003;31:3–23. doi: 10.1046/j..2003.com122.x. [DOI] [PubMed] [Google Scholar]
- 2.Nunn ME, Braunstein NS, Krall Kaye EA, Dietrich T, Garcia RI, Henshaw MM. Healthy eating index is a predictor of early childhood caries. J Dent Res. 2009;88:361–6. doi: 10.1177/0022034509334043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mortada A, King NM. A simplified technique for the restoration of severely mutilated primary anterior teeth. J Clin Pediatr Dent. 2004;28:187–92. doi: 10.17796/jcpd.28.3.2554xv412644ru13. [DOI] [PubMed] [Google Scholar]
- 4.Aminabadi NA, Farahani RM. The efficacy of a modified omega wire extension for the treatment of severely damaged primary anterior teeth. J Clin Pediatr Dent. 2009;33:283–8. doi: 10.17796/jcpd.33.4.p8m168x8784719h3. [DOI] [PubMed] [Google Scholar]
- 5.Sharaf AA. The application of fiber core posts in restoring badly destroyed primary incisors. J Clin Pediatr Dent. 2002;26:217–24. doi: 10.17796/jcpd.26.3.y3660x50n5l0jv0p. [DOI] [PubMed] [Google Scholar]
- 6.Island G, White GE. Polyethylene ribbon fibers: a new alternative for restoring badly destroyed primary incisors. J Clin Pediatr Dent. 2005;29:151–6. [PubMed] [Google Scholar]
- 7.Viera CL, Ribeiro CC. Polyethylene fiber tape used as a post and core in decayed primary anterior teeth: a treatment option. J Clin Pediatr Dent. 2001;26:1–4. [PubMed] [Google Scholar]
- 8.Subramaniam P, Babu KL, Sunny R. Glass fiber reinforced composite resin as an intracanal post: a clinical study. J Clin Pediatr Dent. 2008;32:207–10. doi: 10.17796/jcpd.32.3.700t77h520473149. [DOI] [PubMed] [Google Scholar]
- 9.Claudia DA, Wanderely MT. Biological restoration of primary anterior teeth. Quintessence Int. 2000;31:404–6. [PubMed] [Google Scholar]
- 10.Lolayekar NV, Bhat SV, Bhat SS. Disinfection methods of extracted human teeth. J Oral Health Community Dent. 2007;27:27–9. [Google Scholar]
- 11.Pantera EA, Jr, Schuster GS. Sterilization of extracted human teeth. J Dent Educ. 1990;54:283–5. [PubMed] [Google Scholar]
- 12.Parsell DE, Stewart BM, Barker JR, Nick TG, Karns L, Johnson RB. The effect of steam sterilization on the physical properties and perceived cutting characteristics of extracted teeth. J Dent Educ. 1998;62:260–3. [PubMed] [Google Scholar]
- 13.Rocha Rde O, Das Neves LT, Marotti NR, Wanderley MT, Correa MSNP. Intracanal reinforcement fiberin pediatric dentistry: a case report. Quintessence Int. 2004;35:263–8. [PubMed] [Google Scholar]
- 14.Martelli R. Fourth-generation intraradicular posts for the aesthetic restoration of anterior teeth. Pract Periodontics Aesthet Dent. 2000;12:579–84; quiz 586-8. [PubMed] [Google Scholar]
- 15.Busato AL, Loguercio AD, Barbosa AN, Sanseverino Mdo C, Macedo RP, Baldissera RA. Biological restorations using tooth fragments. Am J Dent. 1998;11:46–9. [PubMed] [Google Scholar]